
Endobronchial Ultrasonography with a Guide Sheath Transbronchial Biopsy for Diagnosing Peripheral Pulmonary Lesions within or near Fibrotic Lesions in Patients with Interstitial Lung Disease

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
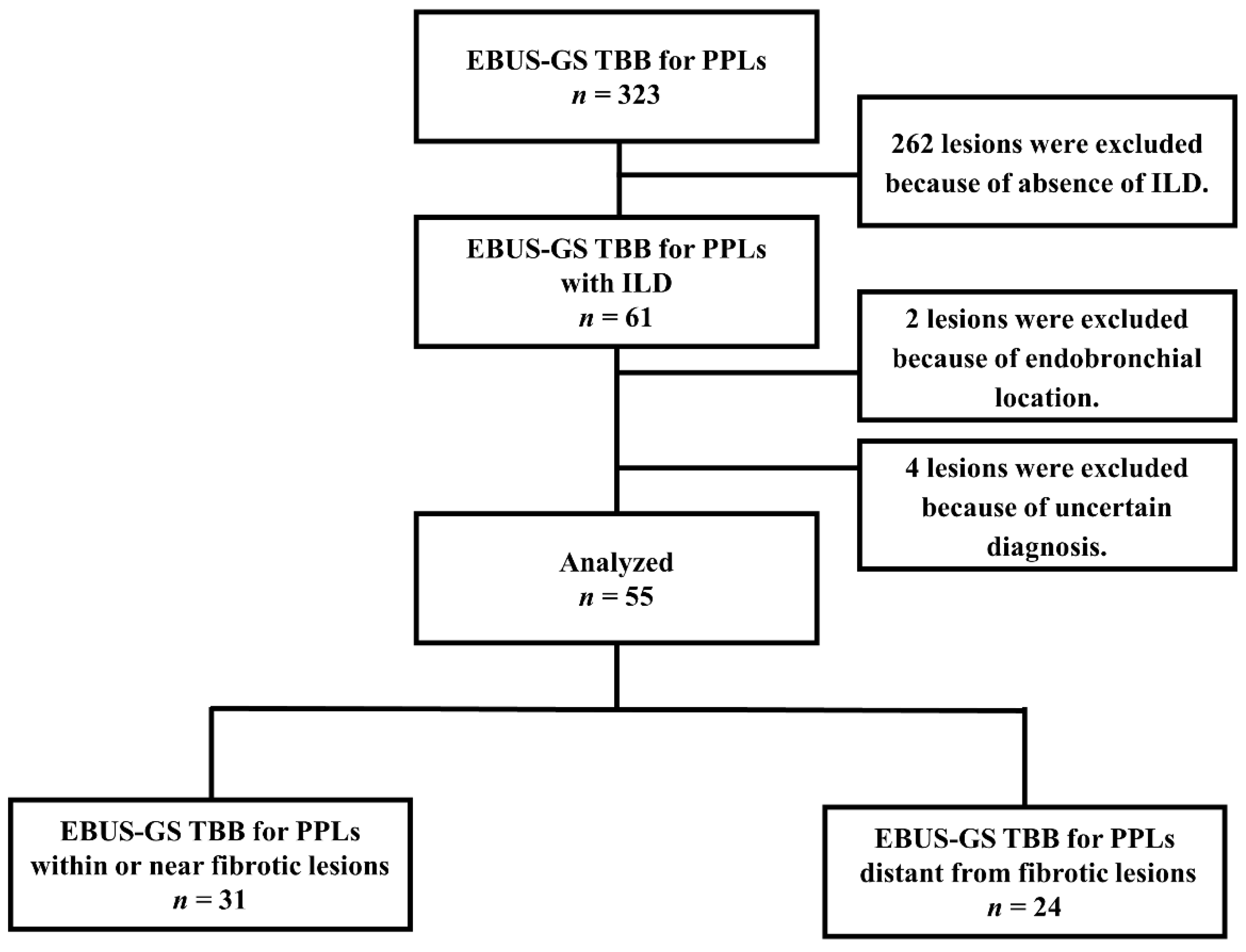
2.1. Patient Enrolment
2.2. EBUS-GS TBB Procedure
2.3. Variables
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Diagnostic Yields by Probe Location and Disease Type between PPLs within or near Fibrotic Lesions and Those Distant from Fibrotic Lesions
3.3. Factors Related to Successful Diagnosis of PPLs by EBUS-GS TBB in Patients with ILD
3.4. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Naccache, J.M.; Gibiot, Q.; Monnet, I.; Antoine, M.; Wislez, M.; Chouaid, C.; Cadranel, J. Lung cancer and interstitial lung disease: A literature review. J. Thorac. Dis. 2018, 10, 3829–3844. [Google Scholar] [CrossRef]
- Khan, K.A.; Kennedy, M.P.; Moore, E.; Crush, L.; Prendeville, S.; Maher, M.M.; Burke, L.; Henry, M.T. Radiological characteristics, histological features and clinical outcomes of lung cancer patients with coexistent idiopathic pulmonary fibrosis. Lung 2015, 193, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Yung, R.C. Tissue diagnosis of suspected lung cancer: Selecting between bronchoscopy, transthoracic needle aspiration, and resectional biopsy. Respir. Care Clin. N. Am. 2003, 9, 51–76. [Google Scholar] [CrossRef]
- Goto, T. Measuring Surgery Outcomes of Lung Cancer Patients with Concomitant Pulmonary Fibrosis: A Review of the Literature. Cancers 2018, 10, 223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minami-Shimmyo, Y.; Ohe, Y.; Yamamoto, S.; Sumi, M.; Nokihara, H.; Horinouchi, H.; Yamamoto, N.; Sekine, I.; Kubota, K.; Tamura, T. Risk factors treatment-related death associated with chemotherapy and thoracic radiotherapy for lung cancer. J. Thorac. Oncol. 2012, 7, 177–182. [Google Scholar] [CrossRef] [Green Version]
- Mehata, V. Radiation pneumonitis and pulmonary fibrosis in non-small-cell lung cancer: Pulmonary function, prediction, and prevention. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 5–24. [Google Scholar] [CrossRef]
- Memoli, J.S.W.; Nietert, P.J.; Silvestri, G.A. Meta-analysis of guided bronchoscopy for the evaluation of the pulmonary nodule. Chest 2012, 142, 385–393. [Google Scholar] [CrossRef] [Green Version]
- Tzouvelekis, A.; Spagnolo, P.; Bonella, F.; Vancheri, C.; Tzilas, V.; Crestani, B.; Kreuter, M.; Bouros, D. Patients with IPF and lung cancer: Diagnosis and management. Lancet Respir. Med. 2018, 6, 86–88. [Google Scholar] [CrossRef]
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F.; et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef] [PubMed]
- Kurimoto, N.; Miyazawa, T.; Okimasa, S.; Maeda, A.; Oiwa, H.; Miyazu, Y.; Murayama, M. Endobronchial ultrasonography using a guide sheath increases the ability to diagnose peripheral pulmonary lesions endoscopically. Chest 2004, 126, 959–965. [Google Scholar] [CrossRef] [Green Version]
- Guvenc, C.; Yserbyt, J.; Testelmans, D.; Zanca, F.; Carbonez, A.; Ninane, V.; De Wever, W.; Dooms, C. Computed tomography characteristics predictive for radial EBUS-miniprobe-guided diagnosis of pulmonary lesions. J. Thorac. Oncol. 2015, 10, 472–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, C.; Choi, C.M.; Chu, C.M.; Anantham, D.; Chung-Man Ho, J.; Khan, A.Z.; Lee, J.M.; Li, S.Y.; Saenghirunvattana, S.; Yim, A. Evaluation of Pulmonary Nodules: Clinical Practice Consensus Guidelines for Asia. Chest 2016, 150, 877–893. [Google Scholar] [CrossRef] [Green Version]
- Okachi, S.; Imai, N.; Imaizumi, K.; Iwano, S.; Ando, M.; Hase, T.; Aso, H.; Morise, M.; Wakahara, K.; Ito, S.; et al. Factors Affecting the Diagnostic Yield of Transbronchial Biopsy Using Endobronchial Ultrasonography with a Guide Sheath in Peripheral Lung Cancer. Intern. Med. 2016, 55, 1705–1712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, M.S.; Trick, W.; Mba, B.I.; Mohananey, D.; Sethi, J.; Musani, A.I. Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions: A systematic review and meta-analysis. Respirology 2017, 22, 443–453. [Google Scholar] [CrossRef] [Green Version]
- Meyer, K.C.; Raghu, G.; Baughman, R.P.; Brown, K.K.; Costabel, U.; du Bois, R.M.; Drent, M.; Haslam, P.L.; Kim, D.S.; Nagai, S.; et al. An official American Thoracic Society clinical practice guideline: The clinical utility of bronchoalveolar lavage cellular analysis in interstitial lung disease. Am. J. Respir. Crit. Care Med. 2012, 185, 1004–1014. [Google Scholar] [CrossRef]
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E., Jr.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Ando, M.; Kimura, T.; Kataoka, K.; Yokoyama, T.; Shiroshita, E.; Kondoh, Y. The impact of high-flow nasal cannula oxygen therapy on exercise capacity in fibrotic interstitial lung disease: A proof-of-concept randomized controlled crossover trial. BMC. Pulm. Med. 2020, 24, 51. [Google Scholar] [CrossRef]
- Park, J.; Kim, D.S.; Shim, T.S.; Lim, C.M.; Koh, Y.; Lee, S.D.; Kim, W.S.; Kim, W.D.; Lee, J.S.; Song, K.S. Lung cancer in patients with idiopathic pulmonary fibrosis. Eur. Respir. J. 2001, 17, 1216–1219. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, Y.; Izumo, T.; Sasada, S.; Tsuchida, T.; Ohe, Y. Diagnostic utility of endobronchial ultrasound with a guide sheath under the computed tomography workstation (ziostation) for small peripheral pulmonary lesions. Clin. Respir. J. 2017, 11, 185–192. [Google Scholar] [CrossRef]
- Callister, M.E.; Baldwin, D.R.; Akram, A.R.; Barnard, S.; Cane, P.; Draffan, J.; Franks, K.; Gleeson, F.; Graham, R.; Malhotra, P.; et al. British Thoracic Society guidelines for the investigation and management of pulmonary nodules. Thorax 2015, 70, ii1–ii54. [Google Scholar] [CrossRef] [Green Version]
- Gaeta, M.; Pandolfo, I.; Volta, S.; Russi, E.G.; Bartiromo, G.; Girone, G.; La Spada, F.; Barone, M.; Casablanca, G.; Minutoli, A. Bronchus sign on CT in peripheral carcinoma of the lung: Value in predicting results of transbronchial biopsy. AJR Am. J. Roentgenol. 1991, 157, 1181–1185. [Google Scholar] [CrossRef]
- MacMahon, H.; Naidich, D.P.; Goo, J.M.; Lee, K.S.; Leung, A.N.C.; Mayo, J.R.; Mehta, A.C.; Ohno, Y.; Powell, C.A.; Prokop, M.; et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017. Radiology 2017, 284, 228–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujita, J.; Yamadori, I.; Namihira, H.; Suemitsu, I.; Bandoh, S.; Fukunaga, Y.; Hojo, S.; Ueda, Y.; Dobashi, N.; Dohmoto, K.; et al. Increased intensity of lung infiltrates at the side of lung cancer in patients with lung cancer associated with pulmonary fibrosis. Lung Cancer 1999, 26, 169–174. [Google Scholar] [CrossRef]
- Kunimasa, K.; Tachihara, M.; Tamura, D.; Tokunaga, S.; Nakata, K.; Hazeki, N.; Kamiryo, H.; Kobayashi, K.; Sakai, Y.; Nishimura, Y. Diagnostic utility of additional conventional techniques after endobronchial ultrasonography guidance during transbronchial biopsy. Respirology 2016, 21, 1100–1105. [Google Scholar] [CrossRef]
- Tremblay, A.; Myers, R.; Beaudoin, E.L.; Bonifazi, M.; Delage, A.; Fortin, M.; Hergott, C.A.; MacEachern, P.R.; Shaipanich, T.; Shieh, B.; et al. Initial Clinical Experience With a Flexible Peripheral 21-G Needle Device. J. Bronchol. Interv. Pulmonol. 2018, 25, 346–348. [Google Scholar] [CrossRef]
- Naso, J.; Bras, J.; Villamil, C.; Ionescu, D.N.; Wang, G.; Shaipanich, T.; Beaudoin, E.L.; Myers, R.; Lam, S.; Zhou, C. Cytologic features and diagnostic value of PeriView FLEX transbronchial needle aspiration targeting pulmonary nodules. Cancer Cytopathol. 2020, 128, 333–340. [Google Scholar] [CrossRef]
- Sumi, T.; Shijubou, N.; Sawai, T.; Kamada, K.; Yamada, Y.; Nakata, H.; Mori, Y.; Chiba, H. Transbronchial needle aspiration with endobronchial ultrasonography and ultrathin bronchoscopy for peripheral pulmonary lesions. Respir. Investig. 2021, 59, 766–771. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.T.; Ho, C.C.; Tsai, Y.J.; Yu, C.J.; Yang, P.C. Factors influencing visibility and diagnostic yield of transbronchial biopsy using endobronchial ultrasound in peripheral pulmonary lesions. Respirology 2009, 14, 859–864. [Google Scholar] [CrossRef]
- Hayama, M.; Izumo, T.; Matsumoto, Y.; Chavez, C.; Tsuchida, T.; Sasada, S. Complications with Endobronchial Ultrasound with a Guide Sheath for the Diagnosis of Peripheral Pulmonary Lesions. Respiration 2015, 90, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Horinouchi, H.; Asano, F.; Okubo, K.; Okada, Y.; Ohsaki, Y.; Komase, Y.; Hashizume, T.; Kohno, M.; Aoe, M. Safety Management Committee of Japan Society for Respiratory Endoscopy, The 2016 National Survey Working Group. The Incidence of Hemorrhagic Complications was lower with the guide sheath than with the conventional forceps biopsy method: Results of Bronchoscopy in the 2016 Nationwide Survey by the Japan Society for Respiratory Endoscopy. J. Bronchol. Interv. Pulmonol 2020, 27, 253–258. [Google Scholar]
- Geraghty, P.R.; Kee, S.T.; McFarlane, G.; Razavi, M.K.; Sze, D.Y.; Dake, M.D. CT-guided transthoracic needle aspiration biopsy of pulmonary nodules: Needle size and pneumothorax rate. Radiology 2003, 229, 475–481. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | PPLs within or near Fibrotic Lesions n = 31 | PPLs Distant from Fibrotic Lesions n = 24 | p-Value |
|---|---|---|---|
| Age, years, median (range) | 71 (55–84) | 75 (58–84) | 0.028 |
| Sex, male, n (%) | 25 (80.6) | 17 (70.8) | 0.396 |
| Smoking history n (%) | 23 (74.2) | 9 (37.5) | 0.006 |
| Classification of ILD | <0.001 | ||
| IPF, n (%) | 17 (54.8) | 2 (8.3) | |
| Lesion size, mm, median (range) | 23 (9–39) | 23 (13–54) | 0.925 |
| Lesion lobe, n (%) | 0.832 | ||
| Right upper/left upper | 10 (32.2) | 9 (37.5) | |
| Right middle/lingula | 3 (9.7) | 3 (12.5) | |
| Right lower/left lower | 18 (58.1) | 12 (50) | |
| Lesion location, n (%) | 0.002 | ||
| Outer | 23 (74.2) | 8 (33.3) | |
| Lesion structure, n (%) | 0.188 | ||
| Solid | 27 (87.1) | 24 (100) | |
| Part-solid | 3 (9.7) | 0 (0) | |
| Pure ground-glass | 1 (3.2) | 0 (0) | |
| Bronchus sign, n (%) | 0.122 | ||
| Positive | 25 (80.6) | 23 (95.8) | - |
| FVC, percent predicted, %, median (range) | 100 (64–147) | 93 (38–130) | 0.317 |
| DLCO, percent predicted, %, median (range) | 71 (36–25) | 80 (43–133) | 0.302 |
| Visibility on chest X-ray, n (%) | 0.122 | ||
| Visible | 25 (80.6) | 23 (95.8) | |
| Number of biopsies, median (range) | 7.1 (3–14) | 6.8 (3–9) | 0.642 |
| Malignant lesions, n (%) | 24 (77.4) | 15 (62.5) | 0.227 |
| PPLs within or near Fibrotic Lesions n = 31 | PPLs Distant from Fibrotic Lesions n = 24 | p-Value | |
|---|---|---|---|
| EBUS image, n (%) | |||
| Within | 9/16 (56.3) | 12/12 (100) | 0.023 |
| Adjacent to | 2/6 (33.3) | 5/6 (83.3) | 0.242 |
| Invisible | 3/9 (33.3) | 3/6 (50) | 0.622 |
| Final diagnosis, n (%) | |||
| Malignant lesions | 10/24 (41.7) | 15/15 (100) | <0.001 |
| Benign lesions | 4/7 (57.1) | 5/9 (55.6) | 0.671 |
| Total | 14/31 (45.2) | 20/24 (83.3) | 0.004 |
| Variables | Reference | OR (95% CI) | p-Value |
|---|---|---|---|
| Positional relation to fibrotic lesions PPLs distant from fibrotic lesions (n = 24) | PPLs within or near fibrotic lesions (n = 31) | 7.509 (1.856–30.381) | 0.005 |
| Size ≤ 20 mm (n = 23) | >20 mm (n = 32) | 0.985 (0.266–3.642) | 0.982 |
| Location inner (n = 24) | outer (n = 31) | 1.239 (0.341–4.509) | 0.745 |
| Bronchus sign positive (n = 48) | negative (n = 7) | 0.950 (0.034–26.727) | 0.976 |
| EBUS image within (n = 28) | others (n = 27) | 4.172 (1.077–16.167) | 0.039 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ito, T.; Okachi, S.; Kimura, T.; Kataoka, K.; Suzuki, Y.; Kinoshita, F.; Wakahara, K.; Hashimoto, N.; Kondoh, Y. Endobronchial Ultrasonography with a Guide Sheath Transbronchial Biopsy for Diagnosing Peripheral Pulmonary Lesions within or near Fibrotic Lesions in Patients with Interstitial Lung Disease. Cancers 2021, 13, 5751. https://doi.org/10.3390/cancers13225751
Ito T, Okachi S, Kimura T, Kataoka K, Suzuki Y, Kinoshita F, Wakahara K, Hashimoto N, Kondoh Y. Endobronchial Ultrasonography with a Guide Sheath Transbronchial Biopsy for Diagnosing Peripheral Pulmonary Lesions within or near Fibrotic Lesions in Patients with Interstitial Lung Disease. Cancers. 2021; 13(22):5751. https://doi.org/10.3390/cancers13225751
Chicago/Turabian StyleIto, Takayasu, Shotaro Okachi, Tomoki Kimura, Kensuke Kataoka, Yasuhiko Suzuki, Fumie Kinoshita, Keiko Wakahara, Naozumi Hashimoto, and Yasuhiro Kondoh. 2021. "Endobronchial Ultrasonography with a Guide Sheath Transbronchial Biopsy for Diagnosing Peripheral Pulmonary Lesions within or near Fibrotic Lesions in Patients with Interstitial Lung Disease" Cancers 13, no. 22: 5751. https://doi.org/10.3390/cancers13225751