
Development and Validation of an Efficient MRI Radiomics Signature for Improving the Predictive Performance of 1p/19q Co-Deletion in Lower-Grade Gliomas



Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Baseline Comparison among Different Machine Learning Algorithms and Selecting the Baseline Machine Learning Model
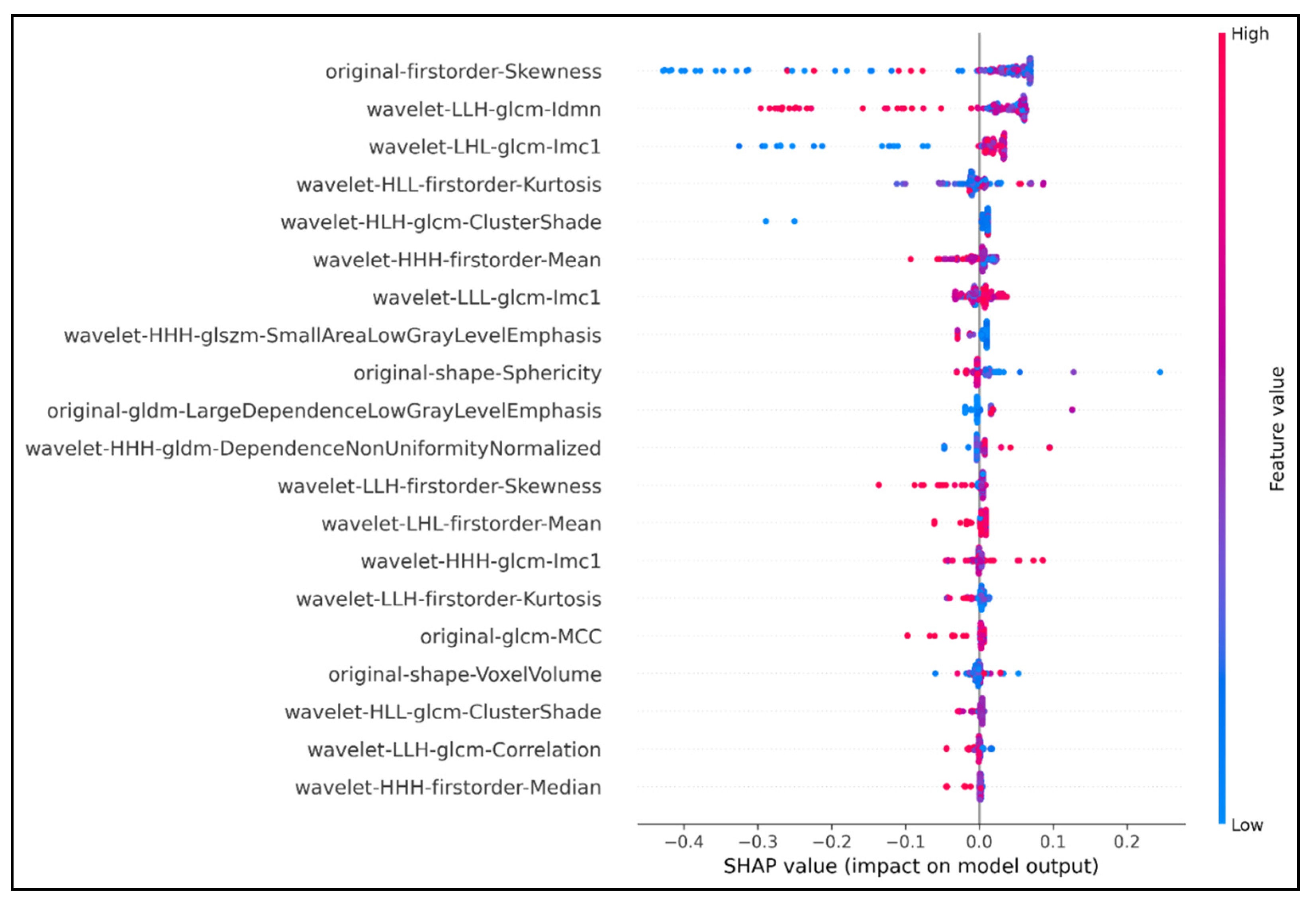
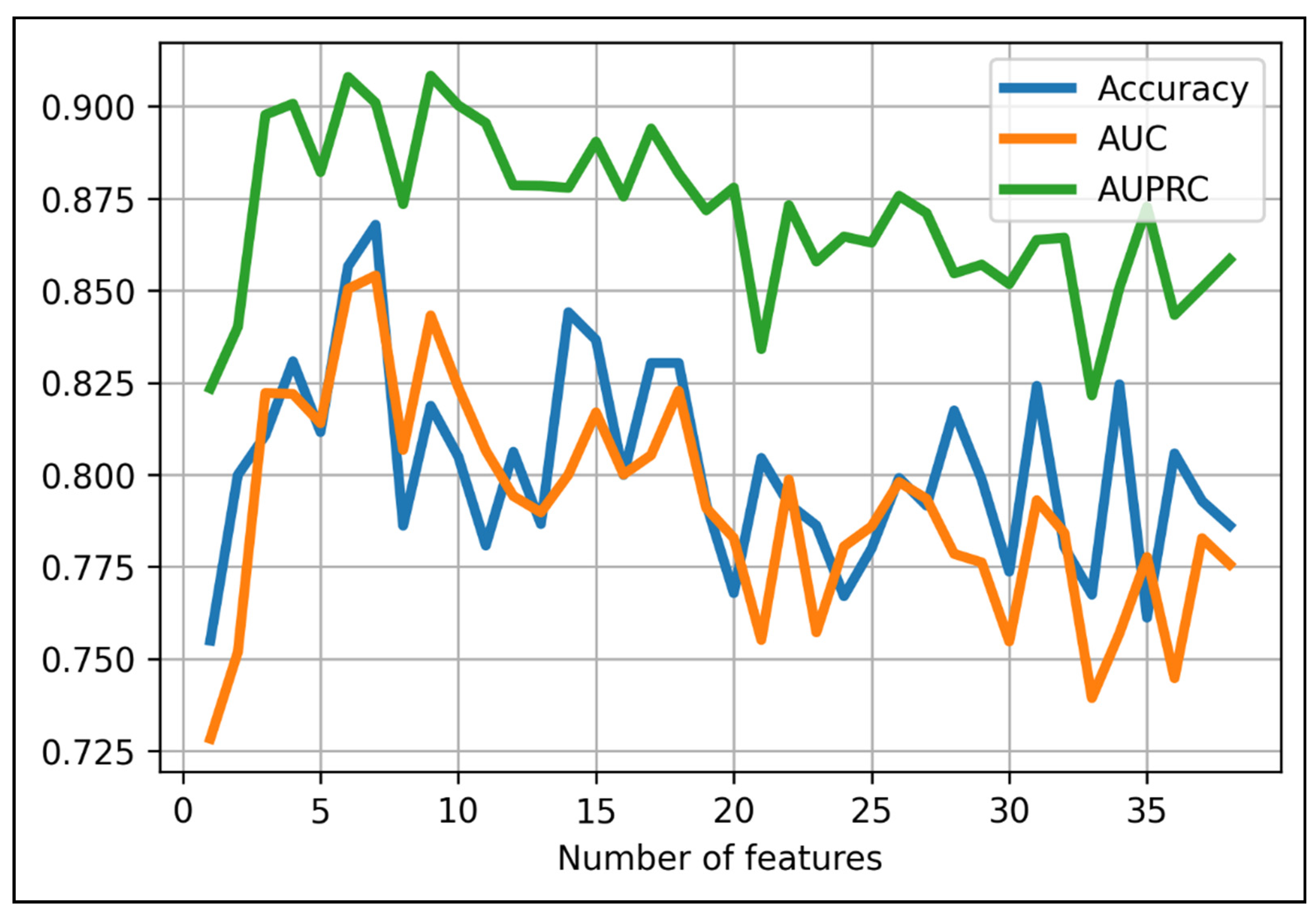
2.2. Radiomics Signature Building
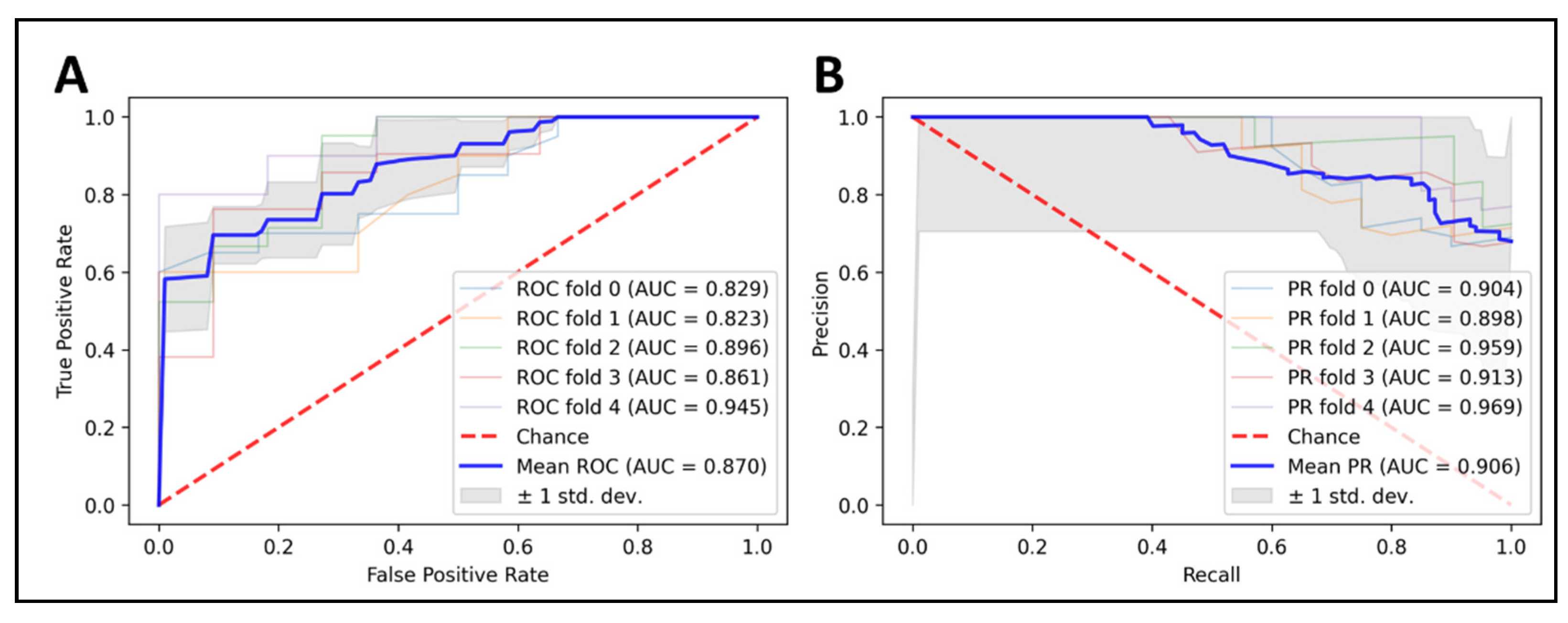
2.3. Model Ensembling and Predictions on the Training Set
2.4. Comparison with Previous Studies on 1p/19q Status Prediction
2.5. Performance Results on the External Test Set
2.6. Performance Results of Our Radiomics Model on Different Patient Subgroups
3. Discussion
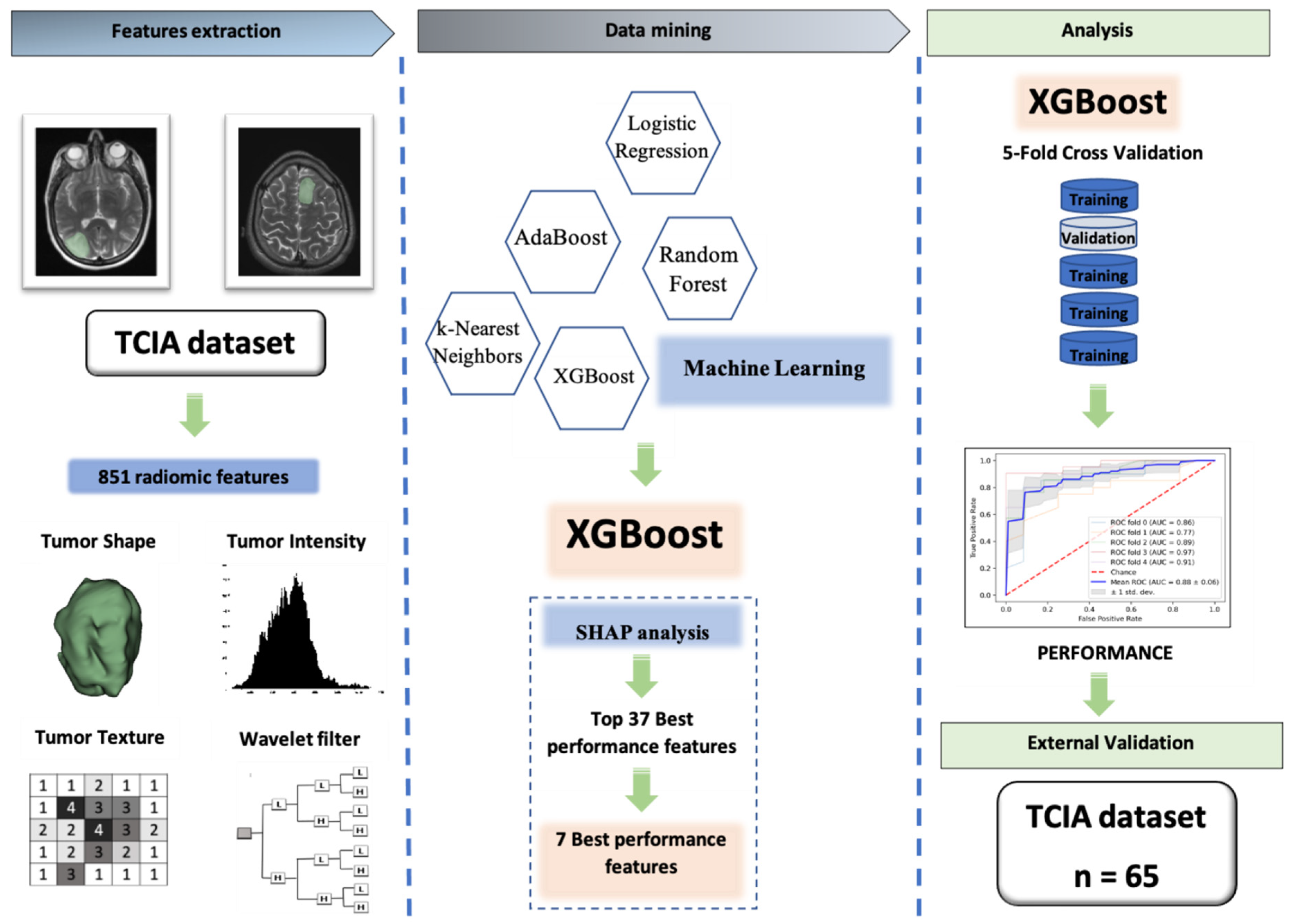
4. Materials and Methods
4.1. Patient Cohort
4.2. Feature Extraction
4.3. Data Mining
4.3.1. Determining the Ground-Truth Labels
4.3.2. Select the Baseline Machine Learning Models
LR
kNN
RF
AdaBoost
XGBoost
4.4. Handling the Imbalance between Two Classes and Features Selection Using the Spearman’s Correlation Coefficient (SCC) and SHAP Analysis
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patel, A.P.; Fisher, J.M.; Nichols, E.; Abdela, J.; Abdelalim, A.; Abraha, H.N.; Agius, D.; Alahdab, F.; Alam, T.; Allen, C.A. Global, regional, and national burden of brain and other CNS cancer, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 376–393. [Google Scholar] [CrossRef] [Green Version]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Cuccarini, V.; Erbetta, A.; Farinotti, M.; Cuppini, L.; Ghielmetti, F.; Pollo, B.; DiMeco, F.; Grisoli, M.; Filippini, G.; Finocchiaro, G.; et al. Advanced MRI may complement histological diagnosis of lower grade gliomas and help in predicting survival. J. Neuro-Oncol. 2015, 126, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Goyal, A. Erratum. The T2-FLAIR–mismatch sign as an imaging biomarker for IDH and 1p/19q status in diffuse low-grade gliomas: A systematic review with a Bayesian approach to evaluation of diagnostic test performance. Neurosurg. Focus 2020, 48, E10. [Google Scholar] [CrossRef]
- Yogananda, C.G.B.; Yogananda, C.; Shah, B.R.; Yu, F.F.; Pinho, M.C.; Nalawade, S.S.; Murugesan, G.K.; Wagner, B.C.; Mickey, B.; Patel, T.R.; et al. A novel fully automated MRI-based deep-learning method for classification of 1p/19q co-deletion status in brain gliomas. Neurooncol. Adv. 2020, 2, vdaa066. [Google Scholar] [PubMed]
- Forst, D.A.; Nahed, B.V.; Loeffler, J.S.; Batchelor, T.T. Low-grade gliomas. Oncologist 2014, 19, 403–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanai, N.; Chang, S.; Berger, M.S. Low-grade gliomas in adults: A review. J. Neurosurg. 2011, 115, 948–965. [Google Scholar] [CrossRef]
- Ruiz, J.; Lesser, G.J. Low-grade gliomas. Curr. Treat. Options Oncol. 2009, 10, 231–242. [Google Scholar] [CrossRef]
- Franceschi, E.; Mura, A.; De Biase, D.; Tallini, G.; Pession, A.; Foschini, M.P.; Danieli, D.; Pizzolitto, S.; Zunarelli, E.; Lanza, G.; et al. The role of clinical and molecular factors in low-grade gliomas: What is their impact on survival? Future Oncol. 2018, 14, 1559–1567. [Google Scholar] [CrossRef]
- Akkus, Z.; Ali, I.; Sedlář, J.; Agrawal, J.P.; Parney, I.F.; Giannini, C.; Erickson, B.J. Predicting deletion of chromosomal arms 1p/19q in low-grade gliomas from MR images using machine intel-ligence. J. Digit. Imaging 2017, 30, 469–476. [Google Scholar] [CrossRef] [Green Version]
- Garcia, C.R.; Slone, S.A.; Pittman, T.; Clair, W.H.S.; Lightner, D.D.; Villano, J.L. Comprehensive evaluation of treatment and outcomes of low-grade diffuse gliomas. PLoS ONE 2018, 13, e0203639. [Google Scholar] [CrossRef] [PubMed]
- Ricard, D.; Kaloshi, G.; Amiel-Benouaich, A.; Lejeune, J.; Marie, Y.; Mandonnet, E.; Kujas, M.; Mokhtari, K.; Taillibert, S.; Laigle-Donadey, F.; et al. Dynamic history of low-grade gliomas before and after temozolomide treatment. Ann. Neurol. 2007, 61, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Bent, M.J.V.D.; Brandes, A.; Taphoorn, M.J.B.; Kros, J.M.; Kouwenhoven, M.; Delattre, J.-Y.; Bernsen, H.J.J.A.; Frenay, M.; Tijssen, C.C.; Grisold, W.; et al. Adjuvant Procarbazine, Lomustine, and Vincristine Chemotherapy in Newly Diagnosed Anaplastic Oligodendroglioma: Long-Term Follow-Up of EORTC Brain Tumor Group Study 26951. J. Clin. Oncol. 2013, 31, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Riche, M.; Amelot, A.; Peyre, M.; Capelle, L.; Carpentier, A.; Mathon, B. Complications after frame-based stereotactic brain biopsy: A systematic review. Neurosurg. Rev. 2020, 44, 301–307. [Google Scholar] [CrossRef]
- Malone, H.; Yang, J.; Hershman, D.L.; Wright, J.D.; Bruce, J.N.; Neugut, A.I. Complications Following Stereotactic Needle Biopsy of Intracranial Tumors. World Neurosurg. 2015, 84, 1084–1089. [Google Scholar] [CrossRef]
- Pouratian, N.; Schiff, D. Management of Low-Grade Glioma. Curr. Neurol. Neurosci. Rep. 2010, 10, 224–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillies, R.J.; Kinahan, P.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaddad, A.; Kucharczyk, M.; Daniel, P.; Sabri, S.; Jean-Claude, B.J.; Niazi, T.; Abdulkarim, B. Radiomics in Glioblastoma: Current Status and Challenges Facing Clinical Implementation. Front. Oncol. 2019, 9, 374. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Ou, X.; Wang, J.; Guo, W.; Ma, X. Radiomics-Based Machine Learning in Differentiation Between Glioblastoma and Metastatic Brain Tumors. Front. Oncol. 2019, 9, 806. [Google Scholar] [CrossRef] [Green Version]
- Lee, G.; Lee, H.Y.; Park, H.; Schiebler, M.; van Beek, E.J.; Ohno, Y.; Seo, J.B.; Leung, A. Radiomics and its emerging role in lung cancer research, imaging biomarkers and clinical management: State of the art. Eur. J. Radiol. 2016, 86, 297–307. [Google Scholar] [CrossRef]
- Narang, S.; Lehrer, M.; Yang, D.; Lee, J.; Rao, A. Radiomics in glioblastoma: Current status, challenges and potential opportunities. Transl. Cancer Res. 2016, 5, 383–397. [Google Scholar] [CrossRef]
- Rafique, R.; Islam, S.R.; Kazi, J.U. Machine learning in the prediction of cancer therapy. Comput. Struct. Biotechnol. J. 2021, 19, 4003–4017. [Google Scholar] [CrossRef]
- Huang, C.; Clayton, E.A.; Matyunina, L.V.; McDonald, L.D.; Benigno, B.B.; Vannberg, F.; McDonald, J.F. Machine learning predicts individual cancer patient responses to therapeutic drugs with high accuracy. Sci. Rep. 2018, 8, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, M.J.; Javed, Z.; Sadia, H.; Qureshi, I.A.; Irshad, A.; Ahmed, R.; Malik, K.; Raza, S.; Abbas, A.; Pezzani, R.; et al. Clinical applications of artificial intelligence and machine learning in cancer diagnosis: Looking into the future. Cancer Cell Int. 2021, 21, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.-F.; Hsu, F.-T.; Hsieh, K.L.-C.; Kao, Y.-C.J.; Cheng, S.-J.; Hsu, J.B.-K.; Tsai, P.-H.; Chen, R.-J.; Huang, C.-C.; Yen, Y.; et al. Machine Learning–Based Radiomics for Molecular Subtyping of Gliomas. Clin. Cancer Res. 2018, 24, 4429–4436. [Google Scholar] [CrossRef] [Green Version]
- Akkus, Z.; Sedlar, J.; Coufalova, L.; Korfiatis, P.; Kline, T.L.; Warner, J.D.; Agrawal, J.; Erickson, B.J. Semi-automated segmentation of pre-operative low grade gliomas in magnetic resonance imaging. Cancer Imaging 2015, 15, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Kocak, B.; Durmaz, E.S.; Ates, E.; Sel, I.; Gunes, S.T.; Kaya, O.K.; Zeynalova, A.; Kilickesmez, O. Radiogenomics of lower-grade gliomas: Machine learning–based MRI texture analysis for predicting 1p/19q codeletion status. Eur. Radiol. 2019, 30, 877–886. [Google Scholar] [CrossRef] [PubMed]
- Matsui, Y.; Maruyama, T.; Nitta, M.; Saito, T.; Tsuzuki, S.; Tamura, M.; Kusuda, K.; Fukuya, Y.; Asano, H.; Kawamata, T.; et al. Prediction of lower-grade glioma molecular subtypes using deep learning. J. Neuro-Oncol. 2019, 146, 321–327. [Google Scholar] [CrossRef]
- Aliotta, E.; Dutta, S.W.; Feng, X.; Tustison, N.J.; Batchala, P.P.; Schiff, D.; Lopes, M.B.; Jain, R.; Druzgal, T.J.; Mukherjee, S.; et al. Automated apparent diffusion coefficient analysis for genotype prediction in lower grade glioma: Association with the T2-FLAIR mismatch sign. J. Neuro-Oncol. 2020, 149, 1–11. [Google Scholar] [CrossRef]
- Rathore, S.; Mohan, S.; Bakas, S.; Sako, C.; Badve, C.; Pati, S.; Singh, A.; Bounias, D.; Ngo, P.; Akbari, H.; et al. Multi-institutional noninvasive in vivo characterization of IDH, 1p/19q, and EGFRvIII in glioma using neuro-Cancer Imaging Phenomics Toolkit (neuro-CaPTk). Neurooncol. Adv. 2020, 2, iv22–iv34. [Google Scholar]
- Batchala, P.; Muttikkal, T.; Donahue, J.; Patrie, J.; Schiff, D.; Fadul, C.; Mrachek, E.; Lopes, M.-B.; Jain, R.; Patel, S. Neuroimaging-Based Classification Algorithm for Predicting 1p/19q-Codeletion Status in IDH-Mutant Lower Grade Gliomas. Am. J. Neuroradiol. 2019, 40, 426–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.; Wang, N.; Ravikumar, V.; Raghuram, D.R.; Li, J.; Patel, A.; Wendt, R.E., 3rd; Rao, G.; Rao, A. Prediction of 1p/19q codeletion in diffuse glioma patients using pre-operative multiparametric magnetic reso-nance imaging. Front. Comput. Neurosci. 2019, 13, 52. [Google Scholar] [CrossRef] [Green Version]
- Shboul, Z.A.; Chen, J.; Iftekharuddin, K.M. Prediction of Molecular Mutations in Diffuse Low-Grade Gliomas using MR Imaging Features. Sci. Rep. 2020, 10, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Bakas, S.; Akbari, H.; Sotiras, A.; Bilello, M.; Rozycki, M.; Kirby, J.; Freymann, J.B.; Farahani, K.; Davatzikos, C. Advancing the Cancer Genome Atlas glioma MRI collections with expert segmentation labels and radiomic features. Sci. Data 2017, 4, 170117. [Google Scholar] [CrossRef] [Green Version]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [Green Version]
- Chawla, N.V.; Bowyer, K.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic Minority Over-sampling Technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Lundberg, S.M.; Lee, S.-I. A unified approach to interpreting model predictions. In Proceedings of the 31st International Conference on Neural Information Processing Systems, Long Beach, CA, USA, 4–9 December 2017. [Google Scholar]
- Spearman Rank Correlation Coefficient. In The Concise Encyclopedia of Statistics; Springer: New York, NY, USA, 2008; pp. 502–505.
- van der Voort, S.R.; Incekara, F.; Wijnenga, M.; Kapas, G.; Gardeniers, M.; Schouten, J.W.; Starmans, M.; Nandoe Tewarie, R.; Lycklama, G.J.; French, P.J.; et al. Predicting the 1p/19q codeletion status of presumed low-grade glioma with an externally validated machine learning algorithm. Clin. Cancer Res. 2019, 25, 7455–7462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rundo, L.; Militello, C.; Russo, G.; Vitabile, S.; Gilardi, M.C.; Mauri, G. GTV cut for neuro-radiosurgery treatment planning: An MRI brain cancer seeded image segmentation method based on a cellular automata model. Nat. Comput. 2018, 17, 521–536. [Google Scholar] [CrossRef]
- Pereira, S.; Pinto, J.A.A.D.S.R.; Alves, V.; Silva, C. Brain Tumor Segmentation Using Convolutional Neural Networks in MRI Images. IEEE Trans. Med. Imaging 2016, 35, 1240–1251. [Google Scholar] [CrossRef]
- Chaddad, A.; Daniel, P.; Niazi, T. Radiomics Evaluation of Histological Heterogeneity Using Multiscale Textures Derived From 3D Wavelet Transformation of Multispectral Images. Front. Oncol. 2018, 8, 96. [Google Scholar] [CrossRef]
- Dettori, L.; Semler, L. A comparison of wavelet, ridgelet, and curvelet-based texture classification algorithms in computed tomography. Comput. Biol. Med. 2007, 37, 486–498. [Google Scholar] [CrossRef] [PubMed]
- Weyn, B.; van de Wouwer, G.; Scheunders, P.; van Dyck, D.; van Marck, E.; Jacob, W. Automated breast tumor diagnosis and grading based on wavelet chromatin texture description. Cytometry 1998, 33, 32–40. [Google Scholar] [CrossRef]
- Thongsuwan, S.; Jaiyen, S.; Padcharoen, A.; Agarwal, P. ConvXGB: A new deep learning model for classification problems based on CNN and XGBoost. Nucl. Eng. Technol. 2020, 53, 522–531. [Google Scholar] [CrossRef]
- Wang, C.; Deng, C.; Wang, S. Imbalance-XGBoost: Leveraging weighted and focal losses for binary label-imbalanced classification with XGBoost. Pattern Recognit. Lett. 2020, 136, 190–197. [Google Scholar] [CrossRef]
- Le, N.Q.K.; Huynh, T.-T. Identifying SNAREs by Incorporating Deep Learning Architecture and Amino Acid Embedding Representation. Front. Physiol. 2019, 10. [Google Scholar] [CrossRef]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M.; et al. The Cancer Imaging Archive (TCIA): Maintaining and Operating a Public Information Repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Griethuysen, J.J.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [Green Version]
- Herz, C.; Fillion-Robin, J.-C.; Onken, M.; Riesmeier, J.; Lasso, A.; Pinter, C.; Fichtinger, G.; Pieper, S.; Clunie, D.; Kikinis, R.; et al. dcmqi: An Open Source Library for Standardized Communication of Quantitative Image Analysis Results Using DICOM. Cancer Res. 2017, 77, e87–e90. [Google Scholar] [CrossRef] [Green Version]
- Ulrich, E.; Fedorov, A. 3D Slicer PET-DICOM Extension Documentation. 2017. Available online: https://www.slicer.org/wiki/Documentation/4.6/Extensions/PETDICOM (accessed on 20 March 2021).
- Pinter, C.; Lasso, A.; Wang, A.; Jaffray, D.; Fichtinger, G. SlicerRT: Radiation therapy research toolkit for 3D Slicer. Med. Phys. 2012, 39, 6332–6338. [Google Scholar] [CrossRef]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fix, E.; Hodges, J.L. Nonparametric discrimination: Consistency properties. Randolph Field Tex. Proj. 1951, 21–49. [Google Scholar] [CrossRef]
- Kozma, L. k Nearest Neighbors Algorithm (kNN). 2008. Available online: http://www.lkozma.net/knn2.pdf (accessed on 20 March 2021).
- Pal, M. Random forest classifier for remote sensing classification. Int. J. Remote. Sens. 2005, 26, 217–222. [Google Scholar] [CrossRef]
- Le, N.Q.K.; Kha, Q.H.; Nguyen, V.H.; Chen, Y.-C.; Cheng, S.-J.; Chen, C.-Y. Machine Learning-Based Radiomics Signatures for EGFR and KRAS Mutations Prediction in Non-Small-Cell Lung Cancer. Int. J. Mol. Sci. 2021, 22, 9254. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | Algorithm | Sensitivity | Specificity | Precision | Accuracy | AUC | AUPRC |
|---|---|---|---|---|---|---|---|
| All features | Logistic Regression | 61.75 ± 5.17 | 32.26 ± 6.69 | 50.19 ± 9.31 | 47.80 ± 5.38 | 0.510 ± 0.095 | 0.687 ± 0.064 |
| k-Nearest Neighbors | 56.20 ± 3.87 | 27.97 ± 3.46 | 44.19 ± 4.98 | 42.16 ± 3.93 | 0.434 ± 0.065 | 0.607 ± 0.027 | |
| Random Forest | 72.13 ± 3.07 | 57.88 ± 7.77 | 79.48 ± 12.34 | 66.67 ± 3.09 | 0.685 ± 0.061 | 0.799 ± 0.040 | |
| AdaBoost | 68.47 ± 7.31 | 47.03 ± 15.80 | 71.33 ± 11.39 | 60.99 ± 10.44 | 0.599 ± 0.082 | 0.740 ± 0.051 | |
| XGBoost | 73.16 ± 2.84 | 61.51 ± 12.25 | 81.19 ± 9.83 | 69.17 ± 6.09 | 0.710 ± 0.079 | 0.827 ± 0.057 | |
| 37 features | Logistic Regression | 64.95 ± 12.05 | 35.71 ± 6.79 | 44.10 ± 8.15 | 48.49 ± 8.20 | 0.587 ± 0.106 | 0.706 ± 0.091 |
| k-Nearest Neighbors | 69.82 ± 8.04 | 42.83 ± 13.25 | 62.86 ± 8.61 | 58.55 ± 9.76 | 0.590 ± 0.116 | 0.720 ± 0.077 | |
| Random Forest | 74.10 ± 7.60 | 54.16 ± 10.94 | 75.29 ± 11.18 | 66.61 ± 7.57 | 0.713 ± 0.078 | 0.858 ± 0.041 | |
| AdaBoost | 71.80 ± 7.50 | 46.67 ± 6.67 | 70.67 ± 7.94 | 62.28 ± 4.72 | 0.632 ± 0.099 | 0.755 ± 0.090 | |
| XGBoost | 77.89 ± 5.75 | 55.85 ± 7.46 | 73.52 ± 3.96 | 69.21 ± 4.83 | 0.753 ± 0.058 | 0.809 ± 0.045 |
| Form | Type | Matrix | Name |
|---|---|---|---|
| original | First Order | Skewness | |
| Wavelet | LLH | GLCM | Inverse Difference Moment Normalized (IDMN) |
| Wavelet | LHL | GLCM | Informational Measure of Correlation 1 (IMC1) |
| Wavelet | HLL | First Order | Kurtosis |
| Wavelet | HLH | GLCM | Cluster Shade |
| Wavelet | HHH | First Order | Mean |
| Wavelet | LLL | GLCM | IMC1 |
| Study | Algorithm | Dataset | Accuracy | Sensitivity | Specificity | AUC |
|---|---|---|---|---|---|---|
| van der Voort et al. | SVM | LGG 284 | 69.8 | 65.7 | 72.1 | 0.755 |
| LGG 108 [39] | 69.3 | 73.2 | 61.7 | 0.723 | ||
| Yogananda et al. | Deep learning | LGG 268 [5] | 93.5 | 0.9 | 95 | 95.3 |
| Akkus et al. | CNN | LGG 159 [10] | 87.7 | 93.3 | 82.2 | - |
| Shboul et al. | XGBoost | LGG 81 | - | 78 | 83 | 0.83 |
| LGG 23 [33] | - | 75 | 85 | 0.8 | ||
| Ours | XGBoost | LGG 159 [10] | 87.0 | 88.2 | 77.2 | 0.87 |
| Subtype | Training Data | External Validation Data | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Acc | Sens | Spec | AUC | AUPRC | Acc | Sens | Spec | AUC | AUPRC | ||
| Grade | 2 | 83.7 ± 11.7 | 87.9 ± 6.6 | 76.3 ± 22.4 | 0.876 ± 0.11 | 0.891 ± 0.07 | 82.1 | 16.7 | 100.0 | 0.695 | 0.855 |
| 3 | 80 ± 15.1 | 97.2 ± 25.9 | 47.4 ± 4.1 | 0.759 ± 0.20 | 0.815 ± 0.13 | 88.6 | 50.0 | 96.6 | 0.847 | 0.885 | |
| Type | Astrocytoma | 76.5 ± 8.6 | 25 ± 9.0 | 92.3 ± 11.9 | 0.85 ± 0.09 | 0.785 ± 0.078 | - | - | - | - | - |
| Oligoastrocytoma | 80.4 ± 2.0 | 82.1 ± 0.9 | 78 ± 4.0 | 0.836 ± 0.04 | 0.858 ± 0.05 | - | - | - | - | - | |
| Oligodendroglioma | 93.3 ± 6.9 | 100.0 ± 0 | 0.0 ± 0 | 0.726 ± 0.07 | 0.864 ± 0.05 | 64.0 | 58.3 | 69.2 | 0.733 | 0.828 | |
| Feature | Subtype | Training Cohort | External Test Cohort | ||
|---|---|---|---|---|---|
| d/d (n = 102) | n/n (n = 57) | d/d (n = 13) | n/n (n = 52) | ||
| Grade | 2 | 66 (64.7%) | 38 (66.7%) | 6 (46.2%) | 22 (42.3%) |
| 3 | 36 (35.3%) | 19 (33.3%) | 7 (53.8%) | 30 (57.7%) | |
| Type | Astrocytoma | 4 (3.9%) | 13 (22.8%) | 0 (0%) | 21 (40.4%) |
| Oligoastrocytoma | 56 (54.9%) | 41 (71.9%) | 0 (0%) | 18 (34.6%) | |
| Oligodendroglioma | 42 (41.2%) | 3 (5.3%) | 13 (100%) | 13 (25%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kha, Q.-H.; Le, V.-H.; Hung, T.N.K.; Le, N.Q.K. Development and Validation of an Efficient MRI Radiomics Signature for Improving the Predictive Performance of 1p/19q Co-Deletion in Lower-Grade Gliomas. Cancers 2021, 13, 5398. https://doi.org/10.3390/cancers13215398
Kha Q-H, Le V-H, Hung TNK, Le NQK. Development and Validation of an Efficient MRI Radiomics Signature for Improving the Predictive Performance of 1p/19q Co-Deletion in Lower-Grade Gliomas. Cancers. 2021; 13(21):5398. https://doi.org/10.3390/cancers13215398
Chicago/Turabian StyleKha, Quang-Hien, Viet-Huan Le, Truong Nguyen Khanh Hung, and Nguyen Quoc Khanh Le. 2021. "Development and Validation of an Efficient MRI Radiomics Signature for Improving the Predictive Performance of 1p/19q Co-Deletion in Lower-Grade Gliomas" Cancers 13, no. 21: 5398. https://doi.org/10.3390/cancers13215398