
A Tissue Section-Based Near-Infrared Spectroscopical Analysis of Salivary Gland Tumors

 , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Preparation of Tissue Sections
2.3. Histological Classification
2.4. NIR Spectroscopical Analysis
2.5. Neuraminidase Treatment of Tissue Sections
2.6. Data Analysis
2.6.1. Data Preprocessing
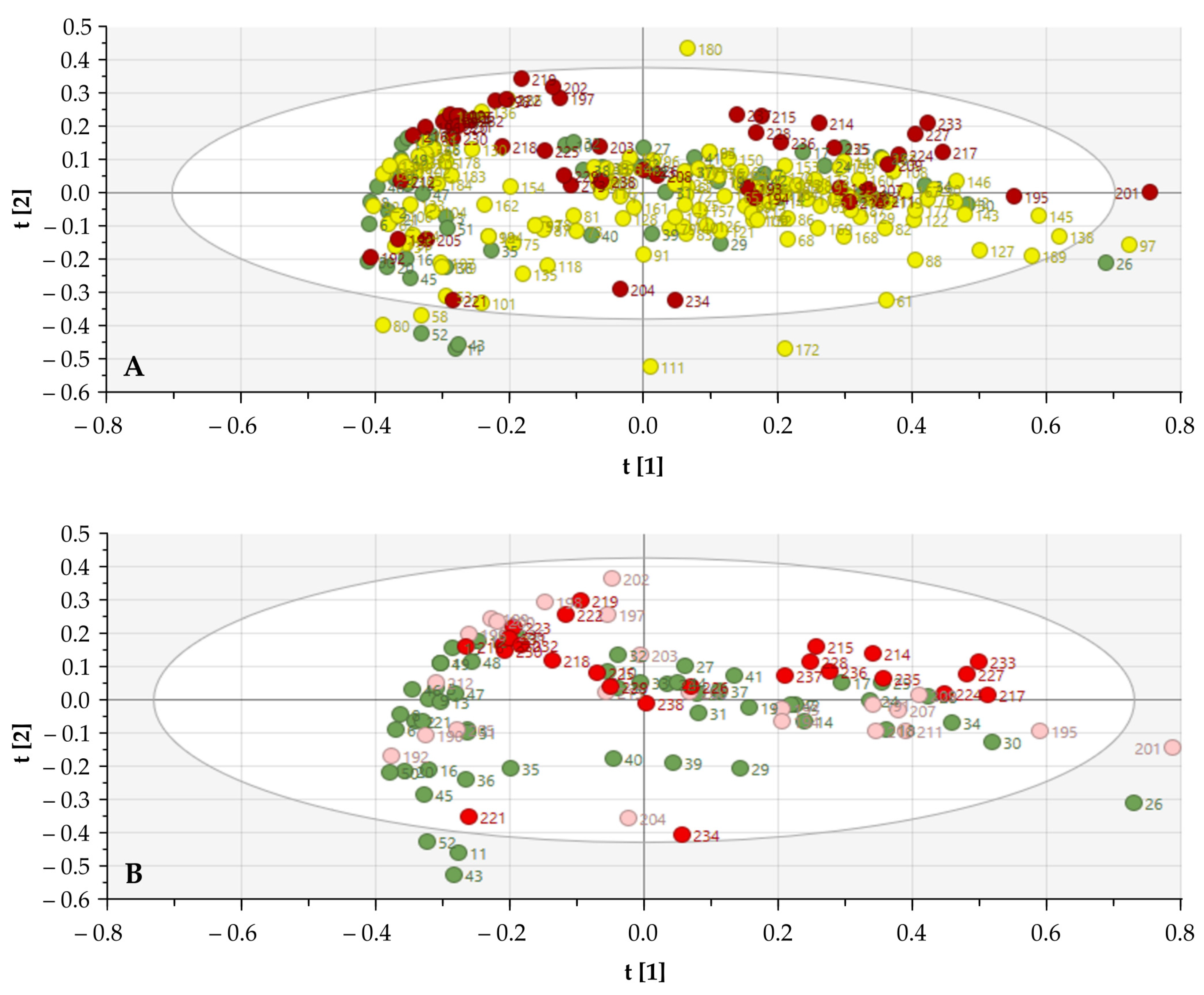
2.6.2. Principal Component Analysis (PCA)
2.6.3. Soft Independent Modelling of Class Analogy (SIMCA)
2.7. Statistical Analysis
3. Results
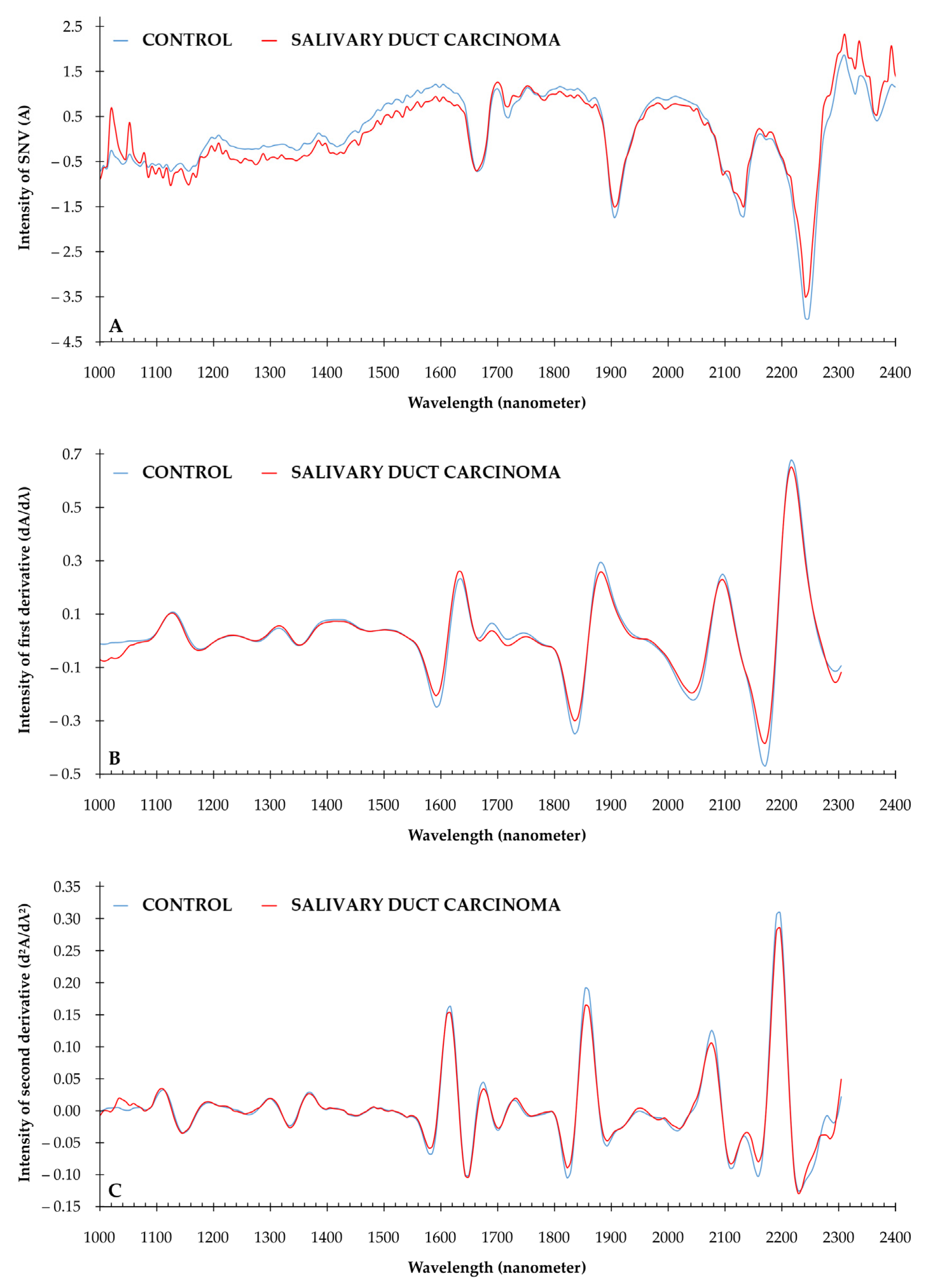
3.1. Descriptive Spectral Analysis of SGTs
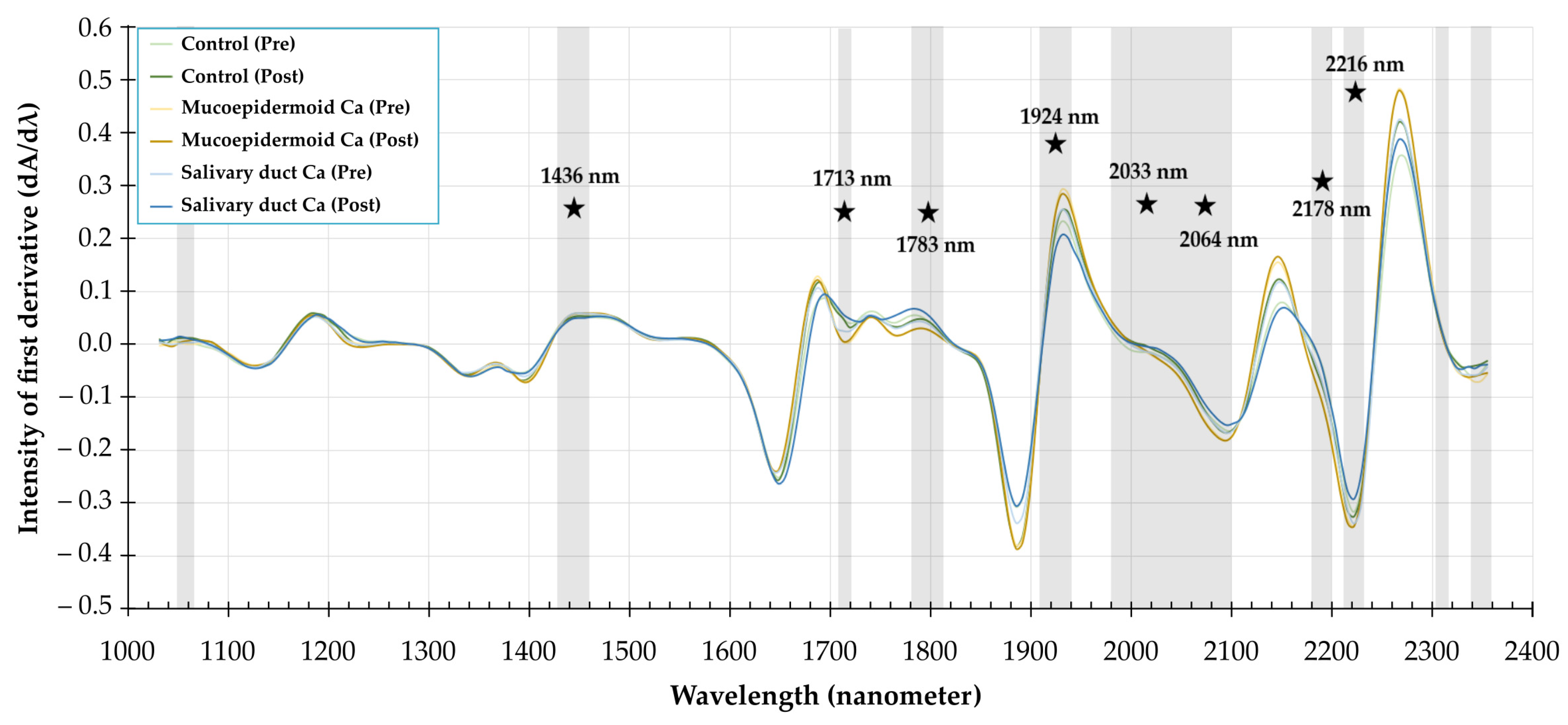
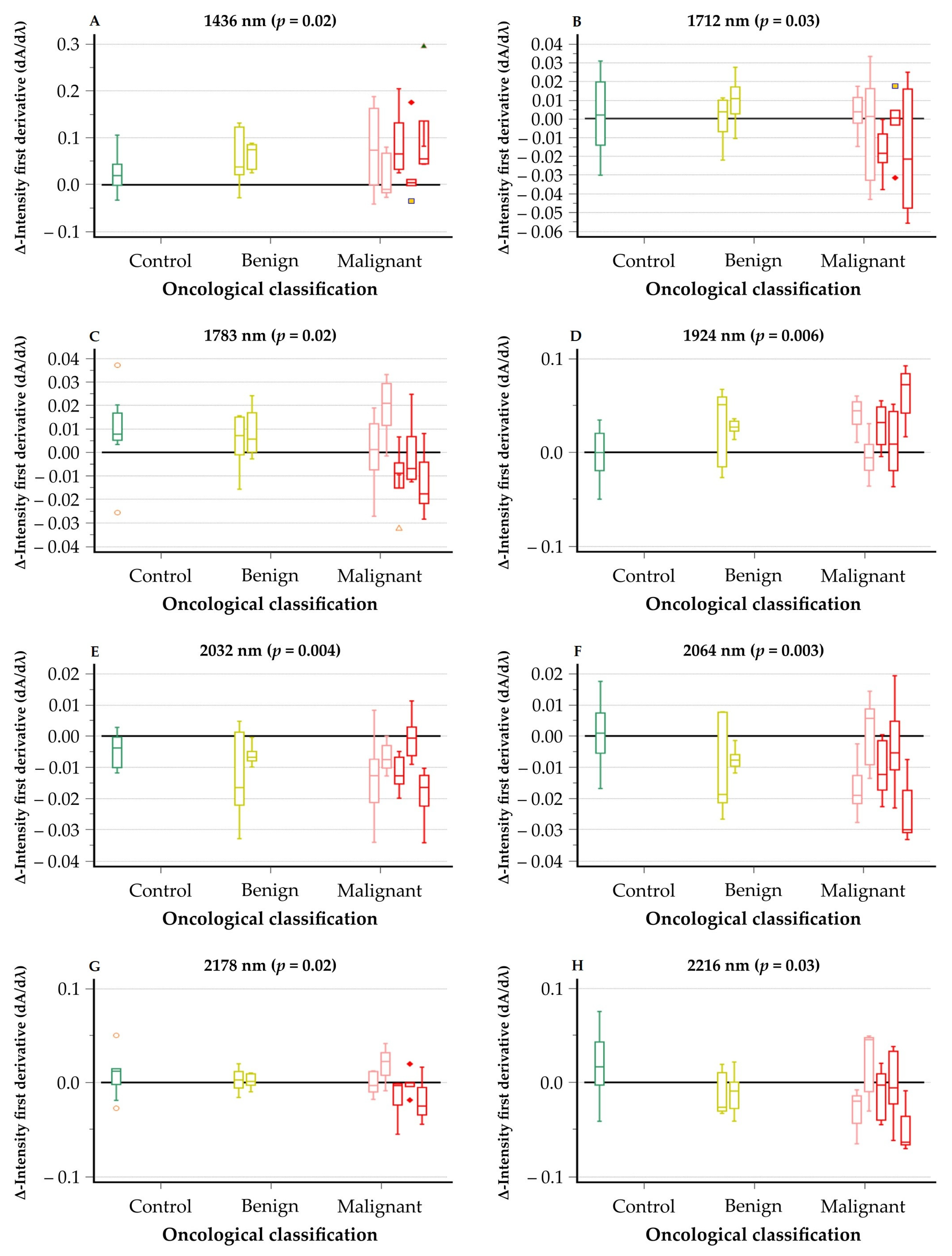
3.2. Neuraminidase Treatment of Tissue Sections—Spectral Analysis
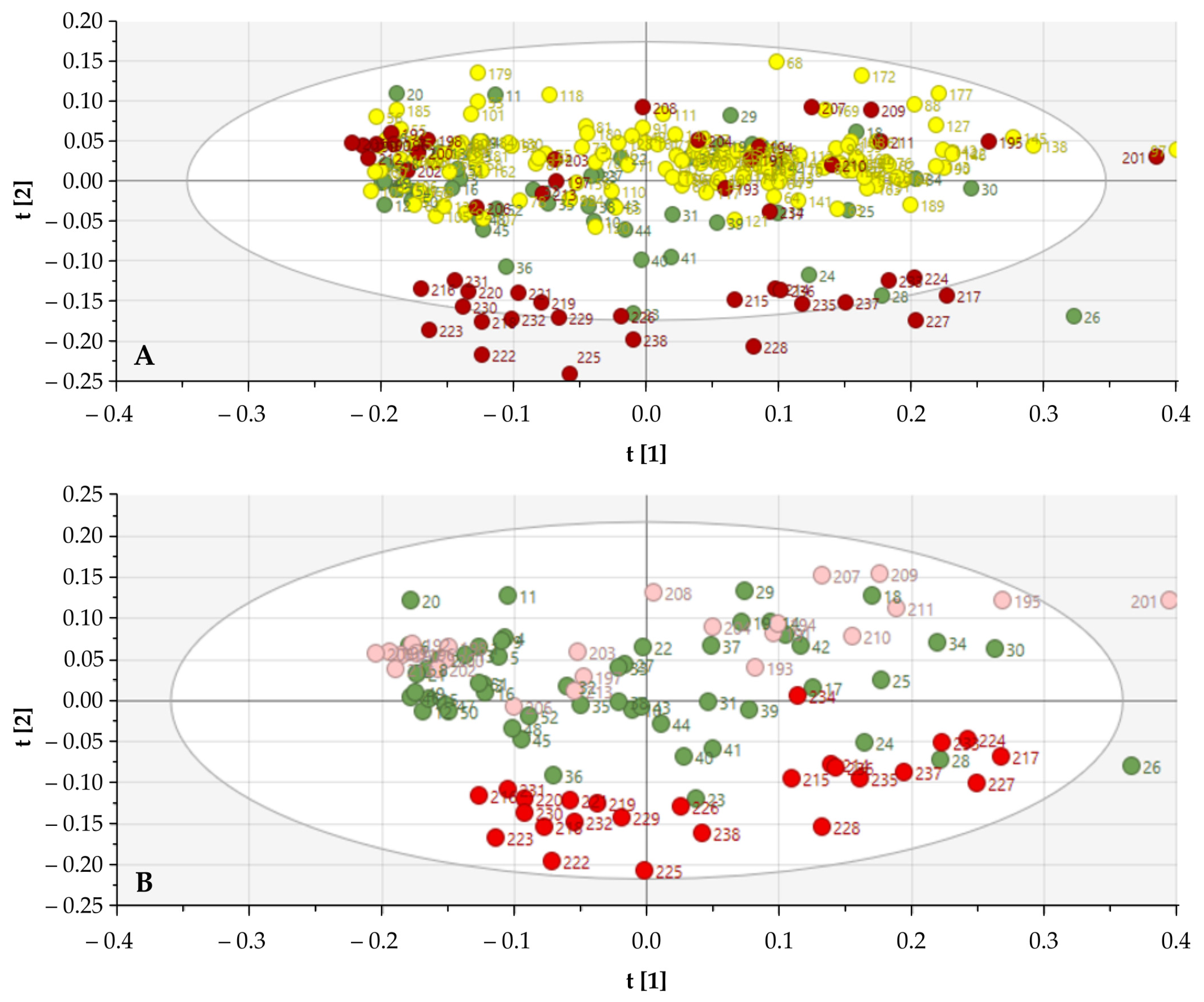
3.3. Discriminative Power of the Biochemical Signature
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- El-Naggar, A.K.; Grandis, J.R.; Takata, T.; Grandis, J.; Slootweg, P. Tumours of Salivary Glands. In WHO Classification of Head and Neck Tumours; International Agency for Research on Cancer: Lyon, France, 2017; ISBN 978-92-832-2438-9. [Google Scholar]
- Sood, S.; McGurk, M.; Vaz, F. Management of Salivary Gland Tumours: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S142–S149. [Google Scholar] [CrossRef] [PubMed]
- Speight, P.M.; Barrett, A.W. Salivary gland tumours: Diagnostic challenges and an update on the latest WHO classification. Diagnostic Histopathol. 2020, 26, 147–158. [Google Scholar] [CrossRef]
- Hellquist, H.; Skalova, A. Histopathology of the Salivary Glands; Springer Publishing: New York, NY, USA, 2014; ISBN 9783540469155. [Google Scholar]
- Kim, Y.J.; Varki, A. Perspectives on the significance of altered glycosylation of glycoproteins in cancer. Glycoconj. J. 1997, 14, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Pinho, S.S.; Reis, C.A. Glycosylation in cancer: Mechanisms and clinical implications. Nat. Rev. Cancer 2015, 15, 540–555. [Google Scholar] [CrossRef]
- Zalewska, A.; Zwierz, K.; Zółkowski, K.; Gindzieński, A. Structure and biosynthesis of human salivary mucins. Acta Biochim. Pol. 2000, 47, 1067–1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Bruyne, S.; Van Dorpe, J.; Himpe, J.; Van Biesen, W.; Delanghe, S.; Speeckaert, M.M.; Delanghe, J.R. Detection and Characterization of a Biochemical Signature Associated with Diabetic Nephropathy Using Near-infrared Spectroscopy on Tissue Sections. J. Clin. Med. 2019, 8, 1022. [Google Scholar] [CrossRef] [Green Version]
- Coopman, R.; Van de Vyver, T.; Kishabongo, A.S.; Katchunga, P.; Van Aken, E.H.; Cikomola, J.; Monteyne, T.; Speeckaert, M.M.; Delanghe, J.R. Glycation in human fingernail clippings using ATR-FTIR spectrometry, a new marker for the diagnosis and monitoring of diabetes mellitus. Clin. Biochem. 2017, 50, 62–67. [Google Scholar] [CrossRef]
- Monteyne, T.; Coopman, R.; Kishabongo, A.S.; Himpe, J.; Lapauw, B.; Shadid, S.; Van Aken, E.H.; Berenson, D.; Speeckaert, M.M.; De Beer, T.; et al. Analysis of Protein Glycation in Human Fingernail Clippings with Near-Infrared (NIR) Spectroscopy as an Alternative Technique for the Diagnosis of Diabetes Mellitus. Clin. Chem. Lab. Med. 2018, 56, 1551–1558. [Google Scholar] [CrossRef]
- Vermassen, T.; De Bruyne, S.; Himpe, J.; Lumen, N.; Callewaert, N.; Rottey, S.; Delanghe, J. N-linked glycosylation and near-infrared spectroscopy in the diagnosis of prostate cancer. Int. J. Mol. Sci. 2019, 20, 1592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afara, I.O.; Shaikh, R.; Nippolainen, E.; Querido, W.; Torniainen, J.; Sarin, J.K.; Kandel, S.; Pleshko, N.; Töyräs, J. Characterization of connective tissues using near-infrared spectroscopy and imaging. Nat. Protoc. 2021, 16, 1297–1329. [Google Scholar] [CrossRef] [PubMed]
- Siesler, H.W.; Ozaki, Y.; Kawata, S.; Heise, H.M. (Eds.) Near-Infrared Spectroscopy; Wiley: Hoboken, NJ, USA, 2001; ISBN 9783527301492. [Google Scholar]
- Roggo, Y.; Chalus, P.; Maurer, L.; Lema-Martinez, C.; Edmond, A.; Jent, N. A review of near infrared spectroscopy and chemometrics in pharmaceutical technologies. J. Pharm. Biomed. Anal. 2007, 44, 683–700. [Google Scholar] [CrossRef] [PubMed]
- De Bruyne, S.; Speeckaert, M.M.; Delanghe, J.R. Applications of mid-infrared spectroscopy in the clinical laboratory setting. Crit. Rev. Clin. Lab. Sci. 2018, 55, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Bro, R.; Smilde, A.K. Principal component analysis. Anal. Methods 2014, 6, 2812–2831. [Google Scholar] [CrossRef] [Green Version]
- Yim, O.; Ramdeen, K.T. Hierarchical Cluster Analysis: Comparison of Three Linkage Measures and Application to Psychological Data. Quant. Methods Psychol. 2015, 11, 8–21. [Google Scholar] [CrossRef]
- Custers, D.; Cauwenbergh, T.; Bothy, J.L.; Courselle, P.; De Beer, J.O.; Apers, S.; Deconinck, E. ATR-FTIR spectroscopy and chemometrics: An interesting tool to discriminate and characterize counterfeit medicines. J. Pharm. Biomed. Anal. 2015, 112, 181–189. [Google Scholar] [CrossRef]
- De Bruyne, S.; Speeckaert, R.; Boelens, J.; Hayette, M.P.; Speeckaert, M.; Delanghe, J. Infrared spectroscopy as a novel tool to diagnose onychomycosis. Br. J. Dermatol. 2019, 180, 637–646. [Google Scholar] [CrossRef] [Green Version]
- Valstar, M.H.; de Ridder, M.; van den Broek, E.C.; Stuiver, M.M.; van Dijk, B.A.C.; van Velthuysen, M.L.F.; Balm, A.J.M.; Smeele, L.E. Salivary gland pleomorphic adenoma in the Netherlands: A nationwide observational study of primary tumor incidence, malignant transformation, recurrence, and risk factors for recurrence. Oral Oncol. 2017, 66, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Paluszkiewicz, C.; Pięta, E.; Woźniak, M.; Piergies, N.; Koniewska, A.; Ścierski, W.; Misiołek, M.; Kwiatek, W.M. Saliva as a first-line diagnostic tool: A spectral challenge for identification of cancer biomarkers. J. Mol. Liq. 2020, 307. [Google Scholar] [CrossRef]
- Brozek-Pluska, B.; Kopec, M.; Niedzwiecka, I.; Morawiec-Sztandera, A. Label-free determination of lipid composition and secondary protein structure of human salivary noncancerous and cancerous tissues by Raman microspectroscopy. Analyst 2015, 140, 2107–2113. [Google Scholar] [CrossRef] [PubMed]
- Giorgini, E.; Balercia, P.; Conti, C.; Ferraris, P.; Sabbatini, S.; Rubini, C.; Tosi, G. Insights on diagnosis of oral cavity pathologies by infrared spectroscopy: A review. J. Mol. Struct. 2013, 1051, 226–232. [Google Scholar] [CrossRef]
- Bel’skaya, L.V.; Sarf, E.A.; Gundyrev, I.A. Study of the IR Spectra of the Saliva of Cancer Patients. J. Appl. Spectrosc. 2019, 85, 1076–1084. [Google Scholar] [CrossRef]
- Bel’skaya, L.V.; Sarf, E.A.; Makarova, N.A. Use of Fourier Transform IR Spectroscopy for the Study of Saliva Composition. J. Appl. Spectrosc. 2018, 85, 445–451. [Google Scholar] [CrossRef]
- Czaplicka, M.; Kowalska, A.A.; Nowicka, A.B.; Kurzydłowski, D.; Gronkiewicz, Z.; Machulak, A.; Kukwa, W.; Kamińska, A. Raman spectroscopy and surface-enhanced Raman spectroscopy (SERS) spectra of salivary glands carcinoma, tumor and healthy tissues and their homogenates analyzed by chemometry: Towards development of the novel tool for clinical diagnosis. Anal. Chim. Acta 2021, 1177, 338784. [Google Scholar] [CrossRef]
- Baker, M.J.; Trevisan, J.; Bassan, P.; Bhargava, R.; Butler, H.J.; Dorling, K.M.; Fielden, P.R.; Fogarty, S.W.; Fullwood, N.J.; Heys, K.A.; et al. Using Fourier transform IR spectroscopy to analyze biological materials. Nat. Protoc. 2014, 9, 1771–1791. [Google Scholar] [CrossRef] [Green Version]
- Baker, M.J.; Byrne, H.J.; Chalmers, J.; Gardner, P.; Goodacre, R.; Henderson, A.; Kazarian, S.G.; Martin, F.L.; Moger, J.; Stone, N.; et al. Clinical applications of infrared and Raman spectroscopy: State of play and future challenges. Analyst 2018, 143, 1735–1757. [Google Scholar] [CrossRef] [PubMed]
- Thompson, L.D.R.; Bishop, J.A. Head and Neck Pathology; Elsevier: Amsterdam, The Netherlands, 2019; ISBN 9780323479165. [Google Scholar]
- Thomsson, K.A.; Prakobphol, A.; Leffler, H.; Reddy, M.S.; Levine, M.J.; Fisher, S.J.; Hansson, G.C. The salivary mucin MG1 (MUC5B) carries a repertoire of unique oligosaccharides that is large and diverse. Glycobiology 2002, 12, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Wickström, C.; Svensäter, G. Salivary gel-forming mucin MUC5B - A nutrient for dental plaque bacteria. Oral Microbiol. Immunol. 2008, 23, 177–182. [Google Scholar] [CrossRef]
- Wickstörm, C.; Herzberg, M.C.; Beighton, D.; Svensäter, G. Proteolytic degradation of human salivary MUC5B by dental biofilms. Microbiology 2009, 155, 2866–2872. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Population | All | Male | Female | |||
|---|---|---|---|---|---|---|
| n | Age (yrs) | n | Age (yrs) | n | Age (yrs) | |
| Total | 238 | 59 (50–69) | 117 | 58 (51–69) | 121 | 59 (48–68) |
| Control group | 52 | 56 (48–68) | 27 | 61 (49–70) | 25 | 55 (48–64) |
| Salivary Gland Tumours | 186 | 59 (51–69) | 90 | 58 (51–69) | 96 | 60 (51–69) |
| Benign | ||||||
| 79 | 55 (47–63) | 37 | 52 (44–67) | 42 | 56 (48–62) |
| 40 | 55 (46–62) | 17 | 54 (44–62) | 23 | 55 (47–62) |
| 7 | 59 (48–62) | 4 | 54 (49–65) | 3 | 60 (48–62) |
| 32 | 55 (47–67) | 16 | 52 (44–71) | 16 | 56 (48–62) |
| 53 | 63 (57–71) | 31 | 63 (56–71) | 22 | 63 (59–72) |
| 5 | 64 (57–81) | 2 | 70 (61–79) | 3 | 64 (51–81) |
| Malignant | ||||||
| 11 | 55 (53–61) | 3 | 53 (50–57) | 8 | 56 (54–65) |
| 4 | 66 (62–75) | 2 | 66 (62–69) | 2 | 71 (62–80) |
| 10 | 57 (51–72) | 4 | 54 (38–69) | 6 | 63 (52–72) |
| 9 | 61 (57–67) | 6 | 60 (53–66) | 3 | 69 (62–71) |
| 9 | 57 (54–67) | 2 | 53 (52–54) | 7 | 57 (55–76) |
| 6 | 59 (56–62) | 3 | 58 (57–60) | 3 | 62 (56–64) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coopman, R.; De Bruyne, S.; Speeckaert, M.; Vermassen, T.; Vermeersch, H.; Creytens, D.; Delanghe, J. A Tissue Section-Based Near-Infrared Spectroscopical Analysis of Salivary Gland Tumors. Cancers 2021, 13, 5356. https://doi.org/10.3390/cancers13215356
Coopman R, De Bruyne S, Speeckaert M, Vermassen T, Vermeersch H, Creytens D, Delanghe J. A Tissue Section-Based Near-Infrared Spectroscopical Analysis of Salivary Gland Tumors. Cancers. 2021; 13(21):5356. https://doi.org/10.3390/cancers13215356
Chicago/Turabian StyleCoopman, Renaat, Sander De Bruyne, Marijn Speeckaert, Tijl Vermassen, Hubert Vermeersch, David Creytens, and Joris Delanghe. 2021. "A Tissue Section-Based Near-Infrared Spectroscopical Analysis of Salivary Gland Tumors" Cancers 13, no. 21: 5356. https://doi.org/10.3390/cancers13215356