
A New Look into Cancer—A Review on the Contribution of Vibrational Spectroscopy on Early Diagnosis and Surgery Guidance

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
3. Results
3.1. Which Are the Clinical Challenges?
3.1.1. Histopathology
3.1.2. Breast Cancer
Breast Cancer Diagnosis
Breast Cancer Surgical Treatment
3.1.3. Head and Neck Cancer
Head and Neck Cancer Diagnosis
Head and Neck Cancer Surgical Treatment
3.2. Raman Spectroscopy
- Spatially offset Raman spectroscopy (SORS), developed in 2005 by Matousek and co-workers [88], allows the detection of penetrating photons into the sample by biasing laterally the detection point from the laser incidence point (Figure 2a) [24,89]. Thus, this methodology provides biochemical information from several layers of tissue. Numerous improvements have been developed, with a view to increase its sensitivity, namely: surface-enhanced spatially offset Raman spectroscopy (SESORS) which couples the signal enhancement of SERS to the depth probing ability of SORS (Figure 2a) [90]; and surface-enhanced spatially offset resonance Raman spectroscopy (SESORRS), that combines resonance Raman (RR) [91] and SORS. These surface-enhanced approaches require the use of functionalised nanoparticles (NPs).
- Coherent Raman scattering (CRS) microscopy takes advantage of two exciting laser beams. Their energy of excitation is chosen according to specific vibrational modes of the sample that the user wishes to highlight (Figure 2b) [92]. In this way, particular biological components may be probed. Taking the example of the moieties of lipid constituents in tissues, the spatial distribution of is obtained.
3.2.1. Early Diagnosis of Breast Cancer by Raman Spectroscopy
3.2.2. Surgical Margins Assessment in Breast Cancer by Raman Spectroscopy
3.2.3. Head and Neck Cancer Early Diagnosis by Raman Spectroscopy
3.2.4. Head and Neck Cancer Surgical Margins Assessment by Raman Spectroscopy
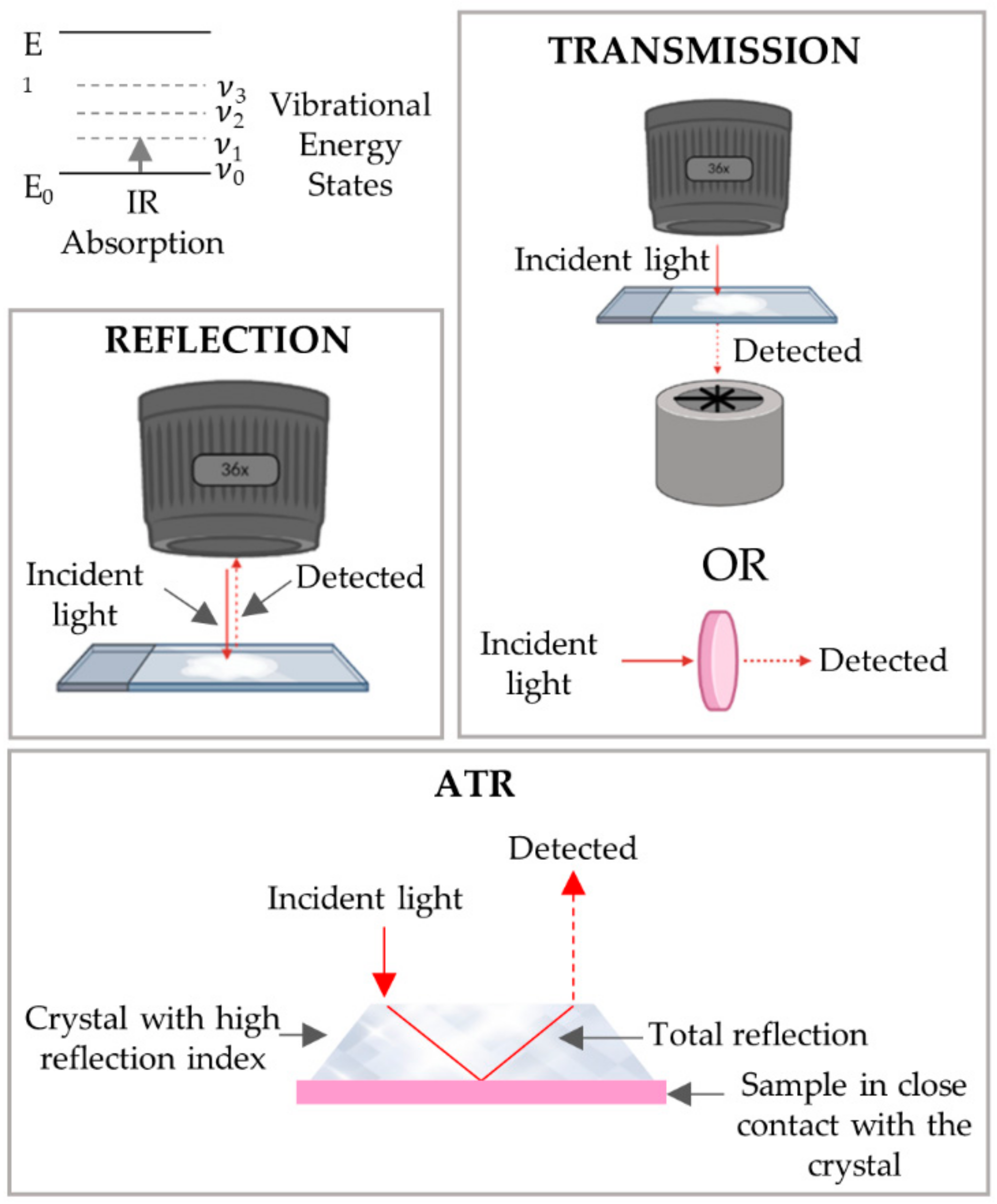
3.3. FTIR Spectroscopy
- The transmission mode, the infrared light travels through the sample, being detected after the interaction with the sample.
- In the reflection mode, in contrast to transmission, the detected infrared light is that reflected by the sample.
- In attenuated total reflectance (ATR) mode, a crystal with a high refractive index is placed in close contact with the sample. The infrared light passing through the crystal is totally reflected by the crystal walls after interacting with the sample through an evanescent wave.
3.3.1. Early Diagnosis of Breast Cancer by FTIR Spectroscopy
3.3.2. Surgical Margins Assessment of Breast Cancer by FTIR Spectroscopy
3.3.3. Early Diagnosis of Head and Neck Cancer by FTIR Spectroscopy
3.3.4. Surgical Margins Assessment of Head and Neck Cancer by FTIR Spectroscopy
3.4. Spectral Histopathology
3.4.1. Spectral Histopathology of the Breast
3.4.2. Spectral Histopathology of the Head and Neck
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Globocan. All Cancers—Number of Deaths in 2020, Both Sexes, All Ages. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/39-All-cancers-fact-sheet.pdf (accessed on 22 March 2021).
- Dai, X.; Xiang, L.; Li, T.; Bai, Z. Cancer Hallmarks, Biomarkers and Breast Cancer Molecular Subtypes. J. Cancer 2016, 7, 1281–1294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bianchini, G.; Balko, J.M.; Mayer, I.A.; Sanders, M.E.; Gianni, L. Triple-negative breast cancer: Challenges and opportunities of a heterogeneous disease. Nat. Rev. Clin. Oncol. 2016, 13, 674–690. [Google Scholar] [CrossRef]
- Bastien, R.R.; Rodriguez-Lescure, A.; Ebbert, M.T.; Prat, A.; Munarriz, B.; Rowe, L.; Miller, P.; Ruiz-Borrego, M.; Anderson, D.; Lyons, B.; et al. PAM50 breast cancer subtyping by RT-qPCR and concordance with standard clinical molecular markers. BMC Med. Genom. 2012, 5, 44. [Google Scholar] [CrossRef] [Green Version]
- Tang, P.; Bui, M.M.; Peng, Y. Immunohistochemistry in Breast Cancer. In Practical Breast Pathology, Practical Anatomic Pathology; Peng, Y., Tang, P., Eds.; Springer: Cham, Switzerland, 2019; pp. 173–192. [Google Scholar] [CrossRef]
- Jurikova, M.; Danihel, L.; Polak, S.; Varga, I. Ki67, PCNA, and MCM proteins: Markers of proliferation in the diagnosis of breast cancer. Acta Histochem. 2016, 118, 544–552. [Google Scholar] [CrossRef]
- Chun, Y.S.; Pawlik, T.M.; Vauthey, J.N. 8th Edition of the AJCC Cancer Staging Manual: Pancreas and Hepatobiliary Cancers. Ann. Surg. Oncol. 2018, 25, 845–847. [Google Scholar] [CrossRef]
- Keshavarzi, M.; Darijani, M.; Momeni, F.; Moradi, P.; Ebrahimnejad, H.; Masoudifar, A.; Mirzaei, H. Molecular Imaging and Oral Cancer Diagnosis and Therapy. J. Cell. Biochem. 2017, 118, 3055–3060. [Google Scholar] [CrossRef]
- Jafari, S.H.; Saadatpour, Z.; Salmaninejad, A.; Momeni, F.; Mokhtari, M.; Nahand, J.S.; Rahmati, M.; Mirzaei, H.; Kianmehr, M. Breast cancer diagnosis: Imaging techniques and biochemical markers. J. Cell Physiol. 2018, 233, 5200–5213. [Google Scholar] [CrossRef]
- Pavlova, N.N.; Thompson, C.B. The Emerging Hallmarks of Cancer Metabolism. Cell. Metab. 2016, 23, 27–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fouad, Y.A.; Aanei, C. Revisiting the hallmarks of cancer. Am. J. Cancer Res. 2017, 7, 1016–1036. [Google Scholar]
- Lopes, J.; Correia, M.; Martins, I.; Henriques, A.G.; Delgadillo, I.; da Cruz, E.S.O.; Nunes, A. FTIR and Raman Spectroscopy Applied to Dementia Diagnosis Through Analysis of Biological Fluids. J. Alzheimer’s Dis. 2016, 52, 801–812. [Google Scholar] [CrossRef] [PubMed]
- Palombo, F.; Tamagnini, F.; Jeynes, J.C.G.; Mattana, S.; Swift, I.; Nallala, J.; Hancock, J.; Brown, J.T.; Randall, A.D.; Stone, N. Detection of Aβ plaque-associated astrogliosis in Alzheimer’s disease brain by spectroscopic imaging and immunohistochemistry. Analyst 2018, 143, 850–857. [Google Scholar] [CrossRef] [Green Version]
- Coopman, R.; Van de Vyver, T.; Kishabongo, A.S.; Katchunga, P.; Van Aken, E.H.; Cikomola, J.; Monteyne, T.; Speeckaert, M.M.; Delanghe, J.R. Glycation in human fingernail clippings using ATR-FTIR spectrometry, a new marker for the diagnosis and monitoring of diabetes mellitus. Clin. Biochem. 2017, 50, 62–67. [Google Scholar] [CrossRef]
- Roman, M.; Kaminska, A.; Drozdz, A.; Platt, M.; Kuzniewski, M.; Malecki, M.T.; Kwiatek, W.M.; Paluszkiewicz, C.; Stepien, E.L. Raman spectral signatures of urinary extracellular vesicles from diabetic patients and hyperglycemic endothelial cells as potential biomarkers in diabetes. Nanomedicine 2019, 17, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Moor, K.; Ohtani, K.; Myrzakozha, D.; Zhanserkenova, O.; Andriana, B.B.; Sato, H. Noninvasive and label-free determination of virus infected cells by Raman spectroscopy. J. Biomed. Opt. 2014, 19, 067003. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Purra, M.; Carre-Camps, M.; de Puig, H.; Bosch, I.; Gehrke, L.; Hamad-Schifferli, K. Surface-Enhanced Raman Spectroscopy-Based Sandwich Immunoassays for Multiplexed Detection of Zika and Dengue Viral Biomarkers. ACS Infect. Dis. 2017, 3, 767–776. [Google Scholar] [CrossRef] [PubMed]
- Rymsza, T.; Ribeiro, E.A.; de Carvalho, L.; Bhattacharjee, T.; de Azevedo Canevari, R. Human papillomavirus detection using PCR and ATR-FTIR for cervical cancer screening. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2018, 196, 238–246. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, X.; Luo, C.; Liu, Z.; Chen, Y.; Dong, S.; Jiang, C.; Yang, S.; Wang, F.; Xiao, X. Volume-Enhanced Raman Scattering Detection of Viruses. Small 2019, 15, e1805516. [Google Scholar] [CrossRef]
- Bird, B.; Miljkovic, M.S.; Remiszewski, S.; Akalin, A.; Kon, M.; Diem, M. Infrared spectral histopathology (SHP): A novel diagnostic tool for the accurate classification of lung cancer. Lab. Investig. 2012, 92, 1358–1373. [Google Scholar] [CrossRef] [Green Version]
- Bassan, P.; Mellor, J.; Shapiro, J.; Williams, K.J.; Lisanti, M.P.; Gardner, P. Transmission FT-IR chemical imaging on glass substrates: Applications in infrared spectral histopathology. Anal. Chem. 2014, 86, 1648–1653. [Google Scholar] [CrossRef]
- Santos, I.P.; Barroso, E.M.; Bakker Schut, T.C.; Caspers, P.J.; van Lanschot, C.G.F.; Choi, D.H.; van der Kamp, M.F.; Smits, R.W.H.; van Doorn, R.; Verdijk, R.M.; et al. Raman spectroscopy for cancer detection and cancer surgery guidance: Translation to the clinics. Analyst 2017, 142, 3025–3047. [Google Scholar] [CrossRef]
- Byrne, H.J.; Behl, I.; Calado, G.; Ibrahim, O.; Toner, M.; Galvin, S.; Healy, C.M.; Flint, S.; Lyng, F.M. Biomedical applications of vibrational spectroscopy: Oral cancer diagnostics. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2021, 252, 119470. [Google Scholar] [CrossRef] [PubMed]
- Matousek, P.; Stone, N. Development of deep subsurface Raman spectroscopy for medical diagnosis and disease monitoring. Chem. Soc. Rev. 2016, 45, 1794–1802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frost, J.; Ludeman, L.; Hillaby, K.; Gornall, R.; Lloyd, G.R.; Kendall, C.; Shore, A.C.; Stone, N. Raman Spectroscopy and Multivariate Analysis for the Non Invasive Diagnosis of Clinically Inconclusive Vulval Lichen Sclerosus. Analyst 2017, 142, 1200–1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, A.T.; Gaifulina, R.; Guppy, N.J.; Isabelle, M.; Dorney, J.; Lloyd, G.R.; Rodriguez-Justo, M.; Kendall, C.; Stone, N.; Thomas, G.M. Developing Raman spectroscopy as a diagnostic tool for label-free antigen detection. J. Biophotonics 2018, 11, e201700028. [Google Scholar] [CrossRef] [PubMed]
- Lasch, P.; Stammler, M.; Zhang, M.; Baranska, M.; Bosch, A.; Majzner, K. FT-IR Hyperspectral Imaging and Artificial Neural Network Analysis for Identification of Pathogenic Bacteria. Anal. Chem. 2018, 90, 8896–8904. [Google Scholar] [CrossRef] [PubMed]
- Veta, M.; Pluim, J.P.; van Diest, P.J.; Viergever, M.A. Breast cancer histopathology image analysis: A review. IEEE Trans. Biomed. Eng. 2014, 61, 1400–1411. [Google Scholar] [CrossRef]
- Brunye, T.T.; Mercan, E.; Weaver, D.L.; Elmore, J.G. Accuracy is in the eyes of the pathologist: The visual interpretive process and diagnostic accuracy with digital whole slide images. J. Biomed. Inform. 2017, 66, 171–179. [Google Scholar] [CrossRef]
- Elmore, J.G.; Longton, G.M.; Carney, P.A.; Geller, B.M.; Onega, T.; Tosteson, A.N.; Nelson, H.D.; Pepe, M.S.; Allison, K.H.; Schnitt, S.J.; et al. Diagnostic concordance among pathologists interpreting breast biopsy specimens. JAMA 2015, 313, 1122–1132. [Google Scholar] [CrossRef]
- Elmore, J.G.; Barnhill, R.L.; Elder, D.E.; Longton, G.M.; Pepe, M.S.; Reisch, L.M.; Carney, P.A.; Titus, L.J.; Nelson, H.D.; Onega, T.; et al. Pathologists’ diagnosis of invasive melanoma and melanocytic proliferations: Observer accuracy and reproducibility study. BMJ 2017, 357, j2813. [Google Scholar] [CrossRef] [Green Version]
- Elmore, J.G.; Nelson, H.D.; Pepe, M.S.; Longton, G.M.; Tosteson, A.N.; Geller, B.; Onega, T.; Carney, P.A.; Jackson, S.L.; Allison, K.H.; et al. Variability in Pathologists’ Interpretations of Individual Breast Biopsy Slides: A Population Perspective. Ann. Intern. Med. 2016, 164, 649–655. [Google Scholar] [CrossRef]
- Gilks, C.B.; Oliva, E.; Soslow, R.A. Poor interobserver reproducibility in the diagnosis of high-grade endometrial carcinoma. Am. J. Surg. Pathol. 2013, 37, 874–881. [Google Scholar] [CrossRef] [PubMed]
- Sangoi, A.R.; Beck, A.H.; Amin, M.B.; Cheng, L.; Epstein, J.I.; Hansel, D.E.; Iczkowski, K.A.; Lopez-Beltran, A.; Oliva, E.; Paner, G.P.; et al. Interobserver reproducibility in the diagnosis of invasive micropapillary carcinoma of the urinary tract among urologic pathologists. Am. J. Surg. Pathol. 2010, 34, 1367–1376. [Google Scholar] [CrossRef]
- Thunnissen, E.; Beasley, M.B.; Borczuk, A.C.; Brambilla, E.; Chirieac, L.R.; Dacic, S.; Flieder, D.; Gazdar, A.; Geisinger, K.; Hasleton, P.; et al. Reproducibility of histopathological subtypes and invasion in pulmonary adenocarcinoma. An international interobserver study. Mod. Pathol. 2012, 25, 1574–1583. [Google Scholar] [CrossRef]
- Globocan. Estimated Age-Standardized Incidence and Mortality Rates (World) in 2020, Worldwide, Both Sexes, All Ages. Available online: https://gco.iarc.fr/today/online-analysis-multi-bars?v=2020&mode=cancer&mode_population=countries&population=900&populations=900&key=asr&sex=0&cancer=39&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=17&nb_items=10&group_cancer=1&include_nmsc=1&include_nmsc_other=1&type_multiple=%257B%2522inc%2522%253Atrue%252C%2522mort%2522%253Atrue%252C%2522prev%2522%253Afalse%257D&orientation=horizontal&type_sort=0&type_nb_items=%257B%2522top%2522%253Atrue%252C%2522bottom%2522%253Afalse%257D (accessed on 15 February 2021).
- Harbeck, N.; Penault-Llorca, F.; Cortes, J.; Gnant, M.; Houssami, N.; Poortmans, P.; Ruddy, K.; Tsang, J.; Cardoso, F. Breast cancer. Nat. Rev. Dis. Primers 2019, 5, 66. [Google Scholar] [CrossRef]
- Byrne, C.; Divekar, S.D.; Storchan, G.B.; Parodi, D.A.; Martin, M.B. Metals and breast cancer. J. Mammary Gland Biol. Neoplasia 2013, 18, 63–73. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Nguyen, N.; Colditz, G.A. Links between alcohol consumption and breast cancer: A look at the evidence. Women’s Health 2015, 11, 65–77. [Google Scholar] [CrossRef] [Green Version]
- Romaniuk, A.; Lyndin, M.; Sikora, V.; Lyndina, Y.; Romaniuk, S.; Sikora, K. Heavy metals effect on breast cancer progression. J. Occup. Med. Toxicol. 2017, 12, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lope, V.; Martin, M.; Castello, A.; Casla, S.; Ruiz, A.; Baena-Canada, J.M.; Casas, A.M.; Calvo, L.; Bermejo, B.; Munoz, M.; et al. Physical activity and breast cancer risk by pathological subtype. Gynecol. Oncol. 2017, 144, 577–585. [Google Scholar] [CrossRef]
- Durand, M.A.; Haas, B.M.; Yao, X.; Geisel, J.L.; Raghu, M.; Hooley, R.J.; Horvath, L.J.; Philpotts, L.E. Early clinical experience with digital breast tomosynthesis for screening mammography. Radiology 2015, 274, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Zaha, D.C. Significance of immunohistochemistry in breast cancer. World J. Clin. Oncol. 2014, 5, 382–392. [Google Scholar] [CrossRef]
- Bertoli, G.; Cava, C.; Castiglioni, I. MicroRNAs: New Biomarkers for Diagnosis, Prognosis, Therapy Prediction and Therapeutic Tools for Breast Cancer. Theranostics 2015, 5, 1122–1143. [Google Scholar] [CrossRef]
- Graveel, C.R.; Calderone, H.M.; Westerhuis, J.J.; Winn, M.E.; Sempere, L.F. Critical analysis of the potential for microRNA biomarkers in breast cancer management. Breast Cancer (Dove Med. Press) 2015, 7, 59–79. [Google Scholar] [CrossRef] [Green Version]
- Erbes, T.; Hirschfeld, M.; Rucker, G.; Jaeger, M.; Boas, J.; Iborra, S.; Mayer, S.; Gitsch, G.; Stickeler, E. Feasibility of urinary microRNA detection in breast cancer patients and its potential as an innovative non-invasive biomarker. BMC Cancer 2015, 15, 193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aggarwal, T.; Wadhwa, R.; Gupta, R.; Paudel, K.R.; Collet, T.; Chellappan, D.K.; Gupta, G.; Perumalsamy, H.; Mehta, M.; Satija, S.; et al. MicroRNAs as Biomarker for Breast Cancer. Endocr. Metab. Immune Disord. Drug Targets 2020, 20, 1597–1610. [Google Scholar] [CrossRef]
- Jia, Y.; Chen, Y.; Wang, Q.; Jayasinghe, U.; Luo, X.; Wei, Q.; Wang, J.; Xiong, H.; Chen, C.; Xu, B.; et al. Exosome: Emerging biomarker in breast cancer. Oncotarget 2017, 8, 41717–41733. [Google Scholar] [CrossRef] [Green Version]
- Halvaei, S.; Daryani, S.; Eslami, S.Z.; Samadi, T.; Jafarbeik-Iravani, N.; Bakhshayesh, T.O.; Majidzadeh, A.K.; Esmaeili, R. Exosomes in Cancer Liquid Biopsy: A Focus on Breast Cancer. Mol. Ther. Nucleic Acids 2018, 10, 131–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hesari, A.; Golrokh Moghadam, S.A.; Siasi, A.; Rahmani, M.; Behboodi, N.; Rastgar-Moghadam, A.; Ferns, G.A.; Ghasemi, F.; Avan, A. Tumor-derived exosomes: Potential biomarker or therapeutic target in breast cancer? J. Cell. Biochem. 2018, 119, 4236–4240. [Google Scholar] [CrossRef] [Green Version]
- Kocan, S.; Gursoy, A. Body Image of Women with Breast Cancer After Mastectomy: A Qualitative Research. J. Breast Health 2016, 12, 145–150. [Google Scholar] [CrossRef] [Green Version]
- Rojas, K.; Onstad, M.; Raker, C.; Clark, M.A.; Stuckey, A.; Gass, J. The impact of mastectomy type on the Female Sexual Function Index (FSFI), satisfaction with appearance, and the reconstructed breast’s role in intimacy. Breast Cancer Res. Treat. 2017, 163, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Pietruski, P.; Noszczyk, B.; Paskal, A.M.; Paskal, W.; Paluch, L.; Jaworowski, J. The Impact of Mastectomy on Women’s Visual Perception of Breast Aesthetics and Symmetry: A Pilot Eye-Tracking Study. Aesthet. Surg. J. 2020, 40, 850–861. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.C.; Yan, W.; Christos, P.J.; Nori, D.; Ravi, A. Equivalent Survival With Mastectomy or Breast-conserving Surgery Plus Radiation in Young Women Aged <40 Years with Early Stage Breast Cancer: A National Registry-based Stage-by-Stage Comparison. Clin. Breast Cancer 2015, 15, 390–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clough, K.B.; Gouveia, P.F.; Benyahi, D.; Massey, E.J.; Russ, E.; Sarfati, I.; Nos, C. Positive Margins After Oncoplastic Surgery for Breast Cancer. Ann. Surg. Oncol. 2015, 22, 4247–4253. [Google Scholar] [CrossRef]
- Corsi, F.; Sorrentino, L.; Bossi, D.; Sartani, A.; Foschi, D. Preoperative localization and surgical margins in conservative breast surgery. Int. J. Surg. Oncol. 2013, 2013, 793819. [Google Scholar] [CrossRef] [Green Version]
- Pilewskie, M.; Morrow, M. Margins in breast cancer: How much is enough? Cancer 2018, 124, 1335–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dupont, E.; Tsangaris, T.; Garcia-Cantu, C.; Howard-McNatt, M.; Chiba, A.; Berger, A.C.; Levine, E.A.; Gass, J.S.; Gallagher, K.; Lum, S.S.; et al. Resection of Cavity Shave Margins in Stage 0-III Breast Cancer Patients Undergoing Breast Conserving Surgery: A Prospective Multicenter Randomized Controlled Trial. Ann. Surg. 2019. [Google Scholar] [CrossRef]
- Maguire, A.; Brogi, E. Sentinel lymph nodes for breast carcinoma: An update on current practice. Histopathology 2016, 68, 152–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, M.; Anninga, B.; Goyal, S.; Young, P.; Pankhurst, Q.A.; Douek, M.; Hamed, H.; Kothari, A.; Kovacs, T.; McWilliams, S.; et al. Magnetic sentinel node and occult lesion localization in breast cancer (MagSNOLL Trial). Br. J. Surg. 2015, 102, 646–652. [Google Scholar] [CrossRef]
- Cserni, G. Intraoperative analysis of sentinel lymph nodes in breast cancer by one-step nucleic acid amplification. J. Clin. Pathol. 2012, 65, 193–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langhans, L.; Jensen, M.B.; Talman, M.M.; Vejborg, I.; Kroman, N.; Tvedskov, T.F. Reoperation Rates in Ductal Carcinoma In Situ vs. Invasive Breast Cancer after Wire-Guided Breast-Conserving Surgery. JAMA Surg. 2017, 152, 378–384. [Google Scholar] [CrossRef]
- Lai, H.W.; Huang, R.H.; Wu, Y.T.; Chen, C.J.; Chen, S.T.; Lin, Y.J.; Chen, D.R.; Lee, C.W.; Wu, H.K.; Lin, H.Y.; et al. Clinicopathologic factors related to surgical margin involvement, reoperation, and residual cancer in primary operable breast cancer—An analysis of 2050 patients. Eur. J. Surg. Oncol. 2018, 44, 1725–1735. [Google Scholar] [CrossRef]
- McCahill, L.E.; Single, R.M.; Aiello Bowles, E.J.; Feigelson, H.S.; James, T.A.; Barney, T.; Engel, J.M.; Onitilo, A.A. Variability in reexcision following breast conservation surgery. JAMA 2012, 307, 467–475. [Google Scholar] [CrossRef] [Green Version]
- Valero, M.G.; Mallory, M.A.; Losk, K.; Tukenmez, M.; Hwang, J.; Camuso, K.; Bunnell, C.; King, T.; Golshan, M. Surgeon Variability and Factors Predicting for Reoperation Following Breast-Conserving Surgery. Ann. Surg. Oncol. 2018, 25, 2573–2578. [Google Scholar] [CrossRef] [PubMed]
- Landercasper, J.; Borgert, A.J.; Fayanju, O.M.; Cody, H., 3rd; Feldman, S.; Greenberg, C.; Linebarger, J.; Pockaj, B.; Wilke, L. Factors Associated with Reoperation in Breast-Conserving Surgery for Cancer: A Prospective Study of American Society of Breast Surgeon Members. Ann. Surg. Oncol. 2019, 26, 3321–3336. [Google Scholar] [CrossRef]
- Marur, S.; D’Souza, G.; Westra, W.H.; Forastiere, A.A. HPV-associated head and neck cancer: A virus-related cancer epidemic. Lancet Oncol. 2010, 11, 781–789. [Google Scholar] [CrossRef] [Green Version]
- Rettig, E.M.; D’Souza, G. Epidemiology of head and neck cancer. Surg Oncol. Clin. N. Am. 2015, 24, 379–396. [Google Scholar] [CrossRef] [PubMed]
- Leemans, C.R.; Snijders, P.J.F.; Brakenhoff, R.H. The molecular landscape of head and neck cancer. Nat. Rev. Cancer 2018, 18, 269–282. [Google Scholar] [CrossRef]
- Globocan. Estimated Number of New Cases in 2020, Worldwide, Both Sexes, All Ages. Available online: https://gco.iarc.fr/today/online-analysis-table?v=2020&mode=cancer&mode_population=continents&population=900&populations=900&key=asr&sex=0&cancer=39&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=17&group_cancer=1&include_nmsc=1&include_nmsc_other=1 (accessed on 15 February 2021).
- Adrien, J.; Bertolus, C.; Gambotti, L.; Mallet, A.; Baujat, B. Why are head and neck squamous cell carcinoma diagnosed so late? Influence of health care disparities and socio-economic factors. Oral Oncol. 2014, 50, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Gregoire, V.; Lefebvre, J.L.; Licitra, L.; Felip, E.; EHNS–ESMO–ESTRO Guidelines Working Group. Squamous cell carcinoma of the head and neck: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2010, 21 (Suppl. 5), v184–v186. [Google Scholar] [CrossRef]
- Ni, X.G.; Wang, G.Q. The Role of Narrow Band Imaging in Head and Neck Cancers. Curr. Oncol. Rep. 2016, 18, 10. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Zhang, J.; Guo, L.; Nie, J.; Zhu, C.; Ma, X. The value of narrow band imaging in diagnosis of head and neck cancer: A meta-analysis. Sci. Rep. 2018, 8, 515. [Google Scholar] [CrossRef]
- Schlecht, N.F.; Brandwein-Gensler, M.; Nuovo, G.J.; Li, M.; Dunne, A.; Kawachi, N.; Smith, R.V.; Burk, R.D.; Prystowsky, M.B. A comparison of clinically utilized human papillomavirus detection methods in head and neck cancer. Mod. Pathol. 2011, 24, 1295–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marur, S.; Forastiere, A.A. Head and Neck Squamous Cell Carcinoma: Update on Epidemiology, Diagnosis, and Treatment. Mayo Clin. Proc. 2016, 91, 386–396. [Google Scholar] [CrossRef] [Green Version]
- Chow, L.Q.M. Head and Neck Cancer. N. Engl. J. Med. 2020, 382, 60–72. [Google Scholar] [CrossRef]
- Thomas Robbins, K.; Triantafyllou, A.; Suarez, C.; Lopez, F.; Hunt, J.L.; Strojan, P.; Williams, M.D.; Braakhuis, B.J.M.; de Bree, R.; Hinni, M.L.; et al. Surgical margins in head and neck cancer: Intra- and postoperative considerations. Auris Nasus Larynx 2019, 46, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Layfield, E.M.; Schmidt, R.L.; Esebua, M.; Layfield, L.J. Frozen Section Evaluation of Margin Status in Primary Squamous Cell Carcinomas of the Head and Neck: A Correlation Study of Frozen Section and Final Diagnoses. Head Neck Pathol. 2018, 12, 175–180. [Google Scholar] [CrossRef]
- Tirelli, G.; Hinni, M.L.; Fernandez-Fernandez, M.M.; Bussani, R.; Gatto, A.; Bonini, P.; Giudici, F.; Boscolo Nata, F. Frozen sections and complete resection in oral cancer surgery. Oral Dis. 2019, 25, 1309–1317. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.D. Determining Adequate Margins in Head and Neck Cancers: Practice and Continued Challenges. Curr. Oncol. Rep. 2016, 18, 54. [Google Scholar] [CrossRef]
- Buchakjian, M.R.; Tasche, K.K.; Robinson, R.A.; Pagedar, N.A.; Sperry, S.M. Association of Main Specimen and Tumor Bed Margin Status with Local Recurrence and Survival in Oral Cancer Surgery. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 1191–1198. [Google Scholar] [CrossRef] [Green Version]
- Wehage, I.C.; Fansa, H. Complex reconstructions in head and neck cancer surgery: Decision making. Head Neck Oncol. 2011, 3, 14. [Google Scholar] [CrossRef] [Green Version]
- Batista de Carvalho, A.L.; Pilling, M.; Gardner, P.; Doherty, J.; Cinque, G.; Wehbe, K.; Kelley, C.; Batista de Carvalho, L.A.; Marques, M.P. Chemotherapeutic response to cisplatin-like drugs in human breast cancer cells probed by vibrational microspectroscopy. Faraday Discuss. 2016, 187, 273–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marques, M.P.M.; Batista de Carvalho, A.L.M.; Mamede, A.P.; Santos, I.P.; Garcia Sakai, V.; Dopplapudi, A.; Cinque, G.; Wolna, M.; Gardner, P.; Batista de Carvalho, L.A.E. Chemotherapeutic Targets in Osteosarcoma: Insights from Synchrotron-MicroFTIR and Quasi-Elastic Neutron Scattering. J. Phys. Chem. B 2019, 123, 6968–6979. [Google Scholar] [CrossRef]
- Hudson, S.D.; Chumanov, G. Bioanalytical applications of SERS (surface-enhanced Raman spectroscopy). Anal. Bioanal. Chem. 2009, 394, 679–686. [Google Scholar] [CrossRef]
- Zong, C.; Xu, M.; Xu, L.J.; Wei, T.; Ma, X.; Zheng, X.S.; Hu, R.; Ren, B. Surface-Enhanced Raman Spectroscopy for Bioanalysis: Reliability and Challenges. Chem. Rev. 2018, 118, 4946–4980. [Google Scholar] [CrossRef] [PubMed]
- Matousek, P.; Clark, I.P.; Draper, E.R.; Morris, M.D.; Goodship, A.E.; Everall, N.; Towrie, M.; Finney, W.F.; Parker, A.W. Subsurface probing in diffusely scattering media using spatially offset Raman spectroscopy. Appl. Spectrosc. 2005, 59, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Matousek, P.; Stone, N. Recent advances in the development of Raman spectroscopy for deep non-invasive medical diagnosis. J. Biophotonics 2013, 6, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Nicolson, F.; Kircher, M.F.; Stone, N.; Matousek, P. Spatially offset Raman spectroscopy for biomedical applications. Chem Soc. Rev. 2021, 50, 556–568. [Google Scholar] [CrossRef]
- Robert, B. Resonance Raman spectroscopy. Photosynth. Res. 2009, 101, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Zhang, D.; Cheng, J.X. Coherent Raman Scattering Microscopy in Biology and Medicine. Annu. Rev. Biomed. Eng. 2015, 17, 415–445. [Google Scholar] [CrossRef] [Green Version]
- Cervo, S.; Mansutti, E.; Del Mistro, G.; Spizzo, R.; Colombatti, A.; Steffan, A.; Sergo, V.; Bonifacio, A. SERS analysis of serum for detection of early and locally advanced breast cancer. Anal. Bioanal. Chem. 2015, 407, 7503–7509. [Google Scholar] [CrossRef] [PubMed]
- Nargis, H.F.; Nawaz, H.; Ditta, A.; Mahmood, T.; Majeed, M.I.; Rashid, N.; Muddassar, M.; Bhatti, H.N.; Saleem, M.; Jilani, K.; et al. Raman spectroscopy of blood plasma samples from breast cancer patients at different stages. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2019, 222, 117210. [Google Scholar] [CrossRef] [Green Version]
- Nargis, H.F.; Nawaz, H.; Bhatti, H.N.; Jilani, K.; Saleem, M. Comparison of surface enhanced Raman spectroscopy and Raman spectroscopy for the detection of breast cancer based on serum samples. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2021, 246, 119034. [Google Scholar] [CrossRef] [PubMed]
- Moisoiu, V.; Stefancu, A.; Gulei, D.; Boitor, R.; Magdo, L.; Raduly, L.; Pasca, S.; Kubelac, P.; Mehterov, N.; Chis, V.; et al. SERS-based differential diagnosis between multiple solid malignancies: Breast, colorectal, lung, ovarian and oral cancer. Int. J. Nanomed. 2019, 14, 6165–6178. [Google Scholar] [CrossRef] [Green Version]
- Moisoiu, V.; Socaciu, A.; Stefancu, A.; Iancu, S.D.; Boros, I.; Alecsa, C.D.; Rachieriu, C.; Chiorean, A.R.; Eniu, D.; Leopold, N.; et al. Breast Cancer Diagnosis by Surface-Enhanced Raman Scattering (SERS) of Urine. Appl. Sci. 2019, 9, 806. [Google Scholar] [CrossRef] [Green Version]
- Lin, X.L.; Wang, L.N.; Lin, H.J.; Lin, D.; Lin, J.Y.; Liu, X.J.; Qiu, S.F.; Xu, Y.J.; Chen, G.N.; Feng, S.Y. A novel urine analysis technique combining affinity chromatography with Au nanoparticle based surface enhanced Raman spectroscopy for potential applications in non-invasive cancer screening. J. Biophotonics 2019, 12. [Google Scholar] [CrossRef] [PubMed]
- Nicolson, F.; Jamieson, L.E.; Mabbott, S.; Plakas, K.; Shand, N.C.; Detty, M.R.; Graham, D.; Faulds, K. Multiplex imaging of live breast cancer tumour models through tissue using handheld surface enhanced spatially offset resonance Raman spectroscopy (SESORRS). Chem. Commun. 2018, 54, 8530–8533. [Google Scholar] [CrossRef] [Green Version]
- Nicolson, F.; Jamieson, L.E.; Mabbott, S.; Plakas, K.; Shand, N.C.; Detty, M.R.; Graham, D.; Faulds, K. Through tissue imaging of a live breast cancer tumour model using handheld surface enhanced spatially offset resonance Raman spectroscopy (SESORRS). Chem. Sci. 2018, 9, 3788–3792. [Google Scholar] [CrossRef] [Green Version]
- Nicolson, F.; Andreiuk, B.; Andreou, C.; Hsu, H.T.; Rudder, S.; Kircher, M.F. Non-invasive In Vivo Imaging of Cancer Using Surface-Enhanced Spatially Offset Raman Spectroscopy (SESORS). Theranostics 2019, 9, 5899–5913. [Google Scholar] [CrossRef]
- Stone, N.; Kerssens, M.; Lloyd, G.R.; Faulds, K.; Graham, D.; Matousek, P. Surface enhanced spatially offset Raman spectroscopic (SESORS) imaging-the next dimension. Chem. Sci. 2011, 2, 776–780. [Google Scholar] [CrossRef]
- Desroches, J.; Jermyn, M.; Pinto, M.; Picot, F.; Tremblay, M.A.; Obaid, S.; Marple, E.; Urmey, K.; Trudel, D.; Soulez, G.; et al. A new method using Raman spectroscopy for in vivo targeted brain cancer tissue biopsy. Sci. Rep. 2018, 8, 1792. [Google Scholar] [CrossRef]
- Saha, A.; Barman, I.; Dingari, N.C.; McGee, S.; Volynskaya, Z.; Galindo, L.H.; Liu, W.; Plecha, D.; Klein, N.; Dasari, R.R.; et al. Raman spectroscopy: A real-time tool for identifying microcalcifications during stereotactic breast core needle biopsies. Biomed. Opt. Express 2011, 2, 2792–2803. [Google Scholar] [CrossRef] [Green Version]
- Barman, I.; Dingari, N.C.; Saha, A.; McGee, S.; Galindo, L.H.; Liu, W.; Plecha, D.; Klein, N.; Dasari, R.R.; Fitzmaurice, M. Application of Raman spectroscopy to identify microcalcifications and underlying breast lesions at stereotactic core needle biopsy. Cancer Res. 2013, 73, 3206–3215. [Google Scholar] [CrossRef] [Green Version]
- Koya, S.K.; Brusatori, M.; Yurgelevic, S.; Huang, C.; Werner, C.W.; Kast, R.E.; Shanley, J.; Sherman, M.; Honn, K.V.; Maddipati, K.R.; et al. Accurate identification of breast cancer margins in microenvironments of ex vivo basal and luminal breast cancer tissues using Raman spectroscopy. Prostaglandins Lipid Mediat. 2020, 151, 106475. [Google Scholar] [CrossRef]
- Kong, K.; Zaabar, F.; Rakha, E.; Ellis, I.; Koloydenko, A.; Notingher, I. Towards intra-operative diagnosis of tumours during breast conserving surgery by selective-sampling Raman micro-spectroscopy. Phys. Med. Biol. 2014, 59, 6141–6152. [Google Scholar] [CrossRef]
- Shipp, D.W.; Rakha, E.A.; Koloydenko, A.A.; Macmillan, R.D.; Ellis, I.O.; Notingher, I. Intra-operative spectroscopic assessment of surgical margins during breast conserving surgery. Breast Cancer Res. 2018, 20, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lizio, M.G.; Liao, Z.; Shipp, D.W.; Boitor, R.; Mihai, R.; Sharp, J.S.; Russel, M.; Khout, H.; Rakha, E.A.; Notingher, I. Combined total internal reflection AF spectral-imaging and Raman spectroscopy for fast assessment of surgical margins during breast cancer surgery. Biomed. Opt. Express 2021, 12, 940–954. [Google Scholar] [CrossRef]
- Liao, Z.; Lizio, M.G.; Corden, C.; Khout, H.; Rakha, E.; Notingher, I. Feasibility of integrated high-wavenumber Raman imaging and fingerprint Raman spectroscopy for fast margin assessment in breast cancer surgery. J. Raman Spectrosc. 2020, 51, 1986–1995. [Google Scholar] [CrossRef]
- Thomas, G.; Nguyen, T.Q.; Pence, I.J.; Caldwell, B.; O’Connor, M.E.; Giltnane, J.; Sanders, M.E.; Grau, A.; Meszoely, I.; Hooks, M.; et al. Evaluating feasibility of an automated 3-dimensional scanner using Raman spectroscopy for intraoperative breast margin assessment. Sci. Rep. 2017, 7, 13548. [Google Scholar] [CrossRef] [Green Version]
- Keller, M.D.; Vargis, E.; de Matos Granja, N.; Wilson, R.H.; Mycek, M.A.; Kelley, M.C.; Mahadevan-Jansen, A. Development of a spatially offset Raman spectroscopy probe for breast tumor surgical margin evaluation. J. Biomed. Opt. 2011, 16, 077006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.W.; Reder, N.P.; Kang, S.; Glaser, A.K.; Yang, Q.; Wall, M.A.; Javid, S.H.; Dintzis, S.M.; Liu, J.T.C. Raman-Encoded Molecular Imaging with Topically Applied SERS Nanoparticles for Intraoperative Guidance of Lumpectomy. Cancer Res. 2017, 77, 4506–4516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horsnell, J.D.; Smith, J.A.; Sattlecker, M.; Sammon, A.; Christie-Brown, J.; Kendall, C.; Stone, N. Raman spectroscopy—A potential new method for the intra-operative assessment of axillary lymph nodes. Surgeon 2012, 10, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Petterson, I.E.; Day, J.C.; Fullwood, L.M.; Gardner, B.; Stone, N. Characterisation of a fibre optic Raman probe within a hypodermic needle. Anal. Bioanal. Chem. 2015, 407, 8311–8320. [Google Scholar] [CrossRef] [PubMed]
- Zuniga, W.C.; Jones, V.; Anderson, S.M.; Echevarria, A.; Miller, N.L.; Stashko, C.; Schmolze, D.; Cha, P.D.; Kothari, R.; Fong, Y.; et al. Raman Spectroscopy for Rapid Evaluation of Surgical Margins during Breast Cancer Lumpectomy. Sci. Rep. 2019, 9, 14639. [Google Scholar] [CrossRef] [Green Version]
- Connolly, J.M.; Davies, K.; Kazakeviciute, A.; Wheatley, A.M.; Dockery, P.; Keogh, I.; Olivo, M. Non-invasive and label-free detection of oral squamous cell carcinoma using saliva surface-enhanced Raman spectroscopy and multivariate analysis. Nanomedicine 2016, 12, 1593–1601. [Google Scholar] [CrossRef] [PubMed]
- Falamas, A.; Faur, C.I.; Ciupe, S.; Chirila, M.; Rotaru, H.; Hedesiu, M.; Pinzaru, S.C. Rapid and noninvasive diagnosis of oral and oropharyngeal cancer based on micro-Raman and FT-IR spectra of saliva. Spectrochim. Acta A 2021, 252, 119477. [Google Scholar] [CrossRef]
- Sahu, A.; Sawant, S.; Mamgain, H.; Krishna, C.M. Raman spectroscopy of serum: An exploratory study for detection of oral cancers. Analyst 2013, 138, 4161–4174. [Google Scholar] [CrossRef] [PubMed]
- Xue, L.; Yan, B.; Li, Y.; Tan, Y.; Luo, X.; Wang, M. Surface-enhanced Raman spectroscopy of blood serum based on gold nanoparticles for tumor stages detection and histologic grades classification of oral squamous cell carcinoma. Int. J. Nanomed. 2018, 13, 4977–4986. [Google Scholar] [CrossRef] [Green Version]
- Elumalai, B.; Prakasarao, A.; Ganesan, B.; Dornadula, K.; Ganesan, S. Raman spectroscopic characterization of urineof normal and oral cancer subjects. J. Raman Spectrosc. 2015, 46, 84–93. [Google Scholar] [CrossRef]
- Brindha, E.; Rajasekaran, R.; Aruna, P.; Koteeswaran, D.; Ganesan, S. High wavenumber Raman spectroscopy in the characterization of urinary metabolites of normal subjects, oral premalignant and malignant patients. Spectrochim. Acta A 2017, 171, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Jaychandran, S.; Meenapriya, P.K.; Ganesan, S. Raman Spectroscopic Analysis of Blood, Urine, Saliva and Tissue of Oral Potentially Malignant Disorders and Malignancy-A Diagnostic Study. Int. J. Oral Craniofacial Sci. 2016, 2, 011–014. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.P.; Deshmukh, A.; Chaturvedi, P.; Krishna, C.M. In vivo Raman spectroscopic identification of premalignant lesions in oral buccal mucosa. J. Biomed. Opt. 2012, 17, 1050021–1050029. [Google Scholar] [CrossRef]
- Krishna, H.; Majumder, S.K.; Chaturvedi, P.; Sidramesh, M.; Gupta, P.K. In vivo Raman spectroscopy for detection of oral neoplasia: A pilot clinical study. J. Biophotonics 2014, 7, 690–702. [Google Scholar] [CrossRef]
- Guze, K.; Pawluk, H.C.; Short, M.; Zeng, H.; Lorch, J.; Norris, C.; Sonis, S. Pilot study: Raman spectroscopy in differentiating premalignant and malignant oral lesions from normal mucosa and benign lesions in humans. Head Neck 2015, 37, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Teh, S.K.; Zheng, W.; Mo, J.; Lin, K.; Shao, X.; Ho, K.Y.; Teh, M.; Yeoh, K.G. Integrated Raman spectroscopy and trimodal wide-field imaging techniques for real-time in vivo tissue Raman measurements at endoscopy. Opt. Lett. 2009, 34, 758–760. [Google Scholar] [CrossRef]
- Bergholt, M.S.; Lin, K.; Zheng, W.; Lau, D.P.; Huang, Z. In vivo, real-time, transnasal, image-guided Raman endoscopy: Defining spectral properties in the nasopharynx and larynx. J. Biomed. Opt. 2012, 17, 077002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vohra, P.; Strobbia, P.; Ngo, H.T.; Lee, W.T.; Vo-Dinh, T. Rapid Nanophotonics Assay for Head and Neck Cancer Diagnosis. Sci. Rep. 2018, 8, 11410. [Google Scholar] [CrossRef] [PubMed]
- Sahu, A.; Shah, N.; Mahimkar, M.; Garud, M.; Pagare, S.; Nair, S.; Krishna, C.M. Raman spectroscopy and oral exfoliative cytology. Photonic Ther. Diagn. X 2014, 8926. [Google Scholar] [CrossRef]
- Sahu, A.; Tawde, S.; Pai, V.; Gera, P.; Chaturvedi, P.; Nair, S.; Krishna, C.M. Raman spectroscopy and cytopathology of oral exfoliated cells for oral cancer diagnosis. Anal. Methods 2015, 7, 7548–7559. [Google Scholar] [CrossRef]
- Sahu, A.; Gera, P.; Pai, V.; Dubey, A.; Tyagi, G.; Waghmare, M.; Pagare, S.; Mahimkar, M.; Krishna, C.M. Raman exfoliative cytology for oral precancer diagnosis. J. Biomed. Opt. 2017, 22, 115003. [Google Scholar] [CrossRef]
- Sahu, A.; Gera, P.; Malik, A.; Nair, S.; Chaturvedi, P.; Krishna, C.M. Raman exfoliative cytology for prognosis prediction in oral cancers: A proof of concept study. J. Biophotonics 2019, 12, e201800334. [Google Scholar] [CrossRef]
- Hole, A.; Tyagi, G.; Sahu, A.; Shaikh, R.; Krishna, C.M. Exploration of Raman exfoliated cytology for oral and cervical cancers. Vib. Spectrosc. 2018, 98, 35–40. [Google Scholar] [CrossRef]
- Ghosh, A.; Raha, S.; Dey, S.; Chatterjee, K.; Roy Chowdhury, A.; Barui, A. Chemometric analysis of integrated FTIR and Raman spectra obtained by non-invasive exfoliative cytology for the screening of oral cancer. Analyst 2019, 144, 1309–1325. [Google Scholar] [CrossRef] [PubMed]
- Behl, I.; Calado, G.; Malkin, A.; Flint, S.; Galvin, S.; Healy, C.M.; Pimentel, M.L.; Byrne, H.J.; Lyng, F.M. A pilot study for early detection of oral premalignant diseases using oral cytology and Raman micro-spectroscopy: Assessment of confounding factors. J. Biophotonics 2020, 13. [Google Scholar] [CrossRef] [PubMed]
- Barroso, E.M.; Smits, R.W.; Bakker Schut, T.C.; ten Hove, I.; Hardillo, J.A.; Wolvius, E.B.; Baatenburg de Jong, R.J.; Koljenovic, S.; Puppels, G.J. Discrimination between oral cancer and healthy tissue based on water content determined by Raman spectroscopy. Anal. Chem. 2015, 87, 2419–2426. [Google Scholar] [CrossRef]
- Barroso, E.M.; Smits, R.W.; van Lanschot, C.G.; Caspers, P.J.; Ten Hove, I.; Mast, H.; Sewnaik, A.; Hardillo, J.A.; Meeuwis, C.A.; Verdijk, R.; et al. Water Concentration Analysis by Raman Spectroscopy to Determine the Location of the Tumor Border in Oral Cancer Surgery. Cancer Res. 2016, 76, 5945–5953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barroso, E.M.; Ten Hove, I.; Bakker Schut, T.C.; Mast, H.; van Lanschot, C.G.F.; Smits, R.W.H.; Caspers, P.J.; Verdijk, R.; Noordhoek Hegt, V.; Baatenburg de Jong, R.J.; et al. Raman spectroscopy for assessment of bone resection margins in mandibulectomy for oral cavity squamous cell carcinoma. Eur. J. Cancer 2018, 92, 77–87. [Google Scholar] [CrossRef]
- Cals, F.L.; Bakker Schut, T.C.; Hardillo, J.A.; Baatenburg de Jong, R.J.; Koljenovic, S.; Puppels, G.J. Investigation of the potential of Raman spectroscopy for oral cancer detection in surgical margins. Lab. Investig. 2015, 95, 1186–1196. [Google Scholar] [CrossRef] [Green Version]
- Cals, F.L.; Koljenovic, S.; Hardillo, J.A.; Baatenburg de Jong, R.J.; Bakker Schut, T.C.; Puppels, G.J. Development and validation of Raman spectroscopic classification models to discriminate tongue squamous cell carcinoma from non-tumorous tissue. Oral Oncol. 2016, 60, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Hoesli, R.C.; Orringer, D.A.; McHugh, J.B.; Spector, M.E. Coherent Raman Scattering Microscopy for Evaluation of Head and Neck Carcinoma. Otolaryngol. Head Neck Surg. 2017, 157, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, I.C.C.; Aguiar, E.M.G.; Silva, A.T.F.; Santos, L.L.D.; Cardoso-Sousa, L.; Araújo, T.G.; Santos, D.W.; Goulart, L.R.; Sabino-Silva, R.; Maia, Y.C.P. Attenuated Total Reflection-Fourier Transform Infrared (ATR-FTIR) Spectroscopy Analysis of Saliva for Breast Cancer Diagnosis. J. Oncol. 2020, 2020, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zelig, U.; Barlev, E.; Bar, O.; Gross, I.; Flomen, F.; Mordechai, S.; Kapelushnik, J.; Nathan, I.; Kashtan, H.; Wasserberg, N.; et al. Early detection of breast cancer using total biochemical analysis of peripheral blood components: A preliminary study. BMC Cancer 2015, 15, 408. [Google Scholar] [CrossRef] [Green Version]
- Elmi, F.; Movaghar, A.F.; Elmi, M.M.; Alinezhad, H.; Nikbakhsh, N. Application of FT-IR spectroscopy on breast cancer serum analysis. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2017, 187, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Sitnikova, V.E.; Kotkova, M.A.; Nosenko, T.N.; Kotkova, T.N.; Martynova, D.M.; Uspenskaya, M.V. Breast cancer detection by ATR-FTIR spectroscopy of blood serum and multivariate data-analysis. Talanta 2020, 214, 120857. [Google Scholar] [CrossRef]
- Mastanduno, M.A.; Xu, J.; El-Ghussein, F.; Jiang, S.; Yin, H.; Zhao, Y.; Michaelsen, K.E.; Wang, K.; Ren, F.; Pogue, B.W.; et al. Sensitivity of MRI-guided near-infrared spectroscopy clinical breast exam data and its impact on diagnostic performance. Biomed. Opt. Express 2014, 5, 3103–3115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Y.; Lu, Y.; Zhu, Y.; Wu, Y.; Zhai, M.; Wang, X.; Yin, J. Submillimetric FTIR detection of articular cartilage by home-made ATRMIR-Hollow optical fiber probe. Infrared Phys. Technol. 2019, 98, 236–239. [Google Scholar] [CrossRef]
- Lu, Y.; Zhao, Y.; Zhu, Y.; Xu, X.; Yin, J. In situ research and diagnosis of breast cancer by using HOF-ATR-FTIR spectroscopy. Spectrochim. Acta A Mol Biomol. Spectrosc. 2020, 235, 118178. [Google Scholar] [CrossRef]
- Tian, P.; Zhang, W.; Zhao, H.; Lei, Y.; Cui, L.; Zhang, Y.; Xu, Z. Intraoperative detection of sentinel lymph node metastases in breast carcinoma by Fourier transform infrared spectroscopy. Br. J. Surg. 2015, 102, 1372–1379. [Google Scholar] [CrossRef]
- Tian, P.; Zhang, W.; Zhao, H.; Lei, Y.; Cui, L.; Wang, W.; Li, Q.; Zhu, Q.; Zhang, Y.; Xu, Z. Intraoperative diagnosis of benign and malignant breast tissues by fourier transform infrared spectroscopy and support vector machine classification. Int. J. Clin. Exp. Med. 2015, 8, 972–981. [Google Scholar]
- Zlotogorski-Hurvitz, A.; Dekel, B.Z.; Malonek, D.; Yahalom, R.; Vered, M. FTIR-based spectrum of salivary exosomes coupled with computational-aided discriminating analysis in the diagnosis of oral cancer. J. Cancer Res. Clin. Oncol. 2019, 145, 685–694. [Google Scholar] [CrossRef]
- Rai, V.; Mukherjee, R.; Routray, A.; Ghosh, A.K.; Roy, S.; Ghosh, B.P.; Mandal, P.B.; Bose, S.; Chakraborty, C. Serum-based diagnostic prediction of oral submucous fibrosis using FTIR spectrometry. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2018, 189, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Townsend, D.; Miljkovic, M.; Bird, B.; Lenau, K.; Old, O.; Almond, M.; Kendall, C.; Lloyd, G.; Shepherd, N.; Barr, H.; et al. Infrared micro-spectroscopy for cyto-pathological classification of esophageal cells. Analyst 2015, 140, 2215–2223. [Google Scholar] [CrossRef]
- Faoláin, E.Ó.; Hunter, M.B.; Byrne, J.M.; Kelehan, P.; McNamara, M.; Byrne, H.J.; Lyng, F.M. A study examining the effects of tissue processing on human tissue sections using vibrational spectroscopy. Vib. Spectrosc. 2005, 38, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Mian, S.A.; Colley, H.E.; Thornhill, M.H.; Rehman, I.u. Development of a Dewaxing Protocol for Tissue-Engineered Models of the Oral Mucosa Used for Raman Spectroscopic Analysis. Appl. Spectrosc. Rev. 2014, 49, 614–617. [Google Scholar] [CrossRef]
- Al Jedani, S.; Smith, C.I.; Gunning, P.; Ellis, B.G.; Gardner, P.; Barrett, S.D.; Triantafyllou, A.; Risk, J.M.; Weightman, P. A de-waxing methodology for scanning probe microscopy. Anal. Methods 2020, 12, 3397–3403. [Google Scholar] [CrossRef] [PubMed]
- Zohdi, V.; Whelan, D.R.; Wood, B.R.; Pearson, J.T.; Bambery, K.R.; Black, M.J. Importance of tissue preparation methods in FTIR micro-spectroscopical analysis of biological tissues: ‘traps for new users’. PLoS ONE 2015, 10, e0116491. [Google Scholar] [CrossRef] [Green Version]
- Meksiarun, P.; Ishigaki, M.; Huck-Pezzei, V.A.; Huck, C.W.; Wongravee, K.; Sato, H.; Ozaki, Y. Comparison of multivariate analysis methods for extracting the paraffin component from the paraffin-embedded cancer tissue spectra for Raman imaging. Sci. Rep. 2017, 7, 44890. [Google Scholar] [CrossRef] [Green Version]
- Tfayli, A.; Gobinet, C.; Vrabie, V.; Huez, R.; Manfait, M.; Piot, O. Digital dewaxing of Raman signals: Discrimination between nevi and melanoma spectra obtained from paraffin-embedded skin biopsies. Appl. Spectrosc. 2009, 63, 564–570. [Google Scholar] [CrossRef]
- De Lima, F.A.; Gobinet, C.; Sockalingum, G.; Garcia, S.B.; Manfait, M.; Untereiner, V.; Piot, O.; Bachmann, L. Digital de-waxing on FTIR images. Analyst 2017, 142, 1358–1370. [Google Scholar] [CrossRef]
- Vanna, R.; Morasso, C.; Marcinno, B.; Piccotti, F.; Torti, E.; Altamura, D.; Albasini, S.; Agozzino, M.; Villani, L.; Sorrentino, L.; et al. Raman Spectroscopy Reveals That Biochemical Composition of Breast Microcalcifications Correlates with Histopathologic Features. Cancer Res. 2020, 80, 1762–1772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyng, F.M.; Traynor, D.; Nguyen, T.N.Q.; Meade, A.D.; Rakib, F.; Al-Saady, R.; Goormaghtigh, E.; Al-Saad, K.; Ali, M.H. Discrimination of breast cancer from benign tumours using Raman spectroscopy. PLoS ONE 2019, 14, e0212376. [Google Scholar] [CrossRef]
- Verdonck, M.; Denayer, A.; Delvaux, B.; Garaud, S.; De Wind, R.; Desmedt, C.; Sotiriou, C.; Willard-Gallo, K.; Goormaghtigh, E. Characterization of human breast cancer tissues by infrared imaging. Analyst 2016, 141, 606–619. [Google Scholar] [CrossRef] [PubMed]
- Lazaro-Pacheco, D.; Shaaban, A.; Baldwin, G.; Titiloye, A.N.; Rehman, S.; Rehman, I. Deciphering the structural and chemical composition of breast cancer using FTIR spectroscopy. Appl. Spectrosc. Rev. 2020, 1–15. [Google Scholar] [CrossRef]
- Pounder, F.N.; Reddy, R.K.; Bhargava, R. Development of a practical spatial-spectral analysis protocol for breast histopathology using Fourier transform infrared spectroscopic imaging. Faraday Discuss. 2016, 187, 43–68. [Google Scholar] [CrossRef] [Green Version]
- Tang, J.; Kurfürstová, D.; Gardner, P. Breast cancer detection using infrared spectral pathology from H&E stained tissue on glass slides. Clin. Spectrosc. 2021, 3, 1–6. [Google Scholar] [CrossRef]
- Ibrahim, O.; Toner, M.; Flint, S.; Byrne, H.J.; Lyng, F.M. The Potential of Raman Spectroscopy in the Diagnosis of Dysplastic and Malignant Oral Lesions. Cancers 2021, 13, 619. [Google Scholar] [CrossRef]
- Devpura, S.; Thakur, J.S.; Sethi, S.; Naik, V.M.; Naik, R. Diagnosis of head and neck squamous cell carcinoma using Raman spectroscopy: Tongue tissues. J. Raman Spectrosc. 2012, 43, 490–496. [Google Scholar] [CrossRef]
- Pallua, J.D.; Pezzei, C.; Zelger, B.; Schaefer, G.; Bittner, L.K.; Huck-Pezzei, V.A.; Schoenbichler, S.A.; Hahn, H.; Kloss-Brandstaetter, A.; Kloss, F.; et al. Fourier transform infrared imaging analysis in discrimination studies of squamous cell carcinoma. Analyst 2012, 137, 3965–3974. [Google Scholar] [CrossRef]
- Pilling, M.J.; Henderson, A.; Shanks, J.H.; Brown, M.D.; Clarke, N.W.; Gardner, P. Infrared spectral histopathology using haematoxylin and eosin (H&E) stained glass slides: A major step forward towards clinical translation. Analyst 2017, 142, 1258–1268. [Google Scholar] [CrossRef] [Green Version]
- Baker, M.J.; Trevisan, J.; Bassan, P.; Bhargava, R.; Butler, H.J.; Dorling, K.M.; Fielden, P.R.; Fogarty, S.W.; Fullwood, N.J.; Heys, K.A.; et al. Using Fourier transform IR spectroscopy to analyze biological materials. Nat. Protoc. 2014, 9, 1771–1791. [Google Scholar] [CrossRef] [Green Version]
- Butler, H.J.; Ashton, L.; Bird, B.; Cinque, G.; Curtis, K.; Dorney, J.; Esmonde-White, K.; Fullwood, N.J.; Gardner, B.; Martin-Hirsch, P.L.; et al. Using Raman spectroscopy to characterize biological materials. Nat. Protoc. 2016, 11, 664–687. [Google Scholar] [CrossRef] [Green Version]
- Morais, C.L.M.; Lima, K.M.G.; Singh, M.; Martin, F.L. Tutorial: Multivariate classification for vibrational spectroscopy in biological samples. Nat. Protoc. 2020, 15, 2143–2162. [Google Scholar] [CrossRef]
- Traynor, D.; Behl, I.; O’Dea, D.; Bonnier, F.; Nicholson, S.; O’Connell, F.; Maguire, A.; Flint, S.; Galvin, S.; Healy, C.M.; et al. Raman spectral cytopathology for cancer diagnostic applications. Nat. Protoc. 2021, 16, 3716–3735. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Early Diagnosis | ||||||||
|---|---|---|---|---|---|---|---|---|
| Reference | Sample | Sample Preparation | Methodology | Depth | Specificity (%) | Sensitivity (%) | Accuracy (%) | Observations |
| Cervo et al. [93] | Human blood serum (BC patients) | - | SERS | 85 | 92 | 90 | Localised and locally advanced breast cancer distinguished with 84% accuracy | |
| Nargis et al. [94] | Human blood serum (BC patients) | - | SERS | - | 100 | 99 | - | - |
| Nargis et al. [95] | Human blood serum (BC patients) | - | SERS | - | 98.4 | 90 | - | |
| microRamn | 97.7 | 88.2 | ||||||
| Moisoiu et al. [96] | Human blood serum (cancer patients) | - | SERS | - | 93.6 | 93.7 | - | BC was differentiated from lung, colorectal, oral and ovarian cancer with 76% accuracy |
| Moisoiu et al. [97] | Human urine (BC patients) | - | SERS | - | 95 | 81 | 88 | - |
| Lin et al. [98] | Human urine (cancer patients) | Filtration through affinity chromatography | SERS | - | 87.5 | 76.5 | - | BC was distinguished from gastric cancer with 82% sensitivity and 90.7% specificity |
| Nicolson et al. [99] | Breast cells | Incubation with nanotags | SESORRS | 10 mm | - | - | - | 3D multicellular cell spheroids |
| Nicolson et al. [100] | Breast cells | Incubation with nanotags | SESORRS | 15 mm | - | - | - | 3D multicellular cell spheroids |
| Nicolson et al. [101] | Mice brain | Injection of Functionalised nanoparticles | SESORS | Through the mice skull | - | - | - | Animal models, in vivo |
| Desroches et al. [103] | Human brain | Intraoperatively | Adaptation of core-needle instrument | - | 90 | 80 | 84 | Clinical trial, in vivo |
| Saha et al. [104] | Human breast | Fresh | Portable spectroscopy system | - | 97 | 77 | - | - |
| Barman et al. [106] | Human breast | Fresh | Portable spectroscopy system | - | - | - | 82 | |
| Connolly et al. [117] | Saliva from HNC patients | - | SERS | - | 57 | 89 | - | - |
| Oral cells from HNC patients | 52 | 68 | - | |||||
| Falamas et al. [118] | Saliva from HNC patients | Liophilised | microRaman | - | - | Seven bands with discriminatorypotential were identified with 83% accuracy. | ||
| Sahu et al. [119] | Blood serum (HNC patients) | - | microRaman | - | - | 78% efficiency | ||
| Xue et al. [120] | Blood serum (HNC patients) | - | SERS | - | - | T1 and T3 OSCC distinguished with 80% accuracy, T2 and T4 with 71.1% and 77.8% accuracy, respectively. N0, N1 and N2 distinguished with 75.5%, 93.8% and 92%, respectively. | ||
| Brindha et al. [121] | Human urine (HNC patients) | - | microRaman | - | 87.1 | 98.6 | 93.7 | - |
| Brindha et al. [122] | Human urine (HNC patients) | - | microRaman | - | 98.7 | 91.9 | - | Only the high wavenumber region was used. Achieving higher classification accuracies. |
| Jaychandra et al. [123] | Human urine (HNC patients) | - | microRaman | - | - | - | 90.5 | Malignant, pre-malignant and healthy samples were tested |
| Human saliva (HNC patients) | - | - | 93.1 | |||||
| Blood serum (HNC patients) | - | - | - | 78 | ||||
| Biopsy-collected tissue | - | - | - | 97.4 | ||||
| Singh et al. [124] | HNC patients | In vivo | Fire-optic probe coupled to a spectrometer | - | Healthy controls, healthy tobacco users and pre-malignant samples were correctly predicted with 94%, 86% and 55% efficiency, respectively | |||
| Krishna et al. [125] | HNC patients | In vivo | Portable Raman device | - | 94 | 94 | - | Pre-malignant lesions were correctly classified in 88% of the measured sites and malignant lesions in 84% of the sites. |
| Guze et al. [126] | Oral abnormalities | In vivo– mimicking a clinical setting | Raman probe | - | 77 | 100 | - | - |
| Bergholt et al. [128] | Transnasal tissues | In vivo | Raman probe–possible integration with endoscopes | - | - | The spectra from different areas of the head and neck obtained and characterised. | ||
| Vohra et al. [129] | RNA from HNSCC | Fresh | SERS | - | 89 | 100 | - | - |
| RNA from Lymph nodes | ||||||||
| Sahu et al. [130,131,132,133] | Exfoliated cells (HNC patients) | Cell pellets, placed on CaF2 | Fibre optic Raman microprobe | - | - | 70 | - | A spectra-wise analysis of the data provided a sensitivity of 77% |
| Hole et al. [134] | Exfoliated cells (HNC patients) | Cell pellets, placed on CaF2 | Fibre optic Raman microprobe | - | - | - | - | Classification efficiency of 86% |
| Ghosh et al. [135] | Exfoliated cells (HNC patients) | Suspension of cells | microRaman | - | - | - | 80 | A spectra-wise analysis of the data provided a sensitivity of 82% |
| Behl et al. [136] | Exfoliated cells (HNC patients) | Monolayer of cells placed on glass slides | microRaman | - | - | 94 | - | Analysing the cells’ nuclei |
| - | - | 86 | - | Analysing the cells’ cytoplasm | ||||
| Surgical Margins Assessment | ||||||||
| Reference | Sample | Sample preparation | Methodology | Acquisition time | Specificity (%) | Sensitivity (%) | Accuracy (%) | Observations |
| Koya et al. [106] | Human breast | Frozen sections | microRaman | - | 90.8 | 88.8 | 90 | - |
| Kong et al. [107] | Human breast | Frozen sections | microRaman | - | 96.2 | 95.6 | - | |
| MSH | 17 min | |||||||
| Shipp et al. [108] | Human breast | Fresh | MSH | 12–24 min | 82 | 95 | - | - |
| Lizio et al. [109] | Human breast | Fresh | MSH (using TIR-AF) | 45 min (possible reduction to 20 min) | - | H&E in agreement with Raman heatmaps. | ||
| Liao et al. [110] | Human breast | Fresh | Altered Raman spectrometer | 20–25 min | - | H&E in agreement with Raman heatmaps. | ||
| Thomas et al. [111] | Human breast | Fresh | Raman 3D scanner | 7–15 min | 85 | 93 | - | - |
| Keller et al. [112] | Human breast | Frozen | SORS probe | - | 100 | 95 | - | |
| Wang et al. [113] | Human breast | Fresh | SERS | 10–15 min | 92.1 | 89.3 | - | |
| Horsnell et al. [114] | Human lymph nodes (breast surgery) | Frozen | microRaman | - | 97 | 81 | - | |
| Petterson et al. [115] | Human lymph node | Fresh | Multifibre Raman probe in a hypodermic needle | Some seconds | - | Spectra with good signal to noise obtained. | ||
| Zúñiga et al. [116] | Human breast | Frozen | Portable and commercially available Raman devices | - | - | - | > 90 | - |
| Barroso et al. [137] | SCC of the tongue | Fresh | Built in Raman equipment | Within 30 min after excision | 92 | 99 | - | |
| Barroso et al. [138] | Oral SCC | Fresh | Built in Raman equipment | Within 30 min after excision | - | Water concentration in the tumour was found to be 76% ± 8% and, 56% ± 24% in the surrounding healthy tissue | ||
| Barroso et al. [139] | Oral SCC—bone | Fresh | Built in Raman equipment | <30 min | 87 | 95 | 95 | - |
| Cals et al. [140] | Oral SCC | Frozen | Inverted microRaman | Within 60 min after excision | - | - | 97 | |
| Cals et al. [141] | SCC of the tongue | Frozen | Inverted microRaman | Too long for clinical application | 78 | 100 | 91 | |
| 66 | 100 | 86 | ||||||
| Hoesli et al. [142] | Human head and neck | Frozen | CRS | - | - | H&E in agreement with Raman heatmaps | ||
| Early Diagnosis | |||||||
|---|---|---|---|---|---|---|---|
| Reference | Sample | Sample Preparation | Methodology | Specificity (%) | Sensitivity (%) | Accuracy (%) | Observations |
| Ferreira et al. [143] | Saliva (BC patients) | Lyophilised | ATR | 70 | 90 | - | - |
| Zelig et al. [144] | Blood serum and peripheral mononuclear cells (BC patients) | Air dried on ZnSe slides | microFTIR | 78 | 87 | ||
| Elmi et al. [145] | Blood serum (BC patients) | Dry at room temperature | ATR | 85 | 92 | 90 | |
| Sitnikova et al. [146] | Blood serum (BC patients) | Dry at room temperature | ATR | 87.1 | 92.3 | - | |
| Mastanduno et al. [147] | BC patients | In vivo | MRI-NIRS | - | Successful identification of malignant apart from benign lesions. | ||
| Zlotogorski-Hurvitz et al. [152] | Exossomes from the saliva of HNC patients | Dry at room temperature | ATR | 89 | 100 | 95 | - |
| Falamas et al. [118] | Saliva from HNC patients | Dry on KBr tablets | FTIR, transmission mode | - | Three main signals found to be biomarkers with 82% accuracy. | ||
| Rai et al. [153] | Bold serum from OSF patients | Dried under vacuum | TR-FTIR | - | Predictive capability and explained variance higher than 0.9. | ||
| Townsend et al. [154] | Exfoliated cells (HNC patients) | Cell pellets, placed on low-e slides | microFTIR, in reflection mode | >90 | |||
| Ghosh et al. [135] | Exfoliated cells (HNC patients) | Suspension of cells | ATR | >80 | The integrated approach of both Raman and FTIR provided an overall accuracy of 97.7% | ||
| Surgical Margins Assessment | |||||||
| Reference | Sample | Sample preparation | Methodology | Specificity (%) | Sensitivity (%) | Accuracy (%) | Observations |
| Lu et al. [149] | Human breast | Fresh | ATR-HOF | - | - | >90 | - |
| Tian et al. [150] | Sentinel lymph nodes from BC patients | Fresh | ATR-HOF | 90.1 | 94.7 | - | |
| Tian et al. [151] | Human breast | Fresh | ATR-HOF | 98 | 90 | - | |
| Spectral Histopathology | |||||||
|---|---|---|---|---|---|---|---|
| Reference | Sample | Sample Preparation | Methodology | Specificity (%) | Sensitivity (%) | Accuracy (%) | Observations |
| Vanna et al. [162] | Human breast | Chemical dewax | microRaman | 80.6 | 93.5 | - | - |
| Lyng et al. [163] | Human breast | Chemical dewax | microRaman | >90 | >90 | - | |
| Verdonck et al. [164] | Human breast | Chemical dewax, on BaF2 slides | microFTIR | >90 | >80 | - | |
| Lazaro-Pacheco et al. [165] | Human breast | Chemical dewax, on CaF2 slides | microFTIR | 86 | 92 | - | |
| Pounder et al. [166] | Human breast | Chemical dewax, on BaF2 slides | microFTIR | - | Area under the ROC curve >0.9 for both transmission and reflection acquisition modes | ||
| Tang et al. [167] | Human breast | H&E stained, on standard histological glass | microFTIR | - | - | 95.8 | Cancerous vs. healthy stroma classified with >90% accuracy; healthy epithelium and cancerous epithelium classified with 73% and 88% accuracy, respectively. |
| Bassan et al. [21] | Human breast | Chemical dewax, on standard histological slides | microFTIR | - | Epithelium, stroma, blood and necrosis correctly classified in 98.25%, 99.94%, 100% and 97.22%, respectively, of the cases | ||
| Ibrahim et al. [168] | Human head and neck | FFPE samples, digitally dewaxed | microRaman | - | Inflammation and smoking factors successfully classified with 94% and 76% accuracy, respectively. | ||
| Devpura et al. [169] | Human head and neck | Chemical dewax | microRaman | - | - | 89 | - |
| Pallua et al. [170] | Oral SCC | Chemical dewax, on CaF2 slides | microFTIR | - | H&E in agreement with FTIR heatmaps | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mamede, A.P.; Santos, I.P.; Batista de Carvalho, A.L.M.; Figueiredo, P.; Silva, M.C.; Tavares, M.V.; Marques, M.P.M.; Batista de Carvalho, L.A.E. A New Look into Cancer—A Review on the Contribution of Vibrational Spectroscopy on Early Diagnosis and Surgery Guidance. Cancers 2021, 13, 5336. https://doi.org/10.3390/cancers13215336
Mamede AP, Santos IP, Batista de Carvalho ALM, Figueiredo P, Silva MC, Tavares MV, Marques MPM, Batista de Carvalho LAE. A New Look into Cancer—A Review on the Contribution of Vibrational Spectroscopy on Early Diagnosis and Surgery Guidance. Cancers. 2021; 13(21):5336. https://doi.org/10.3390/cancers13215336
Chicago/Turabian StyleMamede, Adriana P., Inês P. Santos, Ana L. M. Batista de Carvalho, Paulo Figueiredo, Maria C. Silva, Mariana V. Tavares, Maria P. M. Marques, and Luís A. E. Batista de Carvalho. 2021. "A New Look into Cancer—A Review on the Contribution of Vibrational Spectroscopy on Early Diagnosis and Surgery Guidance" Cancers 13, no. 21: 5336. https://doi.org/10.3390/cancers13215336