1. Introduction
Cutaneous malignant melanoma is on the rise and has the highest mortality rate among the various types of skin cancer [
1]. For example, in 2021, it is estimated that 106,110 new cases of melanoma will be diagnosed in the United States, resulting in 7180 deaths (
https://www.cancer.org, accessed on 1 June 2021). Surgery is the primary treatment for this type of cancer, but in its more advanced stages, treatment can also include immunotherapy, targeted therapy drugs and radiation to extend survival. Accordingly, the development of modern tools is critical for diagnosing melanoma at an earlier stage, thus easing the decision-making process for dermatologists and reducing invasive treatments for patients, in addition to associated costs. The diagnosis of melanoma is, however, a complex task even for expert dermatologists, mainly because of the complexity, variability and ambiguity of symptoms [
2]. Additionally, an extensive variety of morphologies exist even between samples from the same category, which greatly hampers diagnosis. Several studies have shown that the early diagnosis of melanoma can greatly benefit from computational methods [
3], demonstrating that such techniques may even outperform dermatologists in terms of diagnosis [
4], due to various machine learning techniques and learning of data-driven features for specific tasks [
5]. The early proposed methods required the previous extraction of handcrafted features, thus relying on the level of dermatologists’ expertise to extract high quality descriptors. This extraction process of informative and discriminative sets of high-level features, however, remains as a complex and costly task that is usually problem dependent [
6], and it is noteworthy that sometime is impossible to derive invariant features which are independent of the differences in the input images [
7]. On the other hand, there is another type of computational method which can automatically extract and learn high-level features [
8], providing a higher robustness to the inter- and intra-class variability present in melanoma images [
8,
9].
Deep learning models, specifically Convolutional Neural Network (CNN) models, have the capacity of automatically learning high-level features from raw images [
8,
10,
11]. The ImageNet Challenge (ILSVRC) takes place every year since 2010. In 2012 a CNN won the contest for the first time, which increased the popularity of such models for image processing [
12]. CNN models learn automatically abstract features and enable the learning for several tasks. For example, Pérez et al. [
13] summarized the most popular techniques used in CNN models for diagnosing skin images. Furthermore, this type of deep model can extract sets of patterns ranging from single edges and curves to more complex patterns such as a human face. On the other hand, the main downside of CNN models is that the information regarding spatial relationships between extracted features is lost. For example, CNN models could consider two images to be similar if they share the same objects, even if the location within the image is relevant. However, convolution operation is not translation-invariant.
To overcome the above main limitation of CNN models, a new type of deep learning model, named Dynamic Routing Between Capsules (well-know as CapsNet), was proposed in [
14], where the authors designed a method closer to how human vision works. The neurons in this architecture can represent properties of a object such as position, size and texture. Moreover, CapsNet is able to preserve hierarchical spatial relationships, and in theory it could be as effective as any CNN but using fewer samples for training [
14]. Niyaz et al. [
15] reviewed several deep learning methods for the prediction of different types of cancer. In that time the authors did not find evidence of the application of CapsNet in cancer diagnosis. However, the authors acknowledged CapsNet as a promising model for diagnosing cancer and encouraged its application. Accordingly, CapsNet has been applied in medical image analysis, demonstrating to be really effective for lung cancer screening [
16], blood cell image classification [
17], and cervical image classification [
18], to list a few applications. Finally, CapsNet have been recently applied in skin cancer classification. Cruz et al. [
19] used CapsNet to classify skin lesions using images and evaluated their proposal in only one recognized dataset, HAM10000 [
20]. However, to our understanding, the proposal has several issues. Firstly, although skin images are usually high-quality (
in HAM10000), the authors resized images to
, losing a considerable amount of pixels and even ignoring colors in the images, which is important for the diagnosis of melanoma [
21]. Secondly, the authors highlighted their performance relying mainly on overall precision. However, it is well-known that skin images datasets are unbalanced. Looking closely, the authors achieved only a precision of 28% and 41% in melanoma and basal cell carcinoma categories, respectively, leaving open a big margin of improvement.
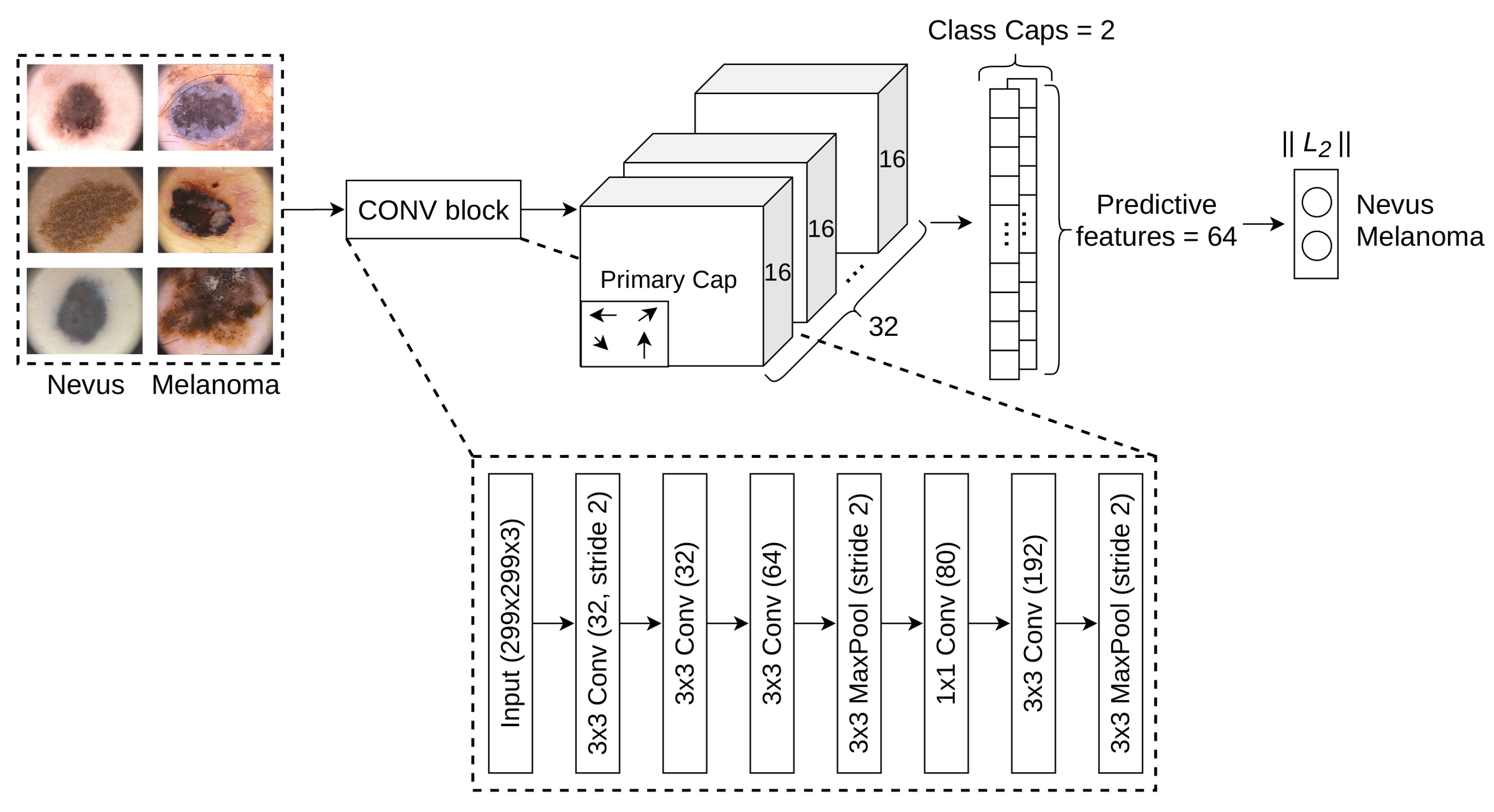
Consequently, this work focuses on assessing the effectiveness of a new architecture for the diagnosis of melanoma. The architecture uses high-quality
skin lesion images and achieves an acceptable performance in both normal and malignant categories. The proposed architecture combines features from convolutional blocks and CapsNet. First, we selected a more sophisticated convolutional computational block, allowing for the extraction of more useful initial features. Second, we replaced the first convolutional block from CapsNet with the above computational block. As a result, we are able to extract more significant features from earlier stages. Next, primary caps extract geometric and color properties present in the images, such as asymmetry, border irregularity, color variegation and the positions of various zones. These have all proven to be very useful attributes to consider when diagnosing melanoma [
21]. In this manner, we can maintain the hierarchical spatial relationships of patterns which yields great benefit. To take full advantage of the architecture, we proposes a hyper-tuning of the main parameters to ensure effective training and learning under limited training data. In addition, the architecture applies data augmentation to enhance the diagnosis of melanoma, significantly increasing the validity of the proposal. The new architecture enables the construction of a transformation-invariant model and the detection of spatial hierarchies between entities within an image. As such, it is more suitable for solving certain real-world situations than convolutional models. To evaluate the suitability of the proposal, an extensive experimental study was conducted on eleven public skin image datasets, allowing for a better analysis of the model’s effectiveness. The results showed that the proposed approach achieved very promising results and was competitive with respect to state-of-the-art CNN models which have previously been used in the diagnosis of melanoma. Finally, Shapley Additive Explanations method (SHAP (
https://github.com/slundberg/shap, accessed on 1 September 2019)) [
22] and Local Interpretable Model-agnostic Explanations (LIME) [
23] were used to show the most important features and give a prediction with a high confidence level. This work, to the best of our knowledge, is the first attempt to thoroughly assess a new architecture based on convolutional blocks and CapsNet for the automatic recognition of melanoma. The hyper-parameters were specifically tuned for the selected task, achieving significantly better performance compared to the state-of-the-art models.
The rest of this work is arranged as follows:
Section 2 briefly presents the state-of-the-art in solving the melanoma diagnosis problem mainly by using CNN models;
Section 3 presents the proposed architecture;
Section 4 presents the experimental study carried out, showing the results and a discussion of them; finally, some concluding remarks are presented in
Section 5.
2. Related Works
CNN models have proven to be a powerful classification method for melanoma diagnosis [
8]. This type of models presents a higher suitability compared to classic methods which depend on hand-crafted features. In addition, sophisticated techniques can be applied to even improve the performance of CNN models in the task of melanoma diagnosis, e.g., by applying data augmentation [
24] and transfer learning techniques [
8].
Data augmentation is a common technique applied to reduce overfitting on CNN models [
25]. It is commonly performed by means of applying random transformations on the source images [
26]. In addition, this technique can be used to tackle imbalance problems [
27,
28]. For example, Hossain and Muhammad [
29] proposed an emotion recognition system using a CNN approach from emotional Big Data. The models trained with augmented data obtained better performance compared to its non-use. In addition, Esteva et al. [
8] applied extensive data augmentation techniques during training; the authors increased the number of images by a factor of 720. Each image was randomly rotated, flipped and cropped. The results achieved a performance comparable to a committee of 21 dermatologists. On the other hand, more advanced techniques such as GANs are being applied to augment data [
30]. GANs can augment a dataset by training simultaneously two models, a generator that creates new samples by randomly selecting points from the latent space, and a discriminator that determines whether a sample is a fake or not. Frid-Adar et al. [
31] proposed methods based on GANs for generating synthetic medical images; their proposal was evaluated on a limited dataset of high quality liver lesion computed tomography. The results showed that the model increased both sensitivity and specificity by using augmented data.
Transfer learning is a technique widely used to increase performance when the number of training examples is limited [
32,
33]. This method transfers and reuses knowledge that was learned from a source task, where a lot of data is commonly available, e.g., the ImageNet dataset with more than one million of images. For instance, Esteva et al. [
8] transferred the knowledge learned by InceptionV3 on ImageNet and applied it to melanoma diagnosis. Moreover, Nasr-Esfahani et al. [
34] applied a pre-trained CNN to distinguishes between melanoma and nevus cases. The results showed that the proposed method is superior in terms of diagnostic accuracy in comparison with the state-of-the-art methods. Finally, Saba et al. [
35] proposed an automated approach for skin lesion detection and recognition using Laplacian filtering, lesion boundary extraction and CNN. The results outperformed several existing methods and attained a high accuracy value.
On the other hand, CapsNet represents a completely novel type of deep learning architectures which attempt to overcome the limits and drawbacks of CNN models. Since CapsNet was recently proposed, only a few studies have explored its applications. Zhang et al. [
18] applied CapsNet to classify the images of cervical lesions. The results showed better performance compared to other classification methods. Mobiny et al. [
16] proposed an improvement on CapsNet that speedup the results compared to the original architecture. After evaluating the performance on computed tomography chest scans, the results showed that CapsNet is a promising alternative to CNN. Zhang et al. [
36] combined CapsNet and fully CNN models in image scene classification, such as VGG16 and InceptionV3. The authors achieved better output compared to state-of-the-art methods. However, it is said that the use of a full CNN model could hamper the main aim behind CapsNet, which is the extraction of spatial hierarchies between entities. In addition, the number of trainable parameters significantly increases by combining such architectures. By demonstrating the benefits of CapsNet in medical imaging in this work, we may be encouraging its wider use. Considering the above, it would be interesting to design a deep learning architecture that combines and leverages features from different approaches such as data augmentation, transfer learning, convolutional blocks and CapsNet. After analyzing CapsNet, we strongly believe that specific blocks could be improved while maintaining their behavior. To augment data, it is important to perform a data augmentation both on training and test phases [
24]. Next, the proposal for melanoma diagnosis, which follows the mentioned approximation, is described.
5. Conclusions
In this work, a novel neural network architecture for diagnosing melanoma has been proposed, allowing the early extraction of richer abstract features before passing them to deeper layers. The use of CapsNet combined with convolutional blocks allowed a better learning of the representations. By this way, better predictive features could be extracted, thus facilitating the learning of better abstract and discriminative features for melanoma diagnosis. The proposed architecture is flexible regarding the design of its blocks. Consequently, custom networks could easily be designed, for example by employing another convolutional block with a simpler or more complex internal structure. Moreover, the predictive features from CapsNet could be used to feed other well-known models, such as Support Vector Machine, which has proven to achieve high performance [
69]. The results corroborated that data augmentation and transfer learning are suitable techniques to improve the proposal and all studied CNN models, overcoming common issues in melanoma diagnosis, such as small datasets and imbalance data. Finally, the proposed model significantly outperformed state-of-the-art CNN models that haven previously been applied for solving melanoma diagnosis problem, confirming the potential that possess this novel neural network architecture.
The research on CapsNet is still at early stage and, therefore, few application on real-world problems can be found so far. Consequently, more research and extensive experimental study should be conducted in order to demonstrate and confirm the full potential of this neural network architecture. As future works, we will also design ensemble learning techniques for a better application in small and medium problems. Finally, we encourage further development of the research line that combines the proposal and other CNN models for a better melanoma diagnosis.




{kind=link}
{kind=link}

