
The Survival Benefit of Chemoradiotherapy following Induction Chemotherapy with Gemcitabine Plus Nab-Paclitaxel for Unresectable Locally Advanced Pancreatic Cancer

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Treatment
2.2. Evaluation of Treatment Outcomes and Adverse Events
2.3. Statistical Analysis
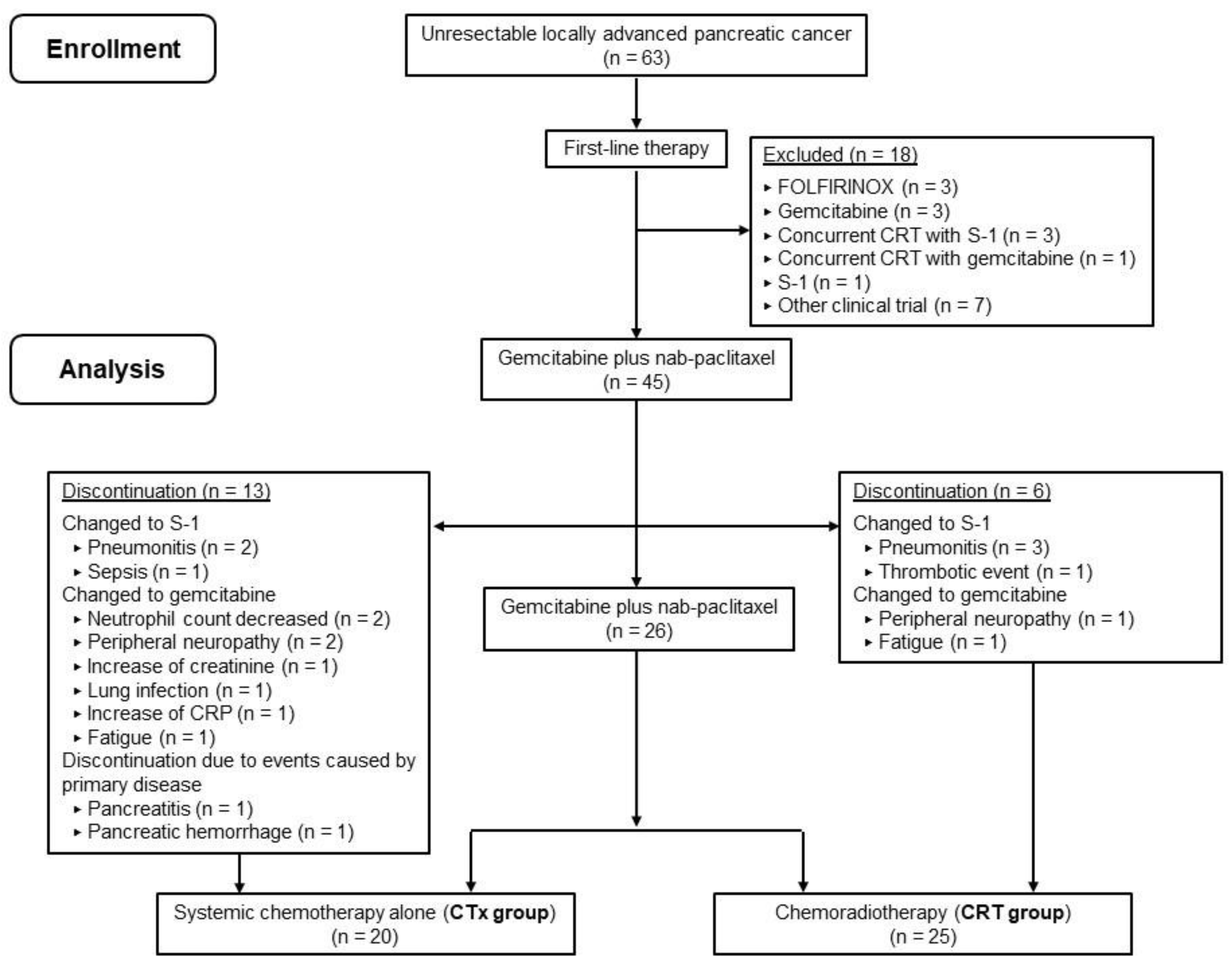
3. Results
3.1. Patient Characteristics
3.2. Treatment Outcomes and AEs
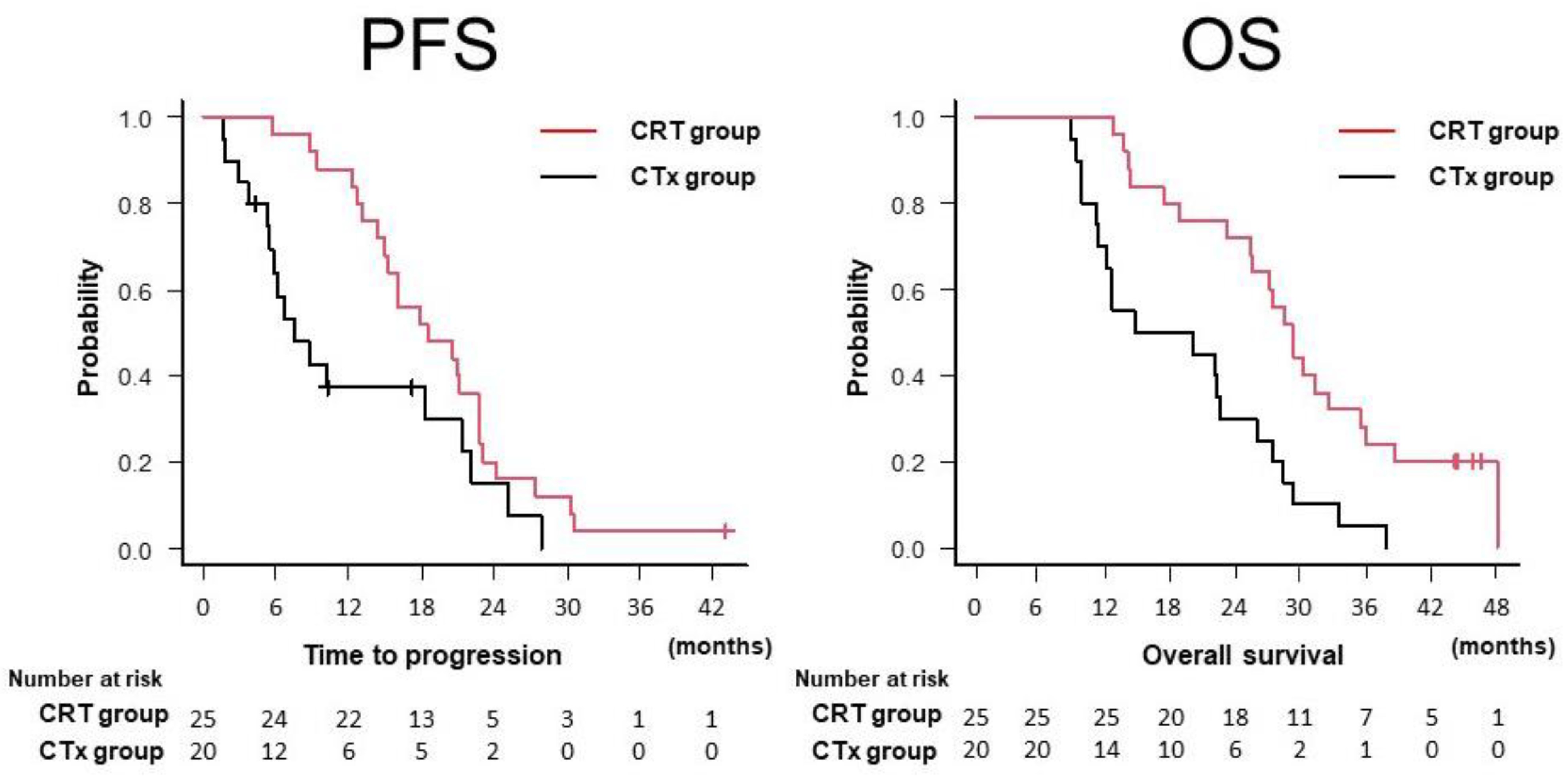
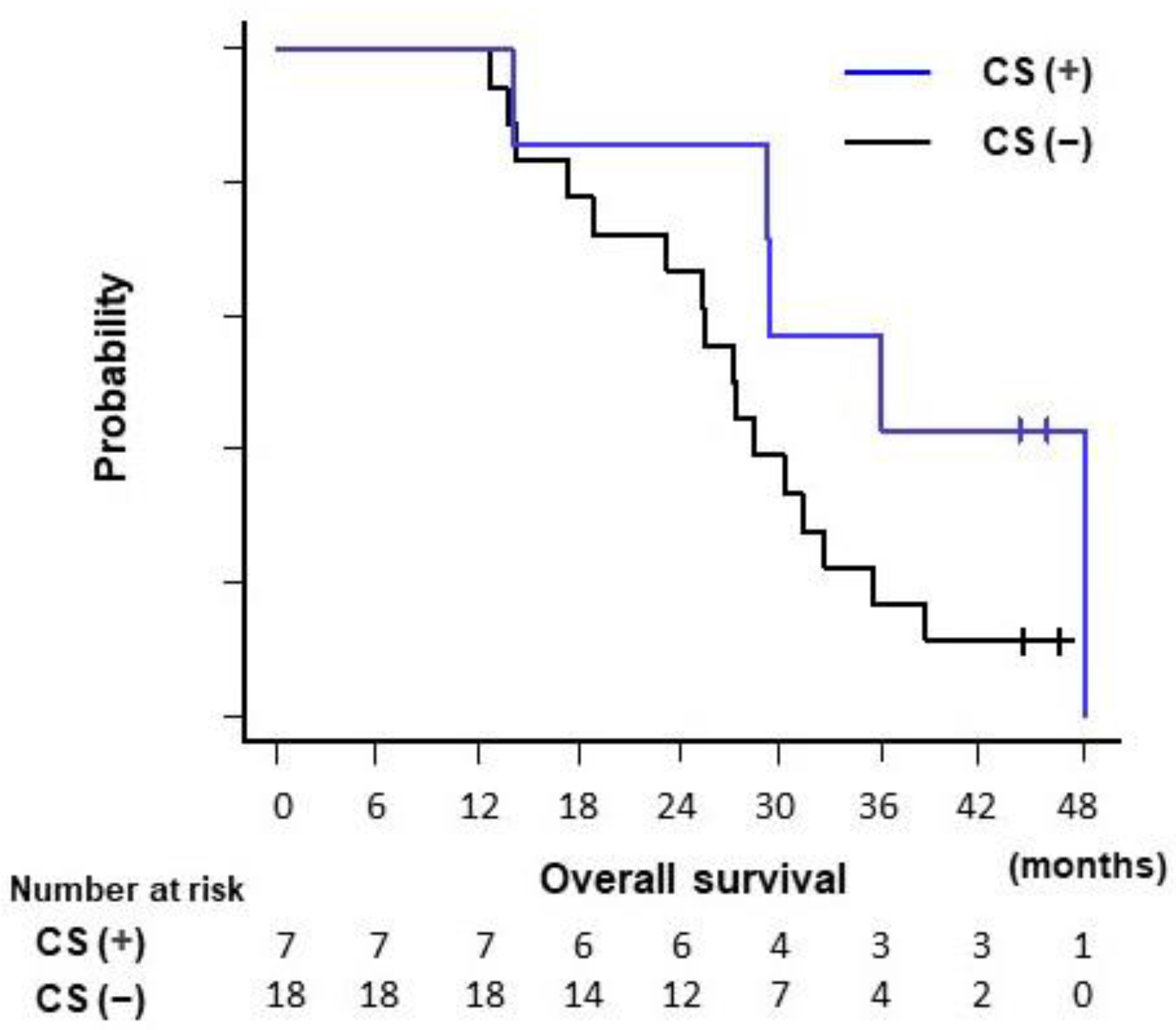
3.3. Survival and Disease Progression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Franck, C.; Müller, C.; Rosania, R.; Croner, R.S.; Pech, M.; Venerito, M. Advanced pancreatic ductal adenocarcinoma: Moving forward. Cancers 2020, 12, 1955. [Google Scholar] [CrossRef]
- Okusaka, T.; Furuse, J. Recent advances in chemotherapy for pancreatic cancer: Evidence from Japan and recommendations in guidelines. J. Gastroenterol. 2020, 55, 369–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikezawa, K.; Kiyota, R.; Takada, R.; Daiku, K.; Maeda, S.; Imai, T.; Abe, Y.; Kai, Y.; Yamai, T.; Fukutake, N.; et al. Efficacy and safety of modified fluorouracil/leucovorin plus irinotecan and oxaliplatin (mFOLFIRINOX) compared with S-1 as second-line chemotherapy in metastatic pancreatic cancer. JGH Open 2021, 5, 679–685. [Google Scholar] [CrossRef]
- Park, H.S.; Kang, B.; Chon, H.J.; Im, H.S.; Lee, C.K.; Kim, I.; Kang, M.J.; Hwang, J.E.; Bae, W.K.; Cheon, J.; et al. Liposomal irinotecan plus fluorouracil/leucovorin versus FOLFIRINOX as the second-line chemotherapy for patients with metastatic pancreatic cancer: A multicenter retrospective study of the Korean Cancer Study Group (KCSG). ESMO Open 2021, 6, 100049. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Pancreatic Adenocarcinoma Version 2.2021. Published 2021. Available online: https://www.nccn.org/guidelines/guidelines-with-evidence-blocks (accessed on 10 April 2021).
- Kircher, S.M.; Krantz, S.B.; Nimeiri, H.S.; Mulcahy, M.F.; Munshi, H.G.; Benson, A.B. Therapy of locally advanced pancreatic adenocarcinoma: Unresectable and borderline patients. Expert Rev. Anticancer Ther. 2011, 11, 1555–1565. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Page, A.J.; Weiss, M.; Wolfgang, C.L.; Herman, J.M.; Pawlik, T.M. Management of borderline and locally advanced pancreatic cancer: Where do we stand? World J. Gastroenterol. 2014, 20, 2255–2266. [Google Scholar] [CrossRef]
- Hammel, P.; Huguet, F.; Van Laethem, J.L.; Goldstein, D.; Glimelius, B.; Artru, P.; Borbath, I.; Bouché, O.; Shannon, J.; André, T.; et al. Effect of chemoradiotherapy vs chemotherapy on survival in patients with locally advanced pancreatic cancer controlled after 4 months of gemcitabine with or without erlotinib the LAP07 randomized clinical trial. JAMA 2016, 315, 1844–1853. [Google Scholar] [CrossRef]
- Loehrer, P.J.; Feng, Y.; Cardenes, H.; Wagner, L.; Brell, J.M.; Cella, D.; Flynn, P.; Ramanathan, R.M.; Crane, C.H.; Alberts, S.R.; et al. Gemcitabine alone versus gemcitabine plus radiotherapy in patients with locally advanced pancreatic cancer: An Eastern Cooperative Oncology Group trial. J. Clin. Oncol. 2011, 29, 4105–4112. [Google Scholar] [CrossRef] [PubMed]
- Chauffert, B.; Mornex, F.; Bonnetain, F.; Rougier, P.; Mariette, C.; Bouche, O.; Bosset, J.F.; Aparicio, T.; Mineur, L.; Azzedine, A.; et al. Phase III trial comparing intensive induction chemoradiotherapy (60 Gy, infusional 5-FU and intermittent cisplatin) followed by maintenance gemcitabine with gemcitabine alone for locally advanced unresectable pancreatic cancer. Definitive results of the 2000-01 FFCD/SFRO study. Ann. Oncol. 2008, 19, 1592–1599. [Google Scholar] [CrossRef]
- Huguet, F.; André, T.; Hammel, P.; Artru, P.; Balosso, J.; Selle, F.; Daniaud-Alexandre, E.; Ruszniewski, P.; Touboul, E.; Labianca, R.; et al. Impact of chemoradiotherapy after disease control with chemotherapy in locally advanced pancreatic adenocarcinoma in GERCOR phase II and III studies. J. Clin. Oncol. 2007, 25, 326–331. [Google Scholar] [CrossRef] [Green Version]
- Ioka, T.; Furuse, J.; Fukutomi, A.; Mizusawa, J.; Nakamura, S.; Hiraoka, N.; Ito, Y.; Katayama, H.; Ueno, M.; Ikeda, M.; et al. Randomized phase II study of chemoradiotherapy with versus without induction chemotherapy for locally advanced pancreatic cancer: Japan Clinical Oncology Group trial, JCOG1106. Jpn. J. Clin. Oncol. 2021, 51, 235–243. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardière, C.; et al. FOLFIRINOX versus Gemcitabine for Metastatic Pancreatic Cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [Green Version]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [Green Version]
- Philip, P.A.; Lacy, J.; Portales, F.; Sobrero, A.; Pazo-Cid, R.; Manzano Mozo, J.L.; Kim, E.J.; Dowden, S.; Zakari, A.; Borg, C.; et al. Nab-paclitaxel plus gemcitabine in patients with locally advanced pancreatic cancer (LAPACT): A multicentre, open-label phase 2 study. Lancet Gastroenterol. Hepatol. 2020, 5, 285–294. [Google Scholar] [CrossRef]
- Takahashi, H.; Yamada, D.; Asukai, K.; Wada, H.; Hasegawa, S.; Hara, H.; Shinno, N.; Ushigome, H.; Haraguchi, N.; Sugimura, K.; et al. Clinical implications of the serum CA19-9 level in “biological borderline resectability” and “biological downstaging” in the setting of preoperative chemoradiation therapy for pancreatic cancer. Pancreatology 2020, 20, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, C.; Hwang, I.; Song, T.J.; Lee, S.S.; Jeong, J.H.; Park, D.H.; Seo, D.W.; Lee, S.K.; Kim, M.H.; Byun, J.H.; et al. FOLFIRINOX in borderline resectable and locally advanced unresectable pancreatic adenocarcinoma. Ther. Adv. Med. Oncol. 2020, 12, 1–9. [Google Scholar] [CrossRef]
- Matsumoto, I.; Kamei, K.; Omae, K.; Suzuki, S.; Matsuoka, H.; Mizuno, N.; Ozaka, M.; Ueno, H.; Kobayashi, S.; Uesugi, K.; et al. FOLFIRINOX for locally advanced pancreatic cancer: Results and prognostic factors of subset analysis from a nation-wide multicenter observational study in Japan. Pancreatology 2019, 19, 296–301. [Google Scholar] [CrossRef]
- Takahashi, H.; Akita, H.; Ioka, T.; Wada, H.; Tomokoni, A.; Asukai, K.; Ohue, M.; Yano, M.; Ishikawa, O. Phase I trial evaluating the safety of preoperative gemcitabine/ nab-paclitaxel with concurrent radiation therapy for borderline resectable pancreatic cancer. Pancreas 2018, 47, 1135–1141. [Google Scholar] [CrossRef]
- Zheng, Y.; Gao, W.; Spratt, D.E.; Sun, Y.; Xing, L. Management of gastrointestinal perforation related to radiation. Int. J. Clin. Oncol. 2020, 25, 1010–1015. [Google Scholar] [CrossRef]
- Kelly, P.; Das, P.; Pinnix, C.C.; Beddar, S.; Briere, T.; Pham, M.; Krishnan, S.; Delclos, M.E.; Crane, C.H. Duodenal toxicity after fractionated chemoradiation for unresectable pancreatic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, e143–e149. [Google Scholar] [CrossRef]
- Satoi, S.; Yamaue, H.; Kato, K.; Takahashi, S.; Hirono, S.; Takeda, S.; Eguchi, H.; Sho, M.; Wada, K.; Shinchi, H.; et al. Role of adjuvant surgery for patients with initially unresectable pancreatic cancer with a long-term favorable response to non-surgical anti-cancer treatments: Results of a project study for pancreatic surgery by the Japanese Society of Hepato-Biliary-Pancreatic Surgery. J. Hepatobiliary Pancreat. Sci. 2013, 20, 590–600. [Google Scholar] [CrossRef] [PubMed]
- Bednar, F.; Zenati, M.S.; Steve, J.; Winters, S.; Ocuin, L.M.; Bahary, N.; Hogg, M.E.; Zeh, H.J., 3rd; Zureikat, A.H. Analysis of predictors of resection and survival in locally advanced stage III pancreatic cancer: Does the nature of chemotherapy regimen influence outcomes? Ann. Surg. Oncol. 2017, 24, 1406–1413. [Google Scholar] [CrossRef] [PubMed]
- Roselló, S.; Pizzo, C.; Huerta, M.; Muñoz, E.; Aliaga, R.; Vera, A.; Alfaro-Cervelló, C.; Jordá, E.; Garcés-Albir, M.; Roda, D.; et al. Neoadjuvant treatment for locally advanced unresectable and borderline resectable pancreatic cancer: Oncological outcomes at a single academic centre. ESMO Open 2020, 5, e000929. [Google Scholar] [CrossRef] [PubMed]
- Kunzmann, V.; Siveke, J.T.; Algül, H.; Goekkurt, E.; Siegler, G.; Martens, U.; Waldschmidt, D.; Pelzer, U.; Fuchs, M.; Kullmann, F.; et al. Nab-paclitaxel plus gemcitabine versus nab-paclitaxel plus gemcitabine followed by FOLFIRINOX induction chemotherapy in locally advanced pancreatic cancer (NEOLAP-AIO-PAK-0113): A multicentre, randomised, phase 2 trial. Lancet Gastroenterol. Hepatol. 2021, 6, 128–138. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All | CRT Group | CTx Group | p-Value | |
|---|---|---|---|---|
| (n = 45) | (n = 25) | (n = 20) | ||
| Age (years) * | 68 (48–82) | 67 (48–82) | 68 (48–76) | 0.514 |
| Sex (male/female) | 24/21 | 11/14 | 10/10 | 0.769 |
| ECOG PS (0/1) | 33/12 | 17/8 | 16/4 | 0.502 |
| Location (head/body and tail) | 31/14 | 9/16 | 5/15 | 0.525 |
| Tumor size (mm) * | 37.0 (20.0–100.0) | 33.0 (20.0–100.0) | 38.5 (24.0–74.0) | 0.134 |
| Duodenal invasion (yes/no) | 11/34 | 3/22 | 8/12 | 0.041 |
| Biliary drainage (yes/no) | 15/30 | 9/16 | 6/14 | 0.757 |
| CA19-9 (U/mL) * | 372.0 (<2.0–13, 856.0) | 372 (<2.0–13, 856.0) | 464 (<2.0–13, 292.0) | 0.404 |
| CEA (ng/mL) * | 3.2 (0.8–103.3) | 2.9 (0.8–103.3) | 4.35 (1.5–100.4) | 0.17 |
| Follow-up period (months) * | 25.5 (8.9–48.2) |
| All | CRT Group | CTx Group | p-Value | |
|---|---|---|---|---|
| (n = 45) | (n = 25) | (n = 20) | ||
| Best response | ||||
| CR | 1 | 1 | 0 | |
| PR | 17 | 11 | 6 | |
| SD | 24 | 13 | 11 | |
| PD | 2 | 0 | 2 | |
| NE | 1 | 0 | 1 | |
| Best overall response rate (%) | 40 | 48 | 30 | 0.359 † |
| Disease control rate (%) | 93.3 | 100 | 85 | 0.080 † |
| Progression-free survival time (months § [95% CI]) | 16.0 (12.3–20.9) | 18.5 (15.0–22.7) | 7.6 (5.3–21.4) | 0.036 ‡ |
| Duration of local response (months, § [95% CI]) | 22.0 (18.3–25.4) | 24.2 (20.3–30.4) | 10.3 (5.3–25.2) | 0.005 ‡ |
| Overall survival time (months, § [95% CI]) | 25.5 (18.8–28.5) | 29.2 (25.4–35.4) | 17.4 (11.2–25.9) | <0.001 ‡ |
| No. | Sex | Age (y) | ECOGPS | Tumor Size (mm) | Tumor Location | Duodenal Invasion | Duration of Induction Chemotherapy (Months) | Time to Surgery (Months) | Operation | Resection Margin | DFS (Months) | OS (Months) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (Initial → CRT) | ||||||||||||
| 1 | F | 64 | 1 | 29 → 24 | Head | No | 10.9 | 13 | PD | R0 | 17.7 | 48.2 |
| (dead) | ||||||||||||
| 2 | F | 66 | 0 | 26 → 23 | BT | No | 2.3 | 4.9 | DP-CAR | R1 | 15.8 | 45.9 |
| (alive) | ||||||||||||
| 3 | F | 68 | 1 | 26 → 16 | BT | No | 3.5 | 6.1 | PD | R0 | 17.2 | 44.3 |
| (alive) | ||||||||||||
| 4 | M | 73 | 0 | 29 → 19 | Head | Yes | 6.1 | 10.3 | PD | R0 | 12.7 | 36.0 |
| (dead) | ||||||||||||
| 5 | F | 66 | 0 | 45 → 18 | BT | No | 1.9 | 13.6 | DP-CAR | R0 | 9.4 | 29.4 |
| (dead) | ||||||||||||
| 6 | M | 64 | 1 | 23 → 22 | Head | No | 4.8 | 11.6 | PD | R0 | 8.2 | 29.3 |
| (dead) |
| Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| Age (years) | <70 | 1 | |||
| ≥70 | 1.37 (0.72–2.58) | 0.338 | |||
| Sex | Male | 1 | |||
| Female | 0.90 (0.48–1.68) | 0.746 | |||
| ECOG PS | 0 | 1 | |||
| 1 | 1.01 (0.49–2.08) | 0.976 | |||
| Location | Body and tail | 1 | |||
| Head | 0.93 (0.47–1.83) | 0.825 | |||
| Tumor size (mm) | <40 | 1 | 1 | ||
| ≥40 | 2.25 (1.18–4.30) | 0.014 | 1.71 (0.87–3.35) | 0.119 | |
| Duodenal invasion | No | 1 | |||
| Yes | 1.37 (0.68–2.75) | 0.379 | |||
| Biliary drainage | No | 1 | |||
| Yes | 0.75 (0.38–1.47) | 0.398 | |||
| CRT following induction chemotherapy | No | 1 | 1 | ||
| Yes | 0.34 (0.18–0.65) | 0.001 | 0.40 (0.21–0.79) | 0.008 | |
| CA19-9 (U/mL) | <1000 | 1 | |||
| ≥1000 | 1.53 (0.79–3.00) | 0.21 | |||
| CEA (ng/mL) | <5.0 | 1 | |||
| ≥5.0 | 0.88 (0.45–1.72) | 0.709 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takada, R.; Ikezawa, K.; Daiku, K.; Maeda, S.; Abe, Y.; Urabe, M.; Kai, Y.; Yamai, T.; Fukutake, N.; Nakabori, T.; et al. The Survival Benefit of Chemoradiotherapy following Induction Chemotherapy with Gemcitabine Plus Nab-Paclitaxel for Unresectable Locally Advanced Pancreatic Cancer. Cancers 2021, 13, 4733. https://doi.org/10.3390/cancers13184733
Takada R, Ikezawa K, Daiku K, Maeda S, Abe Y, Urabe M, Kai Y, Yamai T, Fukutake N, Nakabori T, et al. The Survival Benefit of Chemoradiotherapy following Induction Chemotherapy with Gemcitabine Plus Nab-Paclitaxel for Unresectable Locally Advanced Pancreatic Cancer. Cancers. 2021; 13(18):4733. https://doi.org/10.3390/cancers13184733
Chicago/Turabian StyleTakada, Ryoji, Kenji Ikezawa, Kazuma Daiku, Shingo Maeda, Yutaro Abe, Makiko Urabe, Yugo Kai, Takuo Yamai, Nobuyasu Fukutake, Tasuku Nakabori, and et al. 2021. "The Survival Benefit of Chemoradiotherapy following Induction Chemotherapy with Gemcitabine Plus Nab-Paclitaxel for Unresectable Locally Advanced Pancreatic Cancer" Cancers 13, no. 18: 4733. https://doi.org/10.3390/cancers13184733