
Individual 5-Year Lung Cancer Risk Prediction Model in Korea Using a Nationwide Representative Database

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Database Source
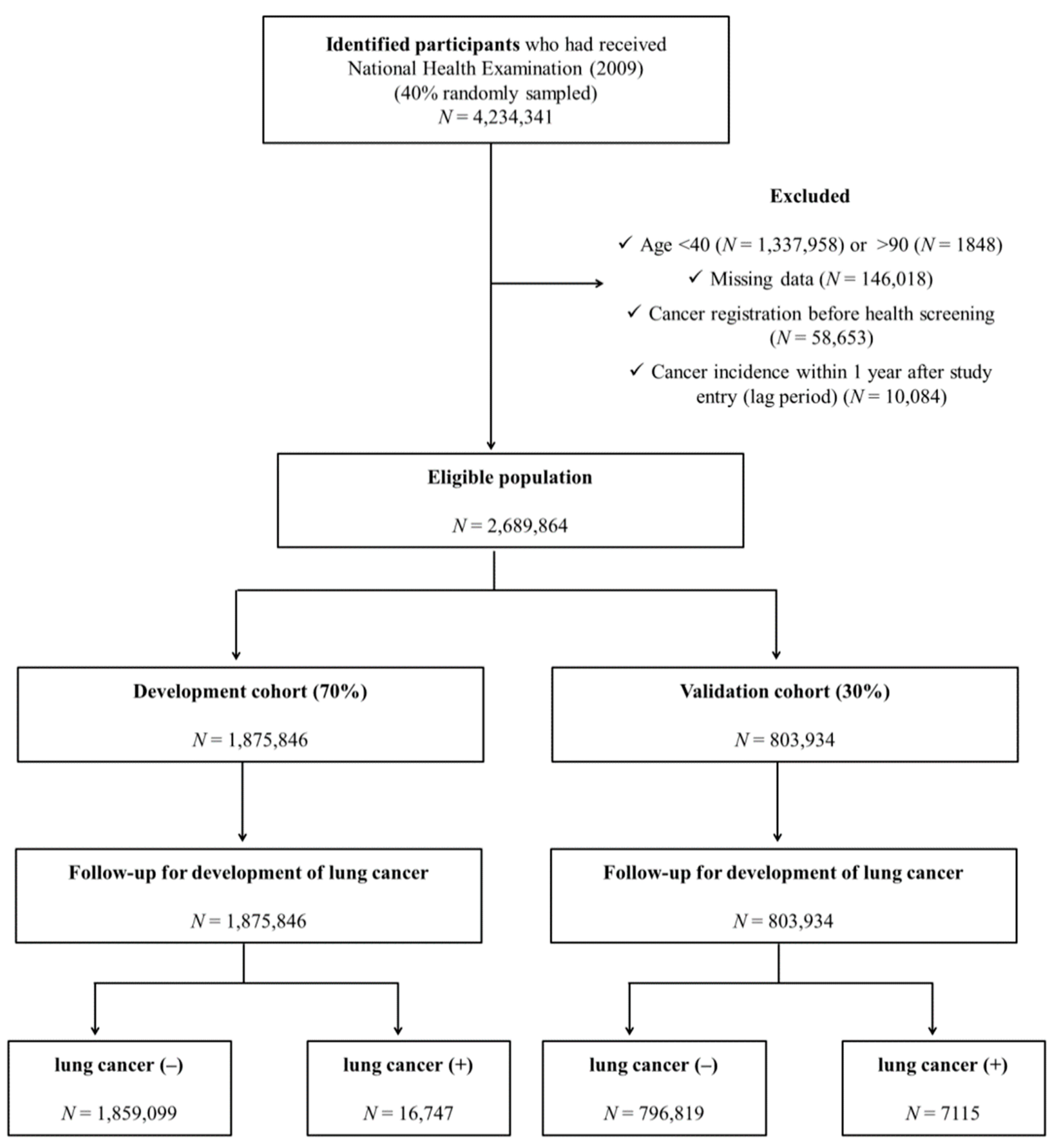
2.2. Study Population
2.3. Predictor Variables
2.4. Lung Cancer as an Outcome
2.5. Development of Risk Prediction Model
2.6. Validation of the Risk Prediction Model
2.7. Statistical Analyses
3. Results
3.1. Clinical Characteristics of the Study Population in the Development and Validation Cohorts
3.2. Selection of Predictor Variables for the Prediction Model
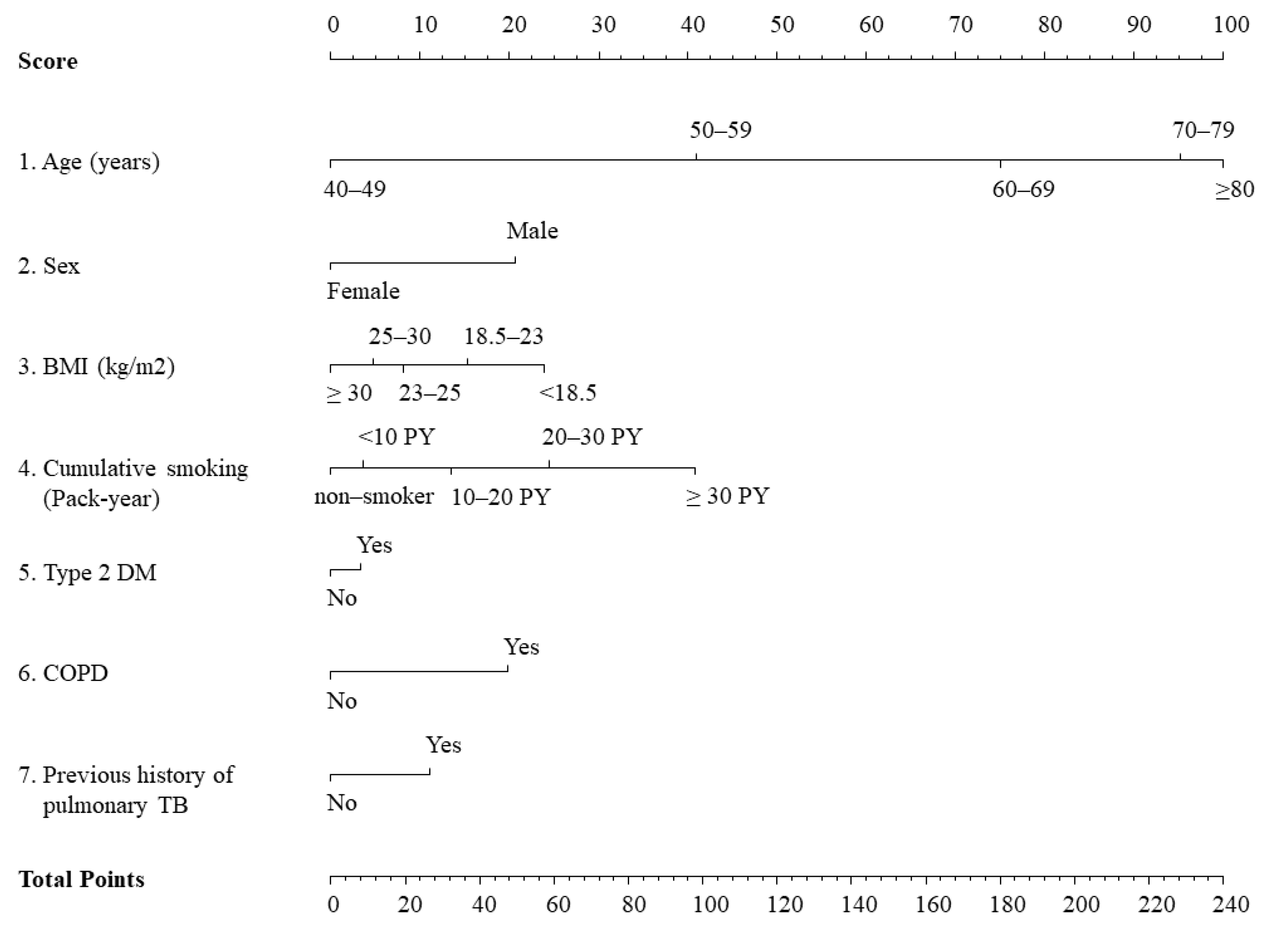
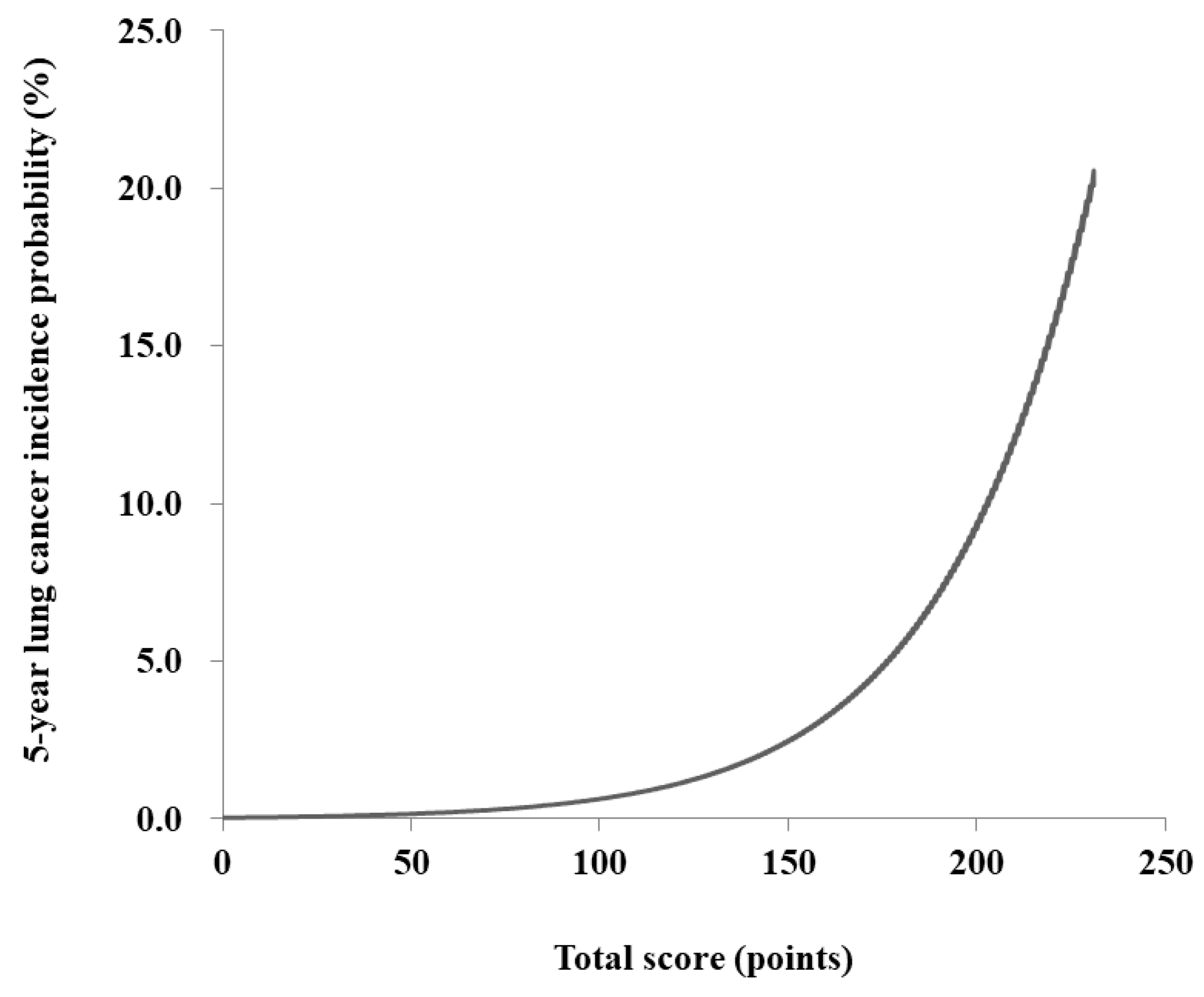
3.3. Development of Scores for Lung Cancer Prediction
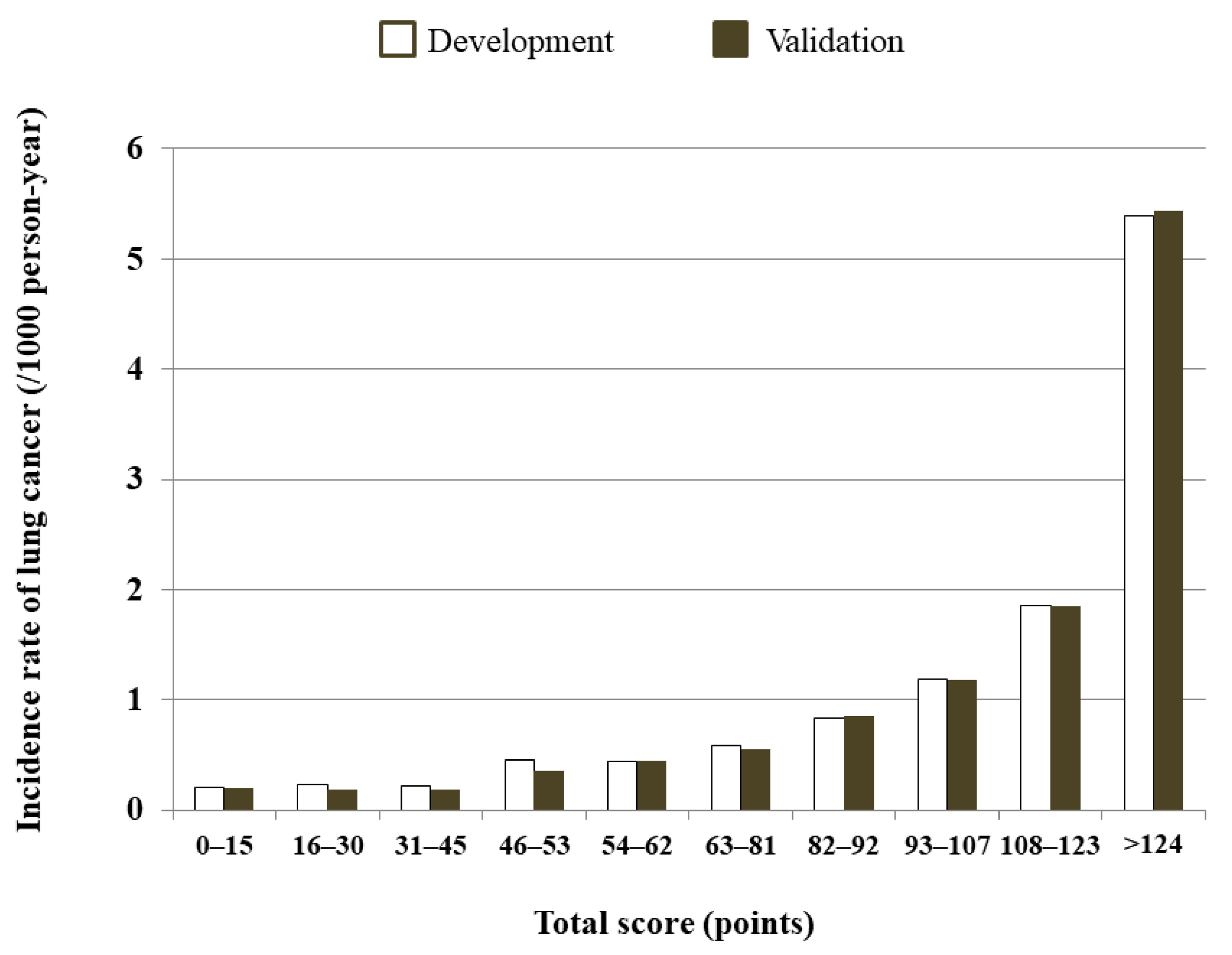
3.4. Validation of the Risk Model
4. Discussion
4.1. Previous Lung Cancer Prediction Models
4.2. Predictor Variables in Lung Cancer
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, K.W.; Won, Y.J.; Kong, H.J.; Lee, E.S. Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2016. Cancer Res. Treat. 2019, 51, 417–430. [Google Scholar] [CrossRef] [Green Version]
- Shin, A.; Oh, C.M.; Kim, B.W.; Woo, H.; Won, Y.J.; Lee, J.S. Lung Cancer Epidemiology in Korea. Cancer Res. Treat. 2017, 49, 616–626. [Google Scholar] [CrossRef] [Green Version]
- Jung, K.W.; Won, Y.J.; Kong, H.J.; Lee, E.S. Prediction of Cancer Incidence and Mortality in Korea, 2019. Cancer Res. Treat. 2019, 51, 431–437. [Google Scholar] [CrossRef]
- Jaklitsch, M.T.; Jacobson, F.L.; Austin, J.H.; Field, J.K.; Jett, J.R.; Keshavjee, S.; MacMahon, H.; Mulshine, J.L.; Munden, R.F.; Salgia, R.; et al. The American Association for Thoracic Surgery guidelines for lung cancer screening using low-dose computed tomography scans for lung cancer survivors and other high-risk groups. J. Thorac. Cardiovasc. Surg. 2012, 144, 33–38. [Google Scholar] [CrossRef] [Green Version]
- Kovalchik, S.A.; Tammemagi, M.; Berg, C.D.; Caporaso, N.E.; Riley, T.L.; Korch, M.; Silvestri, G.A.; Chaturvedi, A.K.; Katki, H.A. Targeting of low-dose CT screening according to the risk of lung-cancer death. N. Engl. J. Med. 2013, 369, 245–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakoda, L.C.; Henderson, L.M.; Caverly, T.J.; Wernli, K.J.; Katki, H.A. Applying Risk Prediction Models to Optimize Lung Cancer Screening: Current Knowledge, Challenges, and Future Directions. Curr. Epidemiol. Rep. 2017, 4, 307–320. [Google Scholar] [CrossRef]
- Tammemagi, C.M.; Pinsky, P.F.; Caporaso, N.E.; Kvale, P.A.; Hocking, W.G.; Church, T.R.; Riley, T.L.; Commins, J.; Oken, M.M.; Berg, C.D.; et al. Lung cancer risk prediction: Prostate, Lung, Colorectal And Ovarian Cancer Screening Trial models and validation. J. Natl. Cancer Inst. 2011, 103, 1058–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tammemagi, M.C.; Katki, H.A.; Hocking, W.G.; Church, T.R.; Caporaso, N.; Kvale, P.A.; Chaturvedi, A.K.; Silvestri, G.A.; Riley, T.L.; Commins, J.; et al. Selection criteria for lung-cancer screening. N. Engl. J. Med. 2013, 368, 728–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcus, M.W.; Chen, Y.; Raji, O.Y.; Duffy, S.W.; Field, J.K. LLPi: Liverpool Lung Project Risk Prediction Model for Lung Cancer Incidence. Cancer Prev. Res 2015, 8, 570–575. [Google Scholar] [CrossRef] [Green Version]
- Cassidy, A.; Myles, J.P.; van Tongeren, M.; Page, R.D.; Liloglou, T.; Duffy, S.W.; Field, J.K. The LLP risk model: An individual risk prediction model for lung cancer. Br. J. Cancer. 2008, 98, 270–276. [Google Scholar] [CrossRef]
- Spitz, M.R.; Hong, W.K.; Amos, C.I.; Wu, X.; Schabath, M.B.; Dong, Q.; Shete, S.; Etzel, C.J. A risk model for prediction of lung cancer. J. Natl. Cancer Inst. 2007, 99, 715–726. [Google Scholar] [CrossRef] [PubMed]
- Hoggart, C.; Brennan, P.; Tjonneland, A.; Vogel, U.; Overvad, K.; Ostergaard, J.N.; Kaaks, R.; Canzian, F.; Boeing, H.; Steffen, A.; et al. A risk model for lung cancer incidence. Cancer Prev. Res. 2012, 5, 834–846. [Google Scholar] [CrossRef] [Green Version]
- Muller, D.C.; Johansson, M.; Brennan, P. Lung Cancer Risk Prediction Model Incorporating Lung Function: Development and Validation in the UK Biobank Prospective Cohort Study. J. Clin. Oncol. 2017, 35, 861–869. [Google Scholar] [CrossRef] [Green Version]
- Bach, P.B.; Kattan, M.W.; Thornquist, M.D.; Kris, M.G.; Tate, R.C.; Barnett, M.J.; Hsieh, L.J.; Begg, C.B. Variations in lung cancer risk among smokers. J. Natl. Cancer Inst. 2003, 95, 470–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, D.O.; Weissfeld, J. A simple model for predicting lung cancer occurrence in a lung cancer screening program: The Pittsburgh Predictor. Lung Cancer 2015, 89, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Nam, B.H.; Yang, H.R.; Lee, J.A.; Lim, H.; Han, J.T.; Park, I.S.; Shin, H.R.; Lee, J.S. Individualized risk prediction model for lung cancer in Korean men. PLoS ONE 2013, 8, e54823. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.J.; Jeon, C.; Jee, S.H. The effect of smoking on lung cancer: Ethnic differences and the smoking paradox. Epidemiol. Health 2016, 38, e2016060. [Google Scholar] [CrossRef]
- Lee, H.; Cho, J.; Shin, D.W.; Lee, S.P.; Hwang, S.S.; Oh, J.; Yang, H.K.; Hwang, S.H.; Son, K.Y.; Chun, S.H.; et al. Association of cardiovascular health screening with mortality, clinical outcomes, and health care cost: A nationwide cohort study. Prev. Med. 2015, 70, 19–25. [Google Scholar] [CrossRef]
- Shin, D.W.; Cho, B.; Guallar, E. Korean National Health Insurance Database. JAMA Intern. Med. 2016, 176, 138. [Google Scholar] [CrossRef]
- Cheol Seong, S.; Kim, Y.Y.; Khang, Y.H.; Heon Park, J.; Kang, H.J.; Lee, H.; Do, C.H.; Song, J.S.; Hyon Bang, J.; Ha, S.; et al. Data Resource Profile: The National Health Information Database of the National Health Insurance Service in South Korea. Int. J. Epidemiol. 2017, 46, 799–800. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Lee, J.S.; Park, S.H.; Shin, S.A.; Kim, K. Cohort Profile: The National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef]
- Duan, P.; Hu, C.; Quan, C.; Yi, X.; Zhou, W.; Yuan, M.; Yu, T.; Kourouma, A.; Yang, K. Body mass index and risk of lung cancer: Systematic review and dose-response meta-analysis. Sci. Rep. 2015, 5, 16938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Dong, J.; Sun, K.; Zhao, L.; Zhao, F.; Wang, L.; Jiao, Y. Obesity and incidence of lung cancer: A meta-analysis. Int. J. Cancer 2013, 132, 1162–1169. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.R.; Fehringer, G.; Zhang, Z.F.; Lee, Y.A.; Meyers, T.; Matsuo, K.; Ito, H.; Vineis, P.; Stucker, I.; Boffetta, P.; et al. Alcohol consumption and lung cancer risk: A pooled analysis from the International Lung Cancer Consortium and the SYNERGY study. Cancer Epidemiol. 2019, 58, 25–32. [Google Scholar] [CrossRef]
- Lee, J.Y.; Jeon, I.; Lee, J.M.; Yoon, J.M.; Park, S.M. Diabetes mellitus as an independent risk factor for lung cancer: A meta-analysis of observational studies. Eur. J. Cancer 2013, 49, 2411–2423. [Google Scholar] [CrossRef] [PubMed]
- Denholm, R.; Schuz, J.; Straif, K.; Stucker, I.; Jockel, K.H.; Brenner, D.R.; De Matteis, S.; Boffetta, P.; Guida, F.; Bruske, I.; et al. Is previous respiratory disease a risk factor for lung cancer? Am. J. Respir. Crit. Care Med. 2014, 190, 549–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, S.; Mok, Y.; Jeon, C.; Jee, S.H.; Samet, J.M. Tuberculosis, smoking and risk for lung cancer incidence and mortality. Int. J. Cancer 2016, 139, 2447–2455. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.I.; McKinley, M.; Cheng, I.; Haile, R.; Wakelee, H.; Gomez, S.L. Lung cancer incidence trends in California by race/ethnicity, histology, sex, and neighborhood socioeconomic status: An analysis spanning 28 years. Lung Cancer 2017, 108, 140–149. [Google Scholar] [CrossRef]
- Wilson, P.W.; D’Agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershatz, H.; Kannel, W.B. Prediction of coronary heart disease using risk factor categories. Circulation 1998, 97, 1837–1847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.H.; Bang, H.; Kim, D.J. How to Establish Clinical Prediction Models. Endocrinol. Metab. 2016, 31, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Royston, P.; Parmar, M.K. Flexible parametric proportional-hazards and proportional-odds models for censored survival data, with application to prognostic modelling and estimation of treatment effects. Stat. Med. 2002, 21, 2175–2197. [Google Scholar] [CrossRef]
- Korea Central Cancer Registry. Annual Report of Cancer Statistics in Korea in 2017; National Cancer Center, Ministry of Health and Welfare: Sejong-si, Korea, 2019.
- Wu, X.; Wen, C.P.; Ye, Y.; Tsai, M.; Wen, C.; Roth, J.A.; Pu, X.; Chow, W.H.; Huff, C.; Cunningham, S.; et al. Personalized Risk Assessment in Never, Light, and Heavy Smokers in a prospective cohort in Taiwan. Sci. Rep. 2016, 6, 36482. [Google Scholar] [CrossRef]
- Jacobson, F.L.; Austin, J.H.; Field, J.K.; Jett, J.R.; Keshavjee, S.; MacMahon, H.; Mulshine, J.L.; Munden, R.F.; Salgia, R.; Strauss, G.M.; et al. Development of The American Association for Thoracic Surgery guidelines for low-dose computed tomography scans to screen for lung cancer in North America: Recommendations of The American Association for Thoracic Surgery Task Force for Lung Cancer Screening and Surveillance. J. Thorac. Cardiovasc. Surg. 2012, 144, 25–32. [Google Scholar] [PubMed] [Green Version]
- Gu, F.; Wacholder, S.; Kovalchik, S.; Panagiotou, O.A.; Reyes-Guzman, C.; Freedman, N.D.; De Matteis, S.; Consonni, D.; Bertazzi, P.A.; Bergen, A.W.; et al. Time to smoke first morning cigarette and lung cancer in a case-control study. J. Natl. Cancer Inst. 2014, 106, dju118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brennan, P.; Crispo, A.; Zaridze, D.; Szeszenia-Dabrowska, N.; Rudnai, P.; Lissowska, J.; Fabianova, E.; Mates, D.; Bencko, V.; Foretova, L.; et al. High cumulative risk of lung cancer death among smokers and nonsmokers in Central and Eastern Europe. Am. J. Epidemiol. 2006, 164, 1233–1241. [Google Scholar] [CrossRef] [Green Version]
- Agudo, A.; Bonet, C.; Travier, N.; Gonzalez, C.A.; Vineis, P.; Bueno-de-Mesquita, H.B.; Trichopoulos, D.; Boffetta, P.; Clavel-Chapelon, F.; Boutron-Ruault, M.C.; et al. Impact of cigarette smoking on cancer risk in the European prospective investigation into cancer and nutrition study. J. Clin. Oncol. 2012, 30, 4550–4557. [Google Scholar] [CrossRef]
- Brenner, D.R.; Boffetta, P.; Duell, E.J.; Bickeboller, H.; Rosenberger, A.; McCormack, V.; Muscat, J.E.; Yang, P.; Wichmann, H.E.; Brueske-Hohlfeld, I.; et al. Previous lung diseases and lung cancer risk: A pooled analysis from the International Lung Cancer Consortium. Am. J. Epidemiol. 2012, 176, 573–585. [Google Scholar] [CrossRef]
- Hemminki, K.; Forsti, A.; Fallah, M.; Sundquist, J.; Sundquist, K.; Ji, J. Risk of cancer in patients with medically diagnosed hay fever or allergic rhinitis. Int. J. Cancer 2014, 135, 2397–2403. [Google Scholar] [CrossRef] [Green Version]
- El-Zein, M.; Parent, M.E.; Siemiatycki, J.; Rousseau, M.C. History of allergic diseases and lung cancer risk. Ann. Allergy Asthma Immunol. 2014, 112, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Nitadori, J.; Inoue, M.; Iwasaki, M.; Otani, T.; Sasazuki, S.; Nagai, K.; Tsugane, S. Association between lung cancer incidence and family history of lung cancer: Data from a large-scale population-based cohort study, the JPHC study. Chest 2006, 130, 968–975. [Google Scholar] [CrossRef] [Green Version]
- Wu, A.H.; Fontham, E.T.; Reynolds, P.; Greenberg, R.S.; Buffler, P.; Liff, J.; Boyd, P.; Correa, P. Family history of cancer and risk of lung cancer among lifetime nonsmoking women in the United States. Am. J. Epidemiol. 1996, 143, 535–542. [Google Scholar] [CrossRef] [Green Version]
- Samet, J.M.; Humble, C.G.; Pathak, D.R. Personal and family history of respiratory disease and lung cancer risk. Am. Rev. Respir. Dis. 1986, 134, 466–470. [Google Scholar]
- Choi, S.; Kim, Y.; Park, S.; Lee, J.; Oh, K. Trends in cigarette smoking among adolescents and adults in South Korea. Epidemiol. Health 2014, 36, e2014023. [Google Scholar] [CrossRef] [Green Version]
- Park, E.J.; Koh, H.K.; Kwon, J.W.; Suh, M.K.; Kim, H.; Cho, S.I. Secular trends in adult male smoking from 1992 to 2006 in South Korea: Age-specific changes with evolving tobacco-control policies. Public Health 2009, 123, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Zhang, S. Body mass index and lung cancer risk in never smokers: A meta-analysis. BMC Cancer 2018, 18, 635. [Google Scholar] [CrossRef] [PubMed]
- Vineis, P.; Perera, F. DNA adducts as markers of exposure to carcinogens and risk of cancer. Int J Cancer. 2000, 88, 325–328. [Google Scholar] [CrossRef]
- Godschalk, R.W.; Feldker, D.E.; Borm, P.J.; Wouters, E.F.; van Schooten, F.J. Body mass index modulates aromatic DNA adduct levels and their persistence in smokers. Cancer Epidemiol. Prev. Biomark. 2002, 11, 790–793. [Google Scholar]
- Calle, E.E.; Kaaks, R. Overweight, obesity and cancer: Epidemiological evidence and proposed mechanisms. Nat. Rev. Cancer 2004, 4, 579–591. [Google Scholar] [CrossRef]
- Song, X.; Pukkala, E.; Dyba, T.; Tuomilehto, J.; Moltchanov, V.; Männistö, S.; Jousilahti, P.; Qiao, Q. Body mass index and cancer incidence: The FINRISK study. Eur. J. Epidemiol. 2014, 29, 477–487. [Google Scholar] [CrossRef]
- Houghton, A.M. Mechanistic links between COPD and lung cancer. Nat. Rev. Cancer 2013, 13, 233–245. [Google Scholar] [CrossRef]
- Azad, N.; Rojanasakul, Y.; Vallyathan, V. Inflammation and lung cancer: Roles of reactive oxygen/nitrogen species. J. Toxicol. Environ. Health B Crit. Rev. 2008, 11, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.W.; Karin, M. A cytokine-mediated link between innate immunity, inflammation, and cancer. J. Clin. Investig. 2007, 117, 1175–1183. [Google Scholar] [CrossRef]
- O’Callaghan, D.S.; O’Donnell, D.; O’Connell, F.; O’Byrne, K.J. The role of inflammation in the pathogenesis of non-small cell lung cancer. J. Thorac. Oncol. 2010, 5, 2024–2036. [Google Scholar] [CrossRef] [Green Version]
- Chaturvedi, A.K.; Caporaso, N.E.; Katki, H.A.; Wong, H.L.; Chatterjee, N.; Pine, S.R.; Chanock, S.J.; Goedert, J.J.; Engels, E.A. C-reactive protein and risk of lung cancer. J. Clin. Oncol. 2010, 28, 2719–2726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dennis, R.J.; Maldonado, D.; Rojas, M.X.; Aschner, P.; Rondon, M.; Charry, L.; Casas, A. Inadequate glucose control in type 2 diabetes is associated with impaired lung function and systemic inflammation: A cross-sectional study. BMC Pulm. Med. 2010, 10, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Developmental Cohort (n = 1,975,846) | Validation Cohort (n = 803,934) | |||||
|---|---|---|---|---|---|---|
| Lung Cancer Did Not Develop (n = 1,859,099) | Lung Cancer Developed (n = 16,747) | p-Value a | Lung Cancer Did Not Develop (n = 796,819) | Lung Cancer Developed (n = 7115) | p-Value a | |
| Age (years) (N, %) | ||||||
| 40–49 | 725,609 (39.0) | 1481 (8.8) | <0.001 | 310,720 (39.0) | 561 (7.9) | <0.0001 |
| 50–59 | 578,958 (31.1) | 3859 (23.0) | 247,804 (31.1) | 1674 (23.5) | ||
| 60–69 | 361,299 (19.4) | 6193 (37.0) | 155,121 (19.5) | 2659 (37.4) | ||
| 70–79 | 168,698 (9.1) | 4606 (27.5) | 72,753 (9.1) | 1989 (28.0) | ||
| ≥80 | 24,535 (1.3) | 608 (3.6) | 10,421 (1.3) | 232 (3.3) | ||
| Sex (male) (N, %) | 926,036 (49.8) | 11,989 (71.6) | <0.001 | 396,541 (49.8) | 5200 (73.1) | <0.0001 |
| BMI (kg/m2) (N, %) | ||||||
| <18.5 | 40,779 (2.2) | 670 (4.0) | <0.001 | 17,599 (2.2) | 260 (3.65) | <0.0001 |
| 18.5–23 | 668,716 (36.0) | 6668 (39.8) | 286,694 (36.0) | 2839 (39.9) | ||
| 23–25 | 496,918 (26.7) | 4329 (25.9) | 212,892 (26.7) | 1868 (26.3) | ||
| 25–30 | 590,430 (31.8) | 4714 (28.2) | 252,927 (31.7) | 2004 (28.2) | ||
| ≥30 | 62,256 (3.4) | 366 (2.2) | 26,707 (3.4) | 144 (2.0) | ||
| Smoking (pack-years) (N, %) | ||||||
| Nonsmoker | 1,193,868 (64.2) | 7247 (43.3) | <0.001 | 512,328 (64.3) | 2973 (41.8) | <0.0001 |
| <10 | 158,726 (8.5) | 979 (5.9) | 68,088 (8.5) | 423 (6.0) | ||
| 10–20 | 185,327 (10.0) | 1571 (9.4) | 79,402 (10.0) | 646 (9.1) | ||
| 20–30 | 157,04 7(8.5) | 1899 (11.3) | 67,004 (8.4) | 861 (12.1) | ||
| ≥30 | 164,131 (8.8) | 5051 (30.2) | 69,997 (8.8) | 2212 (31.0) | ||
| Alcohol drinking (N, %) | ||||||
| Nondrinker | 1,085,573 (58.4) | 9421 (56.3) | <0.001 | 465,956 (58.5) | 3940 (55.4) | <0.0001 |
| Light drinker | 453,362 (24.4) | 3653 (21.8) | 194,041 (24.3) | 1568 (22.0) | ||
| Moderate drinker | 183,947 (9.9) | 1903 (11.3) | 78,682 (9.9) | 828 (11.6) | ||
| Heavy | 136,217 (7.3) | 1770 (10.6) | 58,140 (7.3) | 779 (11.0) | ||
| Type 2 DM (yes) (N, %) | 220,692 (11.9) | 3028 (18.1) | <0.001 | 95,092 (11.9) | 1329 (18.7) | <0.0001 |
| COPD (yes) (N, %) | 64,554 (3.5) | 1997 (11.9) | 28,004 (3.5) | 847 (11.9) | ||
| Pulmonary TB (yes) (N, %) | 22,083 (1.2) | 485 (2.9) | 9688 (1.2) | 228 (3.2) | ||
| Insurance coverage (Medicaid) (N, %) | 76,054 (4.1) | 738 (4.4) | 0.04 | 32,830 (4.1) | 311 (4.4) | 0.29 |
| Number of Subjects | Event | Follow-Up (PYs) | IR | Crude HR (95% CI) | Model 1 aHR (95% CI) | Model 2 aHR (95% CI) | |
|---|---|---|---|---|---|---|---|
| Age (years) | |||||||
| 40–49 | 727,090 | 1481 | 6027, 618.8 | 0.25 | 1 (ref) | 1 (ref) | 1 (ref) |
| 50–59 | 582,817 | 3859 | 4822, 231.1 | 0.80 | 3.26 (3.07–3.46) | 3.03 (2.86–3.22) | 3.05 (2.87–3.24) |
| 60–69 | 367,492 | 6193 | 2996, 657.1 | 2.07 | 8.42 (7.95–8.91) | 7.61 (7.18–8.07) | 7.71 (7.27–8.17) |
| 70–79 | 173,304 | 4606 | 1334, 442.8 | 3.45 | 14.15 (13.34–15.00) | 13.11 (12.33–13.93) | 13.35 (12.57–14.19) |
| 80–89 | 25,143 | 608 | 160, 846.8 | 3.78 | 15.87 (14.44–17.44) | 14.88 (13.51–16.39) | 15.21 (13.82–16.75) |
| Sex | |||||||
| Male | 938,025 | 11,989 | 7597, 638.5 | 1.58 | 1 (ref) | 1 (ref) | 1 (ref) |
| Female | 937,821 | 4758 | 7744, 157.9 | 0.61 | 0.39 (0.38–0.40) | 0.56 (0.53–0.58) | 0.60 (0.52–0.71) |
| BMI (kg/m2) | |||||||
| <18.5 | 41,449 | 670 | 321, 011.2 | 2.09 | 1.73 (1.60–1.88) | 1.26 (1.16–1.36) | 1.20 (0.90–1.59) |
| 18.5–23 | 675,384 | 6668 | 5504, 084.6 | 1.21 | 1 (ref) | 1 (ref) | 1 (ref) |
| 23–25 | 501,247 | 4329 | 4113, 813.5 | 1.05 | 0.87 (0.84–0.90) | 0.82 (0.79–0.86) | 0.86 (0.75–0.98) |
| 25–30 | 595,144 | 4714 | 4889, 253.9 | 0.96 | 0.80 (0.77–0.83) | 0.75 (0.72–0.78) | 0.76 (0.67–0.86) |
| ≥30 | 62,622 | 366 | 513, 633.42 | 0.71 | 0.59 (0.53–0.65) | 0.66 (0.59–0.73) | 0.65 (0.45–0.94) |
| Smoking (pack-year) | |||||||
| Nonsmoker | 1,201,115 | 7247 | 9874, 552.2 | 0.73 | 1 (ref) | 1 (ref) | 1 (ref) |
| <10 | 159,705 | 979 | 1307, 649.6 | 0.75 | 1.023 (0.96–1.09) | 1.12 (1.05–1.21) | 1.28 (1.01–1.63) |
| 10–20 | 186,898 | 1571 | 1524, 583.2 | 1.03 | 1.41 (1.33–1.49) | 1.47 (1.38–1.56) | 1.51 (1.22–1.88) |
| 20–30 | 158,946 | 1899 | 129, 0218.4 | 1.47 | 2.01 (1.91–2.12) | 1.98 (1.87–2.10) | 2.53 (2.09–3.06) |
| ≥30 | 169,182 | 5051 | 1344, 793.1 | 3.76 | 5.14 (4.96–5.33) | 3.07 (2.93–3.22) | 3.47 (2.96–4.07) |
| Alcohol consumption | |||||||
| Nondrinker | 1,094,994 | 9421 | 8951, 014.5 | 1.05 | 1 (ref.) | 1 (ref.) | - |
| Light | 457,015 | 3653 | 3753, 142.2 | 0.97 | 0.93 (0.89–0.96) | 0.89 (0.85–0.92) | |
| Moderate | 185,850 | 1903 | 1518, 858.3 | 1.05 | 1.19 (1.14–1.25) | 0.94 (0.89–0.99) | |
| Heavy | 137,987 | 1770 | 1118, 511.4 | 1.58 | 1.51 (1.43–1.59) | 0.96 (0.91–1.02) | |
| Presence of type 2 DM | |||||||
| No | 1,652,126 | 13,719 | 13,563, 423.2 | 1.01 | 1 (ref) | 1 (ref) | 1 (ref) |
| Yes | 223,720 | 3028 | 1,778,373.3 | 1.70 | 1.67 (1.62–1.76) | 1.09 (1.05–1.14) | 1.22 (1.07–1.40) |
| Presence of COPD | |||||||
| No | 1,809,295 | 14,750 | 14,830, 410.7 | 0.99 | 1 (ref) | 1 (ref) | 1 (ref) |
| Yes | 66,551 | 1997 | 511, 385.8 | 3.91 | 3.94 (3.76–4.13) | 1.70 (1.62–1.79) | 1.70 (1.44–2.00) |
| Presence of pulmonary TB | |||||||
| No | 1,853,278 | 16,262 | 15,165, 257.7 | 1.07 | 1 (ref) | 1 (ref) | 1 (ref) |
| Yes | 22,568 | 485 | 176, 538.8 | 2.75 | 2.57 (2.35–2.81) | 1.34 (1.22–1.47) | 1.62 (1.23–2.14) |
| Insurance coverage | |||||||
| Non-Medicaid | 1,799,054 | 16,009 | 14,712, 765.1 | 1.09 | 1 (ref) | 1 (ref) | - |
| Medicaid | 76,792 | 738 | 629, 031.4 | 1.17 | 1.08 (1.00–1.16) | 1.05 (0.97–1.13) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeo, Y.; Shin, D.W.; Han, K.; Park, S.H.; Jeon, K.-H.; Lee, J.; Kim, J.; Shin, A. Individual 5-Year Lung Cancer Risk Prediction Model in Korea Using a Nationwide Representative Database. Cancers 2021, 13, 3496. https://doi.org/10.3390/cancers13143496
Yeo Y, Shin DW, Han K, Park SH, Jeon K-H, Lee J, Kim J, Shin A. Individual 5-Year Lung Cancer Risk Prediction Model in Korea Using a Nationwide Representative Database. Cancers. 2021; 13(14):3496. https://doi.org/10.3390/cancers13143496
Chicago/Turabian StyleYeo, Yohwan, Dong Wook Shin, Kyungdo Han, Sang Hyun Park, Keun-Hye Jeon, Jungkwon Lee, Junghyun Kim, and Aesun Shin. 2021. "Individual 5-Year Lung Cancer Risk Prediction Model in Korea Using a Nationwide Representative Database" Cancers 13, no. 14: 3496. https://doi.org/10.3390/cancers13143496