
Postoperative Radiochemotherapy Using Modern Radiotherapy Techniques in Elderly Patients with Head and Neck Squamous Cell Carcinoma: The Challenge of Weighing Up Benefits and Harms of Treatment Modalities in Clinical Practice


 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patient Cohort
2.2. Radiotherapy
2.3. Concomitant Systemic Treatment
2.4. Follow-Up Procedures and Toxicity Scoring
2.5. Statistics
3. Results
3.1. Patient and Tumor Characteristics
3.2. Radiochemotherapy
3.3. Toxicities
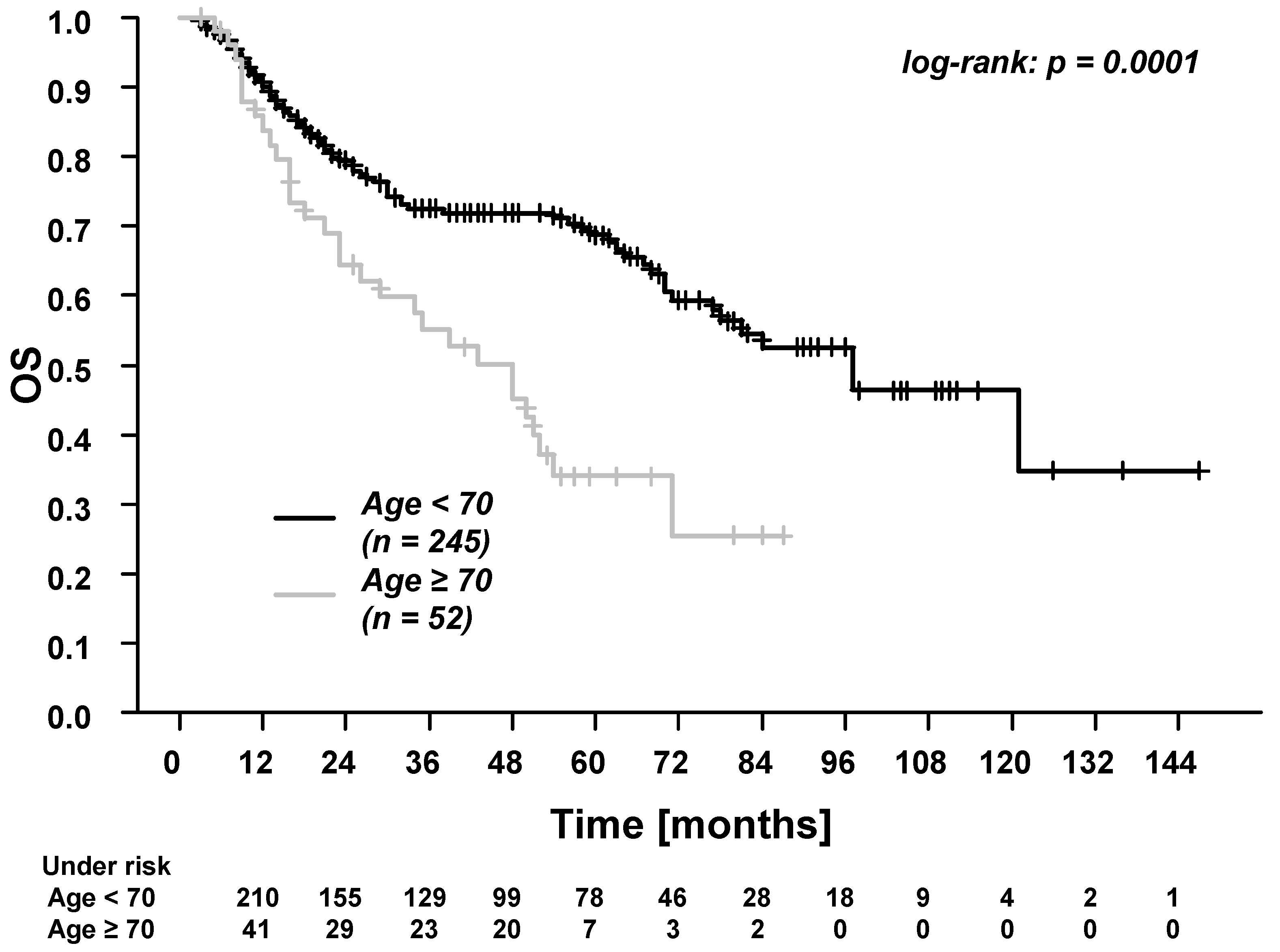
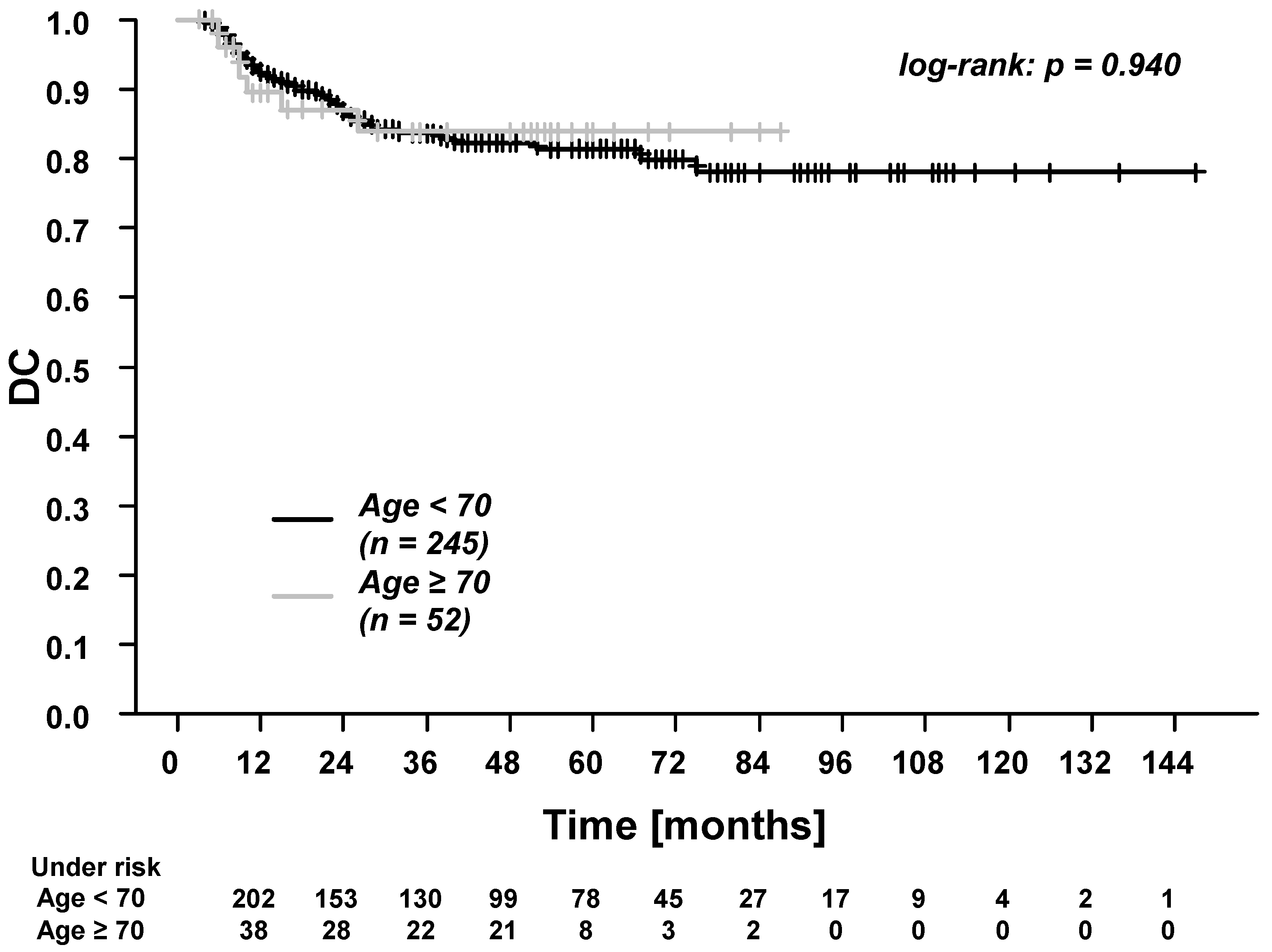
3.4. Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Prim. 2020, 6, 1–22. [Google Scholar] [CrossRef]
- Bernier, J.; Cooper, J.S.; Pajak, T.F.; Ir, M.V.G.; Bourhis, J.; Forastiere, A.; Ozsahin, E.M.; Jacobs, J.R.; Jassem, J.; Ang, K.-K.; et al. Defining risk levels in locally advanced head and neck cancers: A comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (#9501). Head Neck 2005, 27, 843–850. [Google Scholar] [CrossRef]
- Bernier, J.; Domenge, C.; Ozsahin, M.; Matuszewska, K.; Lefèbvre, J.-L.; Greiner, R.H.; Giralt, J.; Maingon, P.; Rolland, F.; Bolla, M.; et al. Postoperative Irradiation with or without Concomitant Chemotherapy for Locally Advanced Head and Neck Cancer. N. Engl. J. Med. 2004, 350, 1945–1952. [Google Scholar] [CrossRef] [Green Version]
- Cooper, J.S.; Pajak, T.F.; Forastiere, A.A.; Jacobs, J.; Campbell, B.; Saxman, S.B.; Kish, J.A.; Kim, H.E.; Cmelak, A.J.; Rotman, M.; et al. Postoperative Concurrent Radiotherapy and Chemotherapy for High-Risk Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2004, 350, 1937–1944. [Google Scholar] [CrossRef] [Green Version]
- Cooper, J.S.; Zhang, Q.; Pajak, T.F.; Forastiere, A.A.; Jacobs, J.; Saxman, S.B.; Kish, J.A.; Kim, H.E.; Cmelak, A.J.; Rotman, M.; et al. Long-term Follow-up of the RTOG 9501/Intergroup Phase III Trial: Postoperative Concurrent Radiation Therapy and Chemotherapy in High-Risk Squamous Cell Carcinoma of the Head and Neck. Int. J. Radiat. Oncol. 2012, 84, 1198–1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghosh-Laskar, S.; Yathiraj, P.H.; Dutta, D.; Rangarajan, V.; Purandare, N.C.; Gupta, T.; Budrukkar, A.; Murthy, V.; Kannan, S.; Agarwal, J.P. Prospective randomized controlled trial to compare 3-dimensional conformal radiotherapy to intensity-modulated radiotherapy in head and neck squamous cell carcinoma: Long-term results. Head Neck 2016, 38, E1481–E1487. [Google Scholar] [CrossRef] [PubMed]
- Gupta, T.; Agarwal, J.; Jain, S.; Phurailatpam, R.; Kannan, S.; Ghosh-Laskar, S.; Murthy, V.; Budrukkar, A.; Dinshaw, K.; Prabhash, K.; et al. Three-dimensional conformal radiotherapy (3D-CRT) versus intensity modulated radiation therapy (IMRT) in squamous cell carcinoma of the head and neck: A randomized controlled trial. Radiother. Oncol. 2012, 104, 343–348. [Google Scholar] [CrossRef]
- Van Der Veen, J.; Nuyts, S. Can Intensity-Modulated-Radiotherapy Reduce Toxicity in Head and Neck Squamous Cell Carcinoma? Cancers 2017, 9, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansen, J.; Eriksen, J.G.; on behalf of the Academy of Geriatric Cancer Research (AgeCare). Trends in cancer of the head and neck in the elderly in Denmark, 1980–2012. Acta Oncol. 2016, 55, 13–18. [Google Scholar] [CrossRef] [Green Version]
- Sarris, E.G.; Harrington, K.J.; Saif, M.W.; Syrigos, K.N. Multimodal treatment strategies for elderly patients with head and neck cancer. Cancer Treat. Rev. 2014, 40, 465–475. [Google Scholar] [CrossRef]
- Noronha, V.; Joshi, A.; Patil, V.M.; Agarwal, J.; Ghosh-Laskar, S.; Budrukkar, A.; Murthy, V.; Gupta, T.; D’Cruz, A.K.; Banavali, S.; et al. Once-a-Week Versus Once-Every-3-Weeks Cisplatin Chemoradiation for Locally Advanced Head and Neck Cancer: A Phase III Randomized Noninferiority Trial. J. Clin. Oncol. 2018, 36, 1064–1072. [Google Scholar] [CrossRef]
- Guigay, J.; Aupérin, A.; Fayette, J.; Saada-Bouzid, E.; Lafond, C.; Taberna, M.; Geoffrois, L.; Martin, L.; Capitain, O.; Cupissol, D.; et al. Cetuximab, docetaxel, and cisplatin versus platinum, fluorouracil, and cetuximab as first-line treatment in patients with recurrent or metastatic head and neck squamous-cell carcinoma (GORTEC 2014-01 TPExtreme): A multicentre, open-label, randomised, phase 2 trial. Lancet Oncol. 2021, 22, 463–475. [Google Scholar] [CrossRef]
- Shia, B.-C.; Qin, L.; Lin, K.-C.; Fang, C.-Y.; Tsai, L.-L.; Kao, Y.-W.; Wu, S.-Y. Outcomes for Elderly Patients Aged 70 to 80 Years or Older with Locally Advanced Oral Cavity Squamous Cell Carcinoma: A Propensity Score–Matched, Nationwide, Oldest Old Patient–Based Cohort Study. Cancers 2020, 12, 258. [Google Scholar] [CrossRef] [Green Version]
- Haehl, E.; Rühle, A.; David, H.; Kalckreuth, T.; Sprave, T.; Stoian, R.; Becker, C.; Knopf, A.; Grosu, A.-L.; Nicolay, N.H. Radiotherapy for geriatric head-and-neck cancer patients: What is the value of standard treatment in the elderly? Radiat. Oncol. 2020, 15, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Maggiore, R.; Zumsteg, Z.S.; BrintzenhofeSzoc, K.; Trevino, K.M.; Gajra, A.; Korc-Grodzicki, B.; Epstein, J.B.; Bond, S.M.; Parker, I.; Kish, J.A.; et al. The Older Adult With Locoregionally Advanced Head and Neck Squamous Cell Carcinoma: Knowledge Gaps and Future Direction in Assessment and Treatment. Int. J. Radiat. Oncol. 2017, 98, 868–883. [Google Scholar] [CrossRef] [Green Version]
- Machiels, J.-P.; Leemans, C.R.; Golusinski, W.; Grau, C.; Licitra, L.; Gregoire, V. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS–ESMO–ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1462–1475. [Google Scholar] [CrossRef] [PubMed]
- Grégoire, V.; Lefebvre, J.-L.; Licitra, L.; Felip, E. Squamous cell carcinoma of the head and neck: EHNS–ESMO–ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2010, 21, v184–v186. [Google Scholar] [CrossRef] [PubMed]
- Leitlinienprogramm Onkologie. S3-Leitlinie: Diagnostik, Therapie und Nachsorge des Larynxkarzinoms. Available online: https://www.leitlinienprogramm-onkologie.de/leitlinien/larynxkarzinom/ (accessed on 5 April 2021).
- Leitlinienprogramm Onkologie. S3-Leitlinie: Diagnostik und Therapie des Mundhöhlenkarzinoms. Available online: https://www.leitlinienprogramm-onkologie.de/leitlinien/mundhoehlenkarzinom/ (accessed on 5 April 2021).
- Beschel, L.M.; Leu, M.; Reichardt, S.D.; Rave-Fränk, M.; Schirmer, M.A.; Stadelmann, C.; Canis, M.; Wolff, H.A.; Reichardt, H.M. T cell abundance in blood predicts acute organ toxicity in chemoradiotherapy for head and neck cancer. Oncotarget 2016, 7, 65902–65915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grégoire, V.; Evans, M.; Le, Q.-T.; Bourhis, J.; Budach, V.; Chen, A.; Eisbruch, A.; Feng, M.; Giralt, J.; Gupta, T.; et al. Delineation of the primary tumour Clinical Target Volumes (CTV-P) in laryngeal, hypopharyngeal, oropharyngeal and oral cavity squamous cell carcinoma: AIRO, CACA, DAHANCA, EORTC, GEORCC, GORTEC, HKNPCSG, HNCIG, IAG-KHT, LPRHHT, NCIC CTG, NCRI, NRG Oncology, PHNS, SBRT, SOMERA, SRO, SSHNO, TROG consensus guidelines. Radiother. Oncol. 2018, 126, 3–24. [Google Scholar] [CrossRef] [Green Version]
- Grégoire, V.; Ang, K.; Budach, W.; Grau, C.; Hamoir, M.; Langendijk, J.A.; Lee, A.; Le, Q.-T.; Maingon, P.; Nutting, C.; et al. Delineation of the neck node levels for head and neck tumors: A 2013 update. DAHANCA, EORTC, HKNPCSG, NCIC CTG, NCRI, RTOG, TROG consensus guidelines. Radiother. Oncol. 2014, 110, 172–181. [Google Scholar] [CrossRef]
- Vorwerk, H.; Hess, C.F. Guidelines for delineation of lymphatic clinical target volumes for high conformal radiotherapy: Head and neck region. Radiat. Oncol. 2011, 6, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkpatrick, J.P.; van der Kogel, A.J.; Schultheiss, T.E. Radiation Dose–Volume Effects in the Spinal Cord. Int. J. Radiat. Oncol. 2010, 76, S42–S49. [Google Scholar] [CrossRef] [PubMed]
- Deasy, J.O.; Moiseenko, V.; Marks, L.; Chao, K.C.; Nam, J.; Eisbruch, A. Radiotherapy Dose–Volume Effects on Salivary Gland Function. Int. J. Radiat. Oncol. 2010, 76, S58–S63. [Google Scholar] [CrossRef] [Green Version]
- Rancati, T.; Schwarz, M.; Allen, A.M.; Feng, F.; Popovtzer, A.; Mittal, B.; Eisbruch, A. Radiation Dose–Volume Effects in the Larynx and Pharynx. Int. J. Radiat. Oncol. 2010, 76, S64–S69. [Google Scholar] [CrossRef] [Green Version]
- Wolff, H.A.; Bosch, J.; Jung, K.; Overbeck, T.; Hennies, S.; Matthias, C.; Hess, C.F.; Roedel, R.M.; Christiansen, P.D.H. High-Grade Acute Organ Toxicity as Positive Prognostic Factor in Primary Radio(chemo)therapy for Locally Advanced, Inoperable Head and Neck Cancer. Strahlenther. Onkol. 2010, 186, 262–268. [Google Scholar] [CrossRef]
- Wolff, H.A.; Overbeck, T.; Roedel, R.M.; Hermann, R.M.; Herrmann, M.K.A.; Kertesz, T.; Vorwerk, H.; Hille, A.; Matthias, C.; Hess, C.F.; et al. Toxicity of daily low dose cisplatin in radiochemotherapy for locally advanced head and neck cancer. J. Cancer Res. Clin. Oncol. 2008, 135, 961–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonner, J.A.; Harari, P.M.; Giralt, J.; Azarnia, N.; Shin, D.M.; Cohen, R.B.; Jones, C.U.; Sur, R.; Raben, D.; Jassem, J.; et al. Radiotherapy plus Cetuximab for Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2006, 354, 567–578. [Google Scholar] [CrossRef] [Green Version]
- US Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE), Version 5.0; US Department of Health and Human Services: Washington, DC, USA; Bethesda: Rockville, MD, USA, 2010. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 6 April 2021).
- Rubin, P.; Constine, L.S.; Fajardo, L.F.; Phillips, T.L.; Wasserman, T.H. Overview: Late effects of normal tissues (LENT) scoring system. Int. J. Radiat. Oncol. 1995, 31, 1041–1042. [Google Scholar] [CrossRef]
- Gross, A.; Ziepert, M.; Scholz, M. KMWin—A Convenient Tool for Graphical Presentation of Results from Kaplan-Meier Survival Time Analysis. PLoS ONE 2012, 7, e38960. [Google Scholar] [CrossRef]
- Lichtman, S.M.; Brain, E. The International Society of Geriatric Oncology conference: Paris 2011. Aging Heal. 2012, 8, 123–126. [Google Scholar] [CrossRef]
- SIOG: International Society of Geriatric Oncology. Defining the Elderly. Available online: http://siog.org/content/defining-elderly (accessed on 8 April 2021).
- Tomo, S.; Neto, S.; Collado, F.; Sundefeld, M.; Bernabé, D.; Biasoli, Ér.; Miyahara, G. Head and neck squamous cell carcinoma in young patients: A 26-year clinicopathologic retrospective study in a Brazilian specialized center. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e416–e424. [Google Scholar] [CrossRef] [PubMed]
- Contreras, J.A.; Spencer, C.; DeWees, T.; Haughey, B.; Henke, L.E.; Chin, R.-I.; Paniello, R.; Rich, J.; Jackson, R.; Oppelt, P.; et al. Eliminating Postoperative Radiation to the Pathologically Node-Negative Neck: Long-Term Results of a Prospective Phase II Study. J. Clin. Oncol. 2019, 37, 2548–2555. [Google Scholar] [CrossRef] [PubMed]
- Moura, J.; Câmara, A.C.D.S.M.; Nonaka, C.; Pinto, L.P.; De Souza, L.B. Immunohistochemical comparative analysis of lymphatic vessel density and VEGF-C expression in squamous cell carcinomas of the tongue between young and old patients. Pathol. Res. Pr. 2016, 212, 1095–1101. [Google Scholar] [CrossRef]
- Ahn, D.; Lee, G.J.; Sohn, J.H.; Lee, J.E. Phase II trial of individualized/dynamic cisplatin regimens for definitive concurrent chemoradiation therapy in patients with head and neck squamous cell carcinoma. Cancer Med. 2020, 9, 9256–9265. [Google Scholar] [CrossRef]
- Giacalone, N.J.; Qureshi, M.M.; Mak, K.S.; Kirke, D.; Patel, S.A.; Shah, B.A.; Salama, A.R.; Jalisi, S.; Truong, M.T. Adjuvant chemoradiation does not improve survival in elderly patients with high-risk resected head and neck cancer. Laryngoscope 2018, 128, 831–840. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Bonventre, J.V.; Parrish, A.R. The Aging Kidney: Increased Susceptibility to Nephrotoxicity. Int. J. Mol. Sci. 2014, 15, 15358–15376. [Google Scholar] [CrossRef] [Green Version]
- Hurria, A.; Togawa, K.; Mohile, S.G.; Owusu, C.; Klepin, H.D.; Gross, C.P.; Lichtman, S.; Gajra, A.; Bhatia, S.; Katheria, V.; et al. Predicting Chemotherapy Toxicity in Older Adults With Cancer: A Prospective Multicenter Study. J. Clin. Oncol. 2011, 29, 3457–3465. [Google Scholar] [CrossRef] [Green Version]
- Szturz, P.; Vermorken, J.B. Treatment of Elderly Patients with Squamous Cell Carcinoma of the Head and Neck. Front. Oncol. 2016, 6, 199. [Google Scholar] [CrossRef] [Green Version]
- Szturz, P.; Wouters, K.; Kiyota, N.; Tahara, M.; Prabhash, K.; Noronha, V.; Adelstein, D.; Van Gestel, D.; Vermorken, J.B. Low-Dose vs. High-Dose Cisplatin: Lessons Learned From 59 Chemoradiotherapy Trials in Head and Neck Cancer. Front. Oncol. 2019, 9, 86. [Google Scholar] [CrossRef] [Green Version]
- Ahn, M.-J.; D’Cruz, A.; Vermorken, J.B.; Chen, J.-P.; Chitapanarux, I.; Dang, H.Q.T.; Guminski, A.; Kannarunimit, D.; Lin, T.-Y.; Ng, W.T.; et al. Clinical recommendations for defining platinum unsuitable head and neck cancer patient populations on chemoradiotherapy: A literature review. Oral Oncol. 2016, 53, 10–16. [Google Scholar] [CrossRef] [Green Version]
- MDApp. Charlson Comorbidity Index Calculator. Available online: https://www.mdapp.co/charlson-comorbidity-index-cci-calculator-131/ (accessed on 9 April 2021).
- Moye, V.A.; Chandramouleeswaran, S.; Zhao, N.; Muss, H.B.; Weissler, M.C.; Hayes, D.N.; Zevallos, J.P. Elderly Patients with Squamous Cell Carcinoma of the Head and Neck and the Benefit of Multimodality Therapy. Oncologist 2015, 20, 159–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, A.; Mohanti, B.K.; Thakar, A.; Bahadur, S.; Bhasker, S. Concomitant chemoradiation versus radical radiotherapy in advanced squamous cell carcinoma of oropharynx and nasopharynx using weekly cisplatin: A phase II randomized trial. Ann. Oncol. 2010, 21, 2272–2277. [Google Scholar] [CrossRef] [PubMed]
- Von Der Grün, J.M.; Martin, D.; Stöver, T.; Ghanaati, S.; Rödel, C.; Balermpas, P. Chemoradiotherapy as Definitive Treatment for Elderly Patients with Head and Neck Cancer. Biomed Res. Int. 2018, 2018, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.; Noronha, V.; Patil, V.; Menon, N.; Joshi, A.; Prabhash, K. Safety and efficacy of concurrent chemoradiotherapy for head and neck cancers in younger versus older patients: Post hoc analysis of a randomized control trial. Ann. Oncol. 2020, 31, S1351. [Google Scholar] [CrossRef]
- Brown, M.L.; Glanzmann, C.; Huber, G.; Bredell, M.; Rordorf, T.; Studer, G. IMRT/VMAT for malignancies in the head-and-neck region: Outcome in patients aged 80. Strahlenther. Onkol. 2016, 192, 526–536. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Age, <70 Years (n = 245) | Age, ≥70 Years (n = 52) | p-Value |
|---|---|---|---|
| Age (years) | 58 (23–69) | 73 (70–85) | - |
| Sex | 0.52 | ||
| Female | 47 (19.2) | 8 (15.4) | |
| Male | 198 (80.8) | 44 (84.6) | |
| Charlson Comorbidity Index | <0.01 | ||
| 0–3 | 125 (51.0) | 0 (0.0) | |
| 4–7 | 119 (48.6) | 51 (98.1) | |
| 8–10 | 1 (0.4) | 1 (1.9) | |
| Tumor localization | 0.26 | ||
| Hypopharynx | 47 (19.2) | 6 (11.5) | |
| Larynx | 37 (15.1) | 13 (25.0) | |
| Oral cavity | 85 (34.7) | 18 (34.6) | |
| Oropharynx | 76 (31.0) | 15 (28.8) | |
| HPV status | 0.63 | ||
| Positive | 21 (27.6) | 3 (20.0) | |
| Negative | 29 (38.2) | 6 (40.0) | |
| Undetermined | 26 (34.2) | 6 (40.0) | |
| Grading | 0.76 | ||
| G1 | 9 (3.7) | 1 (1.9) | |
| G2 | 193 (78.8) | 41 (78.8) | |
| G3 | 41 (16.7) | 10 (19.2) | |
| Undetermined | 2 (0.8) | 0 (0.0) | |
| pT status | 0.09 | ||
| T0 | 5 (2.0) | 4 (7.7) | |
| T1 | 38 (15.5) | 6 (11.5) | |
| T2 | 61 (24.9) | 12 (23.1) | |
| T3 | 85 (34.7) | 13 (25.0) | |
| T4 | 56 (22.9) | 17 (32.7) | |
| pN status | <0.01 | ||
| N0 | 56 (22.9) | 24 (46.1) | |
| N1 | 55 (22.4) | 8 (15.4) | |
| N2 | 119 (48.6) | 8 (15.4) | |
| N3 | 15 (6.1) | 12 (23.1) | |
| Presence of ECE | 0.36 | ||
| Yes | 64 (34.0) | 12 (42.9) | |
| AJCC classification (8th edition, 2017) 1 | 0.86 | ||
| I 1 | 18 (7.3) | 3 (5.8) | |
| II 1 | 16 (6.5) | 5 (9.6) | |
| III | 75 (30.6) | 15 (28.8) | |
| IV | 136 (55.5) | 29 (55.8) | |
| Resection status | 0.59 | ||
| R0 | 235 (95.9) | 49 (94.2) | |
| R1 | 10 (4.1) | 3 (5.9) |
| Characteristics | Age, <70 Years (n = 245) | Age, ≥70 Years (n = 52) | p-Value |
|---|---|---|---|
| Radiotherapy | |||
| Technique | 0.77 * | ||
| VMAT | 142 (58.0) | 29 (55.8) | |
| IMRT | 103 (42.0) | 23 (44.2) | |
| Dose, planned [Gy] | 64.0 (54.0–66.0) | 64.0 (62.4–66.0) | 0.47 # |
| Dose, administered [Gy] | 64.0 (38.0–66.0) | 64.0 (54.0–64.0) | 0.33 # |
| Dose received | 0.28 * | ||
| 100% of planned dose | 231 (94.3) | 51 (98.1) | |
| ≥80–<100% of planned dose | 11 (4.5) | 1 (1.9) | |
| <80% of planned dose | 3 (1.2) | 0 (0.0) | |
| Interruptions/breaks | 117 (47.8) | 29 (55.8) | 0.29 * |
| Systemic treatment | |||
| Received concomitant systemic treatment | 192 (78.4) | 31 (59.6) | 0.04 * |
| Received <100% of planned dose | 72 (37.5) | 17 (54.8) | 0.07 * |
| Systemic treatment type | <0.01 * | ||
| Cetuximab | 3 (1.2) | 3 (9.7) | |
| Cisplatin | 189 (98.8) | 28 (90.3) | |
| Cisplatin regimen | 0.51 * | ||
| 6 mg/m2/d daily | 116 (61.4) | 14 (50.0) | |
| 20 mg/m2/d1–5 (2 cycles) | 0 (0.0) | 1 (3.6) | |
| 40 mg/m2/d weekly | 73 (38.6) | 13 (46.4) |
| Toxicities | Age, <70 Year (n = 245) | Age, ≥70 Years (n = 52) | p-Value |
|---|---|---|---|
| Acute organ toxicity | |||
| Mucositis | 0.03 | ||
| 0 | 13 (5.3) | 9 (17.3) | |
| 1 | 57 (23.3) | 14 (26.9) | |
| 2 | 148 (60.4) | 24 (46.2) | |
| 3 | 25 (10.2) | 5 (9.6) | |
| 4 | 2 (0.8) | 0 (0.0) | |
| ≥grade 3 | 27 (11.0) | 5 (9.6) | 0.91 |
| Dermatitis | <0.01 | ||
| 0 | 6 (2.4) | 7 (13.5) | |
| 1 | 133 (54.3) | 29 (55.8) | |
| 2 | 100 (40.8) | 15 (28.8) | |
| 3 | 6 (2.4) | 1 (1.9) | |
| ≥grade 3 | 6 (2.4) | 1 (1.9) | 0.82 |
| Dysphagia | 0.23 | ||
| 0 | 29 (11.8) | 4 (7.7) | |
| 1 | 41 (16.7) | 5 (9.6) | |
| 2 | 48 (19.6) | 14 (26.9) | |
| 3 | 118 (48.2) | 29 (55.8) | |
| 4 | 9 (3.7) | 0 (0.0) | |
| ≥grade 3 | 127 (52.2) | 29 (55.8) | 0.64 |
| Received feeding tube before RCT | 64 (26.1) | 19 (36.5) | 0.13 |
| Received feeding tube during RCT | 65 (26.5) | 15 (28.8) | 0.73 |
| Overall acute organ toxicity, ≥grade 3 | 137 (55.9) | 30 (57.7) | 0.82 |
| Hematologic toxicity | |||
| Overall hematologic toxicity, ≥grade 3 | 62 (25.3) | 11 (21.2) | 0.53 |
| Anemia, ≥grade 3 | 6 (2.4) | 2 (3.8) | 0.57 |
| Leukopenia, ≥grade 3 | 55 (22.4) | 10 (19.2) | 0.61 |
| Thrombopenia, ≥grade 3 | 10 (4.1) | 0 (0.0) | 0.59 |
| Overall late toxicity, ≥grade 2 * | 90 (40.5) | 17 (37.8) | 0.73 |
| Overall late toxicity, ≥grade 3 * | 31 (14.0) | 3 (6.7) | 0.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leu, M.; Patzer, C.; Guhlich, M.; Possiel, J.; Pilavakis, Y.; Schirmer, M.A.; Rieken, S.; Dröge, L.H. Postoperative Radiochemotherapy Using Modern Radiotherapy Techniques in Elderly Patients with Head and Neck Squamous Cell Carcinoma: The Challenge of Weighing Up Benefits and Harms of Treatment Modalities in Clinical Practice. Cancers 2021, 13, 3384. https://doi.org/10.3390/cancers13143384
Leu M, Patzer C, Guhlich M, Possiel J, Pilavakis Y, Schirmer MA, Rieken S, Dröge LH. Postoperative Radiochemotherapy Using Modern Radiotherapy Techniques in Elderly Patients with Head and Neck Squamous Cell Carcinoma: The Challenge of Weighing Up Benefits and Harms of Treatment Modalities in Clinical Practice. Cancers. 2021; 13(14):3384. https://doi.org/10.3390/cancers13143384
Chicago/Turabian StyleLeu, Martin, Christoph Patzer, Manuel Guhlich, Jacqueline Possiel, Yiannis Pilavakis, Markus Anton Schirmer, Stefan Rieken, and Leif Hendrik Dröge. 2021. "Postoperative Radiochemotherapy Using Modern Radiotherapy Techniques in Elderly Patients with Head and Neck Squamous Cell Carcinoma: The Challenge of Weighing Up Benefits and Harms of Treatment Modalities in Clinical Practice" Cancers 13, no. 14: 3384. https://doi.org/10.3390/cancers13143384