
Serum HPV16 E7 Oncoprotein Is a Recurrence Marker of Oropharyngeal Squamous Cell Carcinomas

 ,
,  , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Samples
2.2. Nucleic Acid Extraction
2.3. HPV Analysis
2.4. Gene Expression Analysis
2.5. Detection of Serum HPV16 L1 Antibodies
2.6. Serum E7 Oncoprotein Level Detection
2.7. Statistical Analysis
3. Results
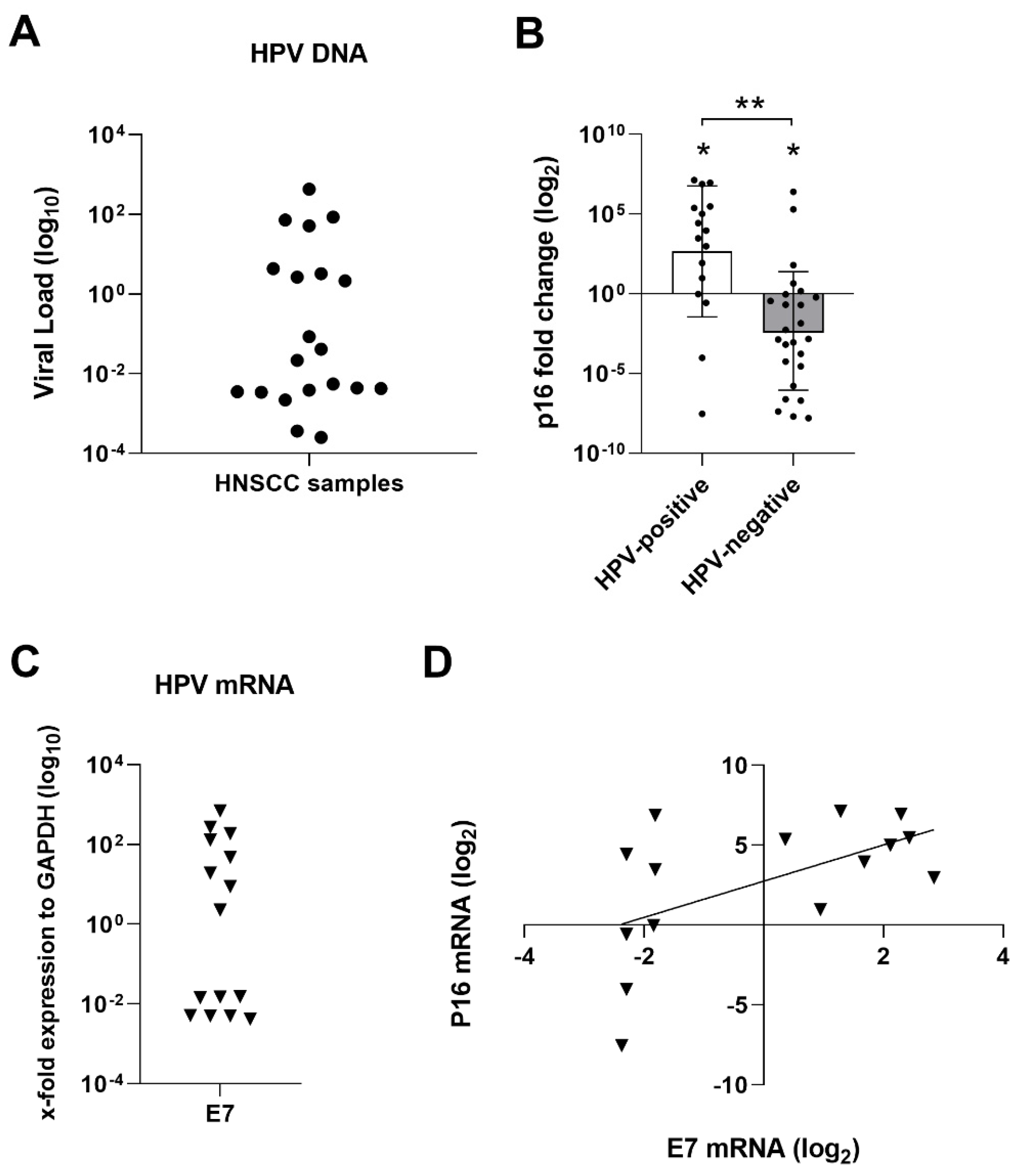
3.1. HPV DNA Analysis
3.2. p16 Gene Expression
3.3. HPV mRNA Expression
3.4. Serological Studies
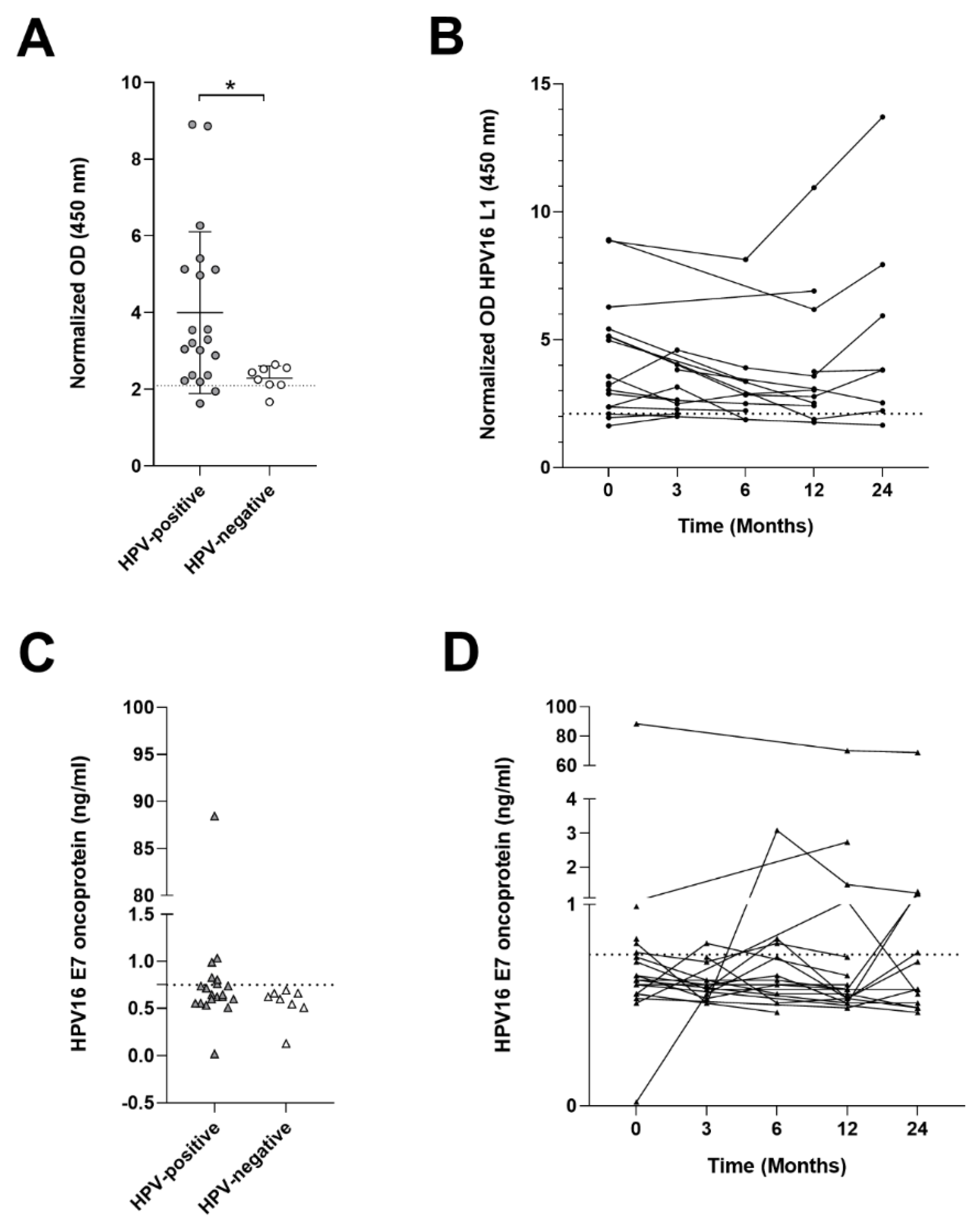
3.4.1. HPV16 L1 Antibody Titer
3.4.2. HPV16 E7 Oncoproteins in Sera
3.5. Survival Analysis
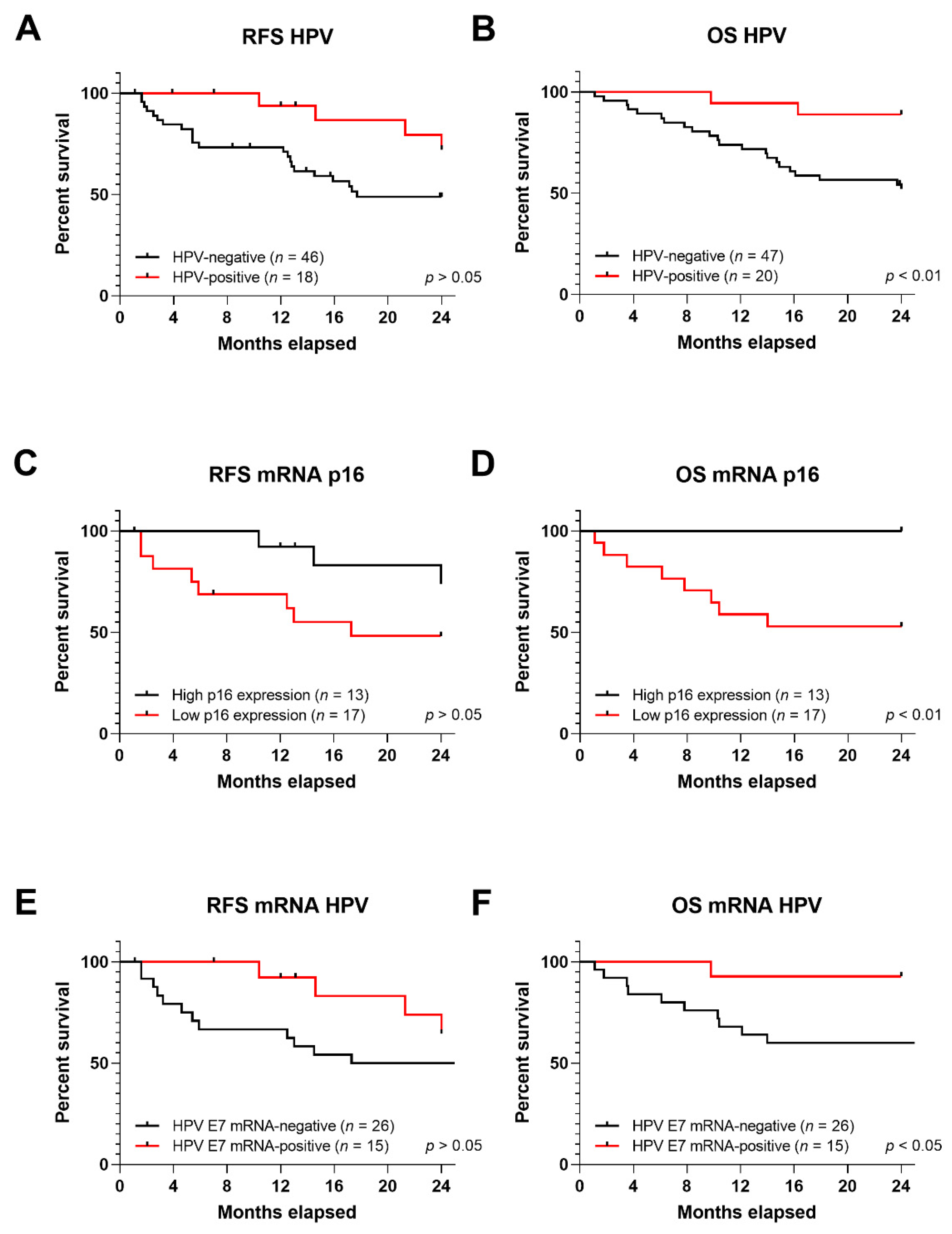
3.5.1. RFS and OS in Correlation to HPV DNA, p16 Expression and HPV mRNA
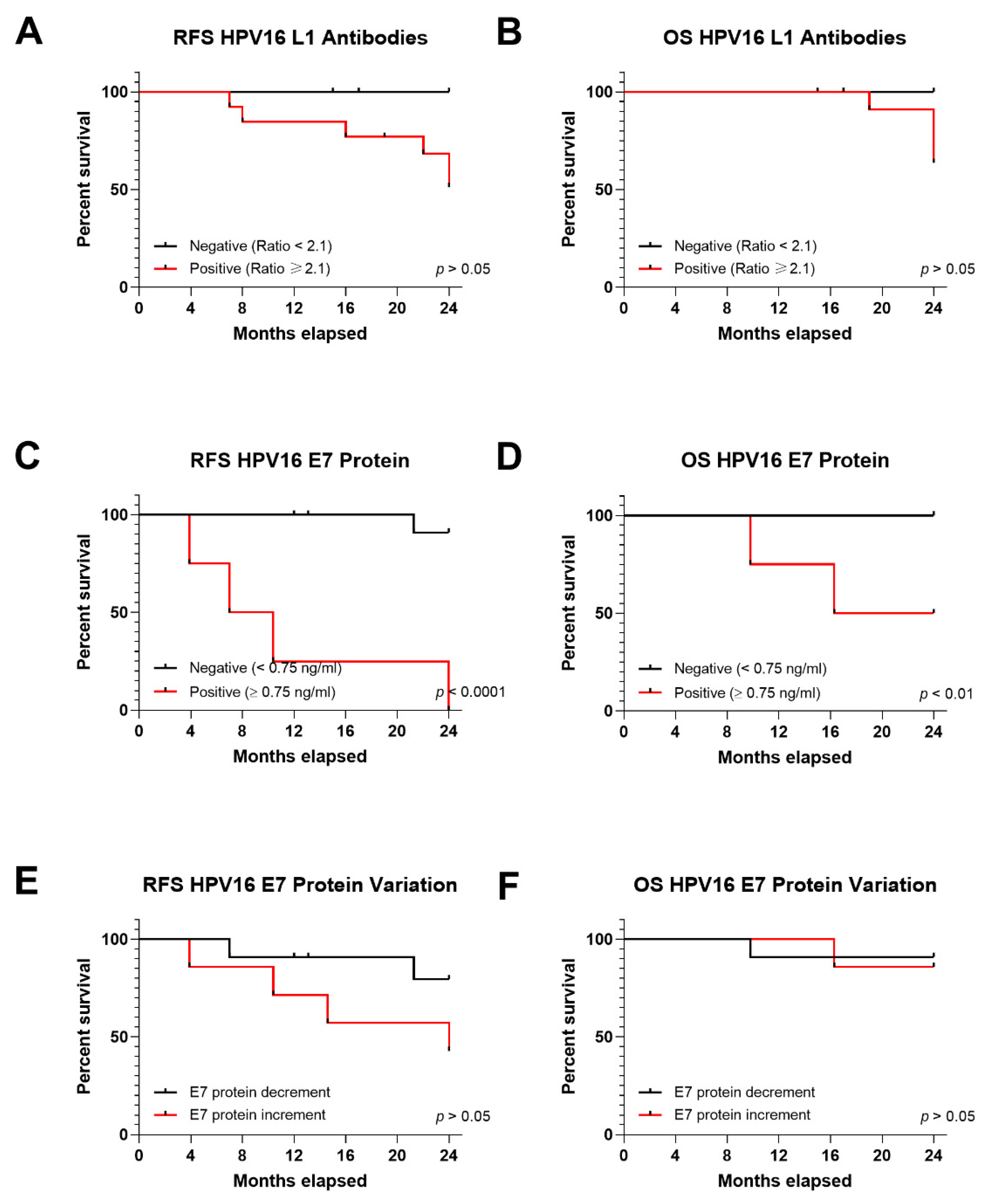
3.5.2. RFS and OS in Relation to Serum HPV16 L1 Antibodies
3.5.3. RFS and OS in Relation to Serum HPV16 E7 Oncoprotein
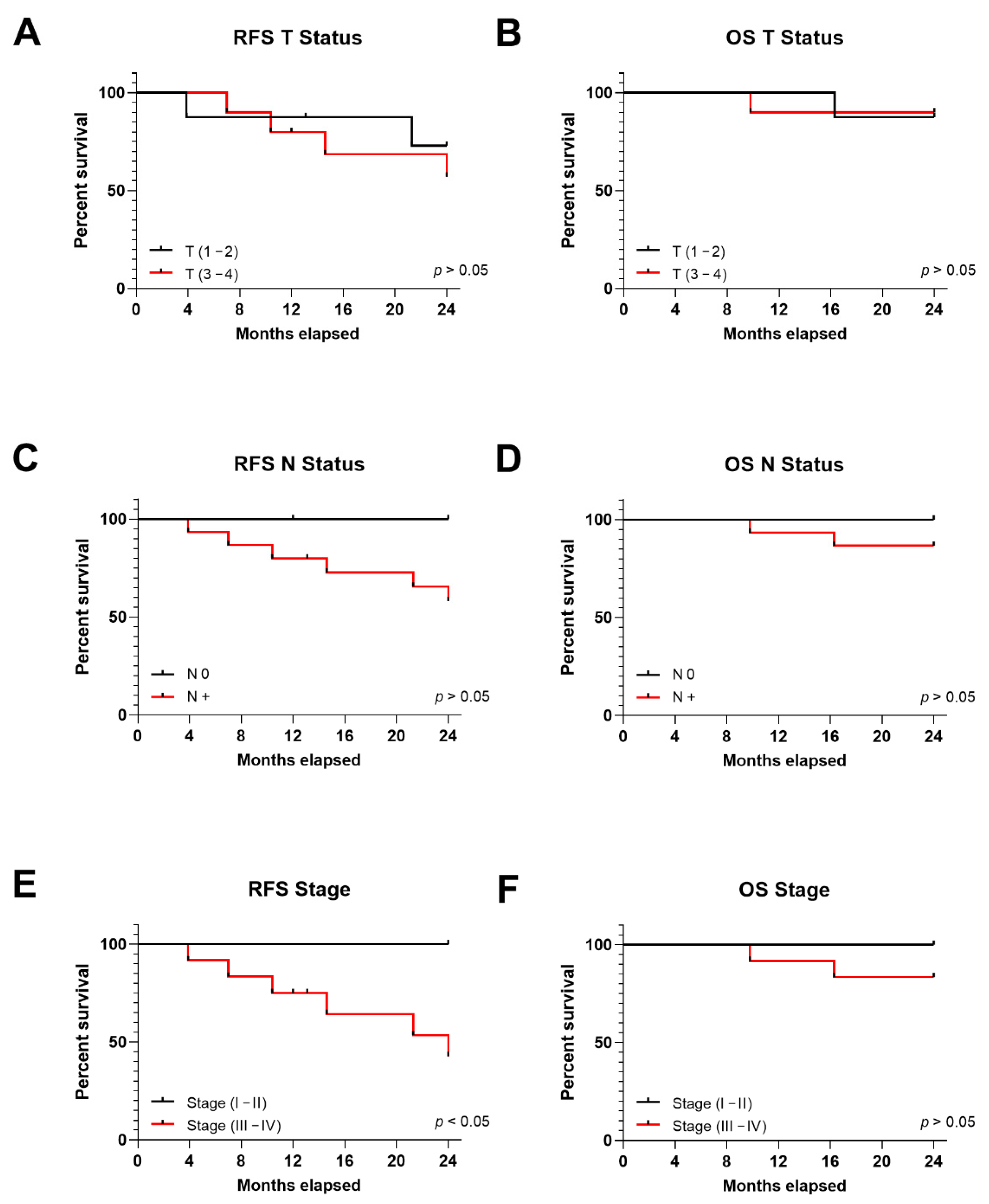
3.6. TNM Stage in Correlation to OPSCC Patient Prognosis and E7 Oncoprotein in Serum
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Primers 2020, 6, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Bruni, L.; Albero, G.; Serrano, B.; Mena, M.; Gómez, D.; Muñoz, J.; Bosch, F.X.; de Sanjose, S. Human Papillomavirus and Related Diseases in Europe. Summary Report 17 June 2019; ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre): Barcelona, Spain, 2019. [Google Scholar]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [Green Version]
- Wittekindt, C.; Wagner, S.; Bushnak, A.; Prigge, E.-S.; von Knebel Doeberitz, M.; Würdemann, N.; Bernhardt, K.; Pons-Kühnemann, J.; Maulbecker-Armstrong, C.; Klussmann, J.P. Increasing incidence rates of oropharyngeal squamous cell carcinoma in germany and significance of disease burden attributed to human papillomavirus. Cancer Prev. Res. 2019, 12, 375–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. (Eds.) AJCC Cancer Staging Manual; Springer: Chicago, IL, USA, 2017; ISBN 978-3-319-40617-6. [Google Scholar]
- Lydiatt, W.M.; Patel, S.G.; O’Sullivan, B.; Brandwein, M.S.; Ridge, J.A.; Migliacci, J.C.; Loomis, A.M.; Shah, J.P. Head and neck cancers-major changes in the American joint committee on cancer eighth edition cancer staging Manual. CA Cancer J. Clin. 2017, 67, 122–137. [Google Scholar] [CrossRef] [PubMed]
- De Cicco, R.; Melo Menezes, R.; Nicolau, U.R.; Pinto, C.A.L.; Villa, L.L.; Kowalski, L.P. Impact of human papillomavirus status on survival and recurrence in a geographic region with a low prevalence of HPV-related cancer: A retrospective cohort study. Head Neck 2020, 42, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Klimentová, J.; Göckel-Krzikalla, E.; Ly, R.; Gmelin, N.; Hotz-Wagenblatt, A.; Řehulková, H.; Stulík, J.; Rösl, F.; Niebler, M. Combined transcriptome and proteome analysis of immortalized human keratinocytes expressing human papillomavirus 16 (HPV16) oncogenes reveals novel key factors and networks in HPV-induced carcinogenesis. Msphere 2019, 4, e00129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hargreaves, S.; Beasley, M.; Hurt, C.; Jones, T.M.; Evans, M. Deintensification of adjuvant treatment after transoral surgery in patients with human papillomavirus-positive oropharyngeal cancer: The conception of the PATHOS study and its development. Front. Oncol. 2019, 9, 936. [Google Scholar] [CrossRef] [Green Version]
- Mirghani, H.; Blanchard, P. Treatment de-escalation for HPV-driven oropharyngeal cancer: Where do we stand? Clin. Transl. Radiat. Oncol. 2018, 8, 4–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, S.; Evans, D.; Mehanna, H.; Parish, J.L. Modelling human papillomavirus biology in oropharyngeal keratinocytes. Philos. Trans. R. Soc. B 2019, 374, 20180289. [Google Scholar] [CrossRef] [Green Version]
- Cohen, E.E.W.; Bell, R.B.; Bifulco, C.B.; Burtness, B.; Gillison, M.L.; Harrington, K.J.; Le, Q.-T.; Lee, N.Y.; Leidner, R.; Lewis, R.L.; et al. The society for immunotherapy of cancer consensus statement on immunotherapy for the treatment of squamous cell carcinoma of the head and neck (HNSCC). J. Immunother. Cancer 2019, 7, 184. [Google Scholar] [CrossRef] [Green Version]
- Economopoulou, P.; Koutsodontis, G.; Avgeris, M.; Strati, A.; Kroupis, C.; Pateras, I.; Kirodimos, E.; Giotakis, E.; Kotsantis, I.; Maragoudakis, P.; et al. HPV16 E6/E7 Expression in circulating tumor cells in oropharyngeal squamous cell cancers: A pilot study. PLoS ONE 2019, 14, e0215984. [Google Scholar] [CrossRef]
- Mehanna, H.; Robinson, M.; Hartley, A.; Kong, A.; Foran, B.; Fulton-Lieuw, T.; Dalby, M.; Mistry, P.; Sen, M.; O’Toole, L.; et al. Radiotherapy plus cisplatin or cetuximab in low-risk human papillomavirus-positive oropharyngeal cancer (De-ESCALaTE HPV): An open-label randomised controlled phase 3 trial. Lancet 2019, 393, 51–60. [Google Scholar] [CrossRef] [Green Version]
- Reuschenbach, M.; Tinhofer, I.; Wittekindt, C.; Wagner, S.; Klussmann, J.P. A systematic review of the HPV-attributable fraction of oropharyngeal squamous cell carcinomas in Germany. Cancer Med. 2019, 8, 1908–1918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lechner, M.; Chakravarthy, A.R.; Walter, V.; Masterson, L.; Feber, A.; Jay, A.; Weinberger, P.M.; McIndoe, R.A.; Forde, C.T.; Chester, K.; et al. Frequent HPV-independent P16/INK4A overexpression in head and neck cancer. Oral Oncol. 2018, 83, 32–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitamura, K.; Nimura, K.; Ito, R.; Saga, K.; Inohara, H.; Kaneda, Y. Evaluation of HPV16 E7 expression in head and neck carcinoma cell lines and clinical specimens. Sci. Rep. 2020, 10, 22138. [Google Scholar] [CrossRef] [PubMed]
- Van Abel, K.M.; Moore, E.J. Focus issue: Neck dissection for oropharyngeal squamous cell carcinoma. ISRN Surg. 2012, 2012, 547017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holzinger, D.; Wichmann, G.; Baboci, L.; Michel, A.; Höfler, D.; Wiesenfarth, M.; Schroeder, L.; Boscolo-Rizzo, P.; Herold-Mende, C.; Dyckhoff, G.; et al. Sensitivity and specificity of antibodies against HPV16 E6 and other early proteins for the detection of HPV16-driven oropharyngeal squamous cell carcinoma. Int. J. Cancer 2017, 140, 2748–2757. [Google Scholar] [CrossRef] [Green Version]
- Dahlstrom, K.R.; Anderson, K.S.; Cheng, J.N.; Chowell, D.; Li, G.; Posner, M.; Sturgis, E.M. HPV serum antibodies as predictors of survival and disease progression in patients with HPV-positive squamous cell carcinoma of the oropharynx. Clin. Cancer Res. 2015, 21, 2861–2869. [Google Scholar] [CrossRef] [Green Version]
- Piontek, T.; Harmel, C.; Pawlita, M.; Carow, K.; Schröter, J.; Runnebaum, I.B.; Dürst, M.; Graw, F.; Waterboer, T. Post-treatment human papillomavirus antibody kinetics in cervical cancer patients. Phil. Trans. R. Soc. B 2019, 374, 20180295. [Google Scholar] [CrossRef] [Green Version]
- Spector, M.E.; Sacco, A.G.; Bellile, E.; Taylor, J.M.G.; Jones, T.; Sun, K.; Brown, W.C.; Birkeland, A.C.; Bradford, C.R.; Wolf, G.T.; et al. E6 and E7 antibody levels are potential biomarkers of recurrence in patients with advanced-stage human papillomavirus-positive oropharyngeal squamous cell carcinoma. Clin. Cancer Res. 2017, 23, 2723–2729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang Kuhs, K.A.; Kreimer, A.R.; Trivedi, S.; Holzinger, D.; Pawlita, M.; Pfeiffer, R.M.; Gibson, S.P.; Schmitt, N.C.; Hildesheim, A.; Waterboer, T.; et al. Human papillomavirus 16 E6 antibodies are sensitive for human papillomavirus-driven oropharyngeal cancer and are associated with recurrence. Cancer 2017, 123, 4382–4390. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.-S.; Smith-McCune, K.; Darragh, T.M.; Lai, Y.; Lin, J.-H.; Chang, T.-C.; Guo, H.-Y.; Kesler, T.; Carter, A.; Castle, P.E.; et al. Direct human papillomavirus E6 whole-cell enzyme-linked immunosorbent assay for objective measurement of E6 oncoproteins in cytology samples. Clin. Vaccine Immunol. 2012, 19, 1474–1479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, L.; Xiao, X.; Lou, H.; Liu, P.; Song, S.; Liu, M.; Xu, T.; Zhang, Y.; Li, C.; Guan, R.; et al. Analysis of the role of the human papillomavirus 16/18 E7 protein assay in screening for cervical intraepithelial neoplasia: A case control study. BMC Cancer 2020, 20, 999. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Cho, Y.S.; Cho, M.C.; Shim, J.H.; Lee, K.A.; Ko, K.K.; Choe, Y.K.; Park, S.N.; Hoshino, T.; Kim, S.; et al. Both E6 and E7 oncoproteins of human papillomavirus 16 inhibit IL-18-induced IFN-gamma production in human peripheral blood mononuclear and NK cells. J. Immunol. 2001, 167, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Rotondo, J.C.; Oton-Gonzalez, L.; Mazziotta, C.; Lanzillotti, C.; Iaquinta, M.R.; Tognon, M.; Martini, F. Simultaneous detection and viral DNA load quantification of different human papillomavirus types in clinical specimens by the high analytical droplet digital PCR method. Front. Microbiol. 2020, 11, 591452. [Google Scholar] [CrossRef] [PubMed]
- Tognon, M.; Tagliapietra, A.; Magagnoli, F.; Mazziotta, C.; Oton-Gonzalez, L.; Lanzillotti, C.; Vesce, F.; Contini, C.; Rotondo, J.C.; Martini, F. Investigation on spontaneous abortion and human papillomavirus infection. Vaccines 2020, 8, 473. [Google Scholar] [CrossRef]
- Oton-Gonzalez, L.; Rotondo, J.C.; Cerritelli, L.; Malagutti, N.; Lanzillotti, C.; Bononi, I.; Ciorba, A.; Bianchini, C.; Mazziotta, C.; De Mattei, M.; et al. Association between oncogenic human papillomavirus type 16 and Killian polyp. Infect. Agent Cancer 2021, 16, 3. [Google Scholar] [CrossRef]
- Olthof, N.C.; Speel, E.-J.M.; Kolligs, J.; Haesevoets, A.; Henfling, M.; Ramaekers, F.C.S.; Preuss, S.F.; Drebber, U.; Wieland, U.; Silling, S.; et al. Comprehensive analysis of HPV16 integration in OSCC reveals no significant impact of physical status on viral oncogene and virally disrupted human gene expression. PLoS ONE 2014, 9, e88718. [Google Scholar] [CrossRef] [PubMed]
- Rotondo, J.C.; Giari, L.; Guerranti, C.; Tognon, M.; Castaldelli, G.; Fano, E.A.; Martini, F. Environmental doses of perfluorooctanoic acid change the expression of genes in target tissues of common carp. Environ. Toxicol. Chem. 2018, 37, 942–948. [Google Scholar] [CrossRef]
- Mazzoni, E.; Bononi, I.; Benassi, M.S.; Picci, P.; Torreggiani, E.; Rossini, M.; Simioli, A.; Casali, M.V.; Rizzo, P.; Tognon, M.; et al. Serum antibodies against simian virus 40 large T antigen, the viral oncoprotein, in osteosarcoma patients. Front. Cell Dev. Biol. 2018, 6, 64. [Google Scholar] [CrossRef]
- Pietrobon, S.; Bononi, I.; Lotito, F.; Perri, P.; Violanti, S.; Mazzoni, E.; Martini, F.; Tognon, M.G. Specific detection of serum antibodies against BKPyV, a small DNA tumour virus, in patients affected by choroidal nevi. Front. Microbiol. 2017, 8, 2059. [Google Scholar] [CrossRef]
- Contini, C.; Rotondo, J.C.; Magagnoli, F.; Maritati, M.; Seraceni, S.; Graziano, A.; Poggi, A.; Capucci, R.; Vesce, F.; Tognon, M.; et al. Investigation on silent bacterial infections in specimens from pregnant women affected by spontaneous miscarriage. J. Cell Physiol. 2018, 234, 100–107. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Cai, S.; Liu, S.; Feng, H.; Zhang, J. Bioinformatics analysis to screen the key prognostic genes in ovarian cancer. J. Ovarian Res. 2017, 10, 27. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer. Human Papillomaviruses: IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; IARC: Lyon, France, 2007; Volume 90, ISBN 978-92-832-1290-4. [Google Scholar]
- Castellsagué, X.; Alemany, L.; Quer, M.; Halec, G.; Quirós, B.; Tous, S.; Clavero, O.; Alòs, L.; Biegner, T.; Szafarowski, T.; et al. HPV involvement in head and neck cancers: Comprehensive assessment of biomarkers in 3680 patients. J. Natl. Cancer Inst. 2016, 108, djv403. [Google Scholar] [CrossRef]
- Betiol, J.; Villa, L.L.; Sichero, L. Impact of HPV infection on the development of head and neck cancer. Braz. J. Med. Biol. Res. 2013, 46, 217–226. [Google Scholar] [CrossRef] [Green Version]
- McIlwain, W.R.; Sood, A.J.; Nguyen, S.A.; Day, T.A. Initial symptoms in patients with HPV-positive and HPV-negative oropharyngeal cancer. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 441. [Google Scholar] [CrossRef] [Green Version]
- Pytynia, K.B.; Dahlstrom, K.R.; Sturgis, E.M. Epidemiology of HPV-Associated Oropharyngeal Cancer. Oral Oncol. 2014, 50, 380–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.; Albers, A.E.; Qin, J.; Kaufmann, A.M. Prognostic significance of overexpressed P16INK4a in patients with cervical cancer: A meta-analysis. PLoS ONE 2014, 9, e106384. [Google Scholar] [CrossRef]
- Schlecht, N.F.; Ben-Dayan, M.; Anayannis, N.; Lleras, R.A.; Thomas, C.; Wang, Y.; Smith, R.V.; Burk, R.D.; Harris, T.M.; Childs, G.; et al. Epigenetic changes in the CDKN2A locus are associated with differential expression of P16INK4A and P14ARF in HPV-positive oropharyngeal squamous cell carcinoma. Cancer Med. 2015, 4, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Ekanayake Weeramange, C.; Tang, K.D.; Vasani, S.; Langton-Lockton, J.; Kenny, L.; Punyadeera, C. DNA methylation changes in human papillomavirus-driven head and neck cancers. Cells 2020, 9, 1359. [Google Scholar] [CrossRef] [PubMed]
- Mascitti, M.; Tempesta, A.; Togni, L.; Capodiferro, S.; Troiano, G.; Rubini, C.; Maiorano, E.; Santarelli, A.; Favia, G.; Limongelli, L. Histological features and survival in young patients with HPV-negative oral squamous cell carcinoma. Oral Dis. 2020, 26, 1640–1648. [Google Scholar] [CrossRef] [PubMed]
- Pierce Campbell, C.M.; Viscidi, R.P.; Torres, B.N.; Lin, H.-Y.; Fulp, W.; Abrahamsen, M.; Lazcano-Ponce, E.; Villa, L.L.; Kreimer, A.R.; Giuliano, A.R. Human papillomavirus (HPV) L1 serum antibodies and the risk of subsequent oral HPV acquisition in men: The HIM study. J. Infect. Dis. 2016, 214, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Routman, D.M.; Jethwa, K.R.; Garda, A.E.; DeWees, T.A.; Joern, L.; Hilfrich, R.; Liu, M.C.; Price, K.A.; Moore, E.J.; Laack, N.N.; et al. HPV16 L1 capsid antibody titers and prognosis in HPV associated malignancy: Oropharyngeal, anal, cervical and vaginal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, E666. [Google Scholar] [CrossRef]
- Kreimer, A.R.; Ferreiro-Iglesias, A.; Nygard, M.; Bender, N.; Schroeder, L.; Hildesheim, A.; Robbins, H.A.; Pawlita, M.; Langseth, H.; Schlecht, N.F.; et al. Timing of HPV16-E6 antibody seroconversion before OPSCC: Findings from the HPVC3 consortium. Ann. Oncol. 2019, 30, 1335–1343. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, R.; Pietrobon, S.; Mazzoni, E.; Bortolotti, D.; Martini, F.; Castellazzi, M.; Casetta, I.; Fainardi, E.; Di Luca, D.; Granieri, E.; et al. Serum IgG against simian virus 40 antigens are hampered by high levels of SHLA-G in patients affected by inflammatory neurological diseases, as multiple sclerosis. J. Transl. Med. 2016, 14, 216. [Google Scholar] [CrossRef] [Green Version]
- Fakhry, C.; Qualliotine, J.R.; Zhang, Z.; Agrawal, N.; Gaykalova, D.A.; Bishop, J.A.; Subramaniam, R.M.; Koch, W.M.; Chung, C.H.; Eisele, D.W.; et al. Serum antibodies to HPV16 early proteins warrant investigation as potential biomarkers for risk stratification and recurrence of HPV-associated oropharyngeal cancer. Cancer Prev. Res. 2016, 9, 135–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schroeder, L.; Wichmann, G.; Willner, M.; Michel, A.; Wiesenfarth, M.; Flechtenmacher, C.; Gradistanac, T.; Pawlita, M.; Dietz, A.; Waterboer, T.; et al. Antibodies against human papillomaviruses as diagnostic and prognostic biomarker in patients with neck squamous cell carcinoma from unknown primary tumor: HPV antibodies as biomarker in NSCCUP patients. Int. J. Cancer 2018, 142, 1361–1368. [Google Scholar] [CrossRef] [Green Version]
- Vergara, N.; Balanda, M.; Vidal, D.; Roldán, F.; Martín, H.S.; Ramírez, E. Detection and quantitation of human papillomavirus DNA in peripheral blood mononuclear cells from blood donors. J. Med. Virol. 2019, 91, 2009–2015. [Google Scholar] [CrossRef]
- Stanley, M. Antibody reactivity to HPV E6 and E7 oncoproteins and early diagnosis of invasive cervical cancer. Am. J. Obstet. Gynecol. 2003, 188, 3–4. [Google Scholar] [CrossRef]
- Rajagopal, C.; Harikumar, K.B. The origin and functions of exosomes in cancer. Front. Oncol. 2018, 8, 66. [Google Scholar] [CrossRef] [Green Version]
- Dwedar, R.A.; Omar, N.M.; Eissa, S.A.-L.; Badawy, A.Y.A.; El-Kareem, D.A.; Ahmed Madkour, L.A.E.-F. Diagnostic and prognostic impact of E6/E7 MRNA compared to HPV DNA and P16 expression in head and neck cancers: An egyptian study. Alex. J. Med. 2020, 56, 155–165. [Google Scholar] [CrossRef]
- Dahlstrom, K.R.; Li, G.; Hussey, C.S.; Vo, J.T.; Wei, Q.; Zhao, C.; Sturgis, E.M. Circulating human papillomavirus DNA as a marker for disease extent and recurrence among patients with oropharyngeal cancer. Cancer 2015, 121, 3455–3464. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathological Variables | HPV-Negative | HPV-Positive | p-Value | Tumor Site (HPV-Positive) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Oral | p-Value * | Oropharynx | p-Value | Hypopharynx | p-Value * | Larynx | p-Value * | ||||
| Tumor Site | |||||||||||
| Oral | 25/47 (53.20%) | 2/20 (10%) | |||||||||
| Oropharynx | 13/47 (27.66%) | 15/20 (75%) | |||||||||
| Hypopharynx | 1/47 (2.13%) | 2/20 (10%) | |||||||||
| Larynx | 6/47 (12.77%) | 1/20 (5%) | |||||||||
| Hidden 1 | 2/47 (4.25%) | - | |||||||||
| Tumor Size | |||||||||||
| T1 | 7/47 (14.89%) | 3/20 (15%) | 0.225 | - | NA | 2/15 (13.33%) | 0.031 | 1/2 (50%) | NA | - | NA |
| T2 | 14/47 (29.79%) | 5/20 (25%) | - | 4/15 (26.67%) | 1/2 (50%) | - | |||||
| T3 | 9/47 (19.15%) | 3/20 (15%) | - | 3/15 (20.00%) | - | - | |||||
| T4 | 17/47 (36.17%) | 9/20 (45%) | 2/2 (100%) | 6/15 (40.00%) | - | 1/1 (100%) | |||||
| Node Status | |||||||||||
| N0 | 9/47 (19.15%) | 3/20 (15%) | 0.108 | - | NA | 2/15 (13.33%) | 0.096 | - | NA | 1/1 (100%) | NA |
| N+ | 38/47 (80.85%) | 17/20 (85%) | 2/2 (100%) | 13/15 (86.67%) | 2/2 (100%) | - | |||||
| Clinical Stage | |||||||||||
| I | 1/47 (2.13%) | 1/20 (5%) | 0.467 | - | 1/15 (6.67%) | 0.336 | - | NA | - | NA | |
| II | 7/47 (14.89%) | 5/20 (25%) | - | 5/15 (33.33%) | - | - | |||||
| III | 7/47 (14.89%) | 5/20 (25%) | - | 4/15 (26.67%) | 1/2 (50%) | - | |||||
| IVa | 25/47 (53.19%) | 9/20 (45%) | 2/2 (100%) | 5/15 (33.33%) | 1/2 (50%) | 1/1 (100%) | |||||
| Ivb/c | 7/47 (14.89%) | - | - | - | - | - | |||||
| Recurrence | 16/47 (42.55%) | 6/20 (30%) | 0.0001 | 1/2 (50%) | NA | 4/15 (26.66%) | 0.001 | 1/2 (50%) | NA | 0/1 (0%) | NA |
| Persistance | 4/47 (8.51%) | 2/20 (10%) | 2/15 (13.33%) | ||||||||
| N/A | 2/47 (4.25%) | 2/20 (10%) | - | 2/15 (13.33%) | - | - | |||||
| Tobacco consumption | |||||||||||
| No | 5/47 (10.64%) | 2/20 (10%) | 0.481 | - | NA | 2/15 (13.33%) | 0.582 | - | NA | - | NA |
| Ex Smoker | 13/47 (27.66%) | 7/20 (35%) | - | 4/15 (26.67%) | 2/2 (100%) | 1/1 (100%) | |||||
| Smoker | 25/47 (53.19%) | 7/20 (35%) | 2/2 (100%) | 5/15 (33.33%) | - | - | |||||
| N/A | 4/47 (8.51%) | 4/20 (20%) | - | 4/15 (26.67%) | - | - | |||||
| Alcohol consumption | |||||||||||
| No | 10/47 (21.28%) | 5/20 (25%) | 0.962 | - | NA | 4/15 (26.67%) | 0.725 | - | NA | 1/1 (100%) | NA |
| Ex consumer | 3/47 (6.38%) | 2/20 (10%) | 1/2 (50%) | 0/15 (0%) | 1/2 (50%) | - | |||||
| Consumer | 27/47 (57.45%) | 9/20 (45%) | 1/2 (50%) | 7/15 (46.67%) | 1/2 (50%) | - | |||||
| N/A | 7/47 (14.89%) | 4/20 (20%) | - | 4/15 (26.67%) | - | - | |||||
| Age | 64.04 ± 11.55 | 67,05 ± 9,05 | 0.709 | 63 ± 1.41 | NA | 65.73 ± 9.15 | 0.409 | 73 ± 1.41 | NA | 83 ± NA | NA |
| Gender | |||||||||||
| Male | 32/47 (68.09%) | 17/20 (85%) | 0.244 | 2/2 (100%) | NA | 12/15 (80%) | 0.289 | 2/2 (100%) | NA | 1/1 (100%) | NA |
| Female | 15/47 (31.91%) | 3/20 (15%) | - | 3/15 (20%) | - | - | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oton-Gonzalez, L.; Rotondo, J.C.; Lanzillotti, C.; Mazzoni, E.; Bononi, I.; Iaquinta, M.R.; Cerritelli, L.; Malagutti, N.; Ciorba, A.; Bianchini, C.; et al. Serum HPV16 E7 Oncoprotein Is a Recurrence Marker of Oropharyngeal Squamous Cell Carcinomas. Cancers 2021, 13, 3370. https://doi.org/10.3390/cancers13133370
Oton-Gonzalez L, Rotondo JC, Lanzillotti C, Mazzoni E, Bononi I, Iaquinta MR, Cerritelli L, Malagutti N, Ciorba A, Bianchini C, et al. Serum HPV16 E7 Oncoprotein Is a Recurrence Marker of Oropharyngeal Squamous Cell Carcinomas. Cancers. 2021; 13(13):3370. https://doi.org/10.3390/cancers13133370
Chicago/Turabian StyleOton-Gonzalez, Lucia, John Charles Rotondo, Carmen Lanzillotti, Elisa Mazzoni, Ilaria Bononi, Maria Rosa Iaquinta, Luca Cerritelli, Nicola Malagutti, Andrea Ciorba, Chiara Bianchini, and et al. 2021. "Serum HPV16 E7 Oncoprotein Is a Recurrence Marker of Oropharyngeal Squamous Cell Carcinomas" Cancers 13, no. 13: 3370. https://doi.org/10.3390/cancers13133370