
The Incidence and Treatment Response of Double Expression of MYC and BCL2 in Patients with Diffuse Large B-Cell Lymphoma: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction and Quality Assessment
- Study: authors, publication year, patient enrollment period, institution, country, design.
- Pathological data: cut-off values of MYC and BCL2 protein expression by IHC, proportion of positive tumor cells for each marker and double expressor status, IHC protocol details.
- Patient: number of patients, age, gender, clinical setting, international prognostic index, Ann Arbor Stage, prevalence of elevated LDH, treatment arm, complete remission (CR) rate.
- DHIT-sig: proportion of DHITsig-positive cases, proportion of DH/TH lymphoma, the numbers of true positives, true negatives, false positives, and false negatives of DHIT-sig for predicting DH/TH lymphoma.
2.3. Data Synthesis and Analysis
3. Results
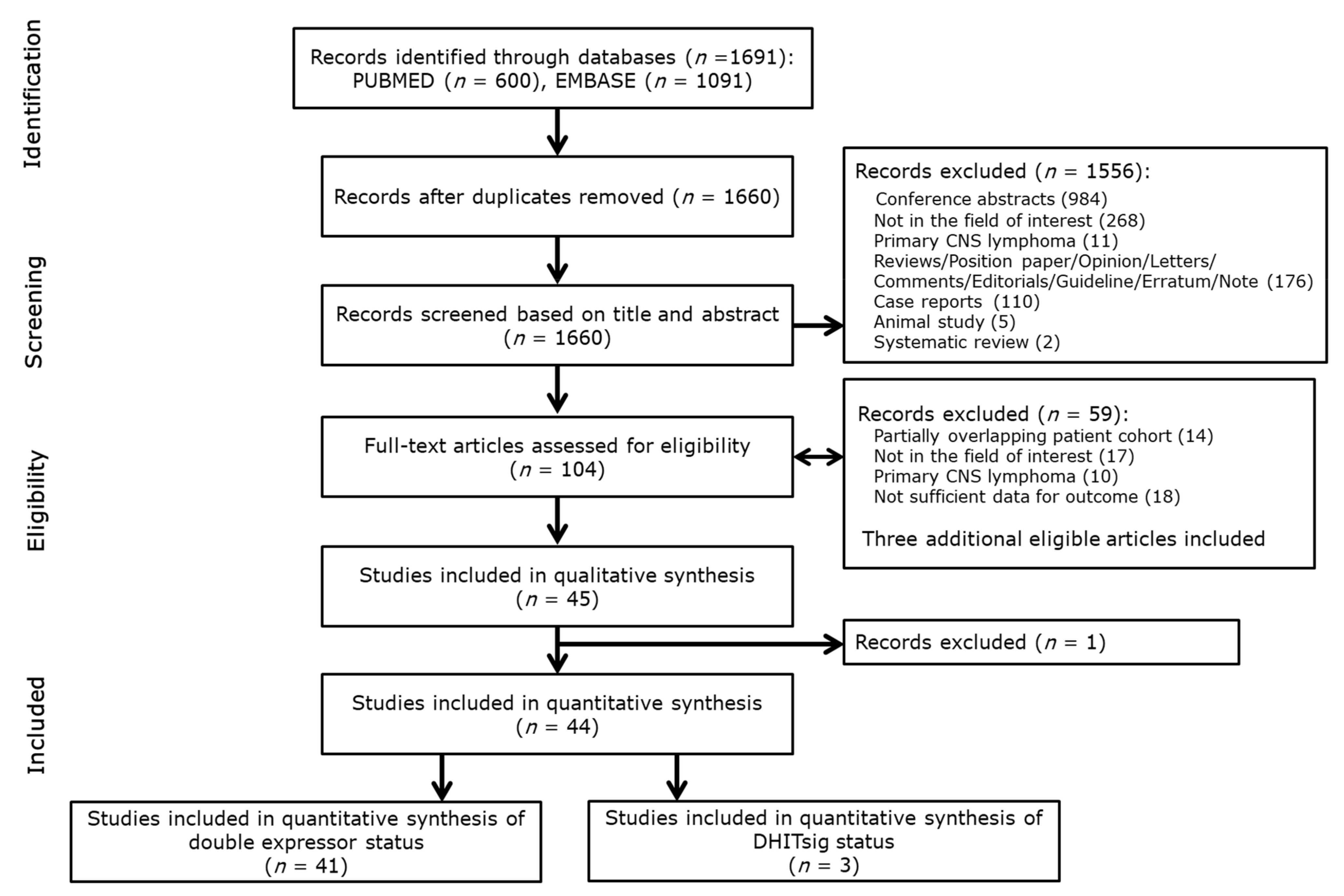
3.1. Literature Search and Quality Assessment
3.2. Characteristics of the Included Studies
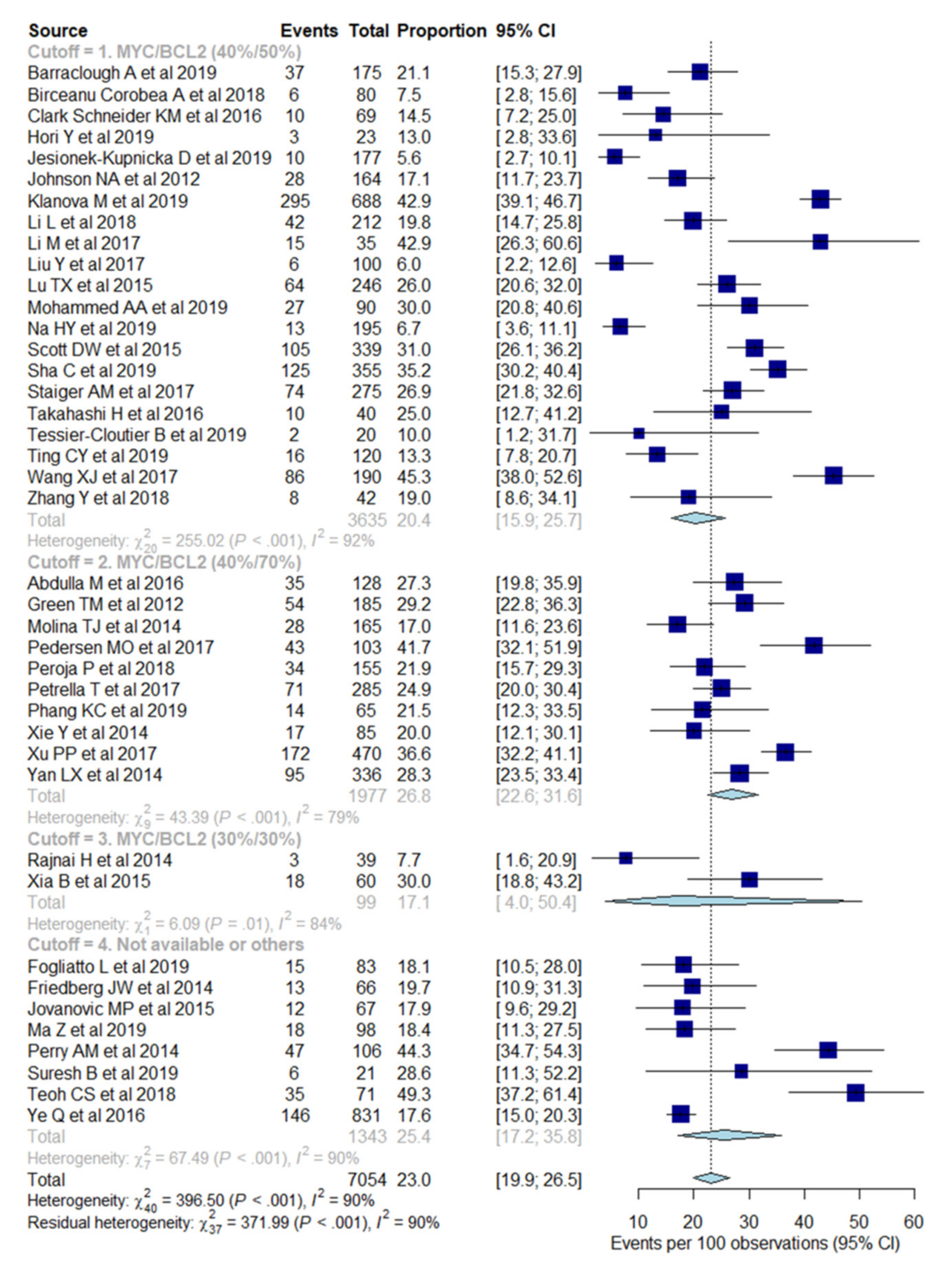
3.3. Meta-Analytic Pooled Prevalence of Double Expressor Status and MYC and BCL2 Protein Expression
3.4. Heterogeneity Exploration
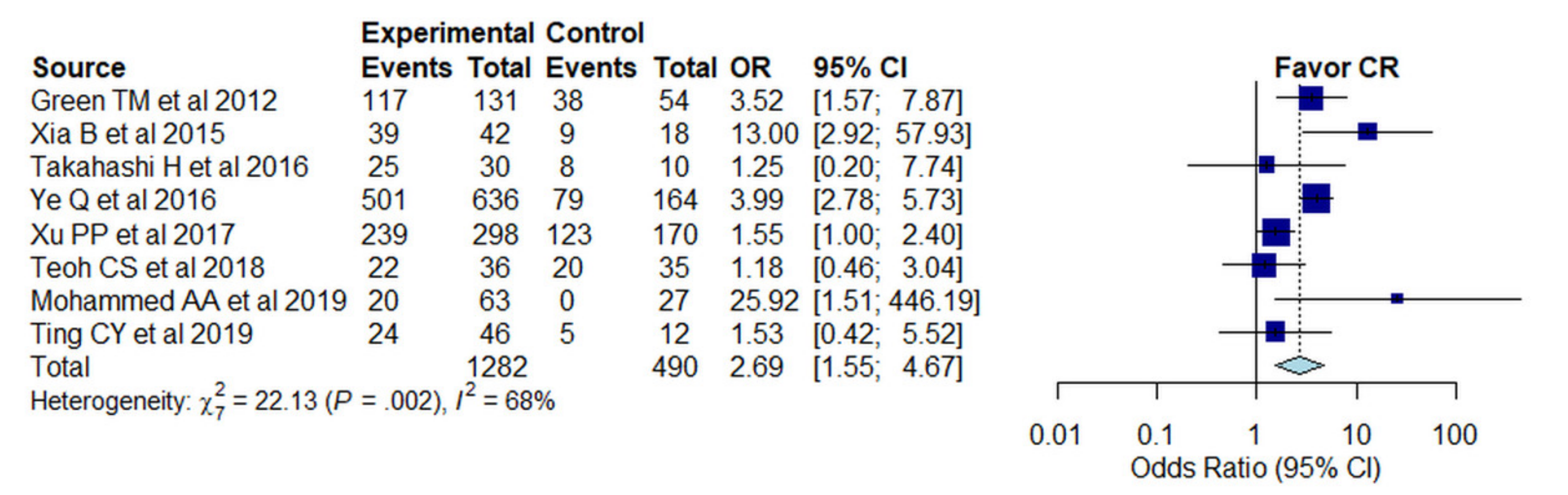
3.5. Odds Ratio for Complete Remission Rate in Those with and without MYC/BCL2 Protein Co-Expression
3.6. Evaluation of the Double-Hit Gene Expression Signature in De Novo DLBCL
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Teras, L.R.; DeSantis, C.E.; Cerhan, J.R.; Morton, L.M.; Jemal, A.; Flowers, C.R. 2016 US lymphoid malignancy statistics by World Health Organization subtypes. CA Cancer J. Clin. 2016, 66, 443–459. [Google Scholar] [CrossRef]
- Liu, Y.; Barta, S.K. Diffuse large B-cell lymphoma: 2019 update on diagnosis, risk stratification, and treatment. Am. J. Hematol. 2019, 94, 604–616. [Google Scholar] [CrossRef]
- Green, T.M.; Young, K.H.; Visco, C.; Xu-Monette, Z.Y.; Orazi, A.; Go, R.S.; Nielsen, O.; Gadeberg, O.V.; Mourits-Andersen, T.; Frederiksen, M.; et al. Immunohistochemical double-hit score is a strong predictor of outcome in patients with diffuse large B-cell lymphoma treated with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 3460–3467. [Google Scholar] [CrossRef]
- Ziepert, M.; Hasenclever, D.; Kuhnt, E.; Glass, B.; Schmitz, N.; Pfreundschuh, M.; Loeffler, M. Standard International prognostic index remains a valid predictor of outcome for patients with aggressive CD20+ B-cell lymphoma in the rituximab era. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 2373–2380. [Google Scholar] [CrossRef]
- Lenz, G.; Staudt, L.M. Aggressive lymphomas. N. Engl. J. Med. 2010, 362, 1417–1429. [Google Scholar] [CrossRef] [PubMed]
- Tomita, N.; Tokunaka, M.; Nakamura, N.; Takeuchi, K.; Koike, J.; Motomura, S.; Miyamoto, K.; Kikuchi, A.; Hyo, R.; Yakushijin, Y.; et al. Clinicopathological features of lymphoma/leukemia patients carrying both BCL2 and MYC translocations. Haematologica 2009, 94, 935–943. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, S.H.; Campo, E.; Pileri, S.A.; Harris, N.L.; Stein, H.; Siebert, R.; Advani, R.; Ghielmini, M.; Salles, G.A.; Zelenetz, A.D.; et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016, 127, 2375–2390. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Seegmiller, A.C.; Lin, P.; Wang, X.J.; Miranda, R.N.; Bhagavathi, S.; Medeiros, L.J. B-cell lymphomas with concurrent MYC and BCL2 abnormalities other than translocations behave similarly to MYC/BCL2 double-hit lymphomas. Mod. Pathol. Off. J. U. S. Can. Acad. Pathol. Inc. 2015, 28, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Collinge, B.; Ben-Neriah, S.; Chong, L.; Boyle, M.; Jiang, A.; Miyata-Takata, T.; Farinha, P.; Craig, J.W.; Slack, G.W.; Ennishi, D.; et al. The impact of MYC and BCL2 structural variants in tumors of DLBCL morphology and mechanisms of false-negative MYC IHC. Blood 2021, 137, 2196–2208. [Google Scholar] [CrossRef] [PubMed]
- Horn, H.; Ziepert, M.; Becher, C.; Barth, T.F.E.; Bernd, H.-W.; Feller, A.C.; Klapper, W.; Hummel, M.; Stein, H.; Hansmann, M.-L.; et al. MYC status in concert with BCL2 and BCL6 expression predicts outcome in diffuse large B-cell lymphoma. Blood 2013, 121, 2253–2263. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Tu, R.; Liu, H.; Qing, G. Regulation of cancer cell metabolism: Oncogenic MYC in the driver’s seat. Signal Transduct. Target. Ther. 2020, 5, 124. [Google Scholar] [CrossRef]
- Bahr, C.; von Paleske, L.; Uslu, V.V.; Remeseiro, S.; Takayama, N.; Ng, S.W.; Murison, A.; Langenfeld, K.; Petretich, M.; Scognamiglio, R.; et al. A Myc enhancer cluster regulates normal and leukaemic haematopoietic stem cell hierarchies. Nature 2018, 553, 515–520. [Google Scholar] [CrossRef]
- Cho, S.W.; Xu, J.; Sun, R.; Mumbach, M.R.; Carter, A.C.; Chen, Y.G.; Yost, K.E.; Kim, J.; He, J.; Nevins, S.A.; et al. Promoter of lncRNA Gene PVT1 Is a Tumor-Suppressor DNA Boundary Element. Cell 2018, 173, 1398–1412.e1322. [Google Scholar] [CrossRef]
- Sesques, P.; Johnson, N.A. Approach to the diagnosis and treatment of high-grade B-cell lymphomas with MYC and BCL2 and/or BCL6 rearrangements. Blood 2017, 129, 280–288. [Google Scholar] [CrossRef]
- Bahram, F.; von der Lehr, N.; Cetinkaya, C.; Larsson, L.G. c-Myc hot spot mutations in lymphomas result in inefficient ubiquitination and decreased proteasome-mediated turnover. Blood 2000, 95, 2104–2110. [Google Scholar] [CrossRef]
- Jiang, J.; Wang, J.; Yue, M.; Cai, X.; Wang, T.; Wu, C.; Su, H.; Wang, Y.; Han, M.; Zhang, Y.; et al. Direct Phosphorylation and Stabilization of MYC by Aurora B Kinase Promote T-cell Leukemogenesis. Cancer Cell 2020, 37, 200–215.e205. [Google Scholar] [CrossRef] [PubMed]
- Herrera, A.F.; Mei, M.; Low, L.; Kim, H.T.; Griffin, G.K.; Song, J.Y.; Merryman, R.W.; Bedell, V.; Pak, C.; Sun, H.; et al. Relapsed or Refractory Double-Expressor and Double-Hit Lymphomas Have Inferior Progression-Free Survival After Autologous Stem-Cell Transplantation. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 24–31. [Google Scholar] [CrossRef]
- Miura, K.; Takahashi, H.; Nakagawa, M.; Izu, A.; Sugitani, M.; Kurita, D.; Sakagami, M.; Ohtake, S.; Uchino, Y.; Hojo, A.; et al. Clinical significance of co-expression of MYC and BCL2 protein in aggressive B-cell lymphomas treated with a second line immunochemotherapy. Leuk. Lymphoma 2016, 57, 1335–1341. [Google Scholar] [CrossRef] [PubMed]
- Abdulla, M.; Laszlo, S.; Triumf, J.; Hedstrom, G.; Berglund, M.; Enblad, G.; Amini, R.M. A population-based study of cellular markers in R-CHOP treated diffuse large B-cell lymphoma patients. Acta Oncol. 2016, 55, 1126–1131. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.A.; Slack, G.W.; Savage, K.J.; Connors, J.M.; Ben-Neriah, S.; Rogic, S.; Scott, D.W.; Tan, K.L.; Steidl, C.; Sehn, L.H.; et al. Concurrent expression of MYC and BCL2 in diffuse large B-cell lymphoma treated with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 3452–3459. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Xu-Monette, Z.Y.; Tzankov, A.; Deng, L.; Wang, X.; Manyam, G.C.; Visco, C.; Montes-Moreno, S.; Zhang, L.; Dybkaer, K.; et al. Prognostic impact of concurrent MYC and BCL6 rearrangements and expression in de novo diffuse large B-cell lymphoma. Oncotarget 2016, 7, 2401–2416. [Google Scholar] [CrossRef]
- Peña, C.; Villegas, P.; Cabrera, M.E. Double or triple-expressor lymphomas: Prognostic impact of immunohistochemistry in patients with diffuse large B-cell lymphoma. Hematol. Transfus. Cell Ther. 2020, 42, 192–193. [Google Scholar] [CrossRef]
- Wawire, J.; Sayed, S.; Moloo, Z.; Sohani, A.R. Diffuse Large B-Cell Lymphoma in Kenya: MYC, BCL2, and the Cell of Origin. J. Glob. Oncol. 2019, 5, 1–8. [Google Scholar] [CrossRef]
- Han, B.; Kim, S.; Koh, J.; Yim, J.; Lee, C.; Heo, D.S.; Kim, T.M.; Paik, J.H.; Jeon, Y.K. Immunophenotypic Landscape and Prognosis of Diffuse Large B-Cell Lymphoma with MYC/BCL2 Double Expression: An Analysis of A Prospectively Immunoprofiled Cohort. Cancers 2020, 12, 3305. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269.w264. [Google Scholar] [CrossRef]
- Donzelli, G.; Llopis-Gonzalez, A.; Llopis-Morales, A.; Cioni, L.; Morales-Suárez-Varela, M. Particulate Matter Exposure and Attention-Deficit/Hyperactivity Disorder in Children: A Systematic Review of Epidemiological Studies. Int. J. Environ. Res. Public Health 2019, 17, 67. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality if Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 6 June 2020).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Suh, C.H.; Park, S.H. Successful Publication of Systematic Review and Meta-Analysis of Studies Evaluating Diagnostic Test Accuracy. Korean J. Radiol. 2016, 17, 5–6. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Wang, J.; Zhou, M.; Xu, J.-Y.; Chen, B.; Ouyang, J. Combination of BCL-2 and MYC protein expression improves high-risk stratification in diffuse large B-cell lymphoma. Onco Targets Ther. 2015, 8, 2645–2650. [Google Scholar] [CrossRef]
- Barraclough, A.; Alzahrani, M.; Ettrup, M.S.; Bishton, M.; van Vliet, C.; Farinha, P.; Gould, C.; Birch, S.; Sehn, L.H.; Sovani, V.; et al. COO and MYC/BCL2 status do not predict outcome among patients with stage I/II DLBCL: A retrospective multicenter study. Blood Adv. 2019, 3, 2013–2021. [Google Scholar] [CrossRef]
- Corobea, A.B.; Evsei, A.; Rosianu, C.; Gheorghe, M.; Birceanu, G.; Copca, N.; Sajin, M.; Lupu, A. The survival impact of combined expression of MYC, BCL2 and BCL6 in diffuse large B cell lymphoma patients. Arch. Balk. Med. Union 2018, 53, 232–238. [Google Scholar] [CrossRef]
- Clark Schneider, K.M.; Banks, P.M.; Collie, A.M.; Lanigan, C.P.; Manilich, E.; Durkin, L.M.; Hill, B.T.; Hsi, E.D. Dual expression of MYC and BCL2 proteins predicts worse outcomes in diffuse large B-cell lymphoma. Leuk. Lymphoma 2016, 57, 1640–1648. [Google Scholar] [CrossRef]
- Fogliatto, L.; Grokoski, K.C.; Strey, Y.M.; Vanelli, T.; Fraga, C.; Barra, M.B.; Pinto, F.C.; Bendit, I.; Bica, C.G. Prognostic impact of MYD88 mutation, proliferative index and cell origin in diffuse large B cell lymphoma. Hematol. Transfus. Cell Ther. 2019, 41, 50–56. [Google Scholar] [CrossRef]
- Friedberg, J.W.; Unger, J.M.; Burack, W.R.; Gopal, A.K.; Raju, R.N.; Nademanee, A.P.; Kaminski, M.S.; Li, H.; Press, O.W.; Miller, T.P.; et al. R-CHOP with iodine-131 tositumomab consolidation for advanced stage diffuse large B-cell lymphoma (DLBCL): SWOG S0433. Br. J. Haematol. 2014, 166, 382–389. [Google Scholar] [CrossRef]
- Hori, Y.; Yamamoto, H.; Nozaki, Y.; Torisu, T.; Fujiwara, M.; Taguchi, K.; Nishiyama, K.; Nakamura, S.; Kitazono, T.; Oda, Y. Colorectal diffuse large B-cell lymphoma: Molecular subclassification and prognostic significance of immunoglobulin gene translocation. Hum. Pathol. 2020, 96, 67–78. [Google Scholar] [CrossRef]
- Jesionek-Kupnicka, D.; Braun, M.; Robak, T.; Kuncman, W.; Kordek, R. A large single-institution retrospective analysis of aggressive B-cell lymphomas according to the 2016/2017 WHO classification. Adv. Clin. Exp. Med. Off. Organ Wroc. Med. Univ. 2019, 28, 1359–1365. [Google Scholar] [CrossRef]
- Jovanovic, M.P.; Mihaljevic, B.; Jakovic, L.; Martinovic, V.C.; Fekete, M.D.; Andjelic, B.; Antic, D.; Bogdanovic, A.; Boricic, N.; Terzic, T.; et al. BCL2 positive and BCL6 negative diffuse large B cell lymphoma patients benefit from R-CHOP therapy irrespective of germinal and non germinal center B cell like subtypes. J. BUON Off. J. Balk. Union Oncol. 2015, 20, 820–828. [Google Scholar]
- Klanova, M.; Sehn, L.H.; Bence-Bruckler, I.; Cavallo, F.; Jin, J.; Martelli, M.; Stewart, D.; Vitolo, U.; Zaja, F.; Zhang, Q.; et al. Integration of cell of origin into the clinical CNS International Prognostic Index improves CNS relapse prediction in DLBCL. Blood 2019, 133, 919–926. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zhang, X.; Zhang, T.; Song, Z.; Hu, G.; Li, W.; Li, L.; Qiu, L.; Qian, Z.; Zhou, S.; et al. Prognostic Significance of BCL-2 and BCL-6 Expression in MYC-positive DLBCL. Clin. Lymphoma Myeloma Leuk. 2018, 18, e381–e389. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Liu, Y.; Wang, Y.; Chen, G.; Chen, Q.; Xiao, H.; Liu, F.; Qi, C.; Yu, Z.; Li, X.; et al. Anaplastic Variant of Diffuse Large B-cell Lymphoma Displays Intricate Genetic Alterations and Distinct Biological Features. Am. J. Surg. Pathol. 2017, 41, 1322–1332. [Google Scholar] [CrossRef]
- Liu, Y.; Yu, K.; Li, M.; Zeng, K.; Wei, J.; Li, X.; Liu, Y.; Zhao, D.; Fan, L.; Yu, Z.; et al. EZH2 overexpression in primary gastrointestinal diffuse large B-cell lymphoma and its association with the clinicopathological features. Hum. Pathol. 2017, 64, 213–221. [Google Scholar] [CrossRef]
- Lu, T.X.; Fan, L.; Wang, L.; Wu, J.Z.; Miao, K.R.; Liang, J.H.; Gong, Q.X.; Wang, Z.; Young, K.H.; Xu, W.; et al. MYC or BCL2 copy number aberration is a strong predictor of outcome in patients with diffuse large B-cell lymphoma. Oncotarget 2015, 6, 18374–18388. [Google Scholar] [CrossRef]
- Ma, Z.; Niu, J.; Cao, Y.; Pang, X.; Cui, W.; Zhang, W.; Li, X. Clinical significance of ‘double-hit’ and ‘double-expression’ lymphomas. J. Clin. Pathol. 2020, 73, 126–138. [Google Scholar] [CrossRef]
- Mohammed, A.A.; Rashed, H.E.; Abdelrahman, A.E.; Obaya, A.A.; Toam, M.; Abdel Nour, H.M.; Abdelhamid, M.I.; Elsayed, F.M. C-MYC and BCL2: Correlation between Protein Over-Expression and Gene Translocation and Impact on Outcome in Diffuse Large B Cell Lymphoma. Asian Pac. J. Cancer Prev. APJCP 2019, 20, 1463–1470. [Google Scholar] [CrossRef]
- Molina, T.J.; Canioni, D.; Copie-Bergman, C.; Recher, C.; Briere, J.; Haioun, C.; Berger, F.; Ferme, C.; Copin, M.C.; Casasnovas, O.; et al. Young patients with non-germinal center B-cell-like diffuse large B-cell lymphoma benefit from intensified chemotherapy with ACVBP plus rituximab compared with CHOP plus rituximab: Analysis of data from the Groupe d’Etudes des Lymphomes de l’Adulte/lymphoma study association phase III trial LNH 03-2B. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, 3996–4003. [Google Scholar] [CrossRef]
- Na, H.Y.; Choe, J.Y.; Shin, S.A.; Kim, H.J.; Han, J.H.; Kim, H.K.; Oh, S.H.; Kim, J.E. Characteristics of CD5-positive diffuse large B-cell lymphoma among Koreans: High incidence of BCL2 and MYC double-expressors. PLoS ONE 2019, 14, e0224247. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, M.O.; Gang, A.O.; Brown, P.; Pedersen, M.; Knudsen, H.; Nielsen, S.L.; Poulsen, T.; Wirenfeldt Klausen, T.; Hogdall, E.; Norgaard, P. Real world data on young patients with high-risk diffuse large B-cell lymphoma treated with R-CHOP or R-CHOEP—MYC, BCL2 and BCL6 as prognostic biomarkers. PLoS ONE 2017, 12, e0186983. [Google Scholar] [CrossRef]
- Peroja, P.; Pedersen, M.; Mantere, T.; Norgaard, P.; Peltonen, J.; Haapasaari, K.M.; Bohm, J.; Jantunen, E.; Turpeenniemi-Hujanen, T.; Rapakko, K.; et al. Mutation of TP53, translocation analysis and immunohistochemical expression of MYC, BCL-2 and BCL-6 in patients with DLBCL treated with R-CHOP. Sci. Rep. 2018, 8, 14814. [Google Scholar] [CrossRef]
- Perry, A.M.; Alvarado-Bernal, Y.; Laurini, J.A.; Smith, L.M.; Slack, G.W.; Tan, K.L.; Sehn, L.H.; Fu, K.; Aoun, P.; Greiner, T.C.; et al. MYC and BCL2 protein expression predicts survival in patients with diffuse large B-cell lymphoma treated with rituximab. Br. J. Haematol. 2014, 165, 382–391. [Google Scholar] [CrossRef] [PubMed]
- Petrella, T.; Copie-Bergman, C.; Briere, J.; Delarue, R.; Jardin, F.; Ruminy, P.; Thieblemont, C.; Figeac, M.; Canioni, D.; Feugier, P.; et al. BCL2 expression but not MYC and BCL2 coexpression predicts survival in elderly patients with diffuse large B-cell lymphoma independently of cell of origin in the phase 3 LNH03-6B trial. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2017, 28, 1042–1049. [Google Scholar] [CrossRef]
- Phang, K.C.; Hussin, N.H.; Abdul Rahman, F.; Tizen, N.M.S.; Mansoor, A.; Masir, N. Characterisation of immunogenotypes of diffuse large B-cell lymphoma. Malays. J. Pathol. 2019, 41, 101–124. [Google Scholar]
- Rajnai, H.; Heyning, F.H.; Koens, L.; Sebestyen, A.; Andrikovics, H.; Hogendoorn, P.C.; Matolcsy, A.; Szepesi, A. The density of CD8+ T-cell infiltration and expression of BCL2 predicts outcome of primary diffuse large B-cell lymphoma of bone. Virchows Arch. Int. J. Pathol. 2014, 464, 229–239. [Google Scholar] [CrossRef]
- Scott, D.W.; Mottok, A.; Ennishi, D.; Wright, G.W.; Farinha, P.; Ben-Neriah, S.; Kridel, R.; Barry, G.S.; Hother, C.; Abrisqueta, P.; et al. Prognostic Significance of Diffuse Large B-Cell Lymphoma Cell of Origin Determined by Digital Gene Expression in Formalin-Fixed Paraffin-Embedded Tissue Biopsies. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 2848–2856. [Google Scholar] [CrossRef]
- Sha, C.; Barrans, S.; Cucco, F.; Bentley, M.A.; Care, M.A.; Cummin, T.; Kennedy, H.; Thompson, J.S.; Uddin, R.; Worrillow, L.; et al. Molecular High-Grade B-Cell Lymphoma: Defining a Poor-Risk Group That Requires Different Approaches to Therapy. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2019, 37, 202–212. [Google Scholar] [CrossRef]
- Staiger, A.M.; Ziepert, M.; Horn, H.; Scott, D.W.; Barth, T.F.E.; Bernd, H.W.; Feller, A.C.; Klapper, W.; Szczepanowski, M.; Hummel, M.; et al. Clinical Impact of the Cell-of-Origin Classification and the MYC/BCL2 Dual Expresser Status in Diffuse Large B-Cell Lymphoma Treated Within Prospective Clinical Trials of the German High-Grade Non-Hodgkin’s Lymphoma Study Group. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 2515–2526. [Google Scholar] [CrossRef]
- Suresh, B.; Asati, V.; Lakshmaiah, K.C.; Babu, G.; Lokanatha, D.; Jacob, L.A.; Lokesh, K.N.; Rudresh, A.H.; Rajeev, L.K.; Smitha, S.; et al. Primary gastrointestinal diffuse large B-cell lymphoma: A prospective study from South India. South Asian J. Cancer 2019, 8, 57–59. [Google Scholar] [CrossRef]
- Takahashi, H.; Miura, K.; Nakagawa, M.; Sugitani, M.; Amano, Y.; Kurita, D.; Sakagami, M.; Ohtake, S.; Uchino, Y.; Kodaira, H.; et al. Negative impact of concurrent overexpression of MYC and BCL2 in patients with advanced diffuse large B-cell lymphoma treated with dose-intensified immunochemotherapy. Leuk. Lymphoma 2016, 57, 2784–2790. [Google Scholar] [CrossRef]
- Teoh, C.S.; Lee, S.Y.; Chiang, S.K.; Chew, T.K.; Goh, A.S. Impact of Double Expression of C-MYC/BCL2 Protein and Cell of Origin Subtypes on the Outcome among Patients with Diffuse Large B-Cell Lymphoma: A Single Asian Center Experience. Asian Pac. J. Cancer Prev. APJCP 2018, 19, 1229–1236. [Google Scholar] [CrossRef] [PubMed]
- Tessier-Cloutier, B.; Twa, D.D.; Baecklund, E.; Gascoyne, R.; Johnson, N.A.; Backlin, C.; Kamen, D.L.; Clarke, A.E.; Ramsey-Goldman, R.; Lee, J.L.; et al. Cell of origin in diffuse large B-cell lymphoma in systemic lupus erythematosus: Molecular and clinical factors associated with survival. Lupus Sci. Med. 2019, 6, e000324. [Google Scholar] [CrossRef]
- Ting, C.Y.; Chang, K.M.; Kuan, J.W.; Sathar, J.; Chew, L.P.; Wong, O.J.; Yusuf, Y.; Wong, L.; Samsudin, A.T.; Pana, M.; et al. Clinical Significance of BCL2, C-MYC, and BCL6 Genetic Abnormalities, Epstein-Barr Virus Infection, CD5 Protein Expression, Germinal Center B Cell/Non-Germinal Center B-Cell Subtypes, Co-expression of MYC/BCL2 Proteins and Co-expression of MYC/BCL2/BCL6 Proteins in Diffuse Large B-Cell Lymphoma: A Clinical and Pathological Correlation Study of 120 Patients. Int. J. Med. Sci. 2019, 16, 556–566. [Google Scholar] [CrossRef]
- Wang, X.J.; Medeiros, L.J.; Bueso-Ramos, C.E.; Tang, G.; Wang, S.; Oki, Y.; Desai, P.; Khoury, J.D.; Miranda, R.N.; Tang, Z.; et al. P53 expression correlates with poorer survival and augments the negative prognostic effect of MYC rearrangement, expression or concurrent MYC/BCL2 expression in diffuse large B-cell lymphoma. Mod. Pathol. Off. J. U. S. Can. Acad. Pathol. Inc. 2017, 30, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Xia, B.; Zhang, L.; Guo, S.Q.; Li, X.W.; Qu, F.L.; Zhao, H.F.; Zhang, L.Y.; Sun, B.C.; You, J.; Zhang, Y.Z. Coexpression of MYC and BCL-2 predicts prognosis in primary gastrointestinal diffuse large B-cell lymphoma. World J. Gastroenterol. 2015, 21, 2433–2442. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Bulbul, M.A.; Ji, L.; Inouye, C.M.; Groshen, S.G.; Tulpule, A.; O’Malley, D.P.; Wang, E.; Siddiqi, I.N. p53 expression is a strong marker of inferior survival in de novo diffuse large B-cell lymphoma and may have enhanced negative effect with MYC coexpression: A single institutional clinicopathologic study. Am. J. Clin. Pathol. 2014, 141, 593–604. [Google Scholar] [CrossRef]
- Xu, P.P.; Zhong, H.J.; Huang, Y.H.; Gao, X.D.; Zhao, X.; Shen, Y.; Cheng, S.; Huang, J.Y.; Chen, S.J.; Wang, L.; et al. B-cell Function Gene Mutations in Diffuse Large B-cell Lymphoma: A Retrospective Cohort Study. EBioMedicine 2017, 16, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.X.; Liu, Y.H.; Luo, D.L.; Zhang, F.; Cheng, Y.; Luo, X.L.; Xu, J.; Cheng, J.; Zhuang, H.G. MYC expression in concert with BCL2 and BCL6 expression predicts outcome in Chinese patients with diffuse large B-cell lymphoma, not otherwise specified. PLoS ONE 2014, 9, e104068. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, H.; Ren, C.; Yu, H.; Fang, W.; Zhang, N.; Gao, S.; Hou, Q. Correlation Between C-MYC, BCL-2, and BCL-6 Protein Expression and Gene Translocation as Biomarkers in Diagnosis and Prognosis of Diffuse Large B-cell Lymphoma. Front. Pharmacol. 2018, 9, 1497. [Google Scholar] [CrossRef] [PubMed]
- Ennishi, D.; Jiang, A.; Boyle, M.; Collinge, B.; Grande, B.M.; Ben-Neriah, S.; Rushton, C.; Tang, J.; Thomas, N.; Slack, G.W.; et al. Double-Hit Gene Expression Signature Defines a Distinct Subgroup of Germinal Center B-Cell-Like Diffuse Large B-Cell Lymphoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2019, 37, 190–201. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.; Perry, A.; Skrabek, P.; Nasr, M.; Herrera, A.F.; Bedell, V.; Murata-Collins, J.; Pillai, R.; Xu, M.; Chen, L.; et al. Validation of the Double-Hit Gene Expression Signature (DLBCL90) in an Independent Cohort of Patients with Diffuse Large B-Cell Lymphoma of Germinal Center Origin. J. Mol. Diagn. JMD 2021, 23, 658–664. [Google Scholar] [CrossRef]
- Isaksen, K.T.; Beiske, K.; Smeland, E.B.; Jørgensen, J.; Brodtkorb, M.; Myklebust, J.H.; Jerkeman, M.; Meriranta, L.; Karjalainen-Lindsberg, M.-L.; Leppä, S.; et al. The DLBCL90 gene-expression assay identifies double-hit lymphomas with high sensitivity in patients from two phase II clinical trials with high-risk diffuse large B-cell lymphoma. eJHaem 2021, 2, 107–111. [Google Scholar] [CrossRef]
- Riedell, P.A.; Smith, S.M. Double hit and double expressors in lymphoma: Definition and treatment. Cancer 2018, 124, 4622–4632. [Google Scholar] [CrossRef]
- Scott, D.W.; King, R.L.; Staiger, A.M.; Ben-Neriah, S.; Jiang, A.; Horn, H.; Mottok, A.; Farinha, P.; Slack, G.W.; Ennishi, D.; et al. High-grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements with diffuse large B-cell lymphoma morphology. Blood 2018, 131, 2060–2064. [Google Scholar] [CrossRef] [PubMed]
- Schraders, M.; de Jong, D.; Kluin, P.; Groenen, P.; van Krieken, H. Lack of Bcl-2 expression in follicular lymphoma may be caused by mutations in the BCL2 gene or by absence of the t(14;18) translocation. J. Pathol. 2005, 205, 329–335. [Google Scholar] [CrossRef]
- Hilton, L.K.; Tang, J.; Ben-Neriah, S.; Alcaide, M.; Jiang, A.; Grande, B.M.; Rushton, C.K.; Boyle, M.; Meissner, B.; Scott, D.W.; et al. The double-hit signature identifies double-hit diffuse large B-cell lymphoma with genetic events cryptic to FISH. Blood 2019, 134, 1528–1532. [Google Scholar] [CrossRef] [PubMed]
- Shenoy, P.J.; Malik, N.; Nooka, A.; Sinha, R.; Ward, K.C.; Brawley, O.W.; Lipscomb, J.; Flowers, C.R. Racial differences in the presentation and outcomes of diffuse large B-cell lymphoma in the United States. Cancer 2011, 117, 2530–2540. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Han, T.; Iqbal, J.; Irons, R.; Chan, W.C.; Zhu, X.; Fu, K. Diffuse large B-cell lymphoma in Chinese patients: Immunophenotypic and cytogenetic analyses of 124 cases. Am. J. Clin. Pathol. 2010, 133, 305–313. [Google Scholar] [CrossRef]
- Hu, S.; Xu-Monette, Z.Y.; Tzankov, A.; Green, T.; Wu, L.; Balasubramanyam, A.; Liu, W.M.; Visco, C.; Li, Y.; Miranda, R.N.; et al. MYC/BCL2 protein coexpression contributes to the inferior survival of activated B-cell subtype of diffuse large B-cell lymphoma and demonstrates high-risk gene expression signatures: A report from The International DLBCL Rituximab-CHOP Consortium Program. Blood 2013, 121, 4021–4031. [Google Scholar] [CrossRef]
- Li, L.; Li, Y.; Que, X.; Gao, X.; Gao, Q.; Yu, M.; Ma, K.; Xi, Y.; Wang, T. Prognostic significances of overexpression MYC and/or BCL2 in R-CHOP-treated diffuse large B-cell lymphoma: A Systematic review and meta-analysis. Sci. Rep. 2018, 8, 6267. [Google Scholar] [CrossRef]
- Ambrosio, M.R.; Lazzi, S.; Bello, G.L.; Santi, R.; Porro, L.D.; de Santi, M.M.; Guazzo, R.; Mundo, L.; Rigacci, L.; Kovalchuck, S.; et al. MYC protein expression scoring and its impact on the prognosis of aggressive B-cell lymphoma patients. Haematologica 2019, 104, e25–e28. [Google Scholar] [CrossRef] [PubMed]
- Ziepert, M.; Lazzi, S.; Santi, R.; Vergoni, F.; Granai, M.; Mancini, V.; Staiger, A.; Horn, H.; Löffler, M.; Pöschel, V.; et al. A 70% cut-off for MYC protein expression in diffuse large B cell lymphoma identifies a high-risk group of patients. Haematologica 2020, 105, 2667–2670. [Google Scholar] [CrossRef] [PubMed]
- Bosch, M.; Akhter, A.; Chen, B.E.; Mansoor, A.; Lebrun, D.; Good, D.; Crump, M.; Shepherd, L.; Scott, D.W.; Stewart, D.A. A bioclinical prognostic model using MYC and BCL2 predicts outcome in relapsed/refractory diffuse large B-cell lymphoma. Haematologica 2018, 103, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.; Ruano Mendez, A.L.; Rybicki, L.; Sawalha, Y.; Jagadeesh, D.; Dean, R.; Pohlman, B.; Smith, M.R.; Hsi, E.D.; Hill, B.T. Co-expression of MYC and BCL2 predicts poorer outcomes for relapsed/refractory diffuse large B-cell lymphoma with R-ICE and intent to transplant. Ther. Adv. Hematol. 2018, 9, 81–87. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| First Author | Publication Year | Patient Enrollment Period | Institution | Country | Design | IHC Cut-Off Values for Protein Expression | |
|---|---|---|---|---|---|---|---|
| MYC | BCL2 | ||||||
| Abdulla M | 2016 | 2002–2012 | Uppsala University and University Hospital | Sweden | R | 40% | 70% |
| Barraclough A | 2019 | 2002–2013 | Various centers | Australia, United kingdom, Canada, Denmark | R | 40% | 50% |
| Birceanu Corobea A | 2018 | NA | Coltea Clinical Hospital | Romania | NA | 40% | 50% |
| Clark Schneider KM | 2016 | NA | Cleveland Clinic | USA | NA | 40% | 50% |
| Fogliatto L | 2019 | 2011–2016 | Hospital Santa Rita | Brazil | R | 40% | 40% |
| Friedberg JW | 2014 | 2005–2010 | Various centers | USA | Secondary analysis (Clinical trial, Phase 2) | 40% | NA |
| Green TM | 2012 | 2001–2008 | Various centers | Denmark | R | 40% | 70% |
| Hori Y | 2019 | 1999–2018 | Kyushu University Hospital and its affiliated hospitals | Japan | R | 40% | 50% |
| Jesionek-Kupnicka D | 2019 | 2017–2018 | Medical University of Lodz | Poland | R | 40% | 50% |
| Johnson NA | 2012 | NA | Various centers | Various countries | NA | 40% | 50% |
| Jovanovic MP | 2015 | 2001–2005 | Clinical Center of Serbia | Serbia | R | 30% | 50% |
| Klanova M | 2019 | 2011–2014 | Various centers | Various countries | Secondary analysis (Clinical trial, Phase 3) | 40% | 50% |
| Li L | 2018 | 2012–2015 | Tianjin MedicalUniversity Cancer Institute and Hospital | China | R | 40% | 50% |
| Li M | 2017 | 2004–2016 | Various centers | China | NA | 40% | 50% |
| Liu Y | 2017 | 2006–2016 | Xi Jing Hospital and Tang Du Hospital in Xi’an | China | R | 40% | 50% |
| Lu TX | 2015 | 2006–2014 | First Affiliated Hospital of Nanjing Medical University | China | R | 40% | 50% |
| Ma Z | 2019 | 2015–2017 | First Affiliated Hospital of Xinjiang Medical University | China | R | 50% | 70% |
| Mohammed AA | 2019 | 2011–2015 | Zagazig University | Egypt | R | 40% | 50% |
| Molina TJ | 2014 | 2003–2008 | Various centers | France, Belgium, and Switzerland | Secondary analysis (Clinical trial, Phase 3) | 40% | 70% |
| Na HY | 2019 | 1996–2016 | Seoul National University Hospital, Seoul National University Bundang Hospital and Seoul National University Boramae Hospital | Korea | R | 40% | 50% |
| Pedersen MO | 2017 | 2004–2008 | NA | Denmark | R | 40% | 70% |
| Peroja P | 2018 | 2003–2011 | Oulu and Kuopio University Hospitals and Central Hospital of Central Finland | Finland | R | 40% | 70% |
| Perry AM | 2014 | NA | University ofNebraska Medical Center | USA | NA | 50% | 30% |
| Petrella T | 2017 | NA | Various centers | France, Belgium, Switzerland, and Portugal | Secondary analysis (Clinical trial, Phase 3) | 40% | 70% |
| Phang KC | 2019 | 2004–2010 | UKM Medical Centre | Malaysia | R | 40% | 70% |
| Rajnai H | 2014 | NA | Semmelweis University and the Leiden University Medical Center | Hungary, Netherlands | NA | 30% | 30% |
| Scott DW | 2015 | NA | British Columbia Cancer Agency | Canada | NA | 40% | 50% |
| Sha C | 2019 | NA | NA | Swiss and England | Secondary analysis (Clinical trial, Phase 3) | 40% | 50% |
| Staiger AM | 2017 | NA | Various centers | Germany and Switzerland | Secondary analysis (Clinical trial, Phase 3) | 40% | 50% |
| Suresh B | 2019 | 2016–2017 | Kidwai Cancer Institute | India | P | NA | NA |
| Takahashi H | 2016 | 2001–2013 | Nihon University School of Medicine | Japan | R | 40% | 50% |
| Teoh CS | 2018 | 2012–2015 | Hospital Pulau Pinang | Malaysia | R | 40% | 30% |
| Tessier-Cloutier B | 2019 | NA | NA | Sweden, Canada, USA | NA | 40% | 50% |
| Ting CY | 2019 | 2012–2013 | Hospital Ampang, Queen Elizabeth Hospital, Hospital Pulau Pinang and Sarawak General Hospital | Malaysia | R | 40% | 50% |
| Wang XJ | 2017 | 2010–2015 | Vanderbilt and MD Anderson Medical Center | USA | R | 40% | 50% |
| Xia B | 2015 | 2005–2010 | Tianjin Medical University Cancer Institute and Hospital | China | NA | 30% | 30% |
| Xie Y | 2014 | 2002–2012 | Los Angeles County and University of Southern California Medical Center | USA | R | 40% | 70% |
| Xu PP | 2017 | 2002–2012 | Shanghai Rui Jin Hospital | China | R | 40% | 70% |
| Yan LX | 2014 | 2000–2012 | Guangdong General Hospital | China | NA | 40% | 70% |
| Ye Q | 2016 | 1998–2010 | Various centers | Various countries | NA | 70% | 70% |
| Zhang Y | 2018 | 2015–2016 | Weifang People’s Hospital | China | R | 40% | 50% |
| First Author | Patients (N) | Age (Range) | Male to Female Ratio | Clinical Setting |
|---|---|---|---|---|
| Abdulla M | 188 | 64 (26–85) | 1.4:1 | De novo DLBCL |
| Barraclough A | 175 | 62 (19–89) | 1:1 | PET-CT defined stage I/II DLBCL |
| Birceanu Corobea A | 80 | 57.26 (19–87) | 1.1:1 | DLBCL |
| Clark Schneider KM | 69 | 62 ** | 1:1 | De novo DLBCL |
| Fogliatto L | 83 | 64 (15–92) | 1:1.4 | DLBCL |
| Friedberg JW | 84 | 64 (29–85) | 1:1.2 | Newly diagnosed advanced stage DLBCL |
| Green TM | 193 | 64 (16–91) | 1.4:1 | De novo DLBCL |
| Hori Y | 23 | 65 (38–84) | 1.3:1 | Primary colorectal DLBCL |
| Jesionek-Kupnicka D | 217 | 68.73 | 1:1.2 | DLBCL |
| Johnson NA | 167 a | 62 (17–92) | NA | De novo DLBCL |
| Jovanovic MP | 103 | 56 (17–87) | 1:1.1 | De novo DLBCL |
| Klanova M | 688 b | NA | NA | DLBCL in the phase 3 GOYA study |
| Li L | 212 | 58.5 (21–86) | 1.2:1 | Newly diagnosed DLBCL |
| Li M | 35 | 62 (23–89) | 2:1 | Anaplastic DLBCL |
| Liu Y | 100 | NA | 1.1:1 | Primary gastrointestinal DLBCL |
| Lu TX | 246 | NA | NA | De novo DLBCL |
| Ma Z | 98 | 55 (8–76) | 1.3:1 | De novo DLBCL |
| Mohammed AA | 90 | 58 (25–90) | 1.2:1 | De novo DLBCL |
| Molina TJ | 379 | NA | NA | De novo DLBCL |
| Na HY | 195 | NA | 1.3:1 | De novo DLBCL |
| Pedersen MO | 103 | NA (18–60) | 1.3:1 | De novo high-risk DLBCL |
| Peroja P | 155 | NA | 1.2:1 | De novo DLBCL |
| Perry AM | 106 c | 61 (19–89) | 1.2:1 | De novo DLBCL |
| Petrella T | 285 | 70 (59–80) | 2.2:1 | Untreated elderly patients with DLBCL |
| Phang KC | 141 | NA | NA | DLBCL |
| Rajnai H | 41 | 50 (11–78) | 2.4:1 | Primary bone DLBCL |
| Scott DW | 344 | 64 (16–92) | 1.6:1 | De novo DLBCL |
| Sha C | 355 d | NA | NA | Newly diagnosed DLBCL |
| Staiger AM | 414 | NA | 1:1 (RICOVER-60 Trial), 1.4:1 (R-MegaCHOEP Trial) | Untreated DLBCL |
| Suresh B | 21 | 46 (27–69) | 2.5:1 | Primary gastrointestinal DLBCL |
| Takahashi H | 40 | 53 (19–68) | 1:1.3 | De novo DLBCL with high/high-intermediate risk by aaIPI |
| Teoh CS | 104 | NA | 1:1 | DLBCL |
| Tessier-Cloutier B | 20 | 58 (48–66) | 9:1 | SLE diagnosed with DLBCL |
| Ting CY | 120 | 54.1 (14.6) ** | 1.1:1 | De novo DLBCL |
| Wang XJ | 201 | 64 (18–92) | 1.9:1 | De novo DLBCL |
| Xia B | 60 | 57 (23–79) | 1.1:1 | Primary gastrointestinal DLBCL |
| Xie Y | 85 | 54 (20–89) | 1.5:1 | De novo DLBCL |
| Xu PP | 470 e | NA | NA | De novo DLBCL |
| Yan LX | 336 | 57 (7–87) | 1.4:1 | De novo DLBCL |
| Ye Q | 898 | 64 (16–95) | NA | De novo DLBCL |
| Zhang Y | 42 | 58.9 (43–80) | 1.6:1 | Newly diagnosed DLBCL |
| Outcome | No. of Studies | Summary Estimate | p Value for Publication Bias c | Trim-and-Fill Estimate | |||
|---|---|---|---|---|---|---|---|
| Pooled Proportion (%) (95% CI) | p Value for Hetero-Geneity a | I2 (%) b | No. of Missing Studies | Adjusted Pooled Proportion (95% CI) | |||
| Double expressor (MYC+, BCL2+) | 41 | 23 (20–26) | <0.001 | 90 | <0.001 | 16 | 31 (27–36) |
| MYC protein expression | 29 | 34 (30–39) | <0.001 | 90 | 0.421 | ||
| BCL2 protein expression | 30 | 58 (53–62) | <0.001 | 90 | 0.585 | ||
| Double expressor (MYC > 40%, BCL2 > 50%) | 21 | 20 (16–26) | <0.001 | 92 | <0.001 | 9 | 32 (26–39) |
| Double expressor (MYC > 40%, BCL2 > 70%) | 10 | 27 (23–32) | <0.001 | 79 | 0.07 | 3 | 30 (25–35) |
| Double expressor in Asian countries | 16 | 23 (17–28) | <0.001 | 87 | 0.05 | 5 | 30 (23–37) |
| Double expressor in Europe | 12 | 21 (17–27) | <0.001 | 87 | 0.006 | 5 | 29 (23–37) |
| Double expressor in North America | 6 | 29 (20–39) | <0.001 | 88 | NA d | ||
| Double expressor in studies with median age ≥ 60.3 | 16 | 25 (19–31) | <0.001 | 93 | 0.16 | ||
| Double expressor in studies with median age < 60.3 | 14 | 20 (16–24) | <0.001 | 63 | 0.03 | 6 | 25 (21–30) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, J.; Suh, C.H.; Kim, K.W.; Kim, H.S.; Kim, A.I.; Craig, J.W.; Chen, K.X.; Roberson, J.; Guenette, J.P.; Huang, R.Y. The Incidence and Treatment Response of Double Expression of MYC and BCL2 in Patients with Diffuse Large B-Cell Lymphoma: A Systematic Review and Meta-Analysis. Cancers 2021, 13, 3369. https://doi.org/10.3390/cancers13133369
Hwang J, Suh CH, Kim KW, Kim HS, Kim AI, Craig JW, Chen KX, Roberson J, Guenette JP, Huang RY. The Incidence and Treatment Response of Double Expression of MYC and BCL2 in Patients with Diffuse Large B-Cell Lymphoma: A Systematic Review and Meta-Analysis. Cancers. 2021; 13(13):3369. https://doi.org/10.3390/cancers13133369
Chicago/Turabian StyleHwang, Jisun, Chong Hyun Suh, Kyung Won Kim, Ho Sung Kim, Austin I. Kim, Jeffrey W. Craig, Ke Xun Chen, Joel Roberson, Jeffrey P. Guenette, and Raymond Y. Huang. 2021. "The Incidence and Treatment Response of Double Expression of MYC and BCL2 in Patients with Diffuse Large B-Cell Lymphoma: A Systematic Review and Meta-Analysis" Cancers 13, no. 13: 3369. https://doi.org/10.3390/cancers13133369