
Extending Age Ranges in Breast Cancer Screening in Four European Countries: Model Estimations of Harm-to-Benefit Ratios

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Model Overview
2.2. Analysis
2.3. Outcomes
- Overdiagnosed breast cancer cases/averted breast cancer deaths;
- False-positive results/averted breast cancer deaths;
- Overdiagnosed breast cancer cases/LYG;
- False-positive results/LYG.
2.4. Sensitivity Analysis
3. Results
3.1. Model Calibration and Validation
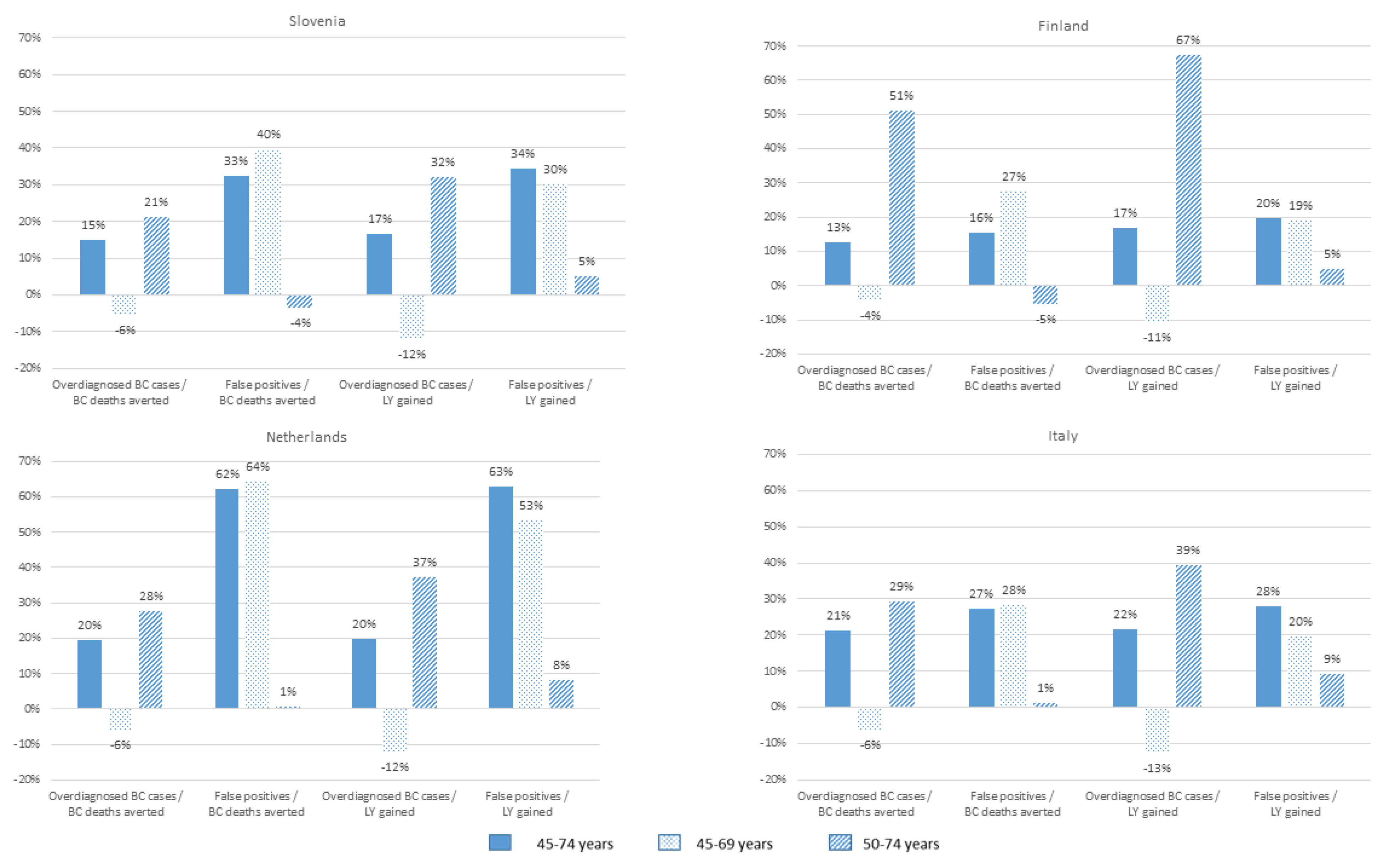
3.2. Outcomes of Different Screening Strategies
3.3. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Council of the European Union. Council Recommendation of 2 December 2003 on Cancer Screening (2003/878/EC). Off. J. Eur. Union 2003, 327, 34–38. [Google Scholar]
- Nelson, H.D.; Fu, R.; Cantor, A.; Pappas, M.; Daeges, M.; Humphrey, L.L. Effectiveness of Breast Cancer Screening: Systematic Review and Meta-analysis to Update the 2009 U.S. Preventive Services Task Force Recommendation. Ann. Intern. Med. 2016, 164, 244–255. [Google Scholar] [CrossRef]
- Broeders, M.; Moss, S.; Nyström, L.; Njor, S.; Jonsson, H.; Paap, E.; Massat, N.; Duffy, S.; Lynge, E.; Paci, E. The impact of mammographic screening on breast cancer mortality in Europe: A review of observational studies. J. Med. Screen. 2012, 19 (Suppl. S1), 14–25. [Google Scholar] [CrossRef] [PubMed]
- Zielonke, N.; Gini, A.; Jansen, E.E.; Anttila, A.; Segnan, N.; Ponti, A.; Veerus, P.; de Koning, H.J.; van Ravesteyn, N.T.; Priaulx, J. Evidence for reducing cancer specific mortality due to screening for breast cancer in Europe: A systematic review. Eur. J. Cancer 2020, 127, 191–206. [Google Scholar] [CrossRef] [Green Version]
- Marmot, M.G.; Altman, D.G.; Cameron, D.A.; Dewar, J.A.; Thompson, S.G.; Wilcox, M. The benefits and harms of breast cancer screening: An independent review. Br. J. Cancer 2013, 108, 2205–2240. [Google Scholar] [CrossRef] [Green Version]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Benbrahim-Tallaa, L.; Bouvard, V.; Bianchini, F.; Straif, K. Breast-Cancer Screening—Viewpoint of the IARC Working Group. N. Engl. J. Med. 2015, 372, 2353–2358. [Google Scholar] [CrossRef] [Green Version]
- European Commission Initiative on Breast Cancer. Recommendations from the European Breast Guidlines. 2021. Available online: https://ecibc.jrc.ec.europa.eu/recommendations/ (accessed on 22 December 2020).
- IARC. Cancer Screening in the European Union. Report on the Implementation of the Council Recommendation on Cancer Screening; IARC: Lyon, France, 2017; Available online: 2017_cancerscreening_2ndreportimplementation_en.pdf (accessed on 8 November 2020).
- Zielonke, N.; Kregting, L.M.; Heijnsdijk, E.A.M.; Veerus, P.; Heinävaara, S.; McKee, M.; de Kok, I.M.; de Koning, H.J.; van Ravesteyn, N.T.; Collaborators, T.E. The potential of breast cancer screening in Europe. Int. J. Cancer 2021, 148, 406–418. [Google Scholar] [CrossRef]
- IARC Working Group. IARC Handbooks of Cancer Prevention, Volume 15: Breast Cancer Screening; International Agency for Research on Cancer: Lyon, France, 2016. [Google Scholar]
- Bray, F.; Colombet, M.; Mery, L.; Pineros, M.; Znaor, A.; Zanetti, R.; Ferlay, J. (Eds.) Cancer Incidence in Five Continents, Vol. XI (Electronic Version); International Agency for Research on Cancer: Lyon, France, 2017; Available online: http://ci5iarcfr (accessed on 14 January 2021).
- van den Ende, C.; Oordt-Speets, A.M.; Vroling, H.; van Agt, H.M. Benefits and harms of breast cancer screening with mammography in women aged 40–49 years: A systematic review. Int. J. Cancer 2017, 141, 1295–1306. [Google Scholar] [CrossRef] [Green Version]
- Mandrik, O.; Zielonke, N.; Meheus, F.; Severens, J.L.; Guha, N.; Acosta, R.H.; Murillo, R. Systematic reviews as a ‘lens of evidence’: Determinants of benefits and harms of breast cancer screening. Int. J. Cancer 2019, 145, 994–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wanders, J.O.; Holland, K.; Veldhuis, W.B.; Mann, R.M.; Pijnappel, R.M.; Peeters, P.H.; van Gils, C.H.; Karssemeijer, N. Volumetric breast density affects performance of digital screening mammography. Breast Cancer Res. Treat. 2017, 162, 95–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beau, A.B.; Lynge, E.; Njor, S.H.; Vejborg, I.; Lophaven, S.N. Benefit-to-harm ratio of the Danish breast cancer screening programme. Int. J. Cancer 2017, 141, 512–518. [Google Scholar] [CrossRef] [Green Version]
- Van Ravesteyn, N.T.; Miglioretti, D.L.; Stout, N.K.; Lee, S.J.; Schechter, C.B.; Buist, D.S.; Huang, H.; Heijnsdijk, E.A.M.; Trentham-Dietz, A.; Alagoz, O.; et al. What level of risk tips the balance of benefits and harms to favor screening mammography starting at age 40? Ann. Intern. Med. 2012, 156, 609–617. [Google Scholar] [CrossRef]
- Sankatsing, V.D.; Heijnsdijk, E.A.; Van Luijt, P.A.; Van Ravesteyn, N.T.; Fracheboud, J.; De Koning, H.J. Cost-effectiveness of digital mammography screening before the age of 50 in The Netherlands. Int. J. Cancer 2015, 137, 1990–1999. [Google Scholar] [CrossRef] [PubMed]
- Tosteson, A.N.A.; Fryback, D.G.; Hammond, C.S.; Hanna, L.G.; Grove, M.R.; Brown, M.; Wang, Q.; Lindfors, K.; Pisano, E.D. Consequences of False-Positive Screening Mammograms. JAMA Intern. Med. 2014, 174, 954–961. [Google Scholar] [CrossRef]
- Jørgensen, K.J.; Klahn, A.; Gøtzsche, P.C. Are benefits and harms in mammography screening given equal attention in scientific articles? A cross-sectional study Review. BMC Med. 2007, 5, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofvind, S.; Román, M.; Sebuødegård, S.; Falk, R.S. Balancing the benefits and detriments among women targeted by the Norwegian Breast Cancer Screening Program. J. Med Screen. 2016, 23, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, J.S.; Sheffield, K.; Li, S.; Tan, A. Receipt of Cancer Screening Is a Predictor of Life Expectancy. J. Gen. Intern. Med. 2016, 31, 1308–1314. [Google Scholar] [CrossRef] [Green Version]
- Sicsic, J.; Pelletier-Fleury, N.; Moumjid, N. Women’s Benefits and Harms Trade-Offs in Breast Cancer Screening: Results from a Discrete-Choice Experiment. Value Health 2018, 21, 78–88. [Google Scholar] [CrossRef] [Green Version]
- Paci, E.; Group, E.W. Summary of the evidence of breast cancer service screening outcomes in Europe and first estimate of the benefit and harm balance sheet. J. Med. Screen. 2012, 19 (Suppl. S1), 5–13. [Google Scholar] [CrossRef]
- De Gelder, R.; Heijnsdijk, E.A.; Van Ravesteyn, N.T.; Fracheboud, J.; Draisma, G.; De Koning, H.J. Interpreting overdiagnosis estimates in population-based mammography screening. Epidemiol. Rev. 2011, 33, 111–121. [Google Scholar] [CrossRef] [Green Version]
- Arrospide, A.; Rue, M.; Van Ravesteyn, N.T.; Comas, M.; Larrañaga, N.; Sarriugarte, G.; Mar, J. Evaluation of health benefits and harms of the breast cancer screening programme in the Basque Country using discrete event simulation. BMC Cancer 2015, 15, 671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Luijt, P.A.; Heijnsdijk, E.A.M.; de Koning, H.J. Cost-effectiveness of the Norwegian breast cancer screening program. Int. J. Cancer 2017, 140, 833–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pashayan, N.; Morris, S.; Gilbert, F.J.; Pharoah, P.D. Cost-effectiveness and Benefit-to-Harm Ratio of Risk-Stratified Screening for Breast Cancer: A Life-Table Model. JAMA Oncol. 2018, 4, 1504–1510. [Google Scholar] [CrossRef] [Green Version]
- Jahn, B.; Sroczynski, G.; Bundo, M.; Mühlberger, N.; Puntscher, S.; Todorovic, J.; Rochau, U.; Oberaigner, W.; Koffijberg, H.; Fischer, T.; et al. Effectiveness, benefit harm and cost effectiveness of colorectal cancer screening in Austria. BMC Gastroenterol. 2019, 19, 209. [Google Scholar] [CrossRef] [Green Version]
- Tabár, L.; Vitak, B.; Chen, T.H.-H.; Yen, A.M.-F.; Cohen, A.; Tot, T.; Chiu, S.Y.-H.; Chen, S.L.-S.; Fann, J.C.-Y.; Rosell, J.; et al. Swedish two-county trial: Impact of mammographic screening on breast cancer mortality during 3 decades. Radiology 2011, 260, 658–663. [Google Scholar] [CrossRef] [Green Version]
- Andersson, I.; Aspegren, K.; Janzon, L.; Landberg, T.; Lindholm, K.; Linell, F.; Ljungberg, O.; Ranstam, J.; Sigfusson, B. Mammographic screening and mortality from breast cancer: The Malmo mammographic screening trial. Br. Med. J. 1988, 297, 943–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Broek, J.J.; van Ravesteyn, N.T.; Mandelblatt, J.S.; Huang, H.; Ergun, M.A.; Burnside, E.S.; Xu, C.; Li, Y.; Alagoz, O.; Lee, S.J.; et al. Comparing CISNET Breast Cancer Incidence and Mortality Predictions to Observed Clinical Trial Results of Mammography Screening from Ages 40 to 49. Med. Decis. Mak. 2018, 38 (Suppl. S1), 140S–150S. [Google Scholar] [CrossRef]


{kind=link}
| Examination Coverage by per Age Group 1 | Slovenia | Finland | Netherlands | Italy |
|---|---|---|---|---|
| 45–49 | 54.3% 2 | 85.0% 2 | 75.5% 2 | 59.6% 2 |
| 50–54 | 54.3% | 85.0% | 75.5% | 59.6% |
| 55–59 | 65.0% | 85.9% | 76.2% | 63.2% |
| 60–64 | 52.4% | 86.8% | 76.3% | 63.9% |
| 65–69 | 48.8% | 73.0% | 75.7% | 61.5% |
| 70–74 | 48.8% 2 | 73.0% 2 | 70.1% | 61.5% 2 |
| Stage-specific sensitivity of digital mammography DCIS | 0.726 | 0.596 3 | 0.865 4 | 0.821 |
| Stage-specific sensitivity of digital mammography T1a | 0.785 | 0.811 | 0.553 3 | 1 4 |
| Stage-specific sensitivity of digital mammography T1b | 0.656 | 0.761 4 | 0.481 3 | 0.717 |
| Stage-specific sensitivity of digital mammography T1c | 0.780 3 | 0.946 4 | 0.857 | 0.814 |
| Stage-specific sensitivity of digital mammography T2+ | 1 | 1 | 1 | 1 |
| Referral rate by age 5 | ||||
| <50 | 0.040 | 0.030 | 0.030 3 | 0.065 4 |
| >50 | 0.034 | 0.028 | 0.023 3 | 0.058 4 |
| Country | Strategy 1 | Number of Screening Tests | Harms | Benefits | Harm-to-Benefit Ratios | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Overdiagnosed BC Cases | False Positives | BC Deaths Averted | LY Gained | Overdiagnosed BC Cases/BC Deaths Averted | False Positives/BC Deaths Averted | Overdiagnosed BC Cases/LY Gained | False Positives/LY Gained | |||
| Slovenia | 50–69 * | 9236 | 3.3 | 275.8 | 7.3 | 96.5 | 0.5 | 37.9 | 0.034 | 2.9 |
| 45–74 | 13,723 | +1.8 | +220.8 | +2.6 | +32.7 | 0.5 | 50.3 | 0.040 | 3.8 | |
| 45–69 | 11,696 | +0.1 | +150.2 | +0.8 | +18.2 | 0.4 | 53.0 | 0.030 | 3.7 | |
| 50–74 | 11,264 | +1.7 | +58.4 | +1.9 | +14.8 | 0.5 | 36.6 | 0.045 | 3.0 | |
| Finland | 50–69 * | 9170 | 2.6 | 212.3 | 7.7 | 105.3 | 0.3 | 27.6 | 0.025 | 2.0 |
| 45–74 | 13,632 | +1.5 | +135.6 | +3.2 | +38.8 | 0.4 | 31.9 | 0.029 | 2.4 | |
| 45–69 | 12,034 | +0.4 | +96.7 | +1.4 | +24.2 | 0.3 | 34.2 | 0.023 | 2.4 | |
| 50–74 | 11,183 | +1.4 | +48.8 | +2.4 | +19.4 | 0.4 | 25.9 | 0.032 | 2.1 | |
| Netherlands | 50–69 | 8948 | 3.2 | 150.1 | 13.0 | 185.6 | 0.2 | 11.6 | 0.017 | 0.8 |
| 45–74 | 13,288 | +1.9 | +172.5 | +4.2 | +59.5 | 0.3 | 18.8 | 0.021 | 1.3 | |
| 45–69 | 11,388 | +0.2 | +129.7 | +1.8 | +40 | 0.2 | 19.0 | 0.015 | 1.2 | |
| 50–74 * | 10,848 | +1.7 | +29.5 | +2.5 | +19.6 | 0.3 | 11.6 | 0.024 | 0.9 | |
| Italy | 50–69 * | 9186 | 2.5 | 488.5 | 10.7 | 152.1 | 0.2 | 45.7 | 0.016 | 3.2 |
| 45–74 | 13,657 | +1.5 | +338.8 | +3.5 | +49.2 | 0.3 | 58.2 | 0.020 | 4.1 | |
| 45–69 | 11,641 | +0.1 | +219.1 | +1.4 | +32.0 | 0.2 | 58.7 | 0.014 | 3.8 | |
| 50–74 | 11,203 | +1.4 | +105.5 | +2.1 | +17.2 | 0.3 | 46.3 | 0.023 | 3.5 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zielonke, N.; Geuzinge, A.; Heijnsdijk, E.A.M.; Heinävaara, S.; Senore, C.; Jarm, K.; de Koning, H.J.; van Ravesteyn, N.T.; on behalf of the EU-TOPIA Consortium. Extending Age Ranges in Breast Cancer Screening in Four European Countries: Model Estimations of Harm-to-Benefit Ratios. Cancers 2021, 13, 3360. https://doi.org/10.3390/cancers13133360
Zielonke N, Geuzinge A, Heijnsdijk EAM, Heinävaara S, Senore C, Jarm K, de Koning HJ, van Ravesteyn NT, on behalf of the EU-TOPIA Consortium. Extending Age Ranges in Breast Cancer Screening in Four European Countries: Model Estimations of Harm-to-Benefit Ratios. Cancers. 2021; 13(13):3360. https://doi.org/10.3390/cancers13133360
Chicago/Turabian StyleZielonke, Nadine, Amarens Geuzinge, Eveline A. M. Heijnsdijk, Sirpa Heinävaara, Carlo Senore, Katja Jarm, Harry J. de Koning, Nicolien T. van Ravesteyn, and on behalf of the EU-TOPIA Consortium. 2021. "Extending Age Ranges in Breast Cancer Screening in Four European Countries: Model Estimations of Harm-to-Benefit Ratios" Cancers 13, no. 13: 3360. https://doi.org/10.3390/cancers13133360