
Impact of Chronic Obstruction Pulmonary Disease on Survival in Patients with Advanced Stage Lung Squamous Cell Carcinoma Undergoing Concurrent Chemoradiotherapy

Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Population
2.2. Inclusion and Exclusion Criteria
2.3. Study Covariates and Statistical Analysis
3. Results
3.1. Study Cohort
3.2. Effects of COPD and Hospitalization for COPDAE on Survival Outcomes of Patients with Lung SCC Receiving Definitive CCRT
3.3. Other Independent Predictors of Overall Survival in Patients with Lung SCC Receiving Definitive CCRT
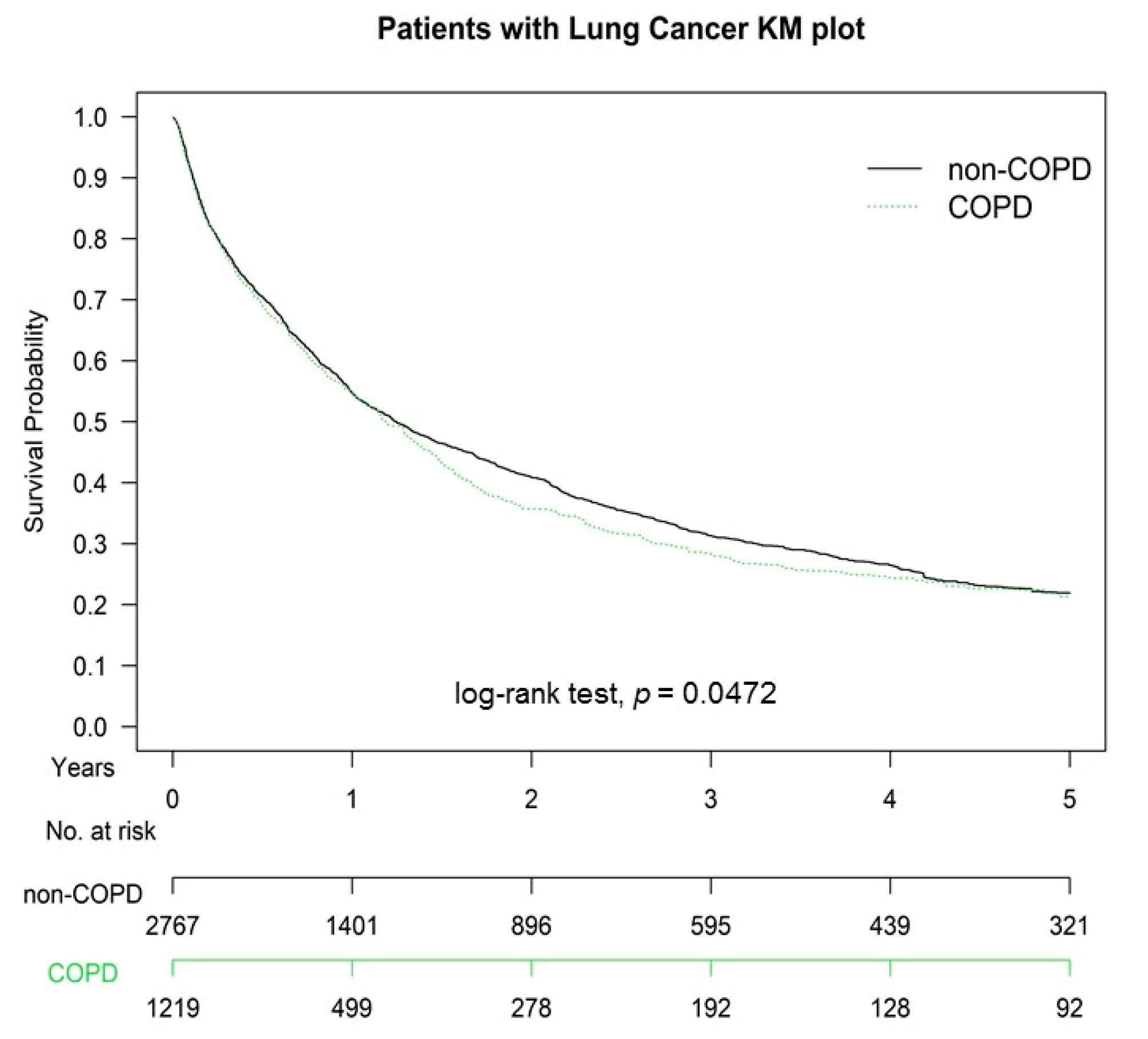
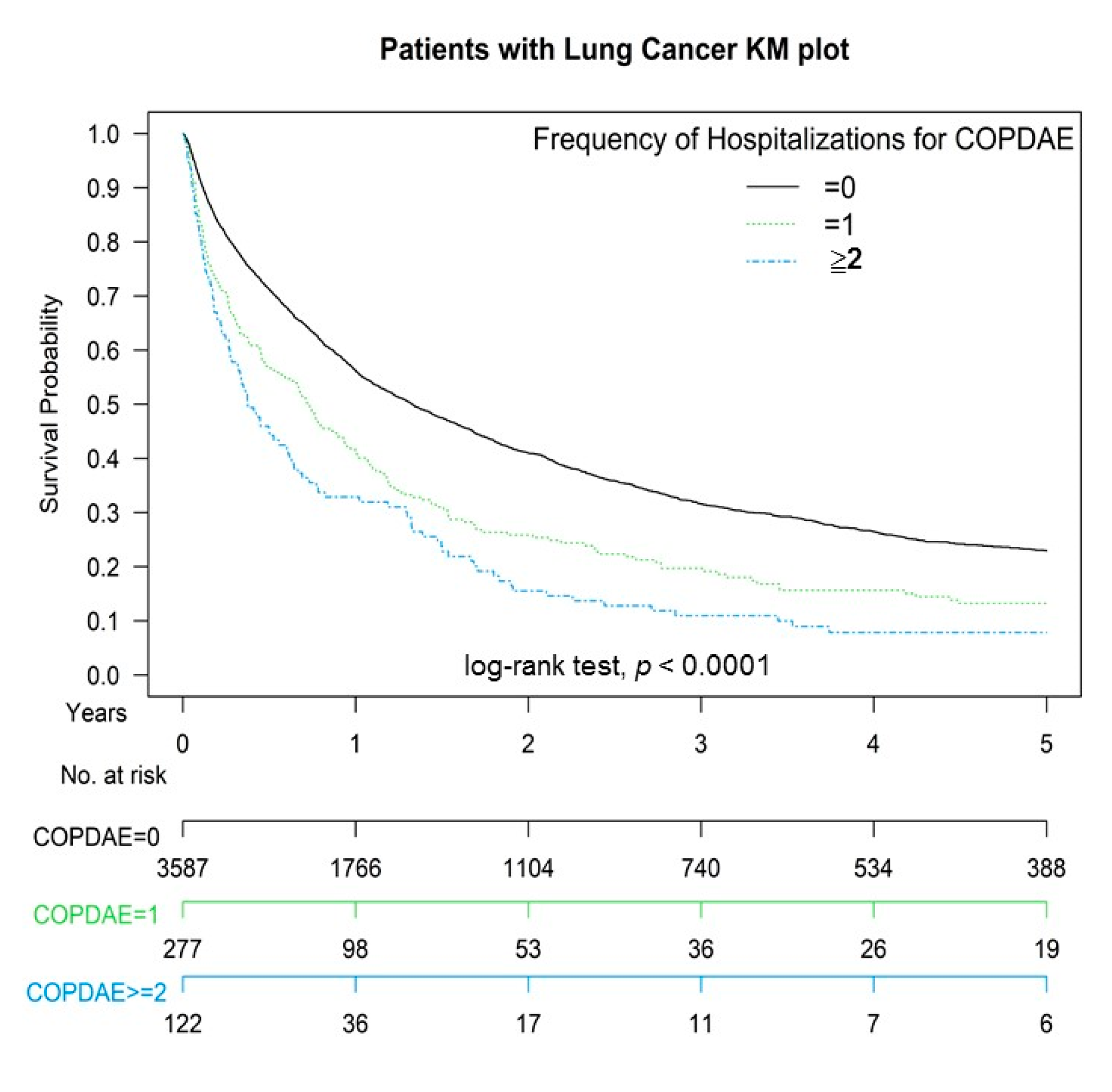
3.4. Survival Curves of COPD and Hospitalization for COPDAE in Patients with Lung SCC Receiving Definitive CCRT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COPD | chronic obstruction pulmonary disease |
| SCC | squamous cell carcinoma |
| CCRT | concurrent chemoradiotherapy |
| COPDAE | COPD with acute exacerbation |
| aHR | adjusted hazard ratio |
| CI | confidence interval |
| IPTW | inverse probability of treatment weighting |
| RT | radiotherapy |
| AJCC | American Joint Committee on Cancer |
| RILI | radiation-induced lung injury |
| RP | radiation pneumonitis |
| TCRD | Taiwan Cancer Registry Database |
| CCI | Charlson comorbidity index |
| ICD-10-CM | International Classification of Diseases, 10th Revision, Clinical Modification |
| CVD | cardiovascular disease |
| AMI | acute myocardial infarction |
| NTD | New Taiwan Dollar |
| NCCN | National Comprehensive Cancer Network |
| GOLD | Global Initiative for Chronic Obstructive Lung Disease |
References
- Papi, A.; Casoni, G.; Caramori, G.; Guzzinati, I.; Boschetto, P.; Ravenna, F.; Calia, N.; Petruzzelli, S.; Corbetta, L.; Cavallesco, G.; et al. COPD increases the risk of squamous histological subtype in smokers who develop non-small cell lung carcinoma. Thorax 2004, 59, 679–681. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, R.J.; Duan, F.; Chiles, C.; Greco, E.M.; Gamble, G.D.; Aberle, D.; Young, R.P. Reduced Expiratory Flow Rate among Heavy Smokers Increases Lung Cancer Risk. Results from the National Lung Screening Trial-American College of Radiology Imaging Network Cohort. Ann. Am. Thorac. Soc. 2017, 14, 392–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durham, A.L.; Adcock, I.M. The relationship between COPD and lung cancer. Lung Cancer 2015, 90, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Young, R.P.; Hopkins, R.J.; Gamble, G.D.; Etzel, C.; El-Zein, R.; Crapo, J.D. Genetic evidence linking lung cancer and COPD: A new perspective. Appl. Clin. Genet. 2011, 4, 99–111. [Google Scholar] [CrossRef] [Green Version]
- Bowman, R.V.; Yang, I.A.; Semmler, A.B.; Fong, K.M. Epigenetics of lung cancer. Respirology 2006, 11, 355–365. [Google Scholar] [CrossRef] [PubMed]
- Houghton, A.M.; Mouded, M.; Shapiro, S.D. Common origins of lung cancer and COPD. Nat. Med. 2008, 14, 1023–1024. [Google Scholar] [CrossRef]
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. 2018 Report; Global Initiative for Chronic Obstructive Lung Disease, Inc.: Fontana, WI, USA, 28 October 2018. [Google Scholar]
- de-Torres, J.P.; Wilson, D.O.; Sanchez-Salcedo, P.; Weissfeld, J.L.; Berto, J.; Campo, A.; Alcaide, A.B.; Garcia-Granero, M.; Celli, B.R.; Zulueta, J.J. Lung cancer in patients with chronic obstructive pulmonary disease. Development and validation of the COPD Lung Cancer Screening Score. Am. J. Respir. Crit. Care Med. 2015, 191, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Donaldson, G.C.; Seemungal, T.A.; Bhowmik, A.; Wedzicha, J.A. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax 2002, 57, 847–852. [Google Scholar] [CrossRef] [Green Version]
- Curran, W.J., Jr.; Paulus, R.; Langer, C.J.; Komaki, R.; Lee, J.S.; Hauser, S.; Movsas, B.; Wasserman, T.; Rosenthal, S.A.; Gore, E.; et al. Sequential vs. concurrent chemoradiation for stage III non-small cell lung cancer: Randomized phase III trial RTOG 9410. J. Natl. Cancer Inst. 2011, 103, 1452–1460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albain, K.S.; Crowley, J.J.; Turrisi, A.T., 3rd; Gandara, D.R.; Farrar, W.B.; Clark, J.I.; Beasley, K.R.; Livingston, R.B. Concurrent cisplatin, etoposide, and chest radiotherapy in pathologic stage IIIB non-small-cell lung cancer: A Southwest Oncology Group phase II study, SWOG 9019. J. Clin. Oncol. 2002, 20, 3454–3460. [Google Scholar] [CrossRef] [PubMed]
- The National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology. Available online: http://www.nccn.org/professionals/physician_gls/f_guidelines.asp (accessed on 11 February 2020).
- Yirmibesoglu, E.; Higginson, D.S.; Fayda, M.; Rivera, M.P.; Halle, J.; Rosenman, J.; Xie, L.; Marks, L.B. Challenges scoring radiation pneumonitis in patients irradiated for lung cancer. Lung Cancer 2012, 76, 350–353. [Google Scholar] [CrossRef] [Green Version]
- Palma, D.; Lagerwaard, F.; Rodrigues, G.; Haasbeek, C.; Senan, S. Curative treatment of Stage I non-small-cell lung cancer in patients with severe COPD: Stereotactic radiotherapy outcomes and systematic review. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 1149–1156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rancati, T.; Ceresoli, G.L.; Gagliardi, G.; Schipani, S.; Cattaneo, G.M. Factors predicting radiation pneumonitis in lung cancer patients: A retrospective study. Radiother. Oncol. 2003, 67, 275–283. [Google Scholar] [CrossRef]
- Ma, L.D.; Taylor, G.A.; Wharam, M.D.; Wiley, J.M. “Recall” pneumonitis: Adriamycin potentiation of radiation pneumonitis in two children. Radiology 1993, 187, 465–467. [Google Scholar] [CrossRef] [PubMed]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.C.; Liu, H.E.; Kao, Y.W.; Qin, L.; Lin, K.C.; Fang, C.Y.; Tsai, L.L.; Shia, B.C.; Wu, S.Y. Definitive radiotherapy or surgery for early oral squamous cell carcinoma in old and very old patients: A propensity-score-matched, nationwide, population-based cohort study. Radiother. Oncol. 2020, 151, 214–221. [Google Scholar] [CrossRef]
- Lin, Y.K.; Hsieh, M.C.; Wang, W.W.; Lin, Y.C.; Chang, W.W.; Chang, C.L.; Cheng, Y.F.; Wu, S.Y. Outcomes of adjuvant treatments for resectable intrahepatic cholangiocarcinoma: Chemotherapy alone, sequential chemoradiotherapy, or concurrent chemoradiotherapy. Radiother. Oncol. 2018, 128, 575–583. [Google Scholar] [CrossRef]
- Lin, Y.K.; Hsieh, M.C.; Chang, C.L.; Chow, J.M.; Yuan, K.S.; Wu, A.T.H.; Wu, S.Y. Intensity-modulated radiotherapy with systemic chemotherapy improves survival in patients with nonmetastatic unresectable pancreatic adenocarcinoma: A propensity score-matched, nationwide, population-based cohort study. Radiother. Oncol. 2018, 129, 326–332. [Google Scholar] [CrossRef]
- Chen, T.M.; Lin, K.C.; Yuan, K.S.; Chang, C.L.; Chow, J.M.; Wu, S.Y. Treatment of advanced nasopharyngeal cancer using low- or high-dose concurrent chemoradiotherapy with intensity-modulated radiotherapy: A propensity score-matched, nationwide, population-based cohort study. Radiother. Oncol. 2017, 129, 23–29. [Google Scholar] [CrossRef]
- Chang, W.W.; Hsiao, P.K.; Qin, L.; Chang, C.L.; Chow, J.M.; Wu, S.Y. Treatment outcomes for unresectable intrahepatic cholangiocarcinoma: Nationwide, population-based, cohort study based on propensity score matching with the Mahalanobis metric. Radiother. Oncol. 2018, 129, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.L.; Tsai, H.C.; Lin, W.C.; Chang, J.H.; Hsu, H.L.; Chow, J.M.; Yuan, K.S.; Wu, A.T.H.; Wu, S.Y. Dose escalation intensity-modulated radiotherapy-based concurrent chemoradiotherapy is effective for advanced-stage thoracic esophageal squamous cell carcinoma. Radiother. Oncol. 2017, 125, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Auperin, A.; Le Pechoux, C.; Rolland, E.; Curran, W.J.; Furuse, K.; Fournel, P.; Belderbos, J.; Clamon, G.; Ulutin, H.C. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J. Clin. Oncol. 2010, 28, 2181–2190. [Google Scholar] [CrossRef] [PubMed]
- Vokes, E.E.; Herndon, J.E., 2nd; Kelley, M.J.; Cicchetti, M.G.; Ramnath, N.; Neill, H.; Atkins, J.N.; Watson, D.M.; Akerley, W.; Green, M.R. Induction chemotherapy followed by chemoradiotherapy compared with chemoradiotherapy alone for regionally advanced unresectable stage III Non-small-cell lung cancer: Cancer and Leukemia Group B. J. Clin. Oncol. 2007, 25, 1698–1704. [Google Scholar] [CrossRef]
- Belani, C.P.; Choy, H.; Bonomi, P.; Scott, C.; Travis, P.; Haluschak, J.; Curran, W.J., Jr. Combined chemoradiotherapy regimens of paclitaxel and carboplatin for locally advanced non-small-cell lung cancer: A randomized phase II locally advanced multi-modality protocol. J. Clin. Oncol. 2005, 23, 5883–5891. [Google Scholar] [CrossRef] [PubMed]
- Su, V.Y.; Yang, K.Y.; Yang, Y.H.; Tsai, Y.H.; Perng, D.W.; Su, W.J.; Chou, K.T.; Su, K.C.; Yen, Y.F.; Chen, P.C. Use of ICS/LABA Combinations or LAMA Is Associated with a Lower Risk of Acute Exacerbation in Patients with Coexistent COPD and Asthma. J. Allergy Clin. Immunol. Pract. 2018, 6, 1927–1935.e3. [Google Scholar] [CrossRef]
- Vatcheva, K.P.; Lee, M.; McCormick, J.B.; Rahbar, M.H. Multicollinearity in Regression Analyses Conducted in Epidemiologic Studies. Epidemiology 2016, 6. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Chen, J.H.; Yen, Y.C.; Yang, H.C.; Liu, S.H.; Yuan, S.P.; Wu, L.L.; Lee, F.P.; Lin, K.C.; Lai, M.T.; Wu, C.C.; et al. Curative-Intent Aggressive Treatment Improves Survival in Elderly Patients with Locally Advanced Head and Neck Squamous Cell Carcinoma and High Comorbidity Index. Medicine 2016, 95, e3268. [Google Scholar] [CrossRef]
- Lin, S.H.; Wang, L.; Myles, B.; Thall, P.F.; Hofstetter, W.L.; Swisher, S.G.; Ajani, J.A.; Cox, J.D.; Komaki, R.; Liao, Z. Propensity score-based comparison of long-term outcomes with 3-dimensional conformal radiotherapy vs intensity-modulated radiotherapy for esophageal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 1078–1085. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef] [PubMed]
- Senan, S.; Brade, A.; Wang, L.H.; Vansteenkiste, J.; Dakhil, S.; Biesma, B.; Martinez Aguillo, M.; Aerts, J.; Govindan, R.; Rubio-Viqueira, B.; et al. PROCLAIM: Randomized Phase III Trial of Pemetrexed-Cisplatin or Etoposide-Cisplatin Plus Thoracic Radiation Therapy Followed by Consolidation Chemotherapy in Locally Advanced Nonsquamous Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2016, 34, 953–962. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Liao, Z.; Wei, X.; Liu, H.H.; Tucker, S.L.; Hu, C.; Ajani, J.A.; Phan, A.; Swisher, S.G.; Mohan, R.; et al. Association between systemic chemotherapy before chemoradiation and increased risk of treatment-related pneumonitis in esophageal cancer patients treated with definitive chemoradiotherapy. J. Thorac. Oncol. 2008, 3, 277–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zinner, R.G.; Komaki, R.; Cox, J.D.; Glisson, B.S.; Pisters, K.M.; Herbst, R.S.; Kies, M.; Liao, Z.; Hong, W.K.; Fossella, F.V. Dose escalation of gemcitabine is possible with concurrent chest three-dimensional rather than two-dimensional radiotherapy: A phase I trial in patients with stage III non-small-cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 119–127. [Google Scholar] [CrossRef]
- Choy, H.; Jain, A.K.; Moughan, J.; Curran, W.; Whipple, G.; Demas, W.F.; Ettinger, D.S. RTOG 0017: A phase I trial of concurrent gemcitabine/carboplatin or gemcitabine/paclitaxel and radiation therapy (“ping-pong trial”) followed by adjuvant chemotherapy for patients with favorable prognosis inoperable stage IIIA/B non-small cell lung cancer. J. Thorac. Oncol. 2009, 4, 80–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Socinski, M.A.; Blackstock, A.W.; Bogart, J.A.; Wang, X.; Munley, M.; Rosenman, J.; Gu, L.; Masters, G.A.; Ungaro, P.; Sleeper, A.; et al. Randomized phase II trial of induction chemotherapy followed by concurrent chemotherapy and dose-escalated thoracic conformal radiotherapy (74 Gy) in stage III non-small-cell lung cancer: CALGB 30105. J. Clin. Oncol. 2008, 26, 2457–2463. [Google Scholar] [CrossRef] [PubMed]
- Arrieta, O.; Gallardo-Rincon, D.; Villarreal-Garza, C.; Michel, R.M.; Astorga-Ramos, A.M.; Martinez-Barrera, L.; de la Garza, J. High frequency of radiation pneumonitis in patients with locally advanced non-small cell lung cancer treated with concurrent radiotherapy and gemcitabine after induction with gemcitabine and carboplatin. J. Thorac. Oncol. 2009, 4, 845–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rengan, R.; Mick, R.; Pryma, D.; Rosen, M.A.; Lin, L.L.; Maity, A.M.; Evans, T.L.; Stevenson, J.P.; Langer, C.J.; Kucharczuk, J.; et al. A phase I trial of the HIV protease inhibitor nelfinavir with concurrent chemoradiotherapy for unresectable stage IIIA/IIIB non-small cell lung cancer: A report of toxicities and clinical response. J. Thorac. Oncol. 2012, 7, 709–715. [Google Scholar] [CrossRef] [Green Version]
- Ju, S.; Lee, H.R.; Kim, J.Y.; Kim, H.C.; Lee, G.W.; You, J.W.; Cho, Y.J.; Jeong, Y.Y.; Lee, J.D.; Lee, S.J. Impact of coexistent chronic obstructive pulmonary disease on the survival of patients with small cell lung cancer receiving chemotherapy. Thorac. Cancer 2018, 9, 1271–1278. [Google Scholar] [CrossRef]
- Lim, J.U.; Kang, H.S.; Yeo, C.D.; Kim, J.S.; Park, C.K.; Kim, Y.H.; Kim, J.W.; Kim, S.J.; Lee, S.H. Impact of Combined Chronic Obstructive Pulmonary Disease Status and Systemic Inflammation on Outcome of Advanced NSCLC: Multicenter Retrospective Cohort Study. Int. J. Chronic Obstr. Pulm. Dis. 2020, 15, 3323–3334. [Google Scholar] [CrossRef]
- Qiang, G.; Liang, C.; Xiao, F.; Yu, Q.; Wen, H.; Song, Z.; Tian, Y.; Shi, B.; Guo, Y.; Liu, D. Impact of chronic obstructive pulmonary disease on postoperative recurrence in patients with resected non-small-cell lung cancer. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Zhai, R.; Yu, X.; Shafer, A.; Wain, J.C.; Christiani, D.C. The impact of coexisting COPD on survival of patients with early-stage non-small cell lung cancer undergoing surgical resection. Chest 2014, 145, 346–353. [Google Scholar] [CrossRef] [Green Version]
- Feary, J.R.; Rodrigues, L.C.; Smith, C.J.; Hubbard, R.B.; Gibson, J.E. Prevalence of major comorbidities in subjects with COPD and incidence of myocardial infarction and stroke: A comprehensive analysis using data from primary care. Thorax 2010, 65, 956–962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cebron Lipovec, N.; Beijers, R.J.; van den Borst, B.; Doehner, W.; Lainscak, M.; Schols, A.M. The Prevalence of Metabolic Syndrome In Chronic Obstructive Pulmonary Disease: A Systematic Review. COPD Int. J. Chronic Obstr. Pulm. Dis. 2016, 13, 399–406. [Google Scholar] [CrossRef] [Green Version]
- Tager, I.B.; Speizer, F.E. Risk estimates for chronic bronchitis in smokers: A study of male-female differences. Am. Rev. Respir. Dis. 1976, 113, 619–625. [Google Scholar] [CrossRef]
- Xu, X.; Weiss, S.T.; Rijcken, B.; Schouten, J.P. Smoking, changes in smoking habits, and rate of decline in FEV1: New insight into gender differences. Eur. Respir. J. 1994, 7, 1056–1061. [Google Scholar] [PubMed]
- Allan, V.; Ramagopalan, S.V.; Mardekian, J.; Jenkins, A.; Li, X.; Pan, X.; Luo, X. Propensity score matching and inverse probability of treatment weighting to address confounding by indication in comparative effectiveness research of oral anticoagulants. J. Comp. Eff. Res. 2020, 9, 603–614. [Google Scholar] [CrossRef]
- Halpern, E.F. Behind the numbers: Inverse probability weighting. Radiology 2014, 271, 625–628. [Google Scholar] [CrossRef]
- Rubin, P.; Johnston, C.J.; Williams, J.P.; McDonald, S.; Finkelstein, J.N. A perpetual cascade of cytokines postirradiation leads to pulmonary fibrosis. Int. J. Radiat. Oncol. Biol. Phys. 1995, 33, 99–109. [Google Scholar] [CrossRef]
- Urvay, S.E.; Yucel, B.; Erdis, E.; Turan, N. Prognostic Factors in Stage III Non-Small-Cell Lung Cancer Patients. Asian Pac. J. Cancer Prev. 2016, 17, 4693–4697. [Google Scholar] [CrossRef] [PubMed]
- Asmis, T.R.; Ding, K.; Seymour, L.; Shepherd, F.A.; Leighl, N.B.; Winton, T.L.; Whitehead, M.; Spaans, J.N.; Graham, B.C.; Goss, G.D.; et al. Age and comorbidity as independent prognostic factors in the treatment of non small-cell lung cancer: A review of National Cancer Institute of Canada Clinical Trials Group trials. J. Clin. Oncol. 2008, 26, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Barletta, J.A.; Yeap, B.Y.; Chirieac, L.R. Prognostic significance of grading in lung adenocarcinoma. Cancer 2010, 116, 659–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giraud, P.; Morvan, E.; Claude, L.; Mornex, F.; Le Pechoux, C.; Bachaud, J.M.; Boisselier, P.; Beckendorf, V.; Morelle, M.; Carrere, M.O. Respiratory gating techniques for optimization of lung cancer radiotherapy. J. Thorac. Oncol. 2011, 6, 2058–2068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giraud, P.; Djadi-Prat, J.; Morvan, E.; Morelle, M.; Remmonay, R.; Pourel, N.; Durdux, C.; Carrie, C.; Mornex, F.; Le Pechoux, C.; et al. Dosimetric and clinical benefits of respiratory-gated radiotherapy for lung and breast cancers: Results of the STIC 2003. Cancer Radiother. 2012, 16, 272–281. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| No COPD before CCRT N = 2767 | COPD before CCRT N = 1219 | p | |||
|---|---|---|---|---|---|
| N | (%) | N | (%) | ||
| Age (mean ± SD) | (65.42 ± 12.90) | (73.10 ± 10.25) | <0.0001 | ||
| Age | <0.0001 | ||||
| Age ≤ 65 years | 1330 | 48.07% | 246 | 20.18% | |
| >65 years Age ≤ 75 years | 743 | 26.85% | 390 | 31.99% | |
| >75 years Age ≤ 85 years | 557 | 20.13% | 465 | 38.15% | |
| Age > 85 years | 137 | 4.95% | 118 | 9.68% | |
| Sex | <0.0001 | ||||
| Female | 1233 | 44.56% | 243 | 19.93% | |
| Male | 1534 | 55.44% | 976 | 80.07% | |
| AJCC clinical stage | 0.9131 | ||||
| Stage IIIA | 111 | 40.33% | 499 | 40.94% | |
| Stage IIIB | 1651 | 59.67% | 720 | 59.06% | |
| Histological degree of differentiation | 0.9137 | ||||
| Low | 636 | 22.99% | 292 | 23.95% | |
| Moderate | 1165 | 42.10% | 524 | 42.99% | |
| Diabetes | 0.0041 | ||||
| No | 2155 | 77.88% | 898 | 73.67% | |
| Yes | 612 | 22.12% | 321 | 26.33% | |
| Chronic bronchitis | <0.0001 | ||||
| No | 2705 | 97.76% | 1101 | 90.32% | |
| Yes | 62 | 2.24% | 118 | 9.68% | |
| Asthma | <0.0001 | ||||
| No | 2477 | 89.52% | 717 | 58.82% | |
| Yes | 290 | 10.48% | 502 | 41.18% | |
| Emphysema | 0.3231 | ||||
| No | 2734 | 98.81% | 1199 | 98.36% | |
| Yes | 33 | 1.19% | 20 | 1.64% | |
| Cardiovascular diseases | <0.0001 | ||||
| No | 1119 | 40.44% | 264 | 21.66% | |
| Yes | 1648 | 59.56% | 955 | 78.34% | |
| AMI | <0.0001 | ||||
| No | 2703 | 97.69% | 1144 | 93.85% | |
| Yes | 64 | 2.31% | 75 | 6.15% | |
| Stroke | <0.0001 | ||||
| No | 2624 | 94.83% | 1118 | 91.71% | |
| Yes | 143 | 5.17% | 101 | 8.29% | |
| CCI score | <0.0001 | ||||
| 0 | 2330 | 84.21% | 844 | 69.24% | |
| 1 | 71 | 2.57% | 49 | 4.02% | |
| ≥2 | 366 | 13.23% | 326 | 26.74% | |
| Income level | <0.0001 | ||||
| <NTD18,000 | 70 | 2.53% | 58 | 4.76% | |
| NTD18,000–22,500 | 1538 | 55.58% | 769 | 63.08% | |
| NTD22,500–30,000 | 726 | 26.24% | 328 | 26.91% | |
| >NTD30,000 | 433 | 15.65% | 64 | 5.25% | |
| Urbanization | <0.0001 | ||||
| Rural | 815 | 29.45% | 437 | 35.85% | |
| Urban | 1952 | 70.55% | 782 | 64.15% | |
| Hospitalizations for COPDAE within 1 year before diagnosis | <0.0001 | ||||
| 0 | 2767 | 100.00% | 820 | 67.27% | |
| 1 | 0 | 0.00% | 277 | 22.72% | |
| ≥2 | 0 | 0.00% | 122 | 10.01% | |
| Follow-up years Median (IQR, Q1, Q3) | 1.92 (0.34, 2.63) | 1.09 (0.22, 1.78) | <0.0001 | ||
| All-cause death | 1885 68.12% | 938 76.95% | <0.0001 | ||
| COPD death | 0 0% | 36 2.95% | <0.0001 | ||
| Lung cancer death | 1790 64.69% | 891 73.10% | <0.0001 | ||
| Crude HR (95% CI) | Adjusted HR (95% CI) * | p | |||
|---|---|---|---|---|---|
| COPD (ref. non-COPD) | |||||
| COPD | 1.37 | (1.26, 1.51) | 1.06 | (1.07, 1.71) | 0.0311 |
| Frequency of hospitalizations for COPDAE before diagnosis (ref. 0) | |||||
| 1 | 1.51 | (1.38, 1.74) | 1.29 | (1.16, 1.43) | <0.0001 |
| ≥2 | 1.97 | (1.61, 2.29) | 1.77 | (1.41, 2.13) | <0.0001 |
| Age (ref. Age > 85 years) | |||||
| Age ≤ 65 years | 0.38 | (0.28, 0.43) | 0.47 | (0.43, 0.57) | <0.0001 |
| >65 years Age ≤ 75 years | 0.45 | (0.39, 0.51) | 0.51 | (0.39, 0.66) | <0.0001 |
| >75 years Age ≤ 85 years | 0.67 | (0.59, 0.79) | 0.73 | (0.69, 0.82) | <0.0001 |
| Sex (ref. Female) | |||||
| Male | 1.47 | (1.39, 1.63) | 1.21 | (1.10, 1.29) | <0.0001 |
| AJCC clinical stage (ref. Stage IIIA) | |||||
| Stage IIIB | 1.28 | (1.06, 1.39) | 1.20 | (1.09, 1.41) | <0.0001 |
| Histological degree of differentiation (ref. Low) | |||||
| Moderate | 1.07 | (0.72, 1.95) | 1.17 | (1.57, 1.89) | 0.003 |
| High | 1.12 | (0.63, 1.53) | 1.35 | (1.08, 1.85) | 0.009 |
| CCI score (ref. 0) | |||||
| 1 | 1.42 | (1.199, 1.74) | 1.12 | (0.81, 1.11) | 0.3181 |
| ≥2 | 1.36 | (1.22, 1.61) | 1.18 | (1.07, 1.27) | <0.0001 |
| Diabetes (ref. No) | |||||
| Yes | 1.08 | (0.89, 1.29) | 1.06 | (0.84, 1.25) | 0.3530 |
| Chronic bronchitis (ref. No) | |||||
| Yes | 1.03 | (0.89, 1.07) | 1.02 | (0.83, 1.09) | 0.1911 |
| Asthma (ref. No) | |||||
| Yes | 1.04 | (0.87, 1.28) | 1.04 | (0.71, 1.24) | 0.2719 |
| Emphysema (ref. No) | |||||
| Yes | 1.11 | (0.95, 1.29) | 1.08 | (0.91, 1.29) | 0.2619 |
| Cardiovascular diseases (ref. No) | |||||
| Yes | 1.07 | (0.95, 1.18) | 1.04 | (0.87, 1.27) | 0.5416 |
| AMI (ref. No) | |||||
| 1.05 | (0.90, 1.07) | 1.03 | (0.89, 1.13) | 0.3801 | |
| Stroke (ref. No) | |||||
| 1.01 | (0.91, 1.06) | 1.00 | (0.82, 1.09) | 0.4797 | |
| Income level (ref. <NTD18,000) | |||||
| NTD18,000–22,500 | 0.93 | (0.71, 1.19) | 0.93 | (0.81, 1.13) | 0.2461 |
| NTD22,500–30,000 | 0.81 | (0.68, 0.97) | 0.81 | (0.71, 1.11) | 0.0881 |
| >NTD30,000 | 0.68 | (0.41, 0.81) | 0.61 | (0.53, 0.77) | <0.0001 |
| Urbanization (ref. Rural) | |||||
| Urban | 0.80 | (0.71, 0.88) | 0.79 | (0.74, 0.87) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, K.-C.; Lin, W.-C.; Chang, C.-L.; Wu, S.-Y. Impact of Chronic Obstruction Pulmonary Disease on Survival in Patients with Advanced Stage Lung Squamous Cell Carcinoma Undergoing Concurrent Chemoradiotherapy. Cancers 2021, 13, 3231. https://doi.org/10.3390/cancers13133231
Chiu K-C, Lin W-C, Chang C-L, Wu S-Y. Impact of Chronic Obstruction Pulmonary Disease on Survival in Patients with Advanced Stage Lung Squamous Cell Carcinoma Undergoing Concurrent Chemoradiotherapy. Cancers. 2021; 13(13):3231. https://doi.org/10.3390/cancers13133231
Chicago/Turabian StyleChiu, Kuo-Chin, Wei-Chun Lin, Chia-Lun Chang, and Szu-Yuan Wu. 2021. "Impact of Chronic Obstruction Pulmonary Disease on Survival in Patients with Advanced Stage Lung Squamous Cell Carcinoma Undergoing Concurrent Chemoradiotherapy" Cancers 13, no. 13: 3231. https://doi.org/10.3390/cancers13133231