
Associations of General and Abdominal Obesity with the Risk of Glioma Development

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Characteristics of the Study Population
2.2. Incidence Rates and Risks of Developing Gliomas According to BMI and WC
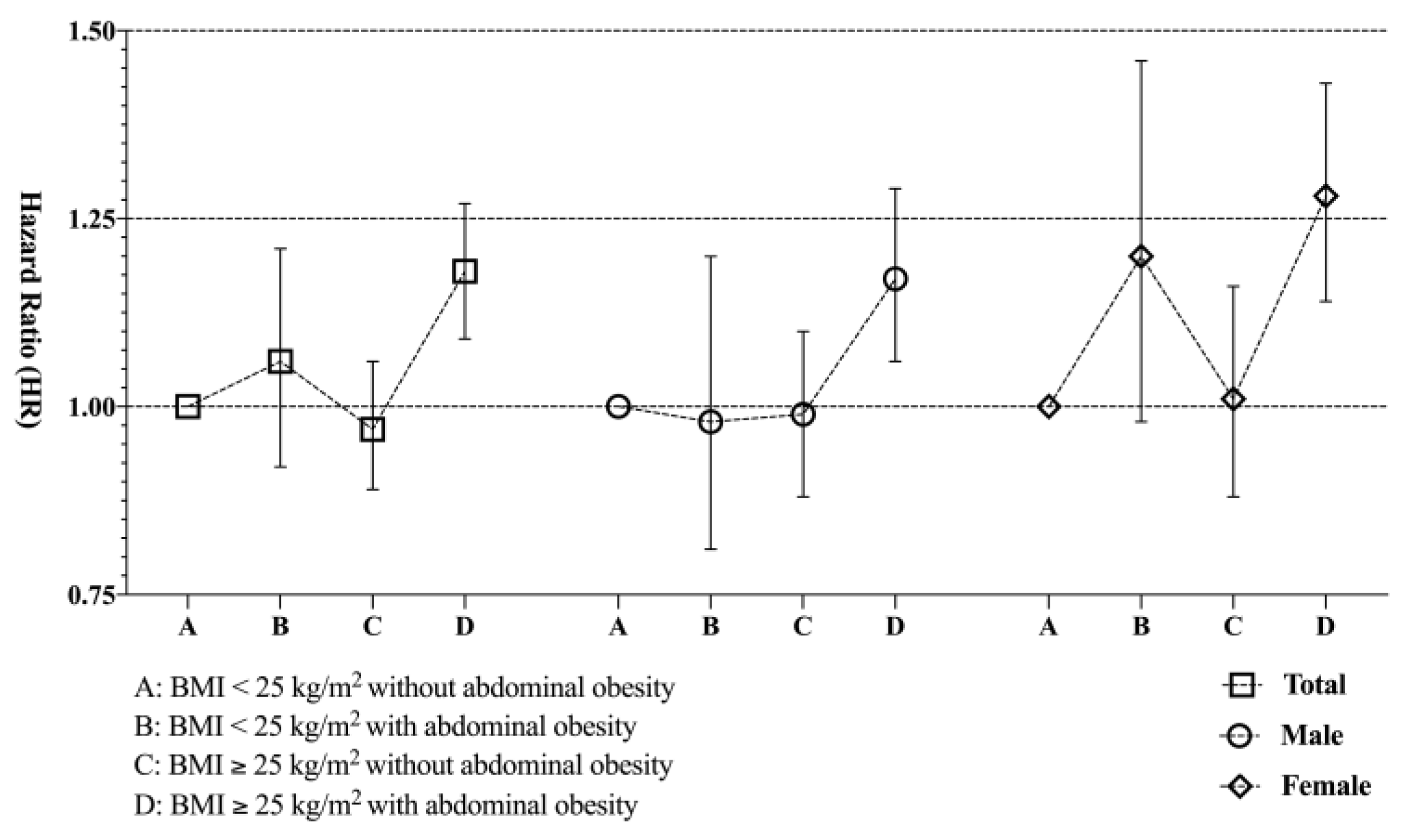
2.3. Impact of Abdominal Obesity on the Association between BMI and Risk of Gliomas
2.4. Subgroup Analysis According to Sex
3. Discussion
4. Materials and Methods
4.1. Ethical Considerations
4.2. Database Resource
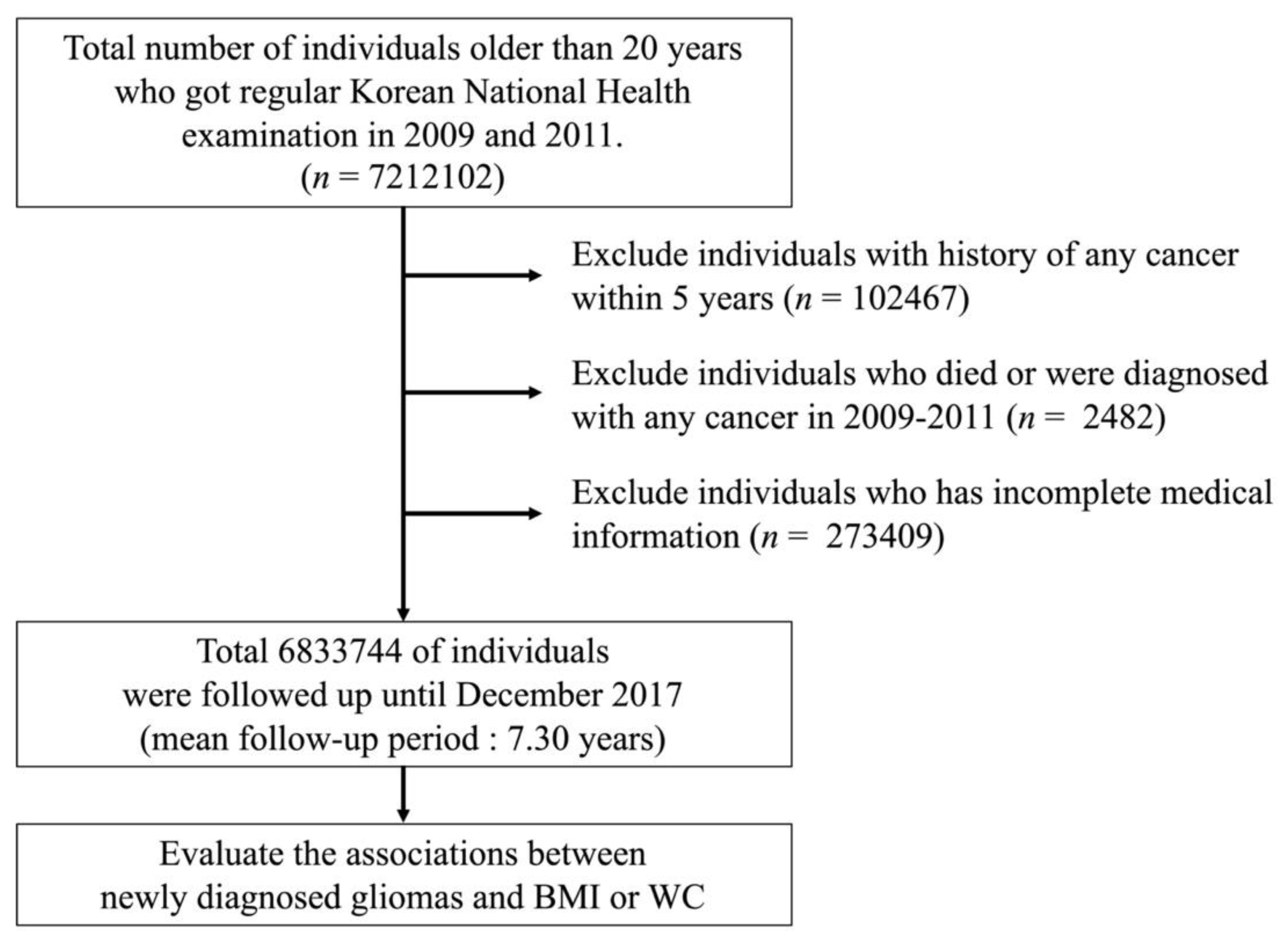
4.3. Study Population
4.4. Definition of Glioma
4.5. Clinical Variables
4.6. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Molinaro, A.M.; Taylor, J.W.; Wiencke, J.K.; Wrensch, M.R. Genetic and molecular epidemiology of adult diffuse glioma. Nat. Rev. Neurol. 2019, 15, 405–417. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization classification of tumors of the central nervous system: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Ostrom, Q.T.; Cioffi, G.; Gittleman, H.; Patil, N.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the United States in 2012–2016. Neuro-Oncol. 2019, 21, 1–100. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Hegi, M.E.; Mason, W.P.; Van Den Bent, M.J.; Taphoorn, M.J.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- Barnholtz-Sloan, J.S.; Ostrom, Q.T.; Cote, D. Epidemiology of brain tumors. Neurolog. Clin. 2018, 36, 395–419. [Google Scholar] [CrossRef]
- Ostrom, Q.T.; Adel Fahmideh, M.; Cote, D.J.; Muskens, I.S.; Schraw, J.M.; Scheurer, M.E.; Bondy, M.L. Risk factors for childhood and adult primary brain tumors. Neuro-Oncol. 2019, 21, 1357–1375. [Google Scholar] [CrossRef] [PubMed]
- Renehan, A.G.; Tyson, M.; Egger, M.; Heller, R.F.; Zwahlen, M. Body-mass index and incidence of cancer: A systematic review and meta-analysis of prospective observational studies. The Lancet 2008, 371, 569–578. [Google Scholar] [CrossRef]
- Calle, E.E.; Rodriguez, C.; Walker-Thurmond, K.; Thun, M.J. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of US adults. N. Engl. J. Med. 2003, 348, 1625–1638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, C.N.; Cornish, A.J.; Kinnersley, B.; Law, P.J.; Claus, E.B.; Il’Yasova, D.; Schildkraut, J.; Barnholtz-Sloan, J.S.; Olson, S.H.; Bernstein, J.L. Lack of association between modifiable exposures and glioma risk: A Mendelian randomization analysis. Neuro-Oncol. 2020, 22, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Cote, D.J.; Downer, M.K.; Smith, T.R.; Smith-Warner, S.A.; Egan, K.M.; Stampfer, M.J. Height, waist circumference, body mass index, and body somatotype across the life course and risk of glioma. Cancer Causes Control. 2018, 29, 707–719. [Google Scholar] [CrossRef] [PubMed]
- Kabat, G.C.; Rohan, T.E. Adiposity at different periods of life and risk of adult glioma in a cohort of postmenopausal women. Cancer Epidemiol. 2018, 54, 71–74. [Google Scholar] [CrossRef]
- Wiedmann, M.K.; Brunborg, C.; Di Ieva, A.; Lindemann, K.; Johannesen, T.B.; Vatten, L.; Helseth, E.; Zwart, J.A. The impact of body mass index and height on the risk for glioblastoma and other glioma subgroups: A large prospective cohort study. Neuro-Oncol. 2017, 19, 976–985. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.; Chen, J.; Wang, J.; Gong, S.; Jin, H.; Sheng, P.; Qi, X.; Lv, L.; Dong, Y.; Hou, L. Body mass index and risk of brain tumors: A systematic review and dose–response meta-analysis. Eur. J. Clin. Nutr. 2016, 70, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Sergentanis, T.N.; Tsivgoulis, G.; Perlepe, C.; Ntanasis-Stathopoulos, I.; Tzanninis, I.-G.; Sergentanis, I.N.; Psaltopoulou, T. Obesity and risk for brain/CNS tumors, gliomas and meningiomas: A meta-analysis. PLoS ONE 2015, 10, e0136974. [Google Scholar] [CrossRef] [Green Version]
- Niedermaier, T.; Behrens, G.; Schmid, D.; Schlecht, I.; Fischer, B.; Leitzmann, M.F. Body mass index, physical activity, and risk of adult meningioma and glioma: A meta-analysis. Neurology 2015, 85, 1342–1350. [Google Scholar] [CrossRef] [PubMed]
- Kitahara, C.M.; Gamborg, M.; Rajaraman, P.; Sørensen, T.I.; Baker, J.L. A prospective study of height and body mass index in childhood, birth weight, and risk of adult glioma over 40 years of follow-up. Am. J. Epidemiol. 2014, 180, 821–829. [Google Scholar] [CrossRef] [Green Version]
- Wiedmann, M.; Brunborg, C.; Lindemann, K.; Johannesen, T.; Vatten, L.; Helseth, E.; Zwart, J. Body mass index and the risk of meningioma, glioma and schwannoma in a large prospective cohort study (The HUNT Study). Brit. J. Cancer 2013, 109, 289–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Little, R.B.; Madden, M.H.; Thompson, R.C.; Olson, J.J.; LaRocca, R.V.; Pan, E.; Browning, J.E.; Egan, K.M.; Nabors, L.B. Anthropometric factors in relation to risk of glioma. Cancer Causes Control. 2013, 24, 1025–1031. [Google Scholar] [CrossRef] [Green Version]
- Chambless, L.B.; Parker, S.L.; Hassam-Malani, L.; McGirt, M.J.; Thompson, R.C. Type 2 diabetes mellitus and obesity are independent risk factors for poor outcome in patients with high-grade glioma. Neuro-Oncol. 2012, 106, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Edlinger, M.; Strohmaier, S.; Jonsson, H.; Bjørge, T.; Manjer, J.; Borena, W.T.; Häggström, C.; Engeland, A.; Tretli, S.; Concin, H. Blood pressure and other metabolic syndrome factors and risk of brain tumour in the large population-based Me-Can cohort study. J. Hypertens. 2012, 30, 290–296. [Google Scholar] [CrossRef]
- Michaud, D.S.; Bové, G.; Gallo, V.; Schlehofer, B.; Tjønneland, A.; Olsen, A.; Overvad, K.; Dahm, C.C.; Teucher, B.; Boeing, H. Anthropometric measures, physical activity, and risk of glioma and meningioma in a large prospective cohort study. Cancer Prevent. Res. 2011, 4, 1385–1392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, S.C.; Rajaraman, P.; Dubrow, R.; Darefsky, A.S.; Koebnick, C.; Hollenbeck, A.; Schatzkin, A.; Leitzmann, M.F. Height, body mass index, and physical activity in relation to glioma risk. Cancer Res. 2009, 69, 8349–8355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benson, V.S.; Pirie, K.; Green, J.; Casabonne, D.; Beral, V. Lifestyle factors and primary glioma and meningioma tumours in the Million Women Study cohort. Brit. J. Cancer 2008, 99, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Almeida, J.; Costa, J.; Coelho, P.; Cea, V.; Galesio, M.; Noronha, J.; Diniz, M.; Prudêncio, C.; Soares, R.; Sala, C. Adipocyte proteome and secretome influence inflammatory and hormone pathways in glioma. Metabol. Brain Dis. 2019, 34, 141–152. [Google Scholar] [CrossRef]
- Furtner, J.; Genbrugge, E.; Gorlia, T.; Bendszus, M.; Nowosielski, M.; Golfinopoulos, V.; Weller, M.; Van Den Bent, M.J.; Wick, W.; Preusser, M. Temporal muscle thickness is an independent prognostic marker in patients with progressive glioblastoma: Translational imaging analysis of the EORTC 26101 trial. Neuro-Oncol. 2019, 21, 1587–1594. [Google Scholar] [CrossRef] [PubMed]
- Furtner, J.; Berghoff, A.S.; Schöpf, V.; Reumann, R.; Pascher, B.; Woitek, R.; Asenbaum, U.; Pelster, S.; Leitner, J.; Widhalm, G. Temporal muscle thickness is an independent prognostic marker in melanoma patients with newly diagnosed brain metastases. Neuro-Oncol. 2018, 140, 173–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Who, E.C. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157. [Google Scholar]
- Cho, J.H.; Shin, C.M.; Han, K.-D.; Yoon, H.; Park, Y.S.; Kim, N.; Lee, D.H. Abdominal obesity increases risk for esophageal cancer: A nationwide population-based cohort study of South Korea. J. Gastroenterol. 2020, 55, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-H.; Kim, S.M.; Han, K.-D.; Jung, J.-H.; Lee, S.-S.; Oh, S.W.; Park, H.S.; Rhee, E.-J.; Lee, W.-Y.; Yoo, S.J. Waist Circumference and All-Cause Mortality Independent of Body Mass Index in Korean Population from the National Health Insurance Health Checkup 2009–2015. J. Clin. Med. 2019, 8, 72. [Google Scholar] [CrossRef] [Green Version]
- Bardou, M.; Barkun, A.N.; Martel, M. Obesity and colorectal cancer. Gut 2013, 62, 933–947. [Google Scholar] [CrossRef]
- Allott, E.H.; Masko, E.M.; Freedland, S.J. Obesity and prostate cancer: Weighing the evidence. Eur. Urol. 2013, 63, 800–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raglan, O.; Kalliala, I.; Markozannes, G.; Cividini, S.; Gunter, M.J.; Nautiyal, J.; Gabra, H.; Paraskevaidis, E.; Martin-Hirsch, P.; Tsilidis, K.K. Risk factors for endometrial cancer: An umbrella review of the literature. Int. J. Cancer 2019, 145, 1719–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iyengar, N.M.; Gucalp, A.; Dannenberg, A.J.; Hudis, C.A. Obesity and cancer mechanisms: Tumor microenvironment and inflammation. J. Clin. Oncol. 2016, 34, 4270. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, B.D.; Goncalves, M.D.; Cantley, L.C. Obesity and cancer mechanisms: Cancer metabolism. J. Clin. Oncol. 2016, 34, 4277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avgerinos, K.I.; Spyrou, N.; Mantzoros, C.S.; Dalamaga, M. Obesity and cancer risk: Emerging biological mechanisms and perspectives. Metabolism 2019, 92, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Doyle, S.L.; Donohoe, C.L.; Finn, S.P.; Howard, J.M.; Lithander, F.E.; Reynolds, J.V.; Pidgeon, G.P.; Lysaght, J. IGF-1 and its receptor in esophageal cancer: Association with adenocarcinoma and visceral obesity. Am. J. Gastroenterol. 2012, 107, 196–204. [Google Scholar] [CrossRef]
- Karnati, H.K.; Panigrahi, M.K.; Li, Y.; Tweedie, D.; Greig, N.H. Adiponectin as a potential therapeutic target for prostate cancer. Curr. Pharmaceut. Des. 2017, 23, 4170–4179. [Google Scholar] [CrossRef] [Green Version]
- Deng, T.; Lyon, C.J.; Bergin, S.; Caligiuri, M.A.; Hsueh, W.A. Obesity, inflammation, and cancer. Ann. Rev. Pathol. Mech. Dis. 2016, 11, 421–449. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.M.M.; White, A.J.; Nichols, H.B.; O’Brien, K.M.; Weinberg, C.R.; Sandler, D.P. The association between metabolic health, obesity phenotype and the risk of breast cancer. Int. J. Cancer 2017, 140, 2657–2666. [Google Scholar] [CrossRef] [Green Version]
- Amin, F.; Fatima, S.S.; Islam, N.; Gilani, A.H. Prevalence of obesity and overweight, its clinical markers and associated factors in a high risk South-Asian population. BMC Obes. 2015, 2, 16. [Google Scholar] [CrossRef] [Green Version]
- Potharaju, M.; Mangaleswaran, B.; Mathavan, A.; John, R.; Thamburaj, V.; Ghosh, S.; Ganesh, S.; Kalvakonda, C.; Loganathan, M.; Bapu, S. Body mass index as a prognostic marker in Glioblastoma Multiforme: A clinical outcome. Int. J. Rad. Oncol. Biol. Phys. 2018, 102, 204–209. [Google Scholar] [CrossRef]
- Ahn, S.; Han, K.-D.; Park, Y.-M.; Bae, J.M.; Kim, S.U.; Jeun, S.-S.; Yang, S.H. Cigarette smoking is associated with increased risk of malignant gliomas: A nationwide population-based cohort study. Cancers 2020, 12, 1343. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.B.; Lee, K.M.; Lee, J.M.; Ko, S.H.; Han, K.D.; Park, Y.G. Waist circumference, body mass index, and colorectal cancer risk according to diabetes status: A Korean nationwide population-based cohort study. J. Gastroenterol. Hepatol. 2021, 36, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Seo, M.H.; Lee, W.-Y.; Kim, S.S.; Kang, J.-H.; Kang, J.-H.; Kim, K.K.; Kim, B.-Y.; Kim, Y.-H.; Kim, W.-J.; Kim, E.M. 2018 Korean Society for the Study of Obesity guideline for the management of obesity in Korea. J. Obes. Metabol. Syndrom. 2019, 28, 40. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n (%) | Healthy Individuals | Glioma Patients | p Value |
|---|---|---|---|
| n = 6,829,273 | n = 4471 | ||
| Mean age, years a | 46.84 ± 13.53 | 56.65 ± 13.01 | <0.001 |
| Male | 3,923,066 (57.44) | 2553 (57.1) | 0.642 |
| Height, cm a | 164.35 ± 9.21 | 162.46 ± 9.14 | <0.001 |
| Weight, kg a | 64.42 ± 11.53 | 63.81 ± 10.93 | 0.004 |
| Waist circumference, cm a | 80.4 ± 9.3 | 82.5 ± 8.4 | <0.001 |
| <80 b/<75 c | 2,471,470 (36.19) | 1193 (26.68) | |
| 80–84.9 b/75–79.9 c | 1,667,249 (24.41) | 1024 (22.90) | |
| 85–89.9 b/80–84.9 c | 1,378,370 (20.18) | 1036 (23.17) | |
| 90–94.9 b/85–89.9 c | 790,962 (11.58) | 679 (15.19) | |
| 95–99.9 b/90–94.9 c | 342,326 (5.01) | 349 (7.81) | |
| ≥100 b/≥95 c | 178,896 (2.62) | 190 (4.25) | |
| BMI, kg/m a | 23.76 ± 3.48 | 24.1 ± 3.14 | <0.001 |
| <18.5 | 223,786 (3.28) | 99 (2.21) | |
| 18.5–22.9 | 2,622,565 (38.4) | 1554 (34.76) | |
| 23.0–24.9 | 1,729,528 (25.33) | 1154 (25.81) | |
| 25.0–29.9 | 2,022,217 (29.61) | 1483 (33.17) | |
| ≥30.0 | 231,177 (3.39) | 181 (4.05) | |
| Smoker | 0.003 | ||
| None | 3,978,206 (58.25) | 2659 (59.47) | |
| Former | 1,053,665 (15.43) | 731 (16.35) | |
| Current | 1,797,402 (26.32) | 1081 (24.18) | |
| Drinker | <0.001 | ||
| None | 3,412,478 (49.97) | 2631 (58.85) | |
| Mild | 2,874,998 (42.1) | 1502 (33.59) | |
| Heavy | 541,797 (7.93) | 338 (7.56) | |
| Regular exercise | 1,282,475 (18.78) | 895 (20.02) | 0.034 |
| Diabetes mellitus | 558,664 (8.18) | 611 (13.67) | <0.001 |
| Hypertension | 959,082 (14.04) | 912 (20.4) | <0.001 |
| Systolic BP a | 122.4 ± 14.7 | 125.51 ± 15.3 | |
| Diastolic BP a | 76.4 ± 9.9 | 77.4 ± 9.9 | |
| Dyslipidemia | 1,233,872 (18.07) | 1095 (24.49) | <0.001 |
| Total cholesterol | 195.6 ± 40.7 | 197.7 ± 43.1 |
| Total, n | Glioma Events, n | Person-Years | Incidence Rates * | Crude (95% CI) | Model 1 HR † (95% CI) | Model 2 HR ‡ (95% CI) | |
|---|---|---|---|---|---|---|---|
| BMI (kg/m2) | |||||||
| <25.0 | 4,578,686 | 2807 | 33,403,700 | 8.40 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≥25.0 | 2,255,058 | 1664 | 16,474,282 | 10.10 | 1.20 (1.13–1.28) | 1.08 (1.02–1.15) | 1.08 (1.02–1.15) |
| BMI (kg/m2) | |||||||
| <18.5 | 223,885 | 99 | 1,616,699 | 6.12 | 0.76 (0.62–0.93) | 0.93(0.76–1.14) | 0.915(0.75,1.12) |
| 18.5–22.9 | 2,624,119 | 1554 | 19,139,370 | 8.12 | 1 (reference) | 1 (reference) | 1 (reference) |
| 23.0–24.9 | 1,730,682 | 1154 | 12,647,631 | 9.12 | 1.12 (1.04–1.21) | 0.97 (0.90–1.05) | 0.97 (0.90–1.05) |
| 25.0–29.9 | 2,023,700 | 1483 | 14,786,709 | 10.03 | 1.24 (1.15–1.33) | 1.04 (0.97–1.12) | 1.04 (0.97–1.12) |
| ≥30.0 | 231,358 | 181 | 1,687,572 | 10.73 | 1.32 (1.13–1.54) | 1.29 (1.10–1.50) | 1.27 (1.09–1.48) |
| WC (cm) | |||||||
| <90 a/85 b | 5,520,342 | 3253 | 40,319,911 | 8.07 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≥90 a/85 b | 1,313,402 | 1218 | 9,558,071 | 12.74 | 1.58 (1.48–1.69) | 1.17 (1.09–1.25) | 1.16 (1.09–1.24) |
| WC (cm) | |||||||
| <80 a/<75 b | 2,472,663 | 1193 | 18,068,195 | 6.60 | 0.64 (0.59–0.70) | 0.95 (0.87–1.03) | 0.95 (0.87–1.03) |
| 80–84.9 a/75–79.9 b | 1,668,273 | 1024 | 12,185,415 | 8.40 | 0.82 (0.75–0.89) | 0.93 (0.85–1.01) | 0.93 (0.85–1.01) |
| 85–89.9 a/80–84.9 b | 1,379,406 | 1036 | 10,066,300 | 10.23 | 1 (reference) | 1 (reference) | 1 (reference) |
| 90–94.9 a/85–89.9 b | 791,641 | 679 | 5,766,604 | 11.78 | 1.14 (1.04–1.26) | 1.05 (0.96–1.16) | 1.05 (0.95–1.16) |
| 95–99.9 a/90–94.9 b | 342,675 | 349 | 2,492,630 | 14.00 | 1.36 (1.20–1.54) | 1.19 (1.05–1.34) | 1.18 (1.05–1.34) |
| ≥100 a/≥95 b | 179,086 | 190 | 1,298,836 | 14.63 | 1.42 (1.22–1.66) | 1.27 (1.09–1.49) | 1.25 (1.07–1.46) |
| BMI (kg/m2) | WC (cm) | Total, n | Glioma Events, n | Person-Years | Incidence Rates * | Crude (95% CI) | Model 1 HR † (95% CI) | Model 2 HR ‡ (95% CI) | |
|---|---|---|---|---|---|---|---|---|---|
| Total | |||||||||
| <25.0 | <90 a/85 b | 4,374,943 | 2588 | 31,934,209 | 8.10 | 1 (reference) | 1 (reference) | 1 (reference) | |
| ≥90 a/85 b | 203,743 | 219 | 1,469,491 | 14.90 | 1.84 (1.60–2.11) | 1.06 (0.92–1.22) | 1.06 (0.92–1.21) | ||
| ≥25.0 | <90 a/85 b | 1,145,399 | 665 | 8,385,701 | 7.93 | 0.98 (0.89–1.07) | 0.97 (0.89–1.05) | 0.97 (0.89–1.06) | |
| ≥90 a/85 b | 1,109,659 | 999 | 8,088,580 | 12.35 | 1.52 (1.42–1.64) | 1.18 (1.10–1.27) | 1.18 (1.09–1.27) | ||
| Males | |||||||||
| <25.0 | <90 a/85 b | 2,353,787 | 1480 | 17,108,111 | 8.65 | 1 (reference) | 1 (reference) | 1 (reference) | |
| ≥90 a/85 b | 107,077 | 110 | 764,599 | 14.39 | 1.66 (1.37–2.02) | 0.99 (0.81–1.20) | 0.98 (0.81–1.20) | ||
| ≥25.0 | <90 a/85 b | 758,916 | 402 | 5,543,757 | 7.25 | 0.84 (0.75–0.94) | 0.97 (0.87–1.08) | 0.99 (0.88–1.10) | |
| ≥90 a/85 b | 705,839 | 561 | 5,124,786 | 10.94 | 1.27 (1.15–1.40) | 1.16 (1.05–1.28) | 1.17 (1.06–1.29) | ||
| Females | |||||||||
| <25.0 | <90 a/85 b | 2,021,156 | 1108 | 14,826,098 | 7.47 | 1 (reference) | 1 (reference) | 1 (reference) | |
| ≥90 a/85 b | 96,666 | 109 | 704,891 | 15.47 | 2.07 (1.70–2.52) | 1.20 (0.98–1.47) | 1.20 (0.98–1.46) | ||
| ≥25.0 | <90 a/85 b | 386,483 | 263 | 2,841,943 | 9.25 | 1.24 (1.08–1.42) | 1.02 (0.89–1.16) | 1.01 (0.88–1.16) | |
| ≥90 a/85 b | 403,820 | 438 | 2,963,794 | 14.78 | 1.98 (1.77–2.21) | 1.29 (1.15-1.45) | 1.28 (1.14–1.43) |
| Total, n | Glioma Events, n | Person-Years | Incidence Rates * | Crude (95% CI) | Model 1 HR † (95% CI) | Model 2 HR ‡ (95% CI) | |
|---|---|---|---|---|---|---|---|
| BMI (kg/m2) | |||||||
| <25.0 | 2,460,864 | 1590 | 17,872,711 | 8.90 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≥25.0 | 1,464,755 | 963 | 10,668,544 | 9.03 | 1.02 (0.94–1.10) | 1.07 (0.99–1.16) | 1.09 (1.00–1.18) |
| BMI (kg/m2) | |||||||
| <18.5 | 77,240 | 51 | 546,617 | 9.33 | 1.02 (0.77–1.35) | 0.92 (0.69–1.22) | 0.89 (0.67–1.18) |
| 18.5–22.9 | 1,304,404 | 872 | 9,464,095 | 9.21 | 1 (reference) | 1 (reference) | 1 (reference) |
| 23.0–24.9 | 1,079,220 | 667 | 7,861,998 | 8.48 | 0.92 (0.83–1.02) | 0.90 (0.814, 0.996) | 0.92 (0.83–1.02) |
| 25.0–29.9 | 1,327,881 | 879 | 9,673,680 | 9.09 | 0.99 (0.90–1.08) | 1.00 (0.91–1.10) | 1.03 (0.93–1.13) |
| ≥30.0 | 136,874 | 84 | 994,863 | 8.44 | 0.92 (0.73–1.15) | 1.23 (0.99–1.54) | 1.24 (0.99–1.56) |
| WC (cm) | |||||||
| <90 | 3,112,703 | 1882 | 22,651,869 | 8.31 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≥90 | 812,916 | 671 | 5,889,385 | 11.39 | 1.37 (1.26–1.50) | 1.13 (1.04–1.24) | 1.14 (1.04–1.24) |
| WC (cm) | |||||||
| <80 | 1,153,492 | 611 | 8,393,298 | 7.28 | 0.74 (0.66–0.82) | 0.93 (0.83–1.04) | 0.91 (0.82–1.02) |
| 80–84.9 | 1,071,622 | 632 | 7,804,377 | 8.10 | 0.82 (0.73–0.91) | 0.90 (0.81–1.01) | 0.90 (0.80–1.01) |
| 85–89.9 | 887,589 | 639 | 6,454,193 | 9.90 | 1 (reference) | 1 (reference) | 1 (reference) |
| 90-94.9 | 510,969 | 395 | 3,706,459 | 10.66 | 1.07 (0.95–1.22) | 1.00 (0.88–1.13) | 1.00 (0.88–1.13) |
| 95–99.9 | 204,118 | 184 | 1,477,318 | 12.46 | 1.26 (1.07–1.48) | 1.15 (0.97–1.35) | 1.14 (0.97–1.35) |
| ≥100 | 97,829 | 92 | 705,608 | 13.04 | 1.32 (1.06–1.64) | 1.29 (1.04–1.60) | 1.27 (1.02–1.59) |
| Total, n | Glioma Events, n | Person-Years | Incidence Rates * | Crude (95% CI) | Model 1 HR † (95% CI) | Model 2 HR ‡ (95% CI) | |
|---|---|---|---|---|---|---|---|
| BMI (kg/m2) | |||||||
| <25.0 | 2,117,822 | 1217 | 15,530,989 | 7.84 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≥25.0 | 790,303 | 701 | 5,805,738 | 12.07 | 1.54 (1.40–1.69) | 1.15 (1.04–1.26) | 1.14 (1.03–1.25) |
| BMI (kg/m2) | |||||||
| <18.5 | 146,645 | 48 | 1,070,081 | 4.49 | 0.64 (0.48–0.85) | 0.90 (0.67–1.20) | 0.90 (0.67–1.20) |
| 18.5–22.9 | 1,319,715 | 682 | 9,675,274 | 7.05 | 1 (reference) | 1 (reference) | 1 (reference) |
| 23.0–24.9 | 651,462 | 487 | 4,785,632 | 10.18 | 1.44 (1.29–1.62) | 1.11 (0.98–1.24) | 1.10 (0.98–1.24) |
| 25.0–29.9 | 695,819 | 604 | 5,113,028 | 11.81 | 1.68 (1.50–1.87) | 1.16 (1.03–1.29) | 1.15 (1.03–1.28) |
| ≥30.0 | 94,484 | 97 | 692,709 | 14.00 | 1.99 (1.60–2.46) | 1.45 (1.17–1.80) | 1.42 (1.15–1.76) |
| WC (cm) | |||||||
| <85 | 2,407,639 | 1371 | 17,668,041 | 7.76 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≥85 | 500,486 | 547 | 3,668,685 | 14.91 | 1.92 (1.74–2.12) | 1.27 (1.14–1.41) | 1.26 (1.13–1.39) |
| WC (cm) | |||||||
| <75 | 1,319,171 | 582 | 9,674,896 | 6.02 | 0.54 (0.48–0.62) | 0.91 (0.80–1.04) | 0.92 (0.80–1.05) |
| 75–79.9 | 596,651 | 392 | 4,381,038 | 8.95 | 0.81 (0.71–0.94) | 0.95 (0.83–1.10) | 0.96 (0.83–1.10) |
| 80–84.9 | 491,817 | 397 | 3,612,106 | 11.00 | 1 (reference) | 1 (reference) | 1 (reference) |
| 85–89.9 | 280,672 | 284 | 2,060,145 | 13.76 | 1.26 (1.08–1.46) | 1.15 (0.98–1.34) | 1.14 (0.98–1.33) |
| 90–94.9 | 138,557 | 165 | 1,015,312 | 16.25 | 1.48 (1.23–1.77) | 1.27 (1.06–1.53) | 1.27 (1.06–1.52) |
| ≥95 | 81,257 | 98 | 593,228 | 16.52 | 1.50 (1.21–1.88) | 1.31 (1.05–1.63) | 1.29 (1.04–1.62) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahn, S.; Han, K.; Lee, J.-E.; Jeun, S.-S.; Park, Y.-M.; Yang, S.H. Associations of General and Abdominal Obesity with the Risk of Glioma Development. Cancers 2021, 13, 2859. https://doi.org/10.3390/cancers13122859
Ahn S, Han K, Lee J-E, Jeun S-S, Park Y-M, Yang SH. Associations of General and Abdominal Obesity with the Risk of Glioma Development. Cancers. 2021; 13(12):2859. https://doi.org/10.3390/cancers13122859
Chicago/Turabian StyleAhn, Stephen, Kyungdo Han, Jung-Eun Lee, Sin-Soo Jeun, Yong-Moon Park, and Seung Ho Yang. 2021. "Associations of General and Abdominal Obesity with the Risk of Glioma Development" Cancers 13, no. 12: 2859. https://doi.org/10.3390/cancers13122859