C-Reactive Protein (CRP) Levels in Immune Checkpoint Inhibitor Response and Progression in Advanced Non-Small Cell Lung Cancer: A Bi-Center Study

 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Concept
2.2. Study Design—Graz Cohort (Discovery Cohort)
2.3. External Validation Cohort
2.4. Laboratory Analysis Graz
2.5. Laboratory Analysis Nuremberg
2.6. Statistical Methods
3. Results
3.1. Analysis at Baseline and Crude Outcome Rates (Graz Cohort)
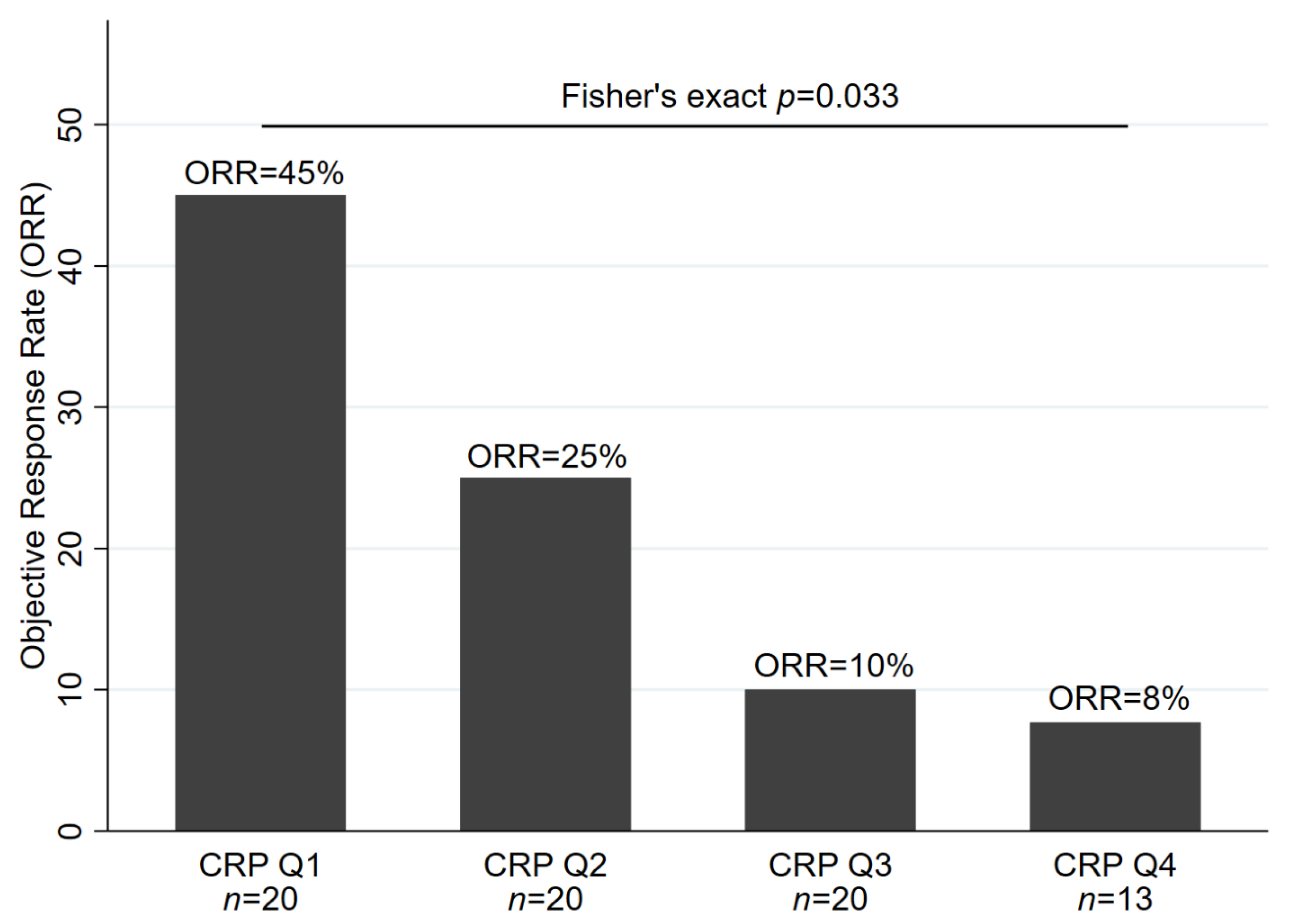
3.2. Elevated Baseline CRP Predicts Poor Response to ICI Therapy (Graz Cohort)
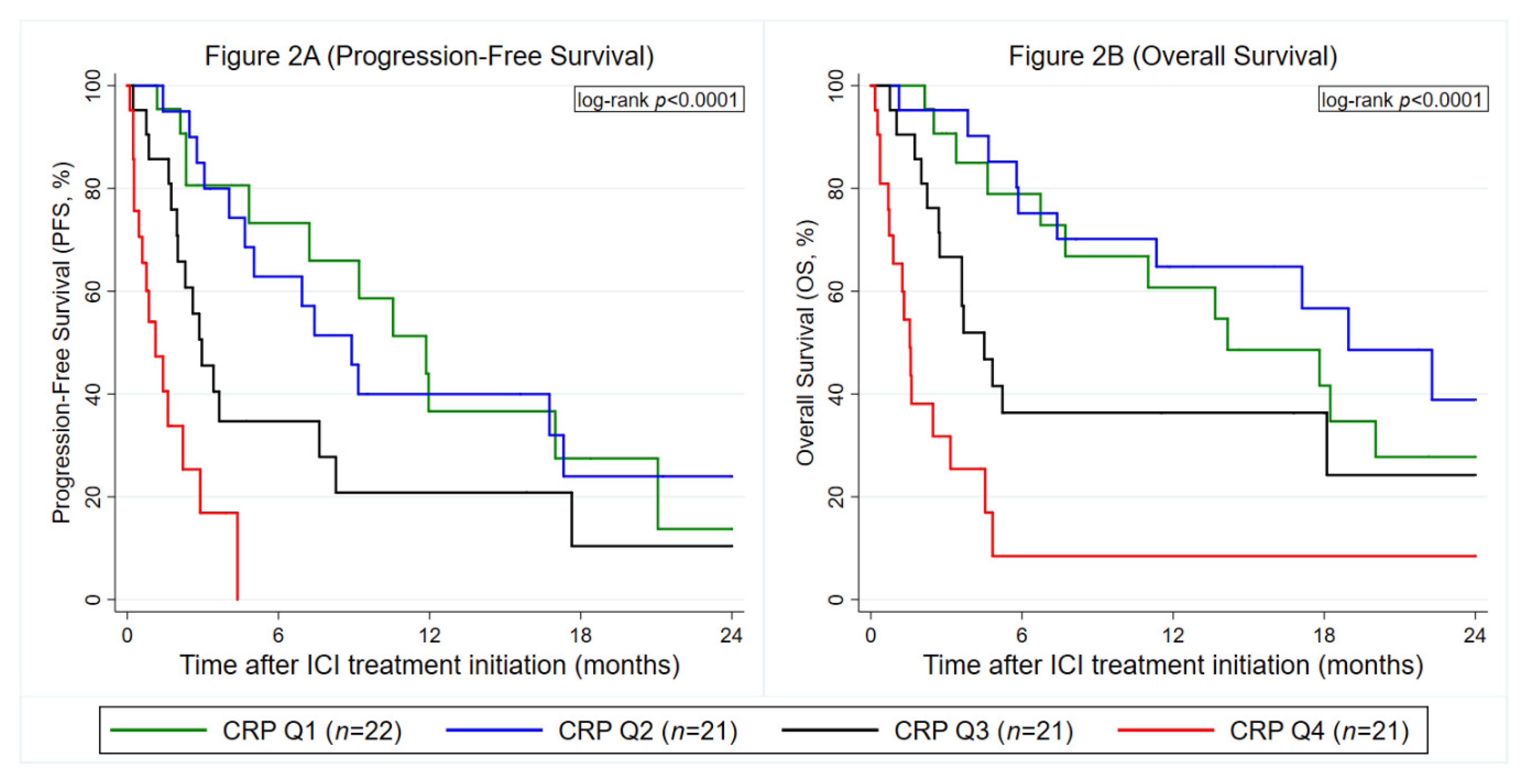
3.3. Elevated Baseline CRP Predicts Disease Progression and Death (Graz Cohort)
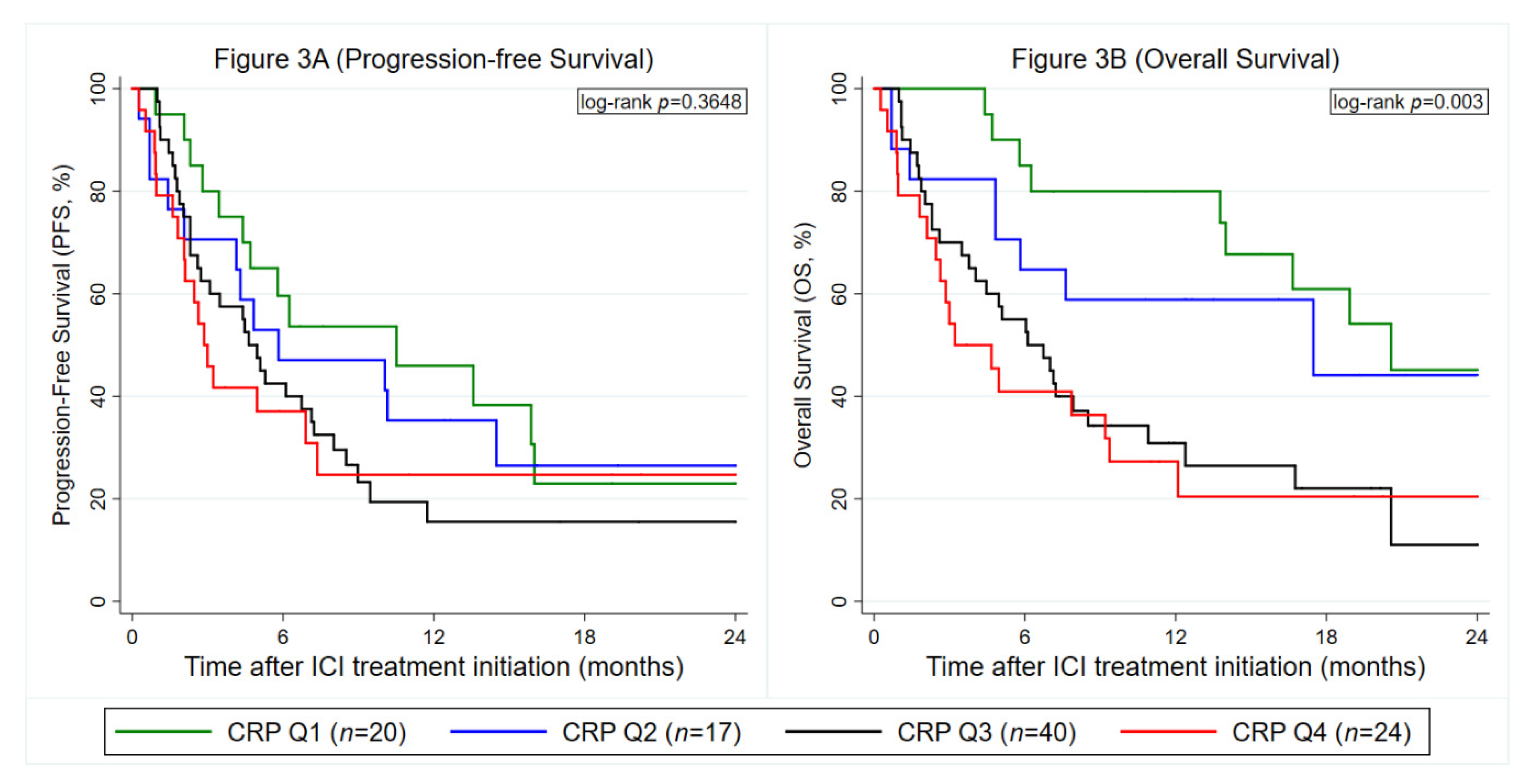
3.4. Baseline CRP is Confirmed as a Predictor of Adverse Progression and Mortality Outcomes But Not Anti PD-(L)1 Treatment Response in External Validation (Nuremberg Cohort)
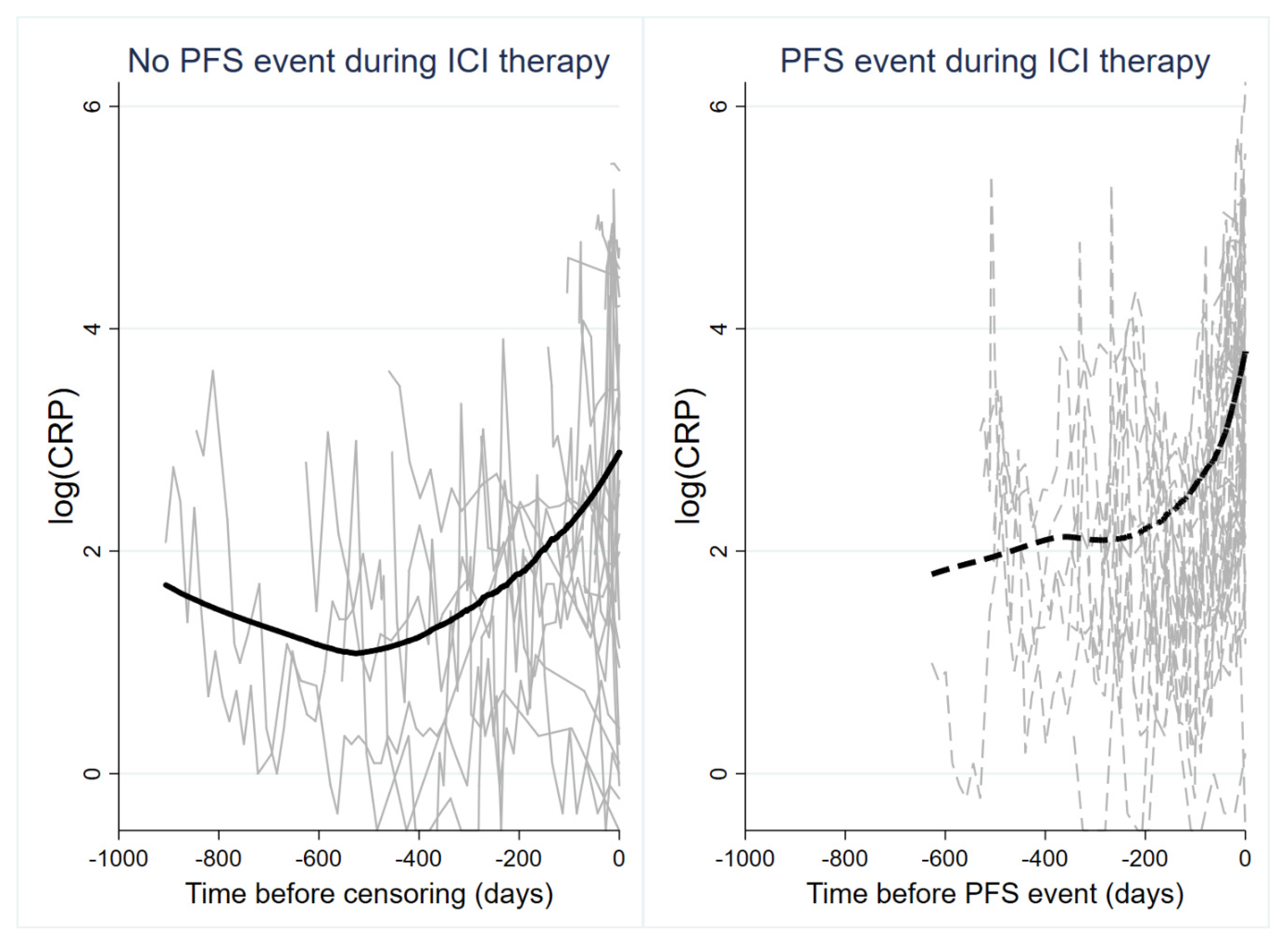
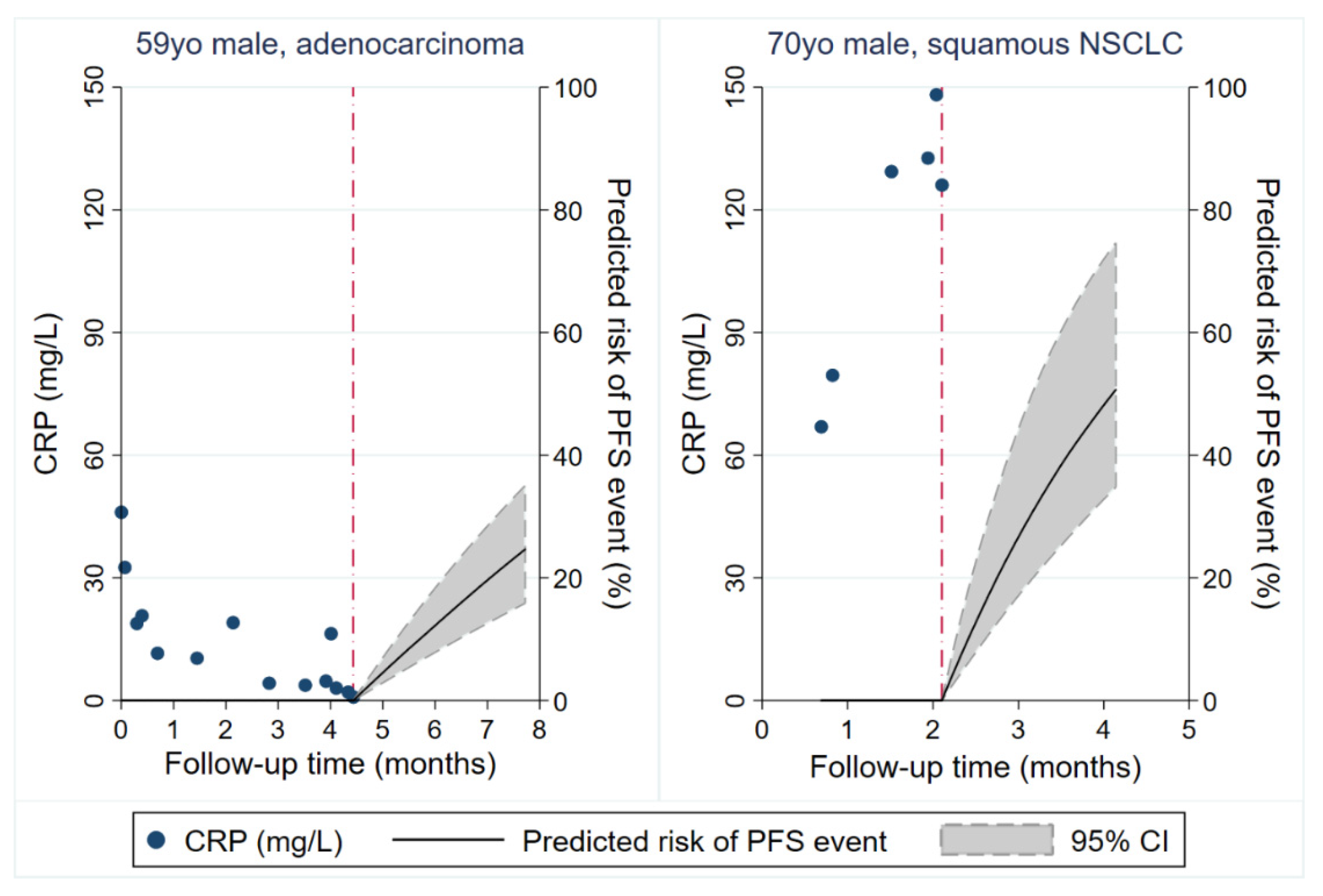
3.5. Analysis of Longitudinal CRP Trajectories During Anti PD-(L)1 Therapy and progression (Graz Cohort)
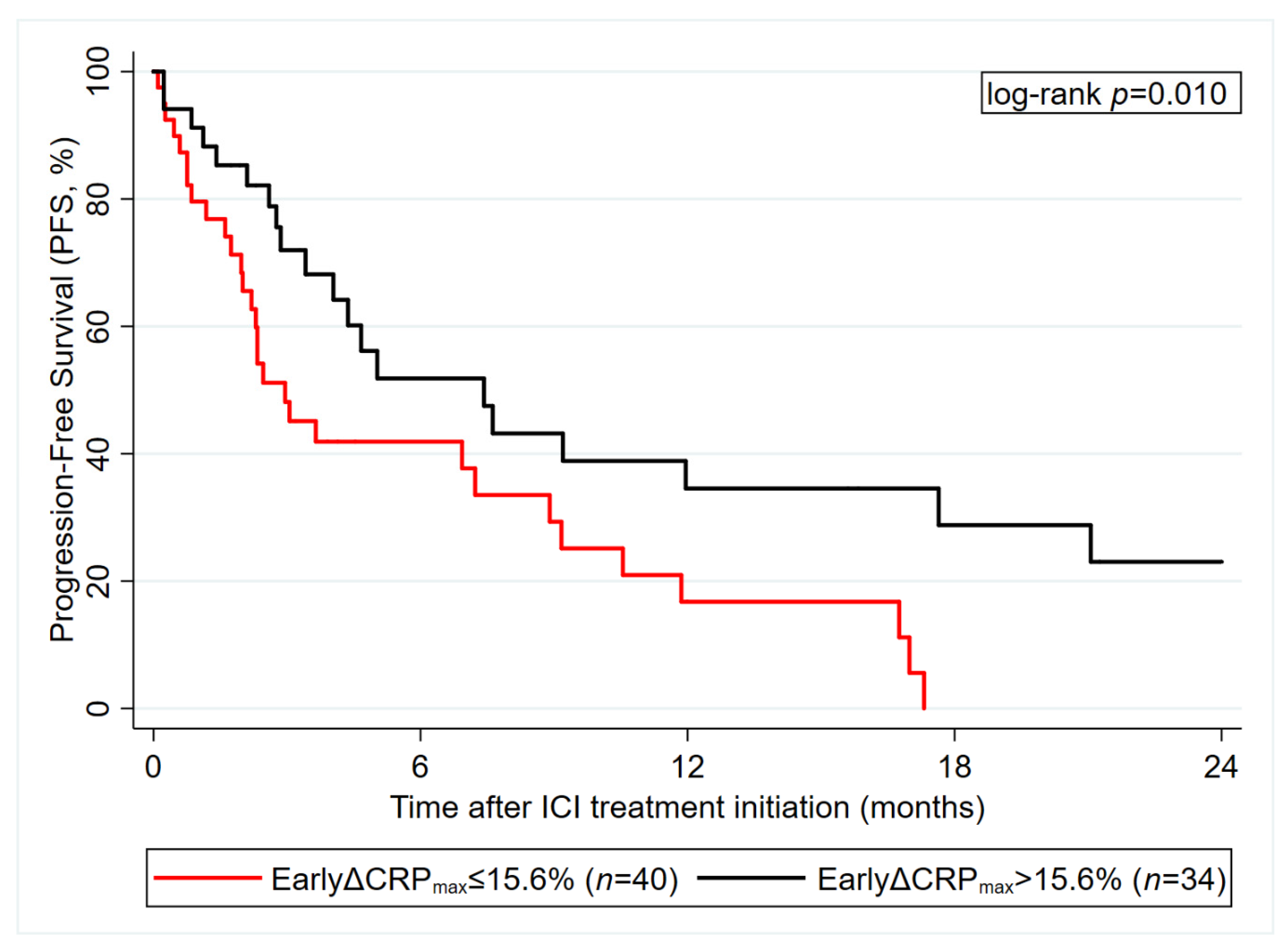
3.6. Early CRP Decline after ICI Initiation Predicts ICI Therapy PFS (Graz Cohort)
4. Discussion
4.1. Pretreatment CRP Levels
4.2. CRP Trajectories
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CRP | C-reactive protein |
| NSCLC | non-small cell lung cancer |
| ICI | immune checkpoint inhibitor(s) |
| PD-(L)1 | programmed death (ligand) 1 |
| PFS | progression-free survival |
| OS | overall survival |
| ORR | objective response rate |
| HR | hazard ratio |
| OR | odds ratio |
| CI | confidence interval |
| NGS | next-generation sequencing |
| (ir)RECIST | (immune-related) response evaluation criteria in solid tumors |
| PD | progressive disease |
| SD | stable disease |
| PR | partial remission |
| CR | complete remission |
| CTLA4 | cytotoxic T-lymphocyte-associated protein 4 |
| ECOG | Eastern cooperation oncology group performance status |
| BMI | body mass index |
| RTX | radiotherapy |
| CTX | chemotherapy |
| RCTX | radiochemotherapy |
| Q | quartile |
| Ref. | reference |
| EGFR | epidermal growth factor receptor |
| EML4–ALK | echinoderm microtubule associated protein-like 4 anaplastic lymphoma kinase |
| ROS1 | ROS proto-oncogene 1 |
| BRAF | v-Raf murine sarcoma viral oncogene homolog B |
References
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crinò, L.; Eberhardt, W.E.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herbst, R.S.; Baas, P.; Kim, D.-W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.-Y.; Molina, J.; Kim, J.-H.; Arvis, C.D.; Ahn, M.-J.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.M.; Hida, T.; Kowalski, D.M.; Dols, M.C.; et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): A phase 3, open-label, multicentre randomised controlled trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodriguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Çay Şenler, F.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fulop, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Updated Analysis of KEYNOTE-024: Pembrolizumab Versus Platinum-Based Chemotherapy for Advanced Non-Small-Cell Lung Cancer With PD-L1 Tumor Proportion Score of 50% or Greater. J. Clin. Oncol. 2019, 37, 537–546. [Google Scholar] [CrossRef]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodriguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef]
- Hellmann, M.D.; Paz-Ares, L.; Bernabe Caro, R.; Zurawski, B.; Kim, S.-W.; Carcereny Costa, E.; Park, K.; Alexandru, A.; Lupinacci, L.; de la Mora Jimenez, E.; et al. Nivolumab plus Ipilimumab in Advanced Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2019, 381, 2020–2031. [Google Scholar] [CrossRef]
- Mok, T.S.K.; Wu, Y.-L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Havel, J.J.; Chowell, D.; Chan, T.A. The evolving landscape of biomarkers for checkpoint inhibitor immunotherapy. Nat. Rev. Cancer 2019, 19, 133–150. [Google Scholar] [CrossRef] [PubMed]
- Scheel, A.H.; Dietel, M.; Heukamp, L.C.; Johrens, K.; Kirchner, T.; Reu, S.; Ruschoff, J.; Schildhaus, H.U.; Schirmacher, P.; Tiemann, M.; et al. Harmonized PD-L1 immunohistochemistry for pulmonary squamous-cell and adenocarcinomas. Mod. Pathol. 2016, 29, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Forrest, L.M.; McMillan, D.C.; McArdle, C.S.; Angerson, W.J.; Dunlop, D.J. Evaluation of cumulative prognostic scores based on the systemic inflammatory response in patients with inoperable non-small-cell lung cancer. Br. J. Cancer 2003, 89, 1028–1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riedl, J.M.; Posch, F.; Moik, F.; Bezan, A.; Szkandera, J.; Smolle, M.A.; Kasparek, A.-K.; Pichler, M.; Stöger, H.; Stotz, M.; et al. Inflammatory biomarkers in metastatic colorectal cancer: Prognostic and predictive role beyond the first line setting. Oncotarget 2017, 8, 96048–96061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilop, S.; Crysandt, M.; Bendel, M.; Mahnken, A.H.; Osieka, R.; Jost, E. Correlation of C-Reactive Protein with Survival and Radiographic Response to First-Line Platinum-Based Chemotherapy in Advanced Non-Small Cell Lung Cancer. Oncol. Res. Treat. 2008, 31, 665–670. [Google Scholar] [CrossRef]
- Lindenmann, J.; Fink-Neuboeck, N.; Taucher, V.; Pichler, M.; Posch, F.; Brcic, L.; Smolle, E.; Koter, S.; Smolle, J.; Smolle-Juettner, F.M. Prediction of Postoperative Clinical Outcomes in Resected Stage I Non-Small Cell Lung Cancer Focusing on the Preoperative Glasgow Prognostic Score. Cancers 2020, 12, 152. [Google Scholar] [CrossRef] [Green Version]
- Diakos, C.I.; Charles, K.A.; McMillan, D.C.; Clarke, S.J. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014, 15, e493–e503. [Google Scholar] [CrossRef]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef]
- Baracos, V.E.; Martin, L.; Korc, M.; Guttridge, D.C.; Fearon, K.C.H. Cancer-associated cachexia. Nat. Rev. Dis. Primers 2018, 4, 17105. [Google Scholar] [CrossRef]
- Bye, A.; Wesseltoft-Rao, N.; Iversen, P.O.; Skjegstad, G.; Holven, K.B.; Ulven, S.; Hjermstad, M.J. Alterations in inflammatory biomarkers and energy intake in cancer cachexia: A prospective study in patients with inoperable pancreatic cancer. Med. Oncol. 2016, 33, 54. [Google Scholar] [CrossRef]
- Fearon, K.C.; Glass, D.J.; Guttridge, D.C. Cancer cachexia: Mediators, signaling, and metabolic pathways. Cell Metab. 2012, 16, 153–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurzrock, R. The role of cytokines in cancer-related fatigue. Cancer 2001, 92, 1684–1688. [Google Scholar] [CrossRef]
- Mahmoud, F.A.; Rivera, N.I. The role of C-reactive protein as a prognostic indicator in advanced cancer. Curr. Oncol. Rep. 2002, 4, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Proctor, M.J.; Morrison, D.S.; Talwar, D.; Balmer, S.M.; O’Reilly, D.S.; Foulis, A.K.; Horgan, P.G.; McMillan, D.C. An inflammation-based prognostic score (mGPS) predicts cancer survival independent of tumour site: A Glasgow Inflammation Outcome Study. Br. J. Cancer 2011, 104, 726–734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, D.; Mahmoud, F.; Barna, B. Assessment of nutritional status and prognosis in advanced cancer: Interleukin-6, C-reactive protein, and the prognostic and inflammatory nutritional index. Support. Care Cancer 2003, 11, 60–62. [Google Scholar] [CrossRef]
- Tumeh, P.C.; Harview, C.L.; Yearley, J.H.; Shintaku, I.P.; Taylor, E.J.; Robert, L.; Chmielowski, B.; Spasic, M.; Henry, G.; Ciobanu, V.; et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 2014, 515, 568–571. [Google Scholar] [CrossRef]
- Iivanainen, S.; Ahvonen, J.; Knuuttila, A.; Tiainen, S.; Koivunen, J.P. Elevated CRP levels indicate poor progression-free and overall survival on cancer patients treated with PD-1 inhibitors. Esmo. Open 2019, 4, e000531. [Google Scholar] [CrossRef] [Green Version]
- Naqash, A.R.; Stroud, C.R.G.; Butt, M.U.; Dy, G.K.; Hegde, A.; Muzaffar, M.; Yang, L.V.; Hafiz, M.; Cherry, C.R.; Walker, P.R. Co-relation of overall survival with peripheral blood-based inflammatory biomarkers in advanced stage non-small cell lung cancer treated with anti-programmed cell death-1 therapy: Results from a single institutional database. Acta Oncol. 2018, 57, 867–872. [Google Scholar] [CrossRef] [Green Version]
- Oya, Y.; Yoshida, T.; Kuroda, H.; Mikubo, M.; Kondo, C.; Shimizu, J.; Horio, Y.; Sakao, Y.; Hida, T.; Yatabe, Y. Predictive clinical parameters for the response of nivolumab in pretreated advanced non-small-cell lung cancer. Oncotarget 2017, 8, 103117–103128. [Google Scholar] [CrossRef] [Green Version]
- Burrell, R.A.; McGranahan, N.; Bartek, J.; Swanton, C. The causes and consequences of genetic heterogeneity in cancer evolution. Nature 2013, 501, 338–345. [Google Scholar] [CrossRef]
- Ibrahim, J.G.; Chu, H.; Chen, L.M. Basic concepts and methods for joint models of longitudinal and survival data. J. Clin. Oncol. 2010, 28, 2796–2801. [Google Scholar] [CrossRef] [PubMed]
- Posch, F.; Leitner, L.; Bergovec, M.; Bezan, A.; Stotz, M.; Gerger, A.; Pichler, M.; Stoger, H.; Liegl-Atzwanger, B.; Leithner, A.; et al. Can Multistate Modeling of Local Recurrence, Distant Metastasis, and Death Improve the Prediction of Outcome in Patients With Soft Tissue Sarcomas? Clin. Orthop. Relat. Res. 2017, 475, 1427–1435. [Google Scholar] [CrossRef] [Green Version]
- Posch, F.; Silina, K.; Leibl, S.; Mundlein, A.; Moch, H.; Siebenhuner, A.; Samaras, P.; Riedl, J.; Stotz, M.; Szkandera, J.; et al. Maturation of tertiary lymphoid structures and recurrence of stage II and III colorectal cancer. Oncoimmunology 2018, 7, e1378844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schemper, M.; Smith, T.L. A note on quantifying follow-up in studies of failure time. Control. Clin. Trials 1996, 17, 343–346. [Google Scholar] [CrossRef]
- Crowther, M.J.; Abrams, K.R.; Lambert, P.C. Flexible parametric joint modelling of longitudinal and survival data. Stat. Med. 2012, 31, 4456–4471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krajsova, I.; Arenberger, P.; Lakomy, R.; Kubala, E.; Brezinova, I.; Poprach, A.; Stastny, M.; Muzik, J.; Melichar, B. Long-term Survival with Ipilimumab: Experience from a National Expanded Access Program for Patients with Melanoma. Anticancer Res. 2015, 35, 6303–6310. [Google Scholar]
- Simeone, E.; Gentilcore, G.; Giannarelli, D.; Grimaldi, A.M.; Caracò, C.; Curvietto, M.; Esposito, A.; Paone, M.; Palla, M.; Cavalcanti, E.; et al. Immunological and biological changes during ipilimumab treatment and their potential correlation with clinical response and survival in patients with advanced melanoma. Cancer Immunol. Immunother. 2014, 63, 675–683. [Google Scholar] [CrossRef]
- Suzuki, K.; Terakawa, T.; Furukawa, J.; Harada, K.; Hinata, N.; Nakano, Y.; Fujisawa, M. C-reactive protein and the neutrophil-to-lymphocyte ratio are prognostic biomarkers in metastatic renal cell carcinoma patients treated with nivolumab. Int. J. Clin. Oncol. 2020, 25, 135–144. [Google Scholar] [CrossRef]
- Mezquita, L.; Auclin, E.; Ferrara, R.; Charrier, M.; Remon, J.; Planchard, D.; Ponce, S.; Ares, L.P.; Leroy, L.; Audigier-Valette, C.; et al. Association of the Lung Immune Prognostic Index With Immune Checkpoint Inhibitor Outcomes in Patients With Advanced Non-Small Cell Lung Cancer. JAMA Oncol. 2018, 4, 351–357. [Google Scholar] [CrossRef]
- Schiwitza, A.; Schildhaus, H.-U.; Zwerger, B.; Rüschoff, J.; Reinhardt, C.; Leha, A.; Andreas, S.; Rittmeyer, A. Monitoring efficacy of checkpoint inhibitor therapy in patients with non-small-cell lung cancer. Immunotherapy 2019, 11, 769–782. [Google Scholar] [CrossRef] [Green Version]
- Posch, F.; Riedl, J.; Reitter, E.M.; Crowther, M.J.; Grilz, E.; Quehenberger, P.; Jilma, B.; Pabinger, I.; Ay, C. Dynamic assessment of venous thromboembolism risk in patients with cancer by longitudinal D-Dimer analysis: A prospective study. J. Thromb Haemost 2020, 18, 1348–1356. [Google Scholar] [CrossRef] [PubMed]
- Andersson, T.M.; Crowther, M.J.; Czene, K.; Hall, P.; Humphreys, K. Mammographic Density Reduction as a Prognostic Marker for Postmenopausal Breast Cancer: Results Using a Joint Longitudinal-Survival Modeling Approach. Am. J. Epidemiol. 2017, 186, 1065–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawrence Gould, A.; Boye, M.E.; Crowther, M.J.; Ibrahim, J.G.; Quartey, G.; Micallef, S.; Bois, F.Y. Joint modeling of survival and longitudinal non-survival data: Current methods and issues. Report of the DIA Bayesian joint modeling working group. Stat. Med. 2015, 34, 2181–2195. [Google Scholar] [CrossRef] [PubMed]
- Haas, M.; Laubender, R.P.; Stieber, P.; Holdenrieder, S.; Bruns, C.J.; Wilkowski, R.; Mansmann, U.; Heinemann, V.; Boeck, S. Prognostic relevance of CA 19-9, CEA, CRP, and LDH kinetics in patients treated with palliative second-line therapy for advanced pancreatic cancer. Tumor Biol. 2010, 31, 351–357. [Google Scholar] [CrossRef]
- Saito, K.; Urakami, S.; Komai, Y.; Yasuda, Y.; Kubo, Y.; Kitsukawa, S.; Okubo, Y.; Yamamoto, S.; Yonese, J.; Fukui, I. Impact of C-reactive protein kinetics on survival of patients with advanced urothelial carcinoma treated by second-line chemotherapy with gemcitabine, etoposide and cisplatin. Bju. Int. 2012, 110, 1478–1484. [Google Scholar] [CrossRef]
- Chen, Z.; Sun, Y.; Wang, J.; Shen, X.; Chen, L.; Zhuang, Z. Prognostic and Predictive Value of Serum C-Reactive Protein Levels in Patients with Metastatic Or Locally Recurrent Gastric Cancer. Int. J. Biol. Markers 2016, 31, 294–299. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n (% miss.) | Overall (n = 90) | No Progression or Death (n = 31) | Progression or Death (n = 59) | p * |
|---|---|---|---|---|---|
| Demographic characteristics | |||||
| Age at ICI initiation (years) | 90 (0%) | 67 (59–74) | 69 (57–76) | 66 (60–73) | 0.527 |
| Female gender | 90 (0%) | 44 (49%) | 11 (35%) | 33 (56%) | 0.065 |
| BMI at ICI initiation (kg/m²) | 83 (8%) | 24.3 (20.7–27.3) | 25.2 (21.2–29.7) | 24.2 (20.5–27.2) | 0.391 |
| Charlson comorbidity index at ICI initiation (points) | 90 (0%) | 8 (5–9) | 8 (5–10) | 8 (5–9) | 0.317 |
| Past or present smoker | 86 (4%) | 67 (78%) | 23 (77%) | 44 (79%) | 0.839 |
| ECOG at ICI initiation (points) | 59 (34%) | 0 (0–1) | 1 (0–1) | 0 (0–1) | 0.843 |
| Second primary malignancy at any time | 86 (4%) | 18 (21%) | 5 (17%) | 13 (23%) | 0.477 |
| Tumor variables | |||||
| Adenocarcinoma | 90 (0%) | 65 (72%) | 21 (68%) | 44 (75%) | 0.492 |
| Stage IV at initial NSCLC diagnosis | 90 (0%) | 55 (61%) | 16 (52%) | 39 (66%) | 0.180 |
| EGFR mutation | 73 (19%) | 2 (3%) | 1 (4%) | 1 (2%) | 0.999 |
| EML4–ALK rearrangement | 73 (19%) | 1 (1%) | 0 (0%) | 1 (2%) | 0.999 |
| ROS1 overexpression | 61 (32%) | 0 (0%) | 0 (0%) | 0 (0%) | N/A |
| BRAF mutation | 23 (74%) | 2 (9%) | 1 (8%) | 1 (9%) | 0.999 |
| PD-L1 expression (%) | 68 (24%) | 45 (1–80) | 60 (15–88) | 15 (0–80) | 0.087 |
| Treatment prior ICI | |||||
| Primary treatment intent: curative ** | 90 (0%) | 32 (36%) | 14 (45%) | 18 (31%) | 0.168 |
| ---Any neoadjuvant therapy (RTx, CTx, RCTx) | 32 (0%) | 8 (25%) | 4 (29%) | 4 (22%) | 0.681 |
| ---Any definitive RCTx | 32 (0%) | 6 (19%) | 4 (29%) | 2 (11%) | 0.365 |
| ---Any curative surgery | 32 (0%) | 23 (72%) | 9 (64%) | 14 (78%) | 0.400 |
| ---Any adjuvant therapy (CTx, RTx) | 32 (0%) | 12 (38%) | 3 (21%) | 9 (50%) | 0.147 |
| ICI treatment variables | |||||
| ICI treatment line | 90 (0%) | / | / | / | 0.170 |
| ---1st-line | / | 38 (42%) | 17 (55%) | 21 (36%) | / |
| ---2nd-line | / | 44 (49%) | 11 (35%) | 33 (56%) | / |
| ---3rd, 4th or 5th-line | / | 8 (9%) | 3 (10%) | 5 (8%) | / |
| ICI agent | 90 (0%) | / | / | / | 0.176 |
| ---nivolumab | / | 49 (54%) | 12 (39%) | 37 (63%) | / |
| ---pembrolizumab | / | 37 (41%) | 17 (55%) | 20 (34%) | / |
| ---Atezolizumab | / | 4 (4%) | 2 (6%) | 2 (4%) | / |
| ICI in more than 1 treatment line | 90 (0%) | 1 (1%) | 0 (0%) | 1 (2%) | 0.999 |
| Number of ICI cycles | 81 (10%) | 5 (3–15) | 7 (3–21) | 5 (2–14) | 0.280 |
| Laboratory variables | |||||
| CRP at baseline (mg/L) | 85 (6%) | 21.6 (7.7–66.1) | 14.0 (5.9–65.3) | 25.5 (8.7–72.6) | 0.258 |
| NLR at baseline (units) | 82 (9%) | 4.7 (3.1–8.9) | 4.6 (3.2–7.6) | 4.7 (3.0–9.2) | 0.807 |
| LDH at baseline (IU/L) | 82 (9%) | 263 (199–347) | 251 (183–313) | 270 (206–398) | 0.240 |
| LIPI score at baseline | 81 (10%) | / | / | / | 0.915 |
| ---0 points | / | 22 (27%) | 8 (30%) | 14 (26%) | / |
| ---1 point | / | 36 (44%) | 12 (44%) | 24 (44%) | / |
| ---2 points | / | 23 (28%) | 7 (26%) | 16 (30%) | / |
| Overall number of CRP measurements | N/A | 2090 | 595 | 1495 | N/A |
| Number of CRP measurements per patient | 90 (0%) | 18 (9–31) | 13 (7–26) | 19 (11–32) | 0.059 |
| Average of all available CRP measurements (mg/L) | 2090 (0%) | 17.8 (5.1–60.9) | 5.5 (1.8–16.5) | 29.0 (8.7–73.2) | <0.0001 |
| Variable | Outcome: Radiographic ORR (n = 73) | Outcome: PFS (n = 85) | Outcome: OS (n = 85) | |||
|---|---|---|---|---|---|---|
| OR | 95% CI (p) | HR | 95% CI (p) | HR | 95% CI (p) | |
| Demographic characteristics | ||||||
| Age at ICI initiation (per 5 years increase) | 1.46 | 1.04–2.05 (p = 0.030) | 0.88 | 0.78–0.98 (p = 0.020) | 0.87 | 0.78–0.97 (p = 0.013) |
| Female Gender | 2.77 | 0.86–8.90 (p = 0.087) | 0.83 | 0.49–1.42 (p = 0.495) | 0.46 | 0.26–0.81 (p = 0.007) |
| BMI at ICI initiation (per 5 kg/m² increase) | 1.56 | 0.88–2.77 (p = 0.127) | 0.81 | 0.56–1.11 (p = 0.195) | 0.87 | 0.64–1.19 (p = 0.380) |
| Charlson comorbidity index at ICI initiation (per 1 point increase) | 1.12 | 0.93–1.36 (p = 0.241) | 0.98 | 0.89–1.07 (p = 0.618) | 0.99 | 0.90–1.09 (p = 0.871) |
| Past or present smoker | 0.86 | 0.23–3.15 (p = 0.816) | 1.35 | 0.69–2.63 (p = 0.379) | 1.59 | 0.77–3.28 (p = 0.211) |
| ECOG at ICI initiation (per 1 point increase) | 0.33 | 0.08–1.44 (p = 0.140) | 1.87 | 0.96–3.65 (p = 0.064) | 1.66 | 0.85–3.27 (p = 0.139) |
| Second primary malignancy at any time | 0.64 | 0.16–2.60 (p = 0.535) | 1.34 | 0.71–2.52 (p = 0.372) | 1.21 | 0.63–2.32 (p = 0.575) |
| Tumor variables | ||||||
| Adenocarcinoma | 0.8 | 0.24–2.67 (p = 0.717) | 1.15 | 0.63–2.08 (p = 0.653) | 1.20 | 0.63–2.29 (p = 0.581) |
| Stage IV at initial NSCLC diagnosis | 0.42 | 0.14–1.27 (p = 0.125) | 1.78 | 1.02–3.10 (p = 0.044) | 1.80 | 1.01–3.21 (p = 0.046) |
| PD-L1 expression (per 10% increase) | 1.07 | 0.91–1.25 (p = 0.408) | 0.98 | 0.90–1.06 p = 0.577) | 0.98 | 0.90–1.07 (p = 0.672) |
| Treatment prior ICI | ||||||
| Primary treatment intent: curative | 1.08 | 0.36–3.27 (p = 0.889) | 0.50 | 0.28–0.90 (p = 0.02) | 0.49 | 0.27–0.91 (p = 0.023) |
| ICI treatment variables | ||||||
| ICI treatment: 1st-line | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| ---2nd-line | 0.57 | 0.19–1.74 (p = 0.325) | 1.61 | 0.91–2.86 (p = 0.100) | 1.89 | 1.03–3.47 (p = 0.040) |
| ---3rd, 4th or 5th-line | n/a | n/a | 1.21 | 0.45–3.26 (p = 0.701) | 1.56 | 0.61–4.00 (p = 0.358) |
| ICI agent | / | / | / | |||
| ---nivolumab | Ref. | Ref. | Ref. | Ref. | Ref | Ref. |
| ---pembrolizumab | 1.33 | 0.45–3.98 (p = 0.606) | 0.98 | 0.56–1.72 (p = 0.943) | 1.19 | 0.66–2.13 (p = 0.561) |
| ---Atezolizumab | n/a | n/a | 1.59 | 0.21–11.81 (p = 0.649) | 2.41 | 0.32–18.09 (p = 0.394) |
| Laboratory variables | ||||||
| NLR (per doubling) | 0.76 | 0.43–1.34 (p = 0.337) | 1.38 | 1.04–1.83 (p = 0.026) | 1.51 | 1.14–2.02 (p = 0.005) |
| LDH (per doubling) | 0.83 | 0.35–1.98 (p = 0.675) | 1.51 | 1.04–2.21 (p = 0.032) | 1.39 | 0.95–2.04 (p = 0.090) |
| LIPI: 0 points | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| ---1point | 1.17 | 0.33–4.19 (p = 0.805) | 1.40 | 0.72–2.71 (p = 0.317) | 1.45 | 0.71–2.98 (p = 0.313) |
| ---2 points | 0.38 | 0.06–2.23 (p = 0.281) | 2.67 | 1.28–5.55 (p = 0.009) | 3.38 | 1.54–7.43 (p = 0.002) |
| Graz Cohort | Nuremberg Cohort * | ||||
|---|---|---|---|---|---|
| Outcome | Variable | OR/HR | 95% CI (p) | OR/HR | 95% CI (p) |
| ORR | CRP (per doubling) | 0.68 | 0.51–0.92 (p = 0.013) | 0.97 | 0.75–1.24 (p = 0.784) |
| PFS | CRP (per doubling) | 1.43 | 1.21–1.70 (p < 0.0001) | 1.20 | 1.02–1.41 (p = 0.028) |
| CRP: Q1 ** | Ref. | Ref. | Ref. | Ref. | |
| CRP: Q2 | 1.04 | 0.47–2.28 (p = 0.921) | 1.34 | 0.60–3.01 (p = 0.480) | |
| CRP: Q3 | 2.18 | 1.03–4.63 (p = 0.043) | 2.04 | 0.96–4.33 (p = 0.064) | |
| CRP: Q4 | 8.46 | 3.62–19.77 (p < 0.0001) | 2.28 | 0.95–5.44 (p = 0.064) | |
| OS | CRP (per doubling) | 1.38 | 1.17–1.64 (p < 0.0001) | 1.30 | 1.12–1.51 (p = 0.001) |
| CRP: Q1 | Ref. | Ref. | Ref. | Ref. | |
| CRP: Q2 | 0.74 | 0.32–1.171 (p = 0.477) | 1.41 | 0.54–3.68 (p = 0.476) | |
| CRP: Q3 | 1.70 | 0.78–3.69 (p = 0.179) | 2.99 | 1.40–6.37 (p = 0.005) | |
| CRP: Q4 | 5.02 | 2.32–10.89 (p < 0.001) | 3.51 | 1.56–7.88 (p = 0.002) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riedl, J.M.; Barth, D.A.; Brueckl, W.M.; Zeitler, G.; Foris, V.; Mollnar, S.; Stotz, M.; Rossmann, C.H.; Terbuch, A.; Balic, M.; et al. C-Reactive Protein (CRP) Levels in Immune Checkpoint Inhibitor Response and Progression in Advanced Non-Small Cell Lung Cancer: A Bi-Center Study. Cancers 2020, 12, 2319. https://doi.org/10.3390/cancers12082319
Riedl JM, Barth DA, Brueckl WM, Zeitler G, Foris V, Mollnar S, Stotz M, Rossmann CH, Terbuch A, Balic M, et al. C-Reactive Protein (CRP) Levels in Immune Checkpoint Inhibitor Response and Progression in Advanced Non-Small Cell Lung Cancer: A Bi-Center Study. Cancers. 2020; 12(8):2319. https://doi.org/10.3390/cancers12082319
Chicago/Turabian StyleRiedl, Jakob M., Dominik A. Barth, Wolfgang M. Brueckl, Gloria Zeitler, Vasile Foris, Stefanie Mollnar, Michael Stotz, Christopher H. Rossmann, Angelika Terbuch, Marija Balic, and et al. 2020. "C-Reactive Protein (CRP) Levels in Immune Checkpoint Inhibitor Response and Progression in Advanced Non-Small Cell Lung Cancer: A Bi-Center Study" Cancers 12, no. 8: 2319. https://doi.org/10.3390/cancers12082319