The Role of Primary Tumor Resection in Colorectal Cancer Patients with Asymptomatic, Synchronous, Unresectable Metastasis: A Multicenter Randomized Controlled Trial

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Baseline Patient Characteristics
2.2. Clinical Manifestations of Upfront Chemotherapy Group (Arm 1)
2.3. Clinical Manifestations of the PTR Group (Arm 2)
2.4. Regimens for Chemotherapy
2.5. Complications Between PTR and Upfront Chemotherapy Groups
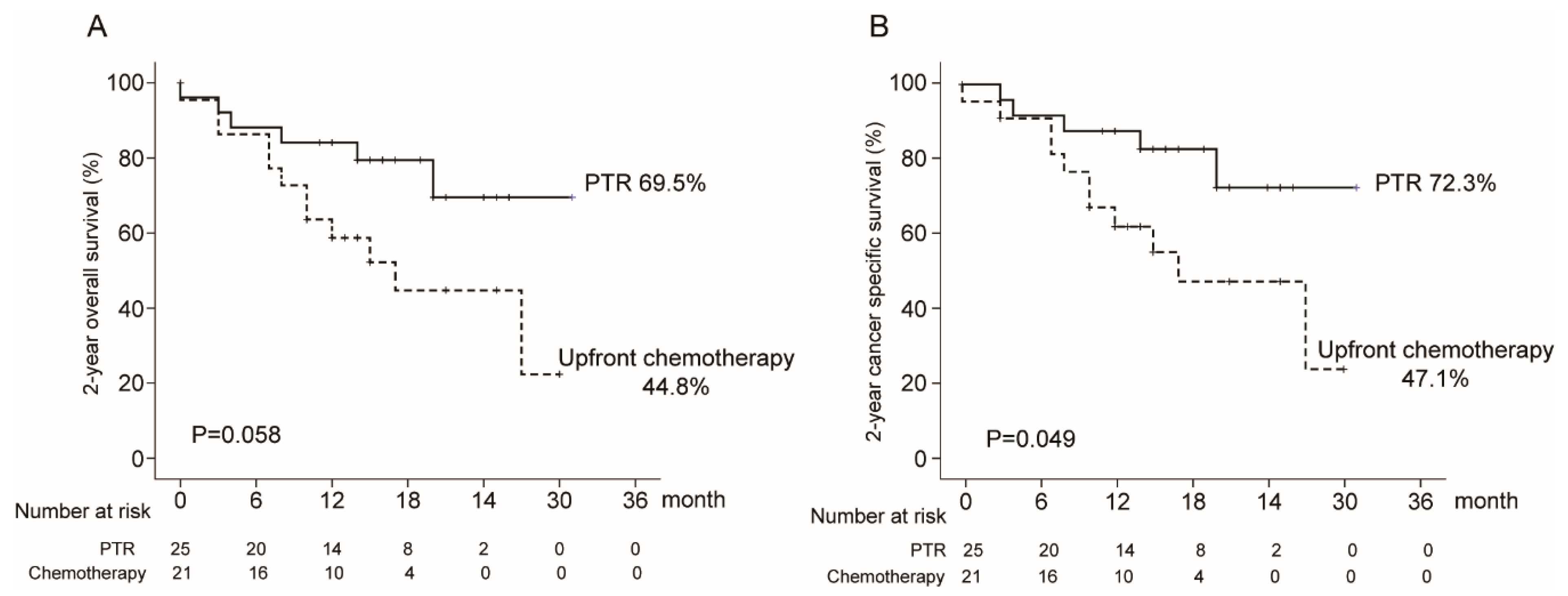
2.6. Survival Outcomes
3. Discussion
4. Materials and Methods
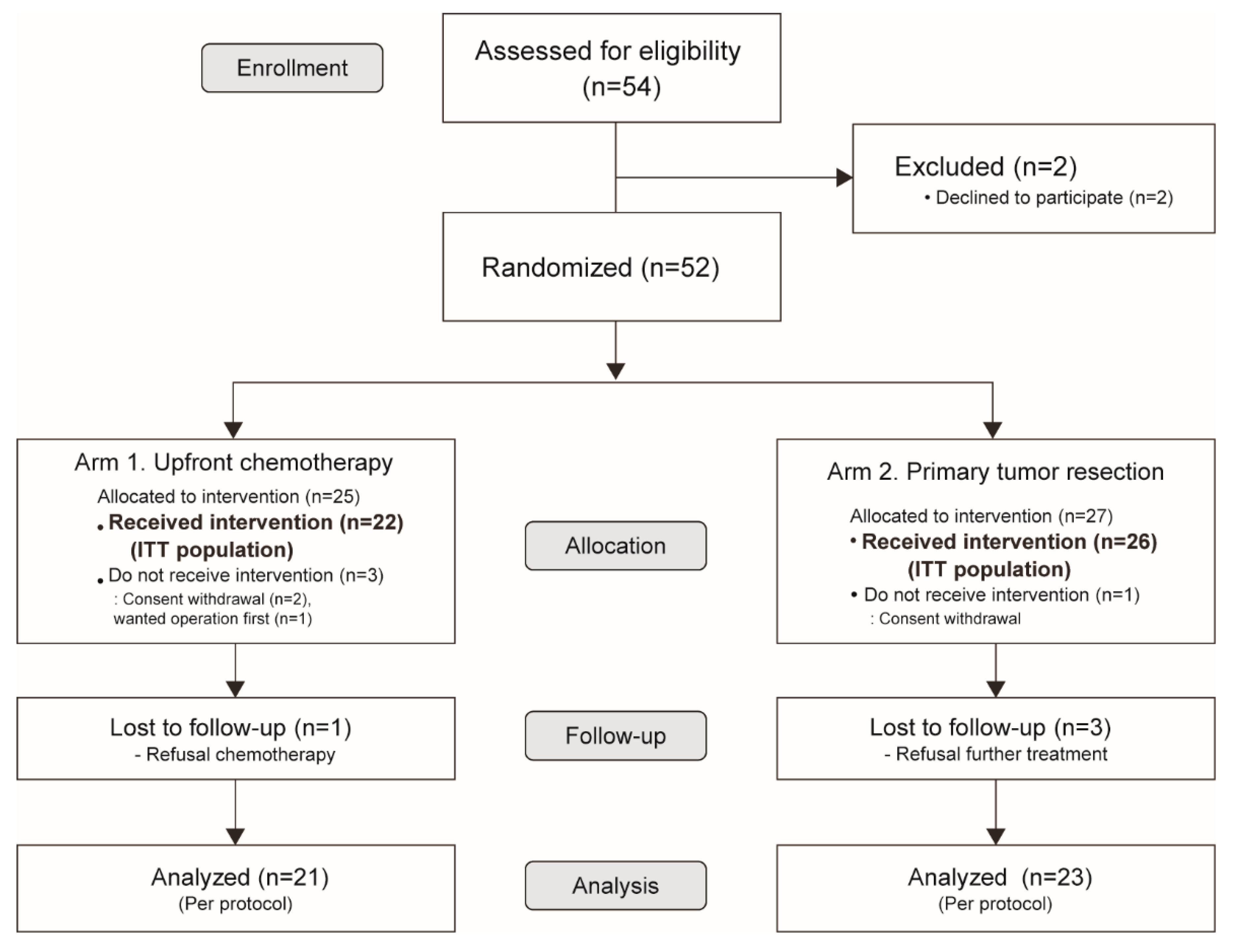
4.1. Study Design
4.2. Participants
4.3. Sample Size Calculation and Randomization
4.4. Study Endpoints and Outcome Parameters
4.5. Data Collection and Monitoring
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Mph, K.D.M.; Jemal, A. Cancer statistics, 2015. CA A Cancer J. Clin. 2015, 65, 5–29. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, U.; Stöß, C.; Stecher, L.; Wilhelm, D.; Friess, H.; Ceyhan, G.O. Meta-analysis of outcomes following resection of the primary tumour in patients presenting with metastatic colorectal cancer. BJS 2017, 105, 784–796. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Chung, M.; Ahn, J.B.; Kim, C.W.; Cho, M.S.; Shin, S.J.; Baek, S.J.; Hur, H.; Min, B.S.; Baik, S.H.; et al. Clinical significance of primary tumor resection in colorectal cancer patients with synchronous unresectable metastasis. J. Surg. Oncol. 2014, 110, 214–221. [Google Scholar] [CrossRef]
- Clancy, C.; Burke, J.P.; Barry, M.; Kalady, M.F.; Coffey, J.C. A Meta-Analysis to Determine the Effect of Primary Tumor Resection for Stage IV Colorectal Cancer with Unresectable Metastases on Patient Survival. Ann. Surg. Oncol. 2014, 21, 3900–3908. [Google Scholar] [CrossRef]
- Tarantino, I.; Warschkow, R.; Worni, M.; Cerny, T.; Ulrich, A.; Schmied, B.M.; Güller, U. Prognostic Relevance of Palliative Primary Tumor Removal in 37,793 Metastatic Colorectal Cancer Patients. Ann. Surg. 2015, 262, 112–120. [Google Scholar] [CrossRef] [Green Version]
- Tarantino, I.; Warschkow, R.; Güller, U. Palliative Primary Tumor Resection in Patients With Metastatic Colorectal Cancer. Ann. Surg. 2017, 265, e59–e60. [Google Scholar] [CrossRef]
- ‘t Lam-Boer, J.; Van Der Geest, L.G.; Verhoef, C.; Elferink, M.E.; Koopman, M.; De Wilt, J.H. Palliative resection of the primary tumor is associated with improved overall survival in incurable stage IV colorectal cancer: A nationwide population-based propensity-score adjusted study in the Netherlands. Int. J. Cancer 2016, 139, 2082–2094. [Google Scholar] [CrossRef] [Green Version]
- Saltz, L.B.; Clarke, S.; Diaz-Rubio, E.; Scheithauer, W.; Figer, A.; Wong, R.; Koski, S.; Lichinitser, M.; Yang, T.-S.; Rivera, F.; et al. Bevacizumab in Combination With Oxaliplatin-Based Chemotherapy As First-Line Therapy in Metastatic Colorectal Cancer: A Randomized Phase III Study. J. Clin. Oncol. 2008, 26, 2013–2019. [Google Scholar] [CrossRef] [Green Version]
- Hurwitz, H.; Fehrenbacher, L.; Novotny, W.; Cartwright, T.; Hainsworth, J.; Heim, W.; Berlin, J.; Baron, A.; Griffing, S.; Holmgren, E.; et al. Bevacizumab plus Irinotecan, Fluorouracil, and Leucovorin for Metastatic Colorectal Cancer. New Engl. J. Med. 2004, 350, 2335–2342. [Google Scholar] [CrossRef] [Green Version]
- Van Cutsem, E.; Köhne, C.-H.; Hitre, E.; Zaluski, J.; Chien, C.-R.C.; Makhson, A.; D’Haens, G.; Pinter, T.; Lim, R.; Bodoky, G.; et al. Cetuximab and Chemotherapy as Initial Treatment for Metastatic Colorectal Cancer. New Engl. J. Med. 2009, 360, 1408–1417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bokemeyer, C.; Bondarenko, I.; Makhson, A.; Hartmann, J.T.; Aparicio, J.; De Braud, F.G.M.; Donea, S.; Ludwig, H.; Schuch, G.; Stroh, C.; et al. Fluorouracil, Leucovorin, and Oxaliplatin With and Without Cetuximab in the First-Line Treatment of Metastatic Colorectal Cancer. J. Clin. Oncol. 2009, 27, 663–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seymour, M.; Maughan, T.S.; Ledermann, J.A.; Topham, C.; James, R.; Gwyther, S.J.; Smith, D.B.; Shepherd, S.; Maraveyas, A.; Ferry, D.R.; et al. Different strategies of sequential and combination chemotherapy for patients with poor prognosis advanced colorectal cancer (MRC FOCUS): A randomised controlled trial. Lancet 2007, 370, 143–152. [Google Scholar] [CrossRef]
- Hu, C.-Y.; Bailey, C.E.; You, Y.-Q.N.; Skibber, J.M.; Rodriguez-Bigas, M.A.; Feig, B.W.; Chang, G.J. Time trend analysis of primary tumor resection for stage IV colorectal cancer: Less surgery, improved survival. JAMA Surg. 2015, 150, 245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poultsides, G.A.; Servais, E.L.; Saltz, L.B.; Patil, S.; Kemeny, N.E.; Guillem, J.G.; Weiser, M.; Temple, L.K.; Wong, W.D.; Paty, P.B. Outcome of Primary Tumor in Patients With Synchronous Stage IV Colorectal Cancer Receiving Combination Chemotherapy Without Surgery As Initial Treatment. J. Clin. Oncol. 2009, 27, 3379–3384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCahill, L.E.; Yothers, G.; Sharif, S.; Petrelli, N.J.; Lai, L.L.; Bechar, N.; Giguere, J.K.; Dakhil, S.R.; Fehrenbacher, L.; Lopa, S.H.; et al. Primary mFOLFOX6 Plus Bevacizumab Without Resection of the Primary Tumor for Patients Presenting With Surgically Unresectable Metastatic Colon Cancer and an Intact Asymptomatic Colon Cancer: Definitive Analysis of NSABP Trial C-10. J. Clin. Oncol. 2012, 30, 3223–3228. [Google Scholar] [CrossRef] [Green Version]
- Nelson, H.; Sargent, D.J.; Wieand, H.S.; Fleshman, J.; Anvari, M.; Stryker, S.J.; Beart, R.W., Jr.; Hellinger, M.; Flanagan, R., Jr.; Peters, W.; et al. A Comparison of Laparoscopically Assisted and Open Colectomy for Colon Cancer. New Engl. J. Med. 2004, 350, 2050–2059. [Google Scholar] [CrossRef] [Green Version]
- Guillou, P.J.; Quirke, P.; Thorpe, H.; Walker, J.; Jayne, D.G.; Smith, A.M.; Heath, R.M.; Brown, J.M. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): Multicentre, randomised controlled trial. Lancet 2005, 365, 1718–1726. [Google Scholar] [CrossRef]
- Zhang, R.-X.; Ma, W.-J.; Gu, Y.-T.; Zhang, T.-Q.; Huang, Z.-M.; Lu, Z.-H.; Gu, Y.-K. Primary tumor location as a predictor of the benefit of palliative resection for colorectal cancer with unresectable metastasis. World J. Surg. Oncol. 2017, 15, 138. [Google Scholar] [CrossRef] [Green Version]
- Karoui, M.; Roudot-Thoraval, F.; Mesli, F.; Mitry, E.; Aparicio, T.; DesGuetz, G.; Louvet, C.; Landi, B.; Tiret, E.; Sobhani, I. Primary Colectomy in Patients With Stage IV Colon Cancer and Unresectable Distant Metastases Improves Overall Survival: Results of a Multicentric Study. Dis. Colon Rectum 2011, 54, 930–938. [Google Scholar] [CrossRef]
- Stillwell, A.P.; Buettner, P.G.; Ho, Y.-H. Meta-Analysis of Survival of Patients with Stage IV Colorectal Cancer Managed with Surgical Resection Versus Chemotherapy Alone. World J. Surg. 2010, 34, 797–807. [Google Scholar] [CrossRef] [PubMed]
- Moritani, K.; Kanemitsu, Y.; Shida, D.; Shitara, K.; Mizusawa, J.; Katayama, H.; Hamaguchi, T.; Shimada, Y. Colorectal Cancer Study Group (CCSG) of Japan Clinical Oncology Group (JCOG) A randomized controlled trial comparing primary tumour resection plus chemotherapy with chemotherapy alone in incurable stage IV colorectal cancer: JCOG1007 (iPACS study). Jpn. J. Clin. Oncol. 2020, 50, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Kanemitsu, Y.; Shitara, K.; Mizusawa, J.; Hamaguchi, T.; Shida, D.; Komori, K.; Ikeda, S.; Ojima, H.; Hasegawa, S.; Shiomi, A.; et al. A randomized phase III trial comparing primary tumor resection plus chemotherapy with chemotherapy alone in incurable stage IV colorectal cancer: JCOG1007 study (iPACS). J. Clin. Oncol. 2020, 38, 7. [Google Scholar] [CrossRef]
- Heinemann, V.; Von Weikersthal, L.F.; Decker, T.; Kiani, A.; Vehling-Kaiser, U.; Al-Batran, S.-E.; Heintges, T.; Lerchenmüller, C.; Kahl, C.; Seipelt, G.; et al. FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment for patients with metastatic colorectal cancer (FIRE-3): A randomised, open-label, phase 3 trial. Lancet Oncol. 2014, 15, 1065–1075. [Google Scholar] [CrossRef]
- Douillard, J.Y.; Cunningham, D.; Roth, A.D.; Navarro, M.; James, R.D.; Karasek, P.; Jandik, P.; Iveson, T.; Carmichael, J.; Alakl, M.; et al. Irinotecan combined with fluorouracil compared with fluorouracil alone as first-line treatment for metastatic colorectal cancer: A multicentre randomised trial. Lancet 2000, 355, 1041–1047. [Google Scholar] [CrossRef]
- ‘tLam-Boer, J.; Mol, L.; Verhoef, C.; De Haan, A.F.J.; Yilmaz, M.; Punt, C.J.A.; De Wilt, J.H.; Koopman, M. The CAIRO4 study: The role of surgery of the primary tumour with few or absent symptoms in patients with synchronous unresectable metastases of colorectal cancer—A randomized phase III study of the Dutch Colorectal Cancer Group (DCCG). BMC Cancer 2014, 14, 741. [Google Scholar] [CrossRef] [Green Version]
- Rahbari, N.N.; Lordick, F.; Fink, C.; Bork, U.; Stange, A.; Jaeger, D.; Luntz, S.P.; Englert, S.; Rossion, I.; Koch, M.; et al. Resection of the primary tumour versus no resection prior to systemic therapy in patients with colon cancer and synchronous unresectable metastases (UICC stage IV): SYNCHRONOUS - a randomised controlled multicentre trial (ISRCTN30964555). BMC Cancer 2012, 12, 142. [Google Scholar] [CrossRef]
- Kim, C.W.; Baek, J.-H.; Choi, G.-S.; Yu, C.S.; Kang, S.-B.; Park, W.C.; Lee, B.H.; Kim, H.R.; Oh, J.H.; Kim, J.H.; et al. The role of primary tumor resection in colorectal cancer patients with asymptomatic, synchronous unresectable metastasis: Study protocol for a randomized controlled trial. Trials 2016, 17, 34. [Google Scholar] [CrossRef] [Green Version]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Atkinson, T.M.; Ryan, S.J.; Bennett, A.V.; Stover, A.; Saracino, R.M.; Rogak, L.J.; Jewell, S.T.; Matsoukas, K.; Li, Y.; Basch, E. The association between clinician-based common terminology criteria for adverse events (CTCAE) and patient-reported outcomes (PRO): A systematic review. Support. Care Cancer 2016, 24, 3669–3676. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Arm 1 Upfront Chemotherapy Group (n = 22) | Arm 2 PTR Group (n = 26) | p Value | |
|---|---|---|---|
| Age, year: | 58.8 ± 12.1 (32–74) | 62.3 ± 11.8 (40–81) | 0.318 † |
| Sex: | |||
| Male | 12 (54.5) | 21 (80.8) | 0.051 ‡ |
| Female | 10 (45.5) | 5 (19.2) | - |
| BMI, kg/m2: | 23.1 ± 2.7 (18.4–28.3) | 22.9 ± 3.9 (13.6–34.4) | 0.846 † |
| ASA score: | 1.000 ‡‡ | ||
| 1 | 9 (40.9) | 12 (46.2) | - |
| 2 | 10 (45.5) | 11 (42.3) | - |
| 3 | 1 (4.5) | 1 (3.8) | - |
| unknown | 2 (9.1) | 2 (7.7) | - |
| ECOG performance status: | 0.714 ‡‡ | ||
| 0 | 13 (59.1) | 18 (69.2) | - |
| 1 | 7 (31.8) | 7 (26.9) | - |
| 2 | 2 (9.1) | 1 (3.8) | - |
| Co-morbidity, n (%): | 0.710 ‡‡ | ||
| Cardiovascular disease | 7 (31.8) | 9 (34.6) | - |
| Pulmonary disease | 0 (0.0) | 2 (7.7) | - |
| Metabolic disease | 2 (9.1) | 3 (11.5) | - |
| None | 13 (59.1) | 12 (46.2) | - |
| Location of the primary cancer: | 0.706 ‡‡ | ||
| Ascending colon | 6 (27.3) | 4 (15.4) | - |
| Transverse colon | 1 (4.5) | 2 (7.7) | - |
| Descending colon | 0 (0.0) | 1 (3.8) | - |
| Sigmoid colon | 11 (50.0) | 10 (38.5) | - |
| Rectosigmoid junction | 1 (4.5) | 2 (7.7) | - |
| Rectum | 3 (13.6) | 7 (26.9) | - |
| Synchronous metastasis: | 0.320 ‡‡ | ||
| Liver only | 11 (50.0) | 16 (61.5) | - |
| Lung only | 1 (4.5) | 2 (7.7) | - |
| Paraaortic lymph node only | 0 (0.0) | 2 (7.7) | - |
| Multiple metastases | 10 (45.5) | 6 (23.1) | - |
| Numbers of synchronous metastases: | 0.090 ‡‡ | ||
| 1 | 12 (54.5) | 20 (76.9) | - |
| 2 | 10 (45.5) | 5 (19.2) | - |
| ≥3 | 0 (0.0) | 1 (3.8) | - |
| Initial CEA: | 121.8 (16.6–1316.1) * | 47.6 (26.6–510.6) * | 0.649 †† |
| Upfront Chemotherapy Group (Arm 1) n = 22 | |
|---|---|
| Resectable conversion, n (%): | 4 (18.2) |
| Liver: | 4 (18.2) |
| Details for the operations of Arm 1: | 8 (36.4) |
| Resectable conversion *: | 4 (18.2) |
| LAR with liver resection | 2 (9.1) |
| AR with liver resection | 1 (4.5) |
| Rt. hemicolectomy with liver resection | 1 (4.5) |
| Palliative PTR **: | 2 (9.1) |
| LAR | 1 (4.5) |
| AR | 1 (4.5) |
| Operations due to intestinal obstruction: | 2 (9.1) |
| Rt. hemicolectomy | 1 (4.5) |
| Laparoscopic AR | 1 (4.5) |
| Intervention: | 5 (22.7) |
| GI stent insertion | 3 (13.6) |
| Salvage radiotherapy | 2 (9.1) |
| PTR Group (Arm 2) n = 26 | |
|---|---|
| Operative outcomes for PTR | |
| PTR procedures: | |
| Right hemicolectomy | 5 (19.2) |
| Left hemicolectomy | 1 (3.8) |
| Anterior resection | 8 (30.8) |
| Low anterior resection | 8 (30.8) |
| Intersphincteric resection with CAA | 2 (7.7) |
| Subtotal colectomy | 1 (3.8) |
| Total colectomy | 1 (3.8) |
| Operative method: | |
| Open | 16 (61.5) |
| Laparoscopy | 10 (38.5) |
| Stoma formation: | 2 (7.7) |
| Synchronous operations: | |
| Segmental resection of small bowel | 1 (3.8) |
| Salpingo-oophorectomy | 1 (3.8) |
| Liver resection, not curative | 1 (3.8) |
| Postoperative clinical outcomes | |
| Hospital stay, day: | 11.8 ± 6.7 (6–34) |
| Re-admission *: | 3 (11.5) |
| Septic shock | 1 (3.8) |
| General weakness | 1 (3.8) |
| Postoperative ileus | 1 (3.8) |
| Mortality * | 1 (3.8) |
| Time to beginning adjuvant chemotherapy, day | 24.8 ± 11.4 (13–66) |
| Pathologic outcomes of PTR | |
| T stages: | |
| T1–2 | 0 (0.0) |
| T3 | 17 (65.4) |
| T4a/T4b | 8 (30.8)/1 (3.8) |
| Histologic grade of the primary tumor: | |
| Well-differentiated | 1 (3.8) |
| Moderately differentiated | 23 (88.5) |
| Poorly differentiated | 2 (7.7) |
| Tumor size, cm: | 6.0 ± 1.8 (3.4–10.0) |
| Number of harvested lymph nodes: | 26.2 ± 11.1 (8–52) |
| Number of positive lymph nodes: | 5.0 ± 5.0 (0–18) |
| Lymphovascular invasion: | 19 (73.1) |
| Resectable conversion: | 4 (15.3) |
| Liver | 3 (11.5) |
| Lung | 1 (3.8) |
| Grade | Upfront Chemotherapy Group (Arm 1) n = 22 | PTR Group (Arm 2) n = 26 | ||
|---|---|---|---|---|
| Primary Tumor-Related Complications | Chemotherapy-Related Toxicity | Postoperative Complications (PTR-Related) | Chemotherapy-Related Toxicity | |
| Grade I | - | 6 (27.3%) Pain (1) Skin eruption (3) Nausea (1) HFS (1) | 2 (7.7%) Fever (1) Wound seroma (1) | 7 (26.9%) Nausea/vomiting (3) Diarrhea (1) Neuropathy (1) HFS (2) |
| Grade II | - | - | 2 (7.7%) Postoperative ileus | - |
| Grade IIIa | 3 (13.6%) Intestinal obstruction | - | - | - |
| Grade IIIb | 2 (9.1%) Intestinal obstruction | - | - | - |
| Grade IV | - | - | - | 1 (3.8%) Pneumonia |
| Grade V | - | - | 1 (3.8%) Pneumonia with sepsis | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, E.J.; Baek, J.-H.; Choi, G.-S.; Park, W.C.; Yu, C.S.; Kang, S.-B.; Min, B.S.; Kim, J.H.; Kim, H.R.; Lee, B.H.; et al. The Role of Primary Tumor Resection in Colorectal Cancer Patients with Asymptomatic, Synchronous, Unresectable Metastasis: A Multicenter Randomized Controlled Trial. Cancers 2020, 12, 2306. https://doi.org/10.3390/cancers12082306
Park EJ, Baek J-H, Choi G-S, Park WC, Yu CS, Kang S-B, Min BS, Kim JH, Kim HR, Lee BH, et al. The Role of Primary Tumor Resection in Colorectal Cancer Patients with Asymptomatic, Synchronous, Unresectable Metastasis: A Multicenter Randomized Controlled Trial. Cancers. 2020; 12(8):2306. https://doi.org/10.3390/cancers12082306
Chicago/Turabian StylePark, Eun Jung, Jeong-Heum Baek, Gyu-Seog Choi, Won Cheol Park, Chang Sik Yu, Sung-Bum Kang, Byung Soh Min, Jae Hwang Kim, Hyeong Rok Kim, Bong Hwa Lee, and et al. 2020. "The Role of Primary Tumor Resection in Colorectal Cancer Patients with Asymptomatic, Synchronous, Unresectable Metastasis: A Multicenter Randomized Controlled Trial" Cancers 12, no. 8: 2306. https://doi.org/10.3390/cancers12082306