Prognostic Value of Genetic Alterations in Elderly Patients with Acute Myeloid Leukemia: A Single Institution Experience

Abstract
:1. Introduction
2. Results
2.1. Initial Patient Characteristics
2.2. Overall Outcome
2.3. Treatment Patterns
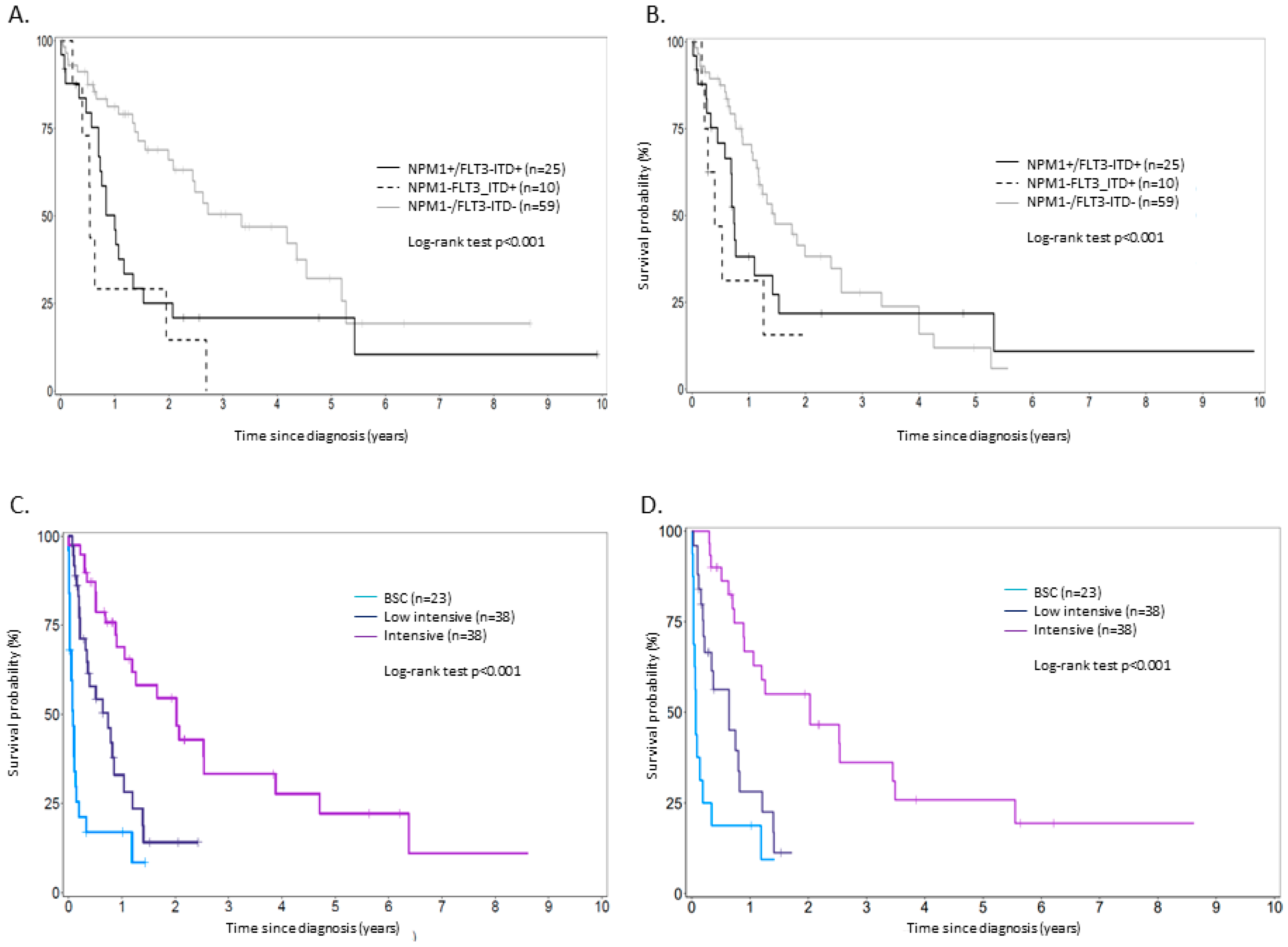
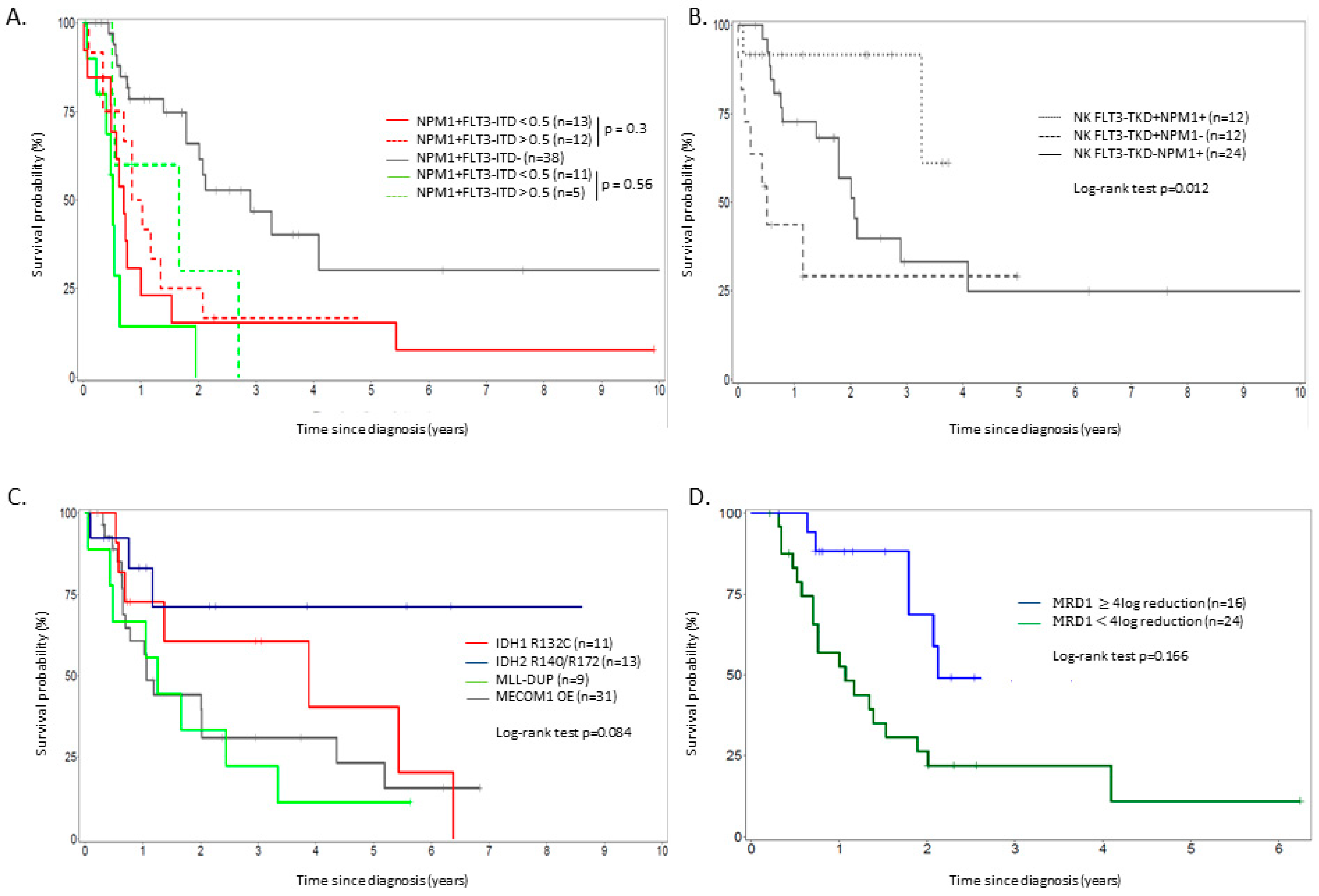
2.4. Outcome According to Molecular Markers and Minimal Residual Disease (MRD) Determined on NPM1 or WT1 Assessment
2.5. Multivariate Analysis
3. Discussion
4. Patients and Methods
4.1. Patients
4.2. Treatments
4.3. Clinical and Molecular Markers
4.4. Outcome Parameters
4.5. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Appelbaum, F.R.; Gundacker, H.; Head, D.R.; Slovak, M.L.; Willman, C.L.; Godwin, J.E.; Anderson, J.E.; Petersdorf, S.H. Age and acute myeloid leukemia. Blood 2006, 107, 3481–3485. [Google Scholar] [CrossRef] [Green Version]
- Kamminga, L.M.; de Haan, G. Cellular memory and hematopoietic stem cell aging. Stem Cell 2006, 24, 1143–1149. [Google Scholar] [CrossRef]
- Liang, Y.; Van Zant, G.; Szilvassy, S.J. Effects of aging on the homing and engraftment of murine hematopoietic stem and progenitor cells. Blood 2005, 106, 1479–1487. [Google Scholar] [CrossRef] [Green Version]
- Döhner, H.; Estey, E.H.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Burnett, A.K.; Dombret, H.; Fenaux, P.; Grimwade, D.; Larson, R.A.; et al. Diagnosis and management of acute myeloid leukemia in adults: Recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood 2010, 115, 453–474. [Google Scholar] [CrossRef] [PubMed]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef]
- Jaiswal, S.; Fontanillas, P.; Flannick, J.; Manning, A.; Grauman, P.V.; Mar, B.G.; Lindsley, R.C.; Mermel, C.H.; Burtt, N.; Chavez, A.; et al. Age-Related Clonal Hematopoiesis Associated with Adverse Outcomes. N. Engl. J. Med. 2014, 371, 2488–2498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coombs, C.C.; Zehir, A.; Devlin, S.M.; Kishtagari, A.; Syed, A.; Jonsson, P.; Hyman, D.M.; Solit, D.B.; Robson, M.E.; Baselga, J.; et al. Therapy-Related Clonal Hematopoiesis in Patients with Non-hematologic Cancers Is Common and Associated with Adverse Clinical Outcomes. Cell Stem Cell 2017, 21, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Walter, M.J.; Shen, D.; Ding, L.; Shao, J.; Koboldt, D.C.; Chen, K.; Larson, D.E.; McLellan, M.D.; Dooling, D.; Abbott, R.; et al. Clonal architecture of secondary acute myeloid leukemia. N. Engl. J. Med. 2012, 366, 1090–1098. [Google Scholar] [CrossRef]
- Mrózek, K.; Marcucci, G.; Nicolet, D.; Maharry, K.S.; Becker, H.; Whitman, S.P.; Metzeler, K.H.; Schwind, S.; Wu, Y.Z.; Kohlschmidt, J.; et al. Prognostic significance of the European LeukemiaNet standardized system for reporting cytogenetic and molecular alterations in adults with acute myeloid leukemia. J. Clin. Oncol. 2012, 30, 4515–4523. [Google Scholar] [CrossRef]
- Rao, A.V.; Valk, P.J.; Metzeler, K.H.; Acharya, C.R.; Tuchman, S.A.; Stevenson, M.M.; Rizzieri, D.A.; Delwel, R.; Buske, C.; Bohlander, S.K.; et al. Age-specific differences in oncogenic pathway dysregulation and anthracycline sensitivity in patients with acute myeloid leukemia. J. Clin. Oncol. 2009, 27, 5580–5586. [Google Scholar] [CrossRef]
- Schoch, C.; Kern, W.; Schnittger, S.; Büchner, T.; Hiddemann, W.; Haferlach, T. The influence of age on prognosis of de novo acute myeloid leukemia differs according to cytogenetic subgroups. Haematologica 2004, 89, 1082–1090. [Google Scholar] [PubMed]
- Mori, M.; Ohta, M.; Miyata, A.; Higashihara, M.; Oshimi, K.; Kimura, H.; Yagasaki, F.; Sunami, K. Treatment of acute myeloid leukemia patients aged more than 75 years: Results of the E-AML-01 trial of the Japanese Elderly Leukemia and Lymphoma Study Group (JELLSG). Leuk Lymphoma 2006, 47, 2062–2069. [Google Scholar] [CrossRef] [PubMed]
- Harb, A.J.; Tan, W.; Wilding, G.E.; Ford, L.; Sait, S.N.; Block, A.W.; Barcos, M.; Wallace, P.K.; Wang, E.S.; Wetzler, M. Treating octogenarian and nonagenarian acute myeloid leukemia patients—Predictive prognostic models. Cancer 2009, 15, 2472–2481. [Google Scholar] [CrossRef]
- Lazarevic, V.; Hörstedt, A.S.; Johansson, B.; Antunovic, P.; Billström, R.; Derolf, A.; Hulegårdh, E.; Lehmann, S.; Möllgård, L.; Nilsson, C.; et al. Incidence and prognostic significance of karyotypic subgroups in older patients with acute myeloid leukemia: The Swedish population-based experience. Blood Cancer J. 2014, 4, e188. [Google Scholar] [CrossRef] [PubMed]
- Kantarjian, H.; O’Brien, S.; Cortes, J.; Giles, F.; Faderl, S.; Jabbour, E.; Garcia-Manero, G.; Wierda, W.; Pierce, S.; Shan, J.; et al. Results of intensive chemotherapy in 998 patients age 65 years or older with acute myeloid leukemia or high-risk myelodysplastic syndrome: Predictive prognostic models for outcome. Cancer 2006, 106, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Juliusson, G.; Antunovic, P.; Derolf, A.; Lehmann, S.; Möllgård, L.; Stockelberg, D.; Tidefelt, U.; Wahlin, A.; Höglund, M. Age and acute myeloid leukemia: Real world data on decision to treat and outcomes from the Swedish Acute Leukemia Registry. Blood 2009, 113, 4179–4187. [Google Scholar] [CrossRef] [PubMed]
- Löwenberg, B.; Zittoun, R.; Kerkhofs, H.; Jehn, U.; Abels, J.; Debusscher, L.; Cauchie, C.; Peetermans, M.; Solbu, G.; Suciu, S.; et al. On the value of intensive remission-induction chemotherapy in elderly patients of 65 years with acute myeloid leukemia: A randomized phase III study of the European organization for research and treatment of cancer leukemia group. J. Clin. Oncol. 1989, 7, 1268–1274. [Google Scholar] [CrossRef]
- Kantarjian, H.; Ravandi, F.; O’Brien, S.; Cortes, J.; Faderl, S.; Garcia-Manero, G.; Jabbour, E.; Wierda, W.; Kadia, T.; Pierce, S.; et al. Intensive chemotherapy does not benefit most older patients (age 70 years or older) with acute myeloid leukemia. Blood 2010, 116, 4422–4429. [Google Scholar] [CrossRef] [Green Version]
- Silva, P.; Neumann, M.; Schroeder, M.P.; Vosberg, S.; Schlee, C.; Isaakidis, K.; Ortiz-Tanchez, J.; Fransecky, L.R.; Hartung, T.; Türkmen, S.; et al. Acute myeloid leukemia in the elderly is characterized by a distinct genetic and epigenetic landscape. Leukemia 2017, 31, 1640–1644. [Google Scholar] [CrossRef] [PubMed]
- Nagel, G.; Weber, D.; Fromm, E.; Erhardt, S.; Lübbert, M.; Fiedler, W.; Kindler, T.; Krauter, J.; Brossart, P.; Kündgen, A.; et al. Epidemiological, genetic, and clinical characterization by age of newly diagnosed acute myeloid leukemia based on an academic population-based registry study (AMLSG BiO). Ann. Hematol. 2017, 96, 1993–2003. [Google Scholar] [CrossRef] [Green Version]
- Perry, M.; Bertoli, S.; Rocher, C.; Hayette, S.; Ducastelle, S.; Barraco, F.; Labussière-Wallet, H.; Salles, G.; Recher, C.; Thomas, X.; et al. FLT3-TKD Mutations associated with NPM1 mutations define a favorable-risk group in patients with acute myeloid leukemia. Clin. Lymphoma Myeloma Leuk 2018, 18, e545–e550. [Google Scholar] [CrossRef]
- Papaemmanuil, E.; Gerstung, M.; Bullinger, L.; Gaidzik, V.I.; Paschka, P.; Roberts, N.D.; Potter, N.E.; Heuser, M.; Thol, F.; Bolli, N.; et al. Genomic classification and prognosis in acute myeloid leukemia. N. Engl. J. Med. 2016, 374, 2209–2221. [Google Scholar] [CrossRef] [PubMed]
- Boddu, P.; Kantarjian, H.; Borthakur, G.; Kadia, T.; Daver, N.; Pierce, S.; Andreeff, M.; Ravandi, F.; Cortes, J.; Kornblau, S.M. Co-occurrence of FLT3-TKD and NPM1 mutations defines a highly favorable prognostic AML group. Blood Adv. 2017, 1, 1546–1550. [Google Scholar] [CrossRef] [Green Version]
- Janke, H.; Pastore, F.; Schumacher, D.; Herold, T.; Hopfner, K.P.; Schneider, S.; Berdel, W.E.; Büchner, T.; Woermann, B.J.; Subklewe, M.; et al. Activating FLT3 mutants show distinct gain-of-function phenotypes in vitro and a characteristic signaling pathway profile associated with prognosis in acute myeloid leukemia. PLoS ONE 2014, 9, e89560. [Google Scholar] [CrossRef] [PubMed]
- Green, C.L.; Evans, C.M.; Zhao, L.; Hills, R.K.; Burnett, A.K.; Linch, D.C.; Gale, R.E. The prognostic significance of IDH2 mutations in AML depends on the location of the mutation. Blood 2011, 118, 409–412. [Google Scholar] [CrossRef] [Green Version]
- Prassek, V.V.; Rothenberg-Thurley, M.; Sauerland, M.C.; Herold, T.; Janke, H.; Ksienzyk, B.; Konstandin, N.P.; Goerlich, D.; Krug, U.; Faldum, A.; et al. Genetics of acute myeloid leukemia in the elderly: Mutation spectrum and clinical impact in intensively treated patients aged 75 years or older. Haematologica 2018, 103, 1853–1861. [Google Scholar] [CrossRef]
- Barjesteh, V.W.V.D.K.; Erpelinck, C.; van Putten, W.L.; Valk, P.J.; Hack, R.; Slater, R.; Smit, E.M.; Beverloo, H.B.; Verhoef, G.; Verdonck, L.F.; et al. High EVI1 expression predicts poor survival in acute myeloid leukemia: A study of 319 de novo AML patients. Blood 2003, 101, 837–845. [Google Scholar]
- Smol, T.; Nibourel, O.; Marceau-Renaut, A.; Celli-Lebras, K.; Berthon, C.; Quesnel, B.; Boissel, N.; Terré, C.; Thomas, X.; Castaigne, S.; et al. Quantification of EVI1 transcript levels in acute myeloid leukemia by RT-qPCR analysis: A study by the ALFA Group. Leuk Res. 2015, 39, 1443–1447. [Google Scholar] [CrossRef]
- Heiblig, M.; Le Jeune, C.; Elhamri, M.; Balsat, M.; Tigaud, I.; Plesa, A.; Barraco, F.; Labussière, H.; Ducastelle, S.; Nicolini, F.; et al. Treatment patterns and comparative effectiveness in elderly acute myeloid leukemia patients (age 70 years or older): The Lyon-university hospital experience. Leuk Lymphoma 2017, 58, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Gardin, C.; Pautas, C.; Lemasle, E.; Bourhis, J.H.; Ades, L.; Marolleau, J.P.; Valère Malfuson, J.; Gastaud, L.; Raffoux, E.; Cano, I.; et al. Role of allogeneic reduced intensity conditioning stem cell transplantation (RIC-SCT) in older patients with acute myeloid leukemia (AML): Analysis of the ALFA-1200 study. Blood 2017, 130, 466. [Google Scholar]
- Foran, J.; Sun, Z.; Claxton, D.; Lazarus, H.; Paietta, E.; Godwin, J.; Luger, S.; Rowe, J.; Altman, J.; Pratz, K.; et al. Prospective study of HLA-matched donor availability and survival in remission after AML in older adults: 1st planned analysis from ECOG-ACRIN E2906 phase III randomized trial in patients age ≥60 years. In Proceedings of the European Hematology Association Congress, Stockholm, Sweden, 16 June 2018. [Google Scholar]
- Balsat, M.; Renneville, A.; Thomas, X.; de Botton, S.; Caillot, D.; Marceau, A.; Lemasle, E.; Marolleau, J.P.; Nibourel, O.; Berthon, C.; et al. Postinduction minimal residual disease predicts outcome and benefit from allogeneic stem cell transplantation in acute myeloid leukemia with NPM1 mutation: A study by the Acute Leukemia French Association Group. J. Clin. Oncol. 2017, 35, 185–193. [Google Scholar] [CrossRef]
- Krönke, J.; Schlenk, R.F.; Jensen, K.O.; Tschürtz, F.; Corbacioglu, A.; Gaidzik, V.I.; Paschka, P.; Onken, S.; Eiwen, K.; Habdank, M.; et al. Monitoring of minimal residual disease in NPM1-mutated acute myeloid leukemia: A study from the German-Austrian acute myeloid leukemia study group. J. Clin. Oncol. 2011, 29, 2709–2716. [Google Scholar] [CrossRef]
- Buccisano, F.; Maurillo, L.; Piciocchi, A.; Del Principe, M.I.; Sarlo, C.; Cefalo, M.; Ditto, C.; Di Veroli, A.; De Santis, G.; Irno Consalvo, M.; et al. Minimal residual disease negativity in elderly patients with acute myeloid leukemia may indicate different postremission strategies than in younger patients. Ann. Hematol. 2015, 94, 1319–1326. [Google Scholar] [CrossRef]
- Boddu, P.; Jorgensen, J.; Kantarjian, H.; Borthakur, G.; Kadia, T.; Daver, N.; Alvarado, Y.; Pemmaraju, N.; Bose, P.; Naqvi, K.; et al. Achievement of a negative minimal residual disease state after hypomethylating agent therapy in older patients with AML reduces the risk of relapse. Leukemia 2017, 32, 241–244. [Google Scholar] [CrossRef]
- Lambert, J.; Lambert, J.; Thomas, X.; Marceau-Renaut, A.; Renneville, A.; Coude, M.M.; Hayette, S.; Recher, C.; Raffoux, E.; Pigneux, A.; et al. Early detection of WT1 minimal residual disease predicts outcome in acute myeloid leukemia and identify patients with high risk of relapse independently of allogeneic stem cell transplantation. Blood 2017, 130, 29. [Google Scholar]
- Bennett, J.M.; Catovsky, D.; Daniel, M.T.; Flandrin, G.; Galton, D.A.; Gralnick, H.R.; Sultan, C. Proposed revised criteria for the classification of acute myeloid leukemia. A report of the French-American-British Cooperative Group. Ann. Intern. Med. 1985, 103, 620–625. [Google Scholar] [CrossRef]
- Plesa, C.; Le, Q.H.; Chelghoum, Y.; Elhamria, M.; Tigaud, I.; Anglaret, B.; Ducastelle, S.; Perrine, M.C.; Nicolini, F.; Belhabri, A.; et al. Prognostic index for older adult patients with newly diagnosed acute myeloid leukemia: The Edouard Herriot hospital experience. Clin. Leuk 2008, 2, 198–204. [Google Scholar] [CrossRef]
- Adès, L.; Guerci, A.; Raffoux, E.; Sanz, M.; Chevallier, P.; Lapusan, S.; Recher, C.; Thomas, X.; Rayon, C.; Castaigne, S.; et al. Very long-term outcome of acute promyelocytic leukemia after treatment with all-trans retinoic acid and chemotherapy: The European APL group experience. Blood 2010, 115, 1690–1696. [Google Scholar] [CrossRef]
- Fattoum, J.; Cannas, G.; Elhamri, M.; Tigaud, I.; Plesa, A.; Heiblig, M.; Plesa, C.; Wattel, E.; Thomas, X. Effect of age on treatment decision-making in elderly patients with acute myeloid leukemia. Clin Lymphoma Myeloma Leuk 2015, 15, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Schaffer, L.G.; Slovak, M.L.; Campbell, L.J. An International System for Human Cytogenetic Nomenclature: Recommendations of the International Standing Committee on Human Cytogenetic Nomenclature; Karger Publishers: Berlin, Germany, 2009. [Google Scholar]
- Pabst, T.; Mueller, B.; Zhang, P.; Radomska, H.S.; Narravula, S.; Schnittger, S.; Behre, G.; Hiddemann, W.; Tenen, D.G. Dominant-negative mutations of CEBPA, encoding CCAAT/enhancer bindingprotein-α (C/EBPα), in acute myeloid leukemia. Nat. Genet. 2001, 27, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Huet, S.; Jallades, L.; Charlot, C.; Chabane, K.; Nicolini, F.E.; Michallet, M.; Magaud, J.P.; Hayette, S. New Quantitative Method to Identify NPM1 Mutations in Acute Myeloid Leukaemia. Leuk Res. Treat. 2013, 2013, 756703. [Google Scholar] [CrossRef] [PubMed]
- Meshinchi, S.; Woods, W.G.; Stirewalt, D.L.; Sweetser, D.A.; Buckley, J.D.; Tjoa, T.K.; Bernstein, I.D.; Radich, J.P. Prevalence and prognostic significance of Flt3 internal tandem duplication in pediatric acute myeloid leukemia. Blood 2001, 97, 89–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Libura, M.; Asnafi, V.; Tu, A.; Delabesse, E.; Tigaud, I.; Cymbalista, F.; Bennaceur-Griscelli, A.; Villarese, P.; Solbu, G.; Hagemeijer, A.; et al. FLT3 and MLL intragenic abnormalities in AML reflect a common category of genotoxic stress. Blood 2003, 2198–2204. [Google Scholar] [CrossRef]
- Caligiuri, M.A.; Strout, M.P.; Schichman, S.A.; Mrózek, K.; Arthur, D.C.; Herzig, G.P.; Baer, M.R.; Schiffer, C.A.; Heinonen, K.; Knuutila, S.; et al. Partial Tandem Duplication of ALL as a Recurrent Molecular Defect in Acute Myeloid Leukemia with Trisomy 11. Cancer Res. 1996, 56, 1418–1425. [Google Scholar] [PubMed]
- Preudhomme, C.; Sagot, C.; Boissel, N.; Cayuela, J.M.; Tigaud, I.; de Botton, S.; Thomas, X.; Raffoux, E.; Lamandin, C.; Castaigne, S.; et al. Favorable prognostic significance of CEBPA mutations in patients with de novo acute myeloid leukemia: A study from the Acute Leukemia French Association (ALFA). Blood 2002, 100, 2717–2723. [Google Scholar] [CrossRef]
- Boissel, N.; Nibourel, O.; Renneville, A.; Gardin, C.; Reman, O.; Contentin, N.; Bordessoule, D.; Pautas, C.; de Revel, T.; Quesnel, B.; et al. Prognostic Impact of Isocitrate Dehydrogenase Enzyme Isoforms 1 and 2 Mutations in Acute Myeloid Leukemia: A Study by the Acute Leukemia French Association Group. J. Clin. Oncol. 2010, 28, 3717–3723. [Google Scholar] [CrossRef] [PubMed]
- Sylvie, M.; Noordermeer, S.M.; Tönnissen, E.; van der Heijden, A.; van de Locht, L.T.; Deutz-Terlouw, P.P.; Marijt, E.W.; Jansen, J.H.; van der Reijden, B.A. Rapid identification of IDH1 and IDH2 mutations in acute myeloid leukaemia using high resolution melting curve analysis. Br. J. Haematol. 2011, 152, 493–496. [Google Scholar] [CrossRef]
- Cilloni, D.; Gottardi, E.; De Micheli, D.; Serra, A.; Volpe, G.; Messa, F.; Rege-Cambrin, G.; Guerrasio, A.; Divona, M.; Lo Coco, F.; et al. Quantitative assessment of WT1 expression by real time quantitative PCR may be a useful tool for monitoring minimal residual disease in acute leukemia patients. Leukemia 2002, 16, 2115–2121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayette, S.; Thomas, X.; Jallades, L.; Chabane, K.; Charlot, C.; Tigaud, I.; Gazzo, S.; Morisset, S.; Cornillet-Lefebvre, P.; Plesa, A.; et al. High DNA Methyltransferase DNMT3B Levels: A Poor Prognostic Marker in Acute Myeloid Leukemia. PLoS ONE 2012, 7, e51527. [Google Scholar] [CrossRef]
- Lancet, J.E.; Uy, G.L.; Cortes, J.E.; Newell, L.F.; Lin, T.L.; Ritchie, E.K.; Stuart, R.K.; Strickland, S.A.; Hogge, D.; Solomon, S.R.; et al. CPX-351 (cytarabine and daunorubicin) Liposome for Injection Versus Conventional Cytarabine Plus Daunorubicin in Older Patients With Newly Diagnosed Secondary Acute Myeloid Leukemia. J. Clin. Oncol. 2018, 36, 2684–2692. [Google Scholar] [CrossRef]
- DiNardo, C.D.; Pratz, K.; Pullarkat, V.; Jonas, B.A.; Arellano, M.; Becker, P.S.; Frankfurt, O.; Konopleva, M.; Wei, A.H.; Kantarjian, H.M.; et al. Venetoclax combined with decitabine or azacitidine in treatment-naive, elderly patients with acute myeloid leukemia. Blood 2018, 133, 7–17. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Total (n = 495) | Group 1: 60–69 yo (n = 260) | Group 2: 70+ yo (n = 235) | p-Value | |
|---|---|---|---|---|---|
| Age at diagnosis, median (range) | 69 (64–73) | 65 (60-69.9) | 74 (70–92.7) | - | |
| Sex ratio M/F (n) | 1.3 (282/213) | 1.3 (143/112) | 1.3 (134/101) | 0.95 | |
| PS > 2, n (%) | 76/440 (17.3%) | 38/223 (17%) | 38/215 (17.7%) | 0.71 | |
| WBC (G/L), median (range) | 5.6 (1.9–32) | 5.9 (1.8–32) | 5.5 (2.06–28.75) | 0.81 | |
| Hb (G/L), median (range) | 9.1 (8.1–10.5) | 9 (8.2–10.4) | 9.1 (8.1–10.6) | 0.58 | |
| Platelets (G/L), median (range) | 60 (30–103) | 60 (29–108.8) | 61 (32–101) | 0.95 | |
| Peripheral blasts, median (range) | 25 (0–100) | 20.5 (0–100) | 28 (0–95) | 0.62 | |
| Medullar blasts, median (range) | 60 (31–85) | 60 (30–80) | 65 (35–90) | 0.21 | |
| LDH (UI/L), median (range) | 452 (266–854) | 532 (310–878) | 354 (248–797) | 0.004 | |
| Extramedullar localization at diagnosis, N (%) | 18/488 (3.7%) | 7/255 (2.7%) | 11/233 (4.7%) | 0.27 | |
| Secondary AML, n (%) Solid cancer MDS/MPN | 125/488 (25.6%) 48 (9.8%) 79 (16.2%) | 68/255 (26.7%) 25 (9.8%) 45 (17.6%) | 57/233 (24.4%) 23 (9.8%) 34 (14.6%) | 0.93 | |
| ELN 2010 risk groups | Favorable, n (%) | 104 (21.1%) | 61 (23.4%) | 43 (18.2%) | 0.84 |
| Intermediate, n (%) | 249 (50.3%) | 129 (49.6%) | 120 (51.1%) | ||
| Unfavorable, n (%) | 121 (24.4%) | 60 (23.1%) | 61 (25.9%) | ||
| Failure, n (%) | 21 (4.2%) | 10 (3.9%) | 11 (4.8%) | ||
| Molecular subgroups | NPM1,n (%) | 110/464 (23.7%) | 62/242 (25.6%) | 48/222 (21.6%) | 0.5 |
| FLT3-ITD,n (%) | 78/464 (16.8%) | 40/242 (16.5%) | 38/222 (17.1%) | 0.88 | |
| FLT3-TKD,n (%) | 36/460 (7.8%) | 26/242 (10.7%) | 10/218 (4.5%) | 0.09 | |
| CEBPα,n (%) | 2/145 (1.4%) | 0/83 | 2/62 (3.2%) | 0.38 | |
| IDH1 R132H, n (%) | 24/367 (6.5%) | 16/221 (7.2%) | 8/146 (5.4%) | 0.85 | |
| IDH2 R140Q/R172K,n (%) | 25/367 (6.8%) | 16/221(7.2%) | 9/177 (5.1%) | 0.85 | |
| MLL-PTD, n (%) | 35/430 (8.1%) | 18/235 (7.6%) | 17/195 (8.7%) | 0.91 | |
| DNMT3A R882,n (%) | 36/143 (25.2%) | 22/93 (23.6%) | 14/50 (28%) | 0.56 | |
| WT1 OE, n (%) | 147/432 (34%) | 77/238 (32.3%) | 70/194 (36.1%) | 0.37 | |
| MECOM1 OE, n (%) | 54/435 (12.4%) | 33/238 (13.9%) | 21/197 (10.6%) | 0.31 | |
| Genetic characteristics available at treatment initiation, n (%) | 290 (58.6%) | 184 (70.7%) | 106 (45.1%) | <0.001 | |
| Variable | Total (n = 495) | Group1: 60–69 yo (n = 260) | Group2: 70+ yo (n = 235) | p-Value | |
|---|---|---|---|---|---|
| 1st line treatment intensity, n (%) | BSC | 92 (18.6%) | 20 (7.7%) | 72 (30.6%) | <0.001 |
| Low intensive HMA LDAC | 128 (25.8%) 68 (13.7%) 60 (12.1%) | 30 (11.5%) 20 (7.7%) 10 (3.8%) | 98 (41.6%) 49 (20.8%) 49 (20.8%) | ||
| Intensive | 259 (52.3%) | 209 (80.3%) * | 50 (21.3%) ** | ||
| Experimental drug | 16 (3.2%) | 1 (<1%) | 15 (6.4%) | 0.06 | |
| 1st line intensive chemotherapy response, n (%) | CRc Favorable *** Intermediate Unfavorable | 157/230 (68.2%) 41/44 (93.2%) 86/127 (67.7%) 23/48 (47.9%) | 135/192 (70.3%) 38/40 (95%) 71/102 (69.6%) 21/43 (48.8%) | 22/38 (57.9%) 3/4 (75%) 15/25 (60%) 2/5 (40%) | 0.13 |
| Refractory | 52/230 (22.6%) | 42/192 (21.9%) | 11/38 (28.9%) | 0.34 | |
| Early death PS 0–1 PS 2 PS 3–4 | 19/230 (8.2%) 2.9% 12% 30% | 14/192 (7.3%) 3.1% 12.5% 20.8% | 5/38 (13.2%) 2.9% 22% 50% | 0.003 | |
| 1st line low- intensive chemotherapy response, n (%) | CRc | 17/128 (13.3%) | 3/30 (10%) | 16/98 (16.3%) | 0.39 |
| Early death | 24/128 (18.7%) | 4/30 (13,3%) | 20/98 (20.4%) | 0.38 | |
| 1st line best supportive care, N (%) | Early death | 54/92 (58.7%) | 12/20 (60%) | 41/72 (56.9%) | 0.73 |
| Median time from CR1 to progression/relapse, months (95% CI) | 7.59 (4.29–13.99) | 7.89 (4.24–14.09) | 7.56 (4.98–12.07) | 0.56 | |
| HSCT in CR1, N (%) | 28 (12.1%) | 28 (14.5%) | 0 | 0.02 | |
| Median follow-up time since diagnosis, months (95% CI) | 7.62 (2.8–20) | 10.13 (4.8–26.1) | 4.6 (1.8–14.1) | 0.01 | |
| Cytogenetic/Molecular Subgroup | Treatment Intensity | CRc Rate, N (%) | Median OS, Months (95% CI) | 1 Year OS Probability, % (95% CI) | p-Value | Median PFS, Months (95% CI) | 1 Year PFS Probability, % (95% CI) | p-Value |
|---|---|---|---|---|---|---|---|---|
| NK NPM1+/FLT3-ITD- | Intensive | 33/34 (97%) | 34.8 (24–NR) | 80.6 (67.9–95.82) | <0.001 | 18.5 (14.8–NR) | 82.7 (69.9–97.9) | <0.001 |
| Low intensive | 3/12 (25%) | 9.4 (4–NR) | 40.9 (19.4–86.3) | 9.4 (3.7–NR) | 40.9 (19.4–86.3) | |||
| BSC | 0 | 2.8 (2–NR) | 26.7 (11.5–61.7) | 2.8 (1.7–NR) | 26.7 (11.5–61.7) | |||
| NK NPM1+/FLT3–ITD+ | Intensive | 17/24 (70.8%) | 10 (8.3–16.1) | 39.3 (23.6–65.3) | <0.001 | 8.4 (5.3–18.3) | 30.6 (15.9–58.5) | <0.001 |
| Low intensive | 2/8 (25%) | 3.9 (3.8–NR) | 0 | 3.9 (3.8–NR) | 0 | |||
| BSC | 0/5 | 1.3 (1.15–NR) | 0 | 1.3 (1.15–NR) | 0 | |||
| NK NPM1-/FLT3-ITD+ | Intensive | 4/10 (40%) | 7.56 (6.3–NR) | 48.2 (27.4–84.7) | 0.18 | 6.7 (3.3–NR) | 34 (15.8–73.4) | 0.37 |
| Low intensive | 0/3 | 8.15 (4.7–NR) | 34.9 (14.3–82.1) | 8.15 (4.7–NR) | 34.3 (14.3–82.1) | |||
| BSC | 0/5 | 1.15 (0.6–NR) | 12.9 (2.1–79.85) | 1.3 (0.7–NR) | 11.4 (1.81–72.0) | |||
| NK NPM1-/FLT3-ITD- | Intensive | 44/60 (73.3%) | 30.2 (10.5–NR) | 70.7 (50.2–89.7) | <0.001 | 17.4 (14–31.5) | 71.8 (59.75–86.2) | <0.001 |
| Low intensive | 2/26 (7.7%) | 13.4 (8.5–NR) | 52.8 (34.25–81.3) | 9.8 (3.2–15.6) | 39 (20.4–59.1) | |||
| BSC | 0/21 | 4.1 (4.1–NR) | 15.8 (6–41.3) | 1.4 (0.48–NR) | 19.85 (7.75–50.8) | |||
| Intermediate abnormal karyotype | Intensive | 22/38 (57.9%) | 24.2 (12.6–NR) | 67.6 (53.3–85.7) | <0.001 | 12.6 (9.1–41.4) | 52.9 (38.2–73.1) | <0.001 |
| Low intensive | 3/38 (7.9%) | 7.7 (4–14.4) | 32 (18.4–55.6) | 7.7 (4–12.5) | 28.7 (15.8–51.9) | |||
| BSC | 0/23 | 0.99 (0.59–2.23) | 16.5 (6.3–43) | 0.99 (0.6–2.2) | 14.1 (4–40) | |||
| Other molecular mutations/overexpression | ||||||||
| FLT3-TKD | Intensive | 16/24 (66.7%) | 36.4 (12.1–NR) | 66.8 (44.5–100) | – | 25.2 (10.1–NR) | 50.1 (34.6–75) | – |
| FLT3-TKD+NPM1- | 5/12 (41.7%) | 6.1 (2–NR) | 43.6 (21.8–87.44) | 0.012 | 2.5 (1.8–NR) | 36.6 (21.8–87.44) | 0.02 | |
| FLT3-TKD+NPM1+ | 11/12 (91.2%) | NR (39.2–NR) | 91.7 (77.3–100) | NR (29.6–NR) | 70.5 (77.3–100) | |||
| IDH1 R132 | 11/13 (84.6%) | 46.6 (16.4–NR) | 72.7 (50.6–100) | 0.08 | 46.6 (16.4–NR) | 72.7 (50.6–100) | 0.06 | |
| IDH2 R140Q/R712K | 13/18 (72.2%) | NR (14–NR) | 83.1 (64.1–100) | NR (11–NR) | 55.2 (34.1–75) | |||
| MLL-PTD | 7/15 (44%) | 15.1 (5.9–NR) | 66.7 (42–100) | 7.2 (3.1–NR) | 46.4 (31–79.7) | |||
| MECOM1 OE | 13/24 (54.2%) | 12.7 (8.4–62.4) | 60.7 (44.3–83.1) | 6.1 (3.2–51.4) | 50.6 (33.3–73.1) | |||
| Variables | PFS | OS | ||||||
|---|---|---|---|---|---|---|---|---|
| HR | Range | p-Value | HR | Range | p-Value | |||
| All cohort | Age < 70 vs. ≥ 70 years old | 1.36 | (1.02–1.83) | 0.039 | 1.28 | (0.95–1.73) | 0.107 | |
| PS > 2 | 1.91 | (1.32–2.75) | <0.001 | 1.88 | (1.30–2.71) | <0.001 | ||
| LDH > 400 UI/L | 1.73 | (1.27–2.35) | <0.001 | 1.56 | (1.15–2.13) | 0.005 | ||
| Risk group | Favorable | 1.00 | - | - | 1.00 | - | - | |
| Intermediate | 0.95 | (0.67–1.35) | 0.785 | 0.85 | (0.60–1.21) | 0.366 | ||
| Unfavorable | 1.24 | (0.85–1.83) | 0.265 | 1.20 | (0.81–1.76) | 0.364 | ||
| FLT3-ITD status: Mut vs. WT | 1.40 | (1.01–1.94) | 0.042 | 1.56 | (1.13–2.16) | 0.007 | ||
| Genetic characteristics at treatment decision (present vs. absent) | 0.31 | (0.19–0.58) | <0.001 | 0.42 | (0.21–0.63) | <0.001 | ||
| Treatment intensity | Intensive | 1.00 | - | - | 1.00 | - | - | |
| Low-intensive | 1.47 | (0.71–3.08) | 0.302 | 1.50 | (0.72–3.17) | 0.282 | ||
| BSC | 2.26 | (1.35–3.78) | 0.002 | 1.90 | (1.15–3.16) | 0.013 | ||
| Intensively treated patients | Age < 70 vs. ≥ 70 years old | 1.15 | (0.67–1.96) | 0.61 | 1.12 | (0.65–1.91) | 0.69 | |
| PS > 2 | 1.98 | (1.11–3.55) | 0.021 | 1.79 | (1.04–3.08) | 0.035 | ||
| Secondary AML vs. de novo | 1.46 | (0.80-2.63) | 0.21 | 1.07 | (0.71–1.59) | 0.76 | ||
| Risk group | Favorable | 1.00 | - | - | 1.00 | - | - | |
| Intermediate | 1.17 | (0.67–2.04) | 0.58 | 1.15 | (0.66–2.02) | 0.63 | ||
| Unfavorable | 2.65 | (1.33–5.28) | 0.006 | 2.78 | (1.45–5.32) | 0.002 | ||
| FLT3-ITD status: Mut vs. WT | 1.72 | (1.06–2.78) | 0.03 | 1.80 | (1.12–2.90) | 0.015 | ||
| IDH2 status: Mut vs. WT | 0.42 | (0.12–1.42) | 0.161 | 0.44 | (0.13–1.50) | 0.19 | ||
| CR1 post-induction (yes vs. no) | 0.36 | (0.23–0.56) | <0.001 | 0.39 | (0.27–0.57) | <0.001 | ||
| HSCT in CR1 (yes vs. no) | 1.02 | (0.57–1.84) | 0.93 | 1.05 | (0.59–1.88) | 0.87 | ||
| Genetic characteristics at treatment decision (present vs. absent) | 0.38 | (0.26–0.56) | <0.001 | 0.38 | (0.25–0.58) | <0.001 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heiblig, M.; Labussière-Wallet, H.; Nicolini, F.E.; Michallet, M.; Hayette, S.; Sujobert, P.; Plesa, A.; Balsat, M.; Paubelle, E.; Barraco, F.; et al. Prognostic Value of Genetic Alterations in Elderly Patients with Acute Myeloid Leukemia: A Single Institution Experience. Cancers 2019, 11, 570. https://doi.org/10.3390/cancers11040570
Heiblig M, Labussière-Wallet H, Nicolini FE, Michallet M, Hayette S, Sujobert P, Plesa A, Balsat M, Paubelle E, Barraco F, et al. Prognostic Value of Genetic Alterations in Elderly Patients with Acute Myeloid Leukemia: A Single Institution Experience. Cancers. 2019; 11(4):570. https://doi.org/10.3390/cancers11040570
Chicago/Turabian StyleHeiblig, Maël, Hélène Labussière-Wallet, Franck Emmanuel Nicolini, Mauricette Michallet, Sandrine Hayette, Pierre Sujobert, Adriana Plesa, Marie Balsat, Etienne Paubelle, Fiorenza Barraco, and et al. 2019. "Prognostic Value of Genetic Alterations in Elderly Patients with Acute Myeloid Leukemia: A Single Institution Experience" Cancers 11, no. 4: 570. https://doi.org/10.3390/cancers11040570