Mitigating Effect of 1-Palmitoyl-2-Linoleoyl-3-Acetyl-Rac-Glycerol (PLAG) on a Murine Model of 5-Fluorouracil-Induced Hematological Toxicity


Abstract
:1. Introduction
2. Results
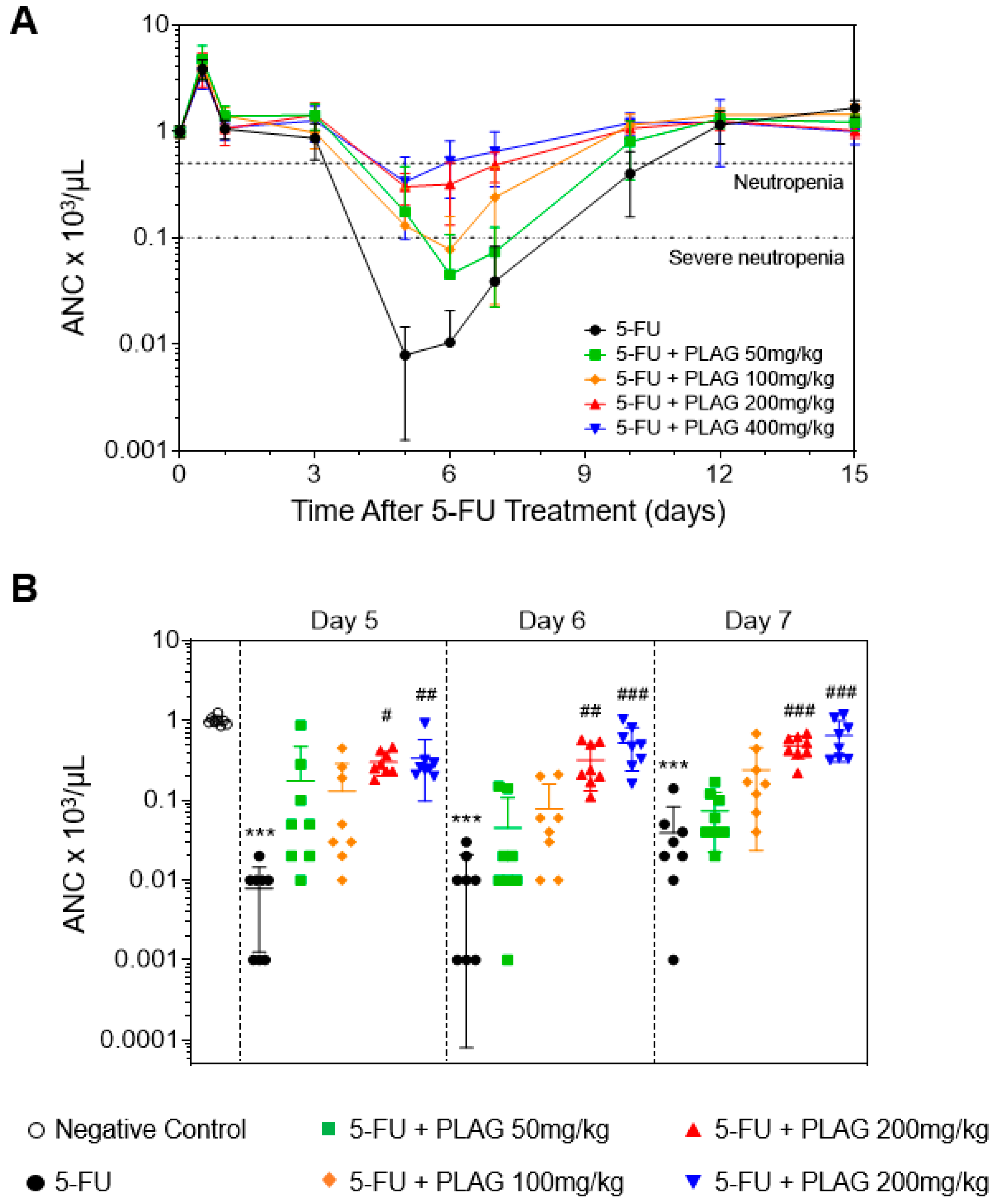
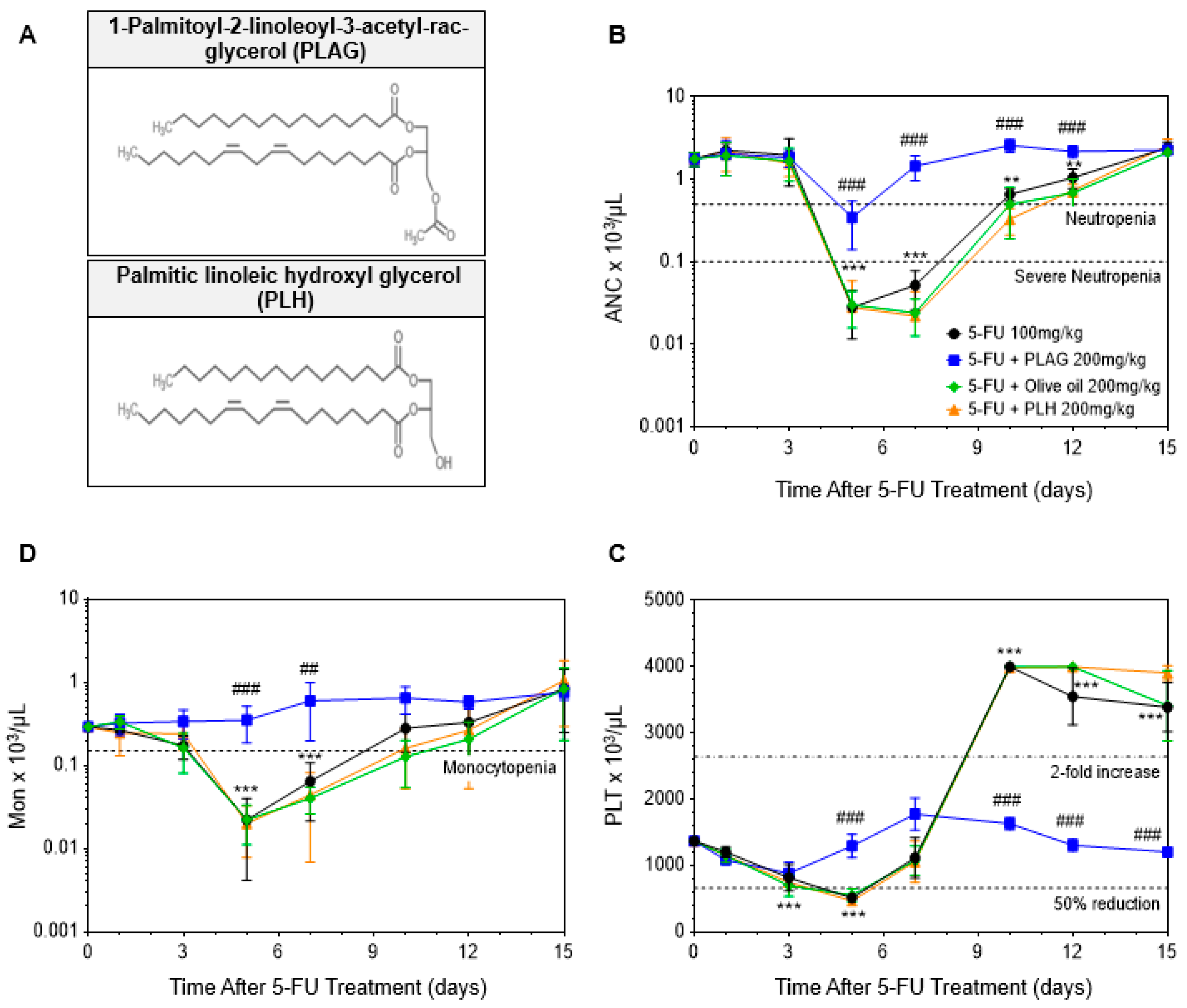
2.1. The Administration of PLAG Attenuates 5-FU-Induced Neutropenia
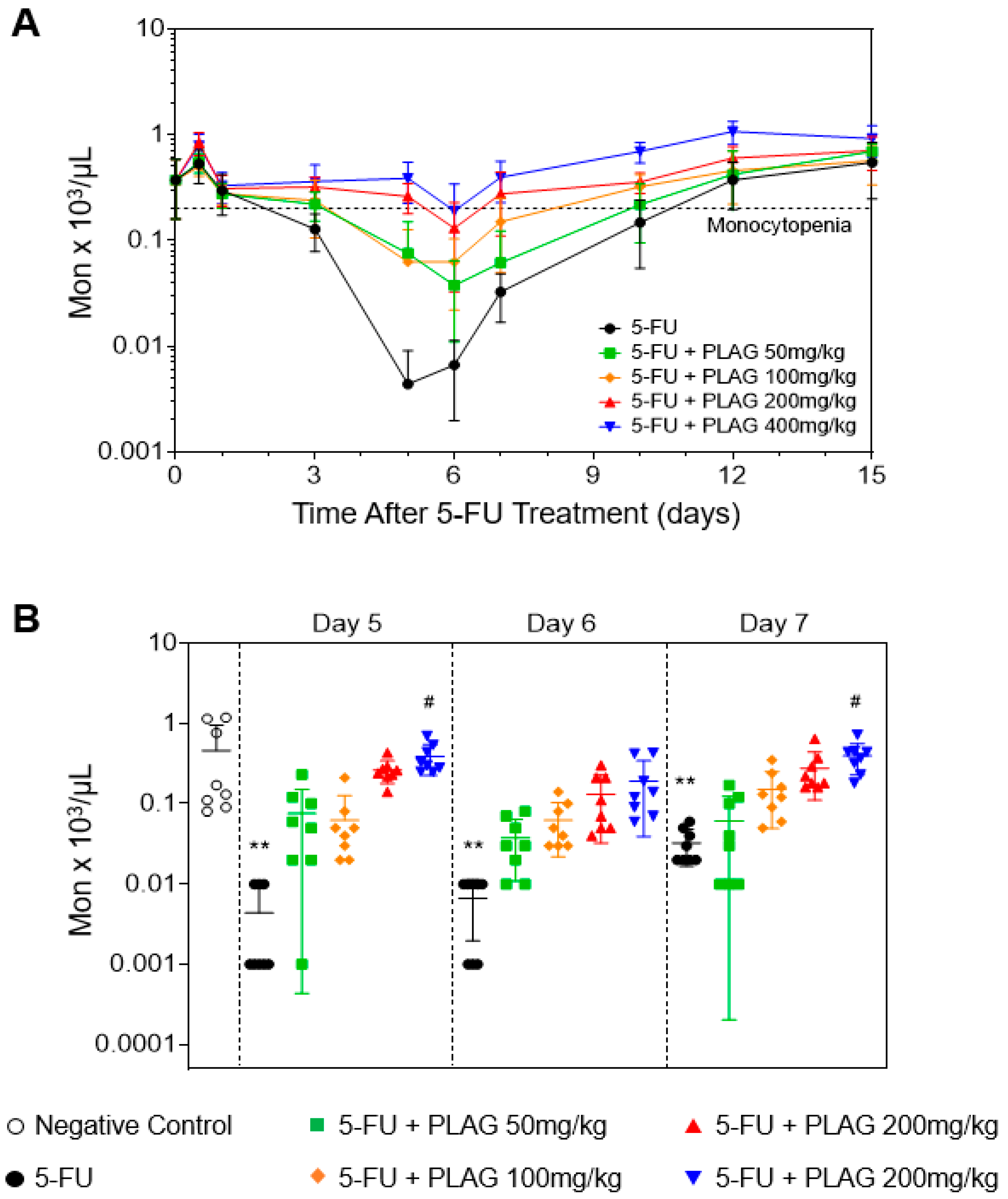
2.2. The Administration of PLAG Attenuates 5-FU-Induced Monocytopenia
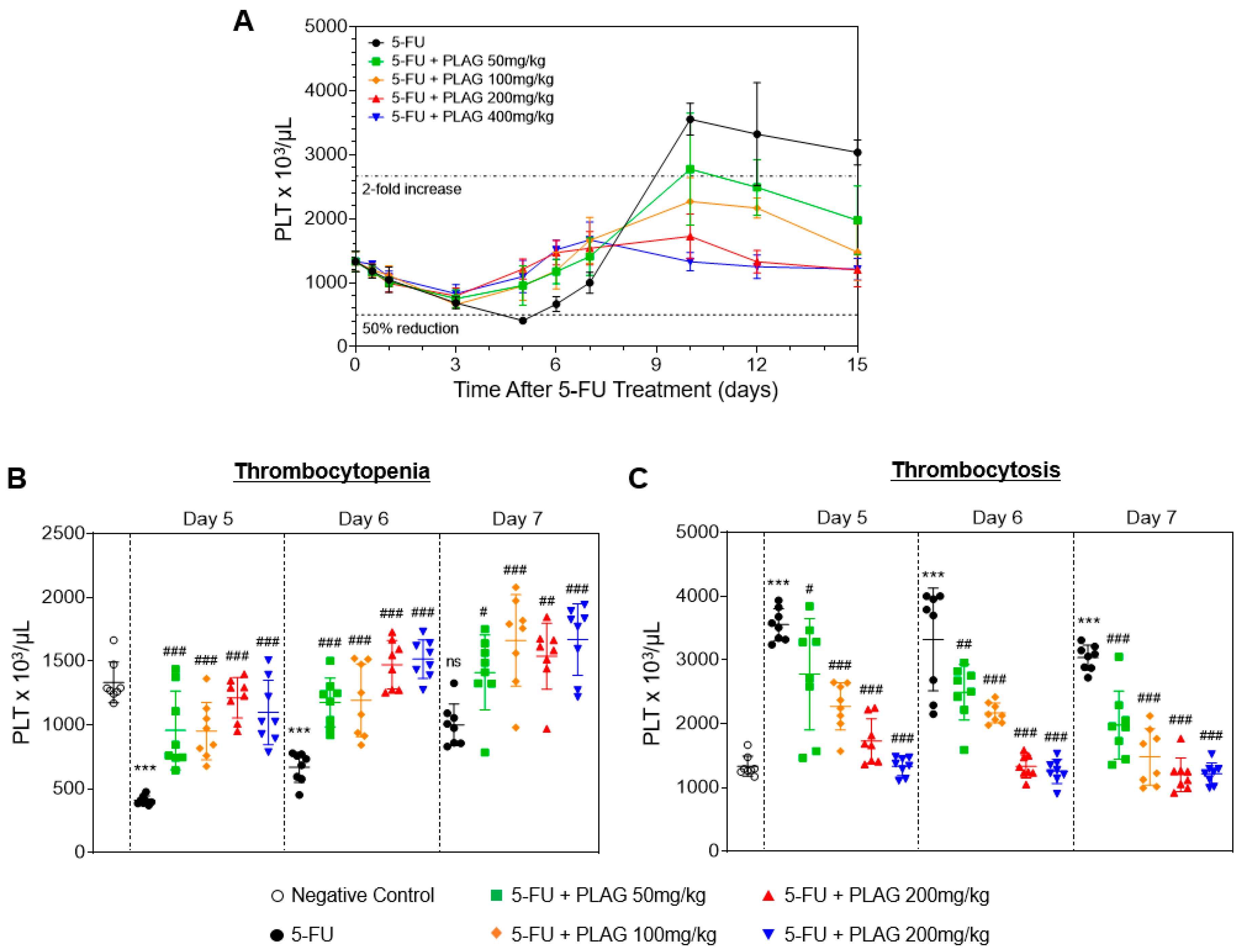
2.3. The Administration of PLAG Attenuates 5-FU-Induced Aberrant Changes in Platelet Counts
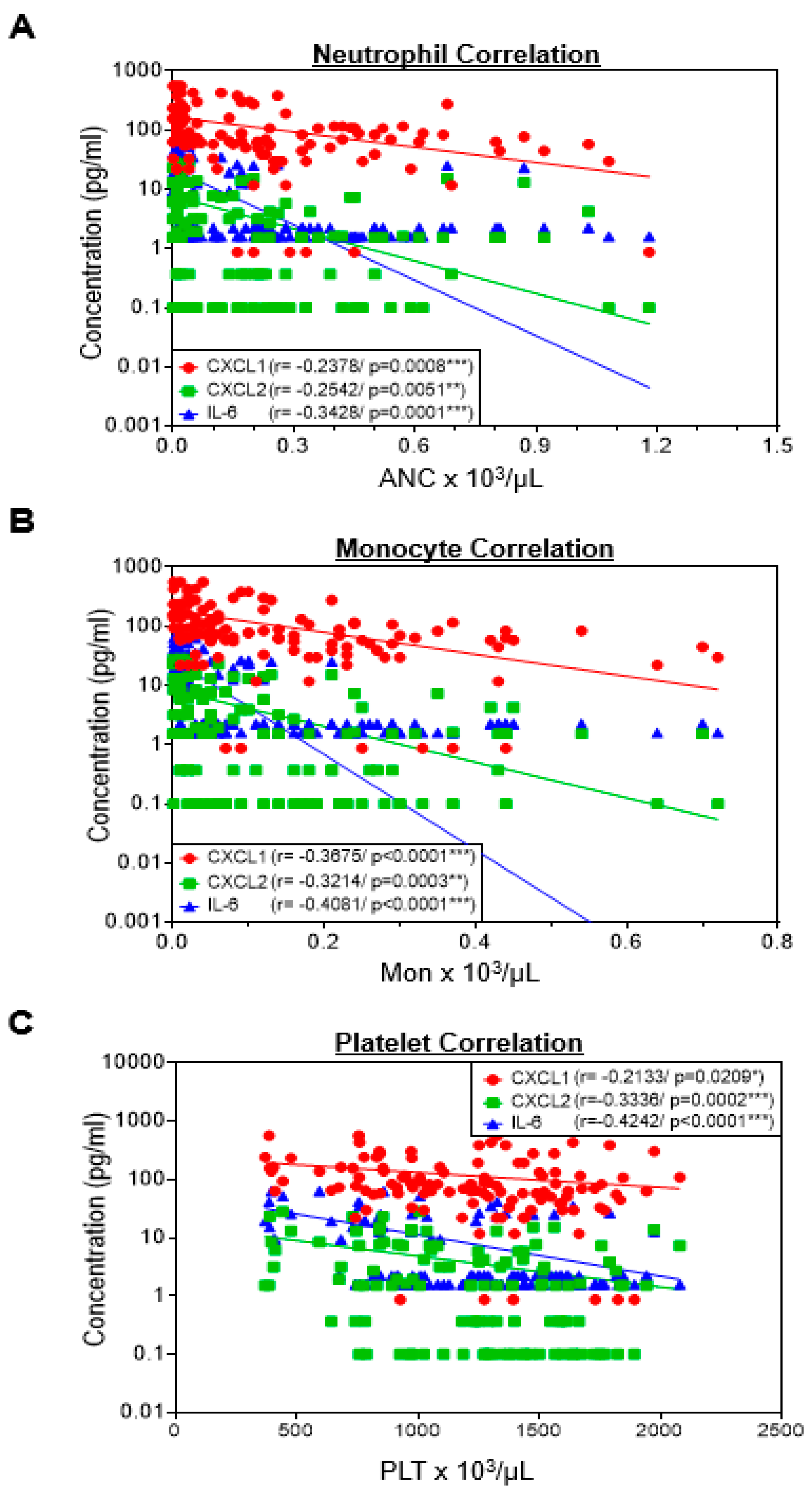
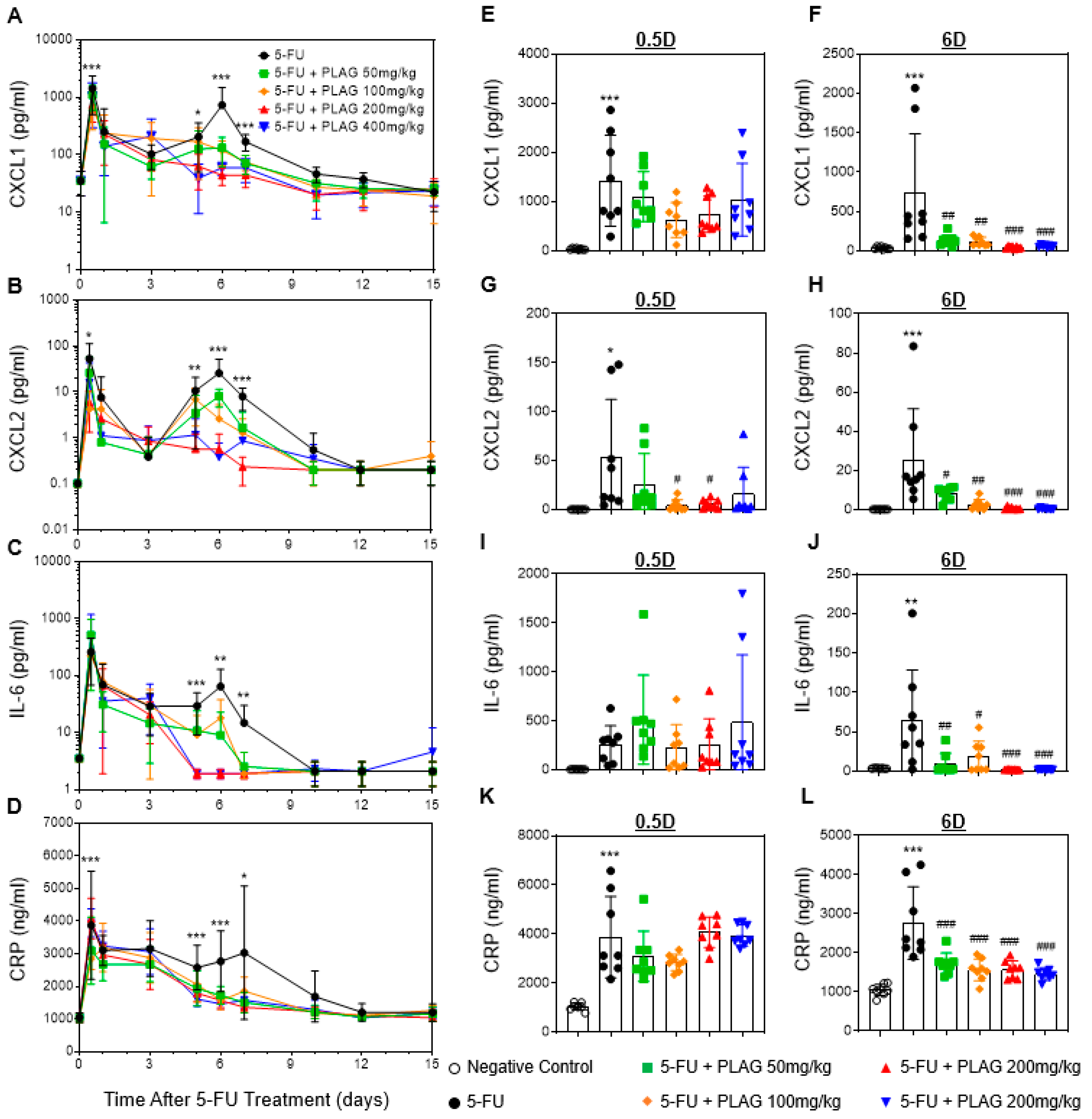
2.4. Correlation Between Hematology and Pro-Inflammatory Cytokine/Chemokines
2.5. The Administration of PLAG Attenuates Blood Levels of 5-FU-Induced Pro-Inflammatory Cytokine/Chemokines and C-Reactive Protein (CRP)
2.6. Comparative Analysis between Administration of PLAG and Olive Oil in 5-FU-Induced Hematological Toxicity
3. Discussion
4. Materials and Methods
4.1. Chemicals
4.2. Animals
4.3. Establishment of a Mouse Model of 5-FU-Induced Hematological Toxicity
4.4. Measurement of Potential Biomarkers for 5-FU-Induced Hematological Toxicity
4.5. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Longley, D.B.; Harkin, D.P.; Johnston, P.G. 5-fluorouracil: Mechanisms of action and clinical strategies. Nat. Rev. Cancer 2003, 3, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, K.; Tsuno, N.H.; Sunami, E.; Tsurita, G.; Kawai, K.; Okaji, Y.; Nishikawa, T.; Shuno, Y.; Hongo, K.; Hiyoshi, M.; et al. Chloroquine potentiates the anti-cancer effect of 5-fluorouracil on colon cancer cells. BMC Cancer 2010, 10, 370. [Google Scholar] [CrossRef]
- Carethers, J.M.; Smith, E.J.; Behling, C.A.; Nguyen, L.; Tajima, A.; Doctolero, R.T.; Cabrera, B.L.; Goel, A.; Arnold, C.A.; Miyai, K.; et al. Use of 5-fluorouracil and survival in patients with microsatellite-unstable colorectal cancer. Gastroenterology 2004, 126, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Chun, H.J.; Choi, H.S.; Kim, E.S.; Seo, Y.S.; Jeen, Y.T.; Lee, H.S.; Um, S.H.; Kim, C.H.; Sul, D. Selenium administration attenuates 5-flurouracil-induced intestinal mucositis. Nutr. Cancer 2017, 69, 616–622. [Google Scholar] [CrossRef] [PubMed]
- Kuchay, R.A. A review of complementary therapies for chemotherapy induced gastrointestinal mucositis. Drug Discov. Ther. 2017, 10, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Costa, D.V.S.; Bon-Frauches, A.C.; Silva, A.; Lima-Junior, R.C.P.; Martins, C.S.; Leitao, R.F.C.; Freitas, G.B.; Castelucci, P.; Bolick, D.T.; Guerrant, R.L.; et al. 5-fluorouracil induces enteric neuron death and glial activation during intestinal mucositis via a s100b-rage-nfkappab-dependent pathway. Sci. Rep. 2019, 9, 665. [Google Scholar] [CrossRef] [PubMed]
- Tecza, K.; Pamula-Pilat, J.; Lanuszewska, J.; Butkiewicz, D.; Grzybowska, E. Pharmacogenetics of toxicity of 5-fluorouracil, doxorubicin and cyclophosphamide chemotherapy in breast cancer patients. Oncotarget 2018, 9, 9114–9136. [Google Scholar] [CrossRef]
- Van Kuilenburg, A.B.; Meinsma, R.; Zoetekouw, L.; Van Gennip, A.H. Increased risk of grade iv neutropenia after administration of 5-fluorouracil due to a dihydropyrimidine dehydrogenase deficiency: High prevalence of the ivs14+1g>a mutation. Int. J. Cancer 2002, 101, 253–258. [Google Scholar] [CrossRef]
- Ten Berg, M.J.; van den Bemt, P.M.; Shantakumar, S.; Bennett, D.; Voest, E.E.; Huisman, A.; van Solinge, W.W.; Egberts, T.C. Thrombocytopenia in adult cancer patients receiving cytotoxic chemotherapy: Results from a retrospective hospital-based cohort study. Drug Saf. 2011, 34, 1151–1160. [Google Scholar] [CrossRef]
- Groopman, J.E.; Itri, L.M. Chemotherapy-induced anemia in adults: Incidence and treatment. J. Natl. Cancer Inst. 1999, 91, 1616–1634. [Google Scholar] [CrossRef]
- Caggiano, V.; Weiss, R.V.; Rickert, T.S.; Linde-Zwirble, W.T. Incidence, cost, and mortality of neutropenia hospitalization associated with chemotherapy. Cancer 2005, 103, 1916–1924. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, V.; Saleem, A. Review: Drug-induced neutropenia--pathophysiology, clinical features, and management. Ann. Clin. Lab. Sci. 2004, 34, 131–137. [Google Scholar] [PubMed]
- Caselli, D.; Cesaro, S.; Arico, M. Biosimilars in the management of neutropenia: Focus on filgrastim. Biologics 2016, 10, 17–22. [Google Scholar] [CrossRef]
- Crawford, J. Once-per-cycle pegfilgrastim (Neulasta) for the management of chemotherapy-induced neutropenia. Semin. Oncol. 2003, 30, 24–30. [Google Scholar] [CrossRef]
- Khoury, H.; Adkins, D.; Brown, R.; Vij, R.; Westervelt, P.; Trinkaus, K.; Goodnough, L.T.; DiPersio, J.F. Adverse side-effects associated with g-csf in patients with chronic myeloid leukemia undergoing allogeneic peripheral blood stem cell transplantation. Bone Marrow Transplant. 2000, 25, 1197–1201. [Google Scholar] [CrossRef]
- Mehta, H.M.; Malandra, M.; Corey, S.J. G-csf and gm-csf in neutropenia. J. Immunol. 2015, 195, 1341–1349. [Google Scholar] [CrossRef]
- Zhao, C.L.; Zhang, G.P.; Xiao, Z.Z.; Ma, Z.K.; Lei, C.P.; Song, S.Y.; Feng, Y.Y.; Zhao, Y.C.; Feng, X.S. Recombinant human granulocyte colony-stimulating factor promotes preinvasive and invasive estrogen receptor-positive tumor development in MMTV-erbB2 mice. J. Breast Cancer 2015, 18, 126–133. [Google Scholar] [CrossRef]
- Aliper, A.M.; Frieden-Korovkina, V.P.; Buzdin, A.; Roumiantsev, S.A.; Zhavoronkov, A. A role for g-csf and gm-csf in nonmyeloid cancers. Cancer Med. 2014, 3, 737–746. [Google Scholar] [CrossRef]
- Morris, K.T.; Khan, H.; Ahmad, A.; Weston, L.L.; Nofchissey, R.A.; Pinchuk, I.V.; Beswick, E.J. G-CSF and G-CSFR are highly expressed in human gastric and colon cancers and promote carcinoma cell proliferation and migration. Br. J. Cancer 2014, 110, 1211–1220. [Google Scholar] [CrossRef]
- Hassan, M.N.; Waller, E.K. Treating chemotherapy-induced thrombocytopenia: Is it time for oncologists to use thrombopoietin agonists? Oncology (Williston Park) 2015, 29, 295–296. [Google Scholar]
- Al-Samkari, H.; Marshall, A.L.; Goodarzi, K.; Kuter, D.J. The use of romiplostim in treating chemotherapy-induced thrombocytopenia in patients with solid tumors. Haematologica 2018, 103, e169–e172. [Google Scholar] [CrossRef] [PubMed]
- Winer, E.S.; Safran, H.; Karaszewska, B.; Bauer, S.; Khan, D.; Doerfel, S.; Burgess, P.; Kalambakas, S.; Mostafa Kamel, Y.; Forget, F. Eltrombopag for thrombocytopenia in patients with advanced solid tumors receiving gemcitabine-based chemotherapy: A randomized, placebo-controlled phase 2 study. Int. J. Hematol. 2017, 106, 765–776. [Google Scholar] [CrossRef] [PubMed]
- Kuter, D.J. Milestones in understanding platelet production: A historical overview. Br. J. Haematol. 2014, 165, 248–258. [Google Scholar] [CrossRef] [PubMed]
- Mittelman, M.; Platzbecker, U.; Afanasyev, B.; Grosicki, S.; Wong, R.S.M.; Anagnostopoulos, A.; Brenner, B.; Denzlinger, C.; Rossi, G.; Nagler, A.; et al. Eltrombopag for advanced myelodysplastic syndromes or acute myeloid leukaemia and severe thrombocytopenia (ASPIRE): A randomised, placebo-controlled, phase 2 trial. Lancet Haematol. 2018, 5, e34–e43. [Google Scholar] [CrossRef]
- Ryu, H.M.; Jeong, Y.S.; Yim, C.S.; Lee, J.H.; Chung, S.J. Quantification of EC-18, a synthetic monoacetyldiglyceride (1-palmitoyl-2-linoleoyl-3-acetyl-rac-glycerol), in rat and mouse plasma by liquid-chromatography/tandem mass spectrometry. J. Pharm. Biomed. Anal. 2017, 137, 155–162. [Google Scholar] [CrossRef]
- Jeong, J.; Kim, Y.J.; Yoon, S.Y.; Kim, Y.J.; Kim, J.H.; Sohn, K.Y.; Kim, H.J.; Han, Y.H.; Chong, S.; Kim, J.W. Plag (1-palmitoyl-2-linoleoyl-3-acetyl-rac-glycerol) modulates eosinophil chemotaxis by regulating CCL26 expression from epithelial cells. PLoS ONE 2016, 11, e0151758. [Google Scholar] [CrossRef]
- Kim, Y.J.; Shin, J.M.; Shin, S.H.; Kim, J.H.; Sohn, K.Y.; Kim, H.J.; Kang, J.K.; Yoon, S.Y.; Kim, J.W. 1-palmitoyl-2-linoleoyl-3-acetyl-rac-glycerol ameliorates arthritic joints through reducing neutrophil infiltration mediated by IL-6/STAT3 and MIP-2 activation. Oncotarget 2017, 8, 96636–96648. [Google Scholar] [CrossRef]
- Ko, Y.E.; Yoon, S.Y.; Ly, S.Y.; Kim, J.H.; Sohn, K.Y.; Kim, J.W. 1-palmitoyl-2-linoleoyl-3-acetyl-rac-glycerol (PLAG) reduces hepatic injury in concanavalin a-treated mice. J. Cell. Biochem. 2018, 119, 1392–1405. [Google Scholar] [CrossRef]
- Lee, H.R.; Yoo, N.; Kim, J.H.; Sohn, K.Y.; Kim, H.J.; Kim, M.H.; Han, M.Y.; Yoon, S.Y.; Kim, J.W. The therapeutic effect of plag against oral mucositis in hamster and mouse model. Front. Oncol. 2016, 6, 209. [Google Scholar] [CrossRef]
- Kim, Y.J.; Jeong, J.; Shin, S.H.; Lee, D.Y.; Sohn, K.Y.; Yoon, S.Y.; Kim, J.W. Mitigating effects of 1-palmitoyl-2-linoleoyl-3-acetyl-rac-glycerol (PLAG) on hematopoietic acute radiation syndrome after total-body ionizing irradiation in mice. Radiat. Res. 2019. [Google Scholar] [CrossRef]
- Jeong, J.; Kim, Y.J.; Lee, D.Y.; Moon, B.G.; Sohn, K.Y.; Yoon, S.Y.; Kim, J.W. 1-palmitoyl-2-linoleoyl-3-acetyl-rac-glycerol (PLAG) attenuates gemcitabine-induced neutrophil extravasation. Cell Biosci. 2019, 9, 4. [Google Scholar] [CrossRef] [PubMed]
- Oh, D.; Kim, M.H.; Song, T.J.; Cho, C.J.; Nam, K.; Cho, M.K.; Chun, J.H.; Jung, K.; Kim, K.P.; Kim, J.W. 1-pamitoyl-2-linoleoyl-3-acetyl-rac-glycerol may reduce incidence of gemcitabine-induced neutropenia: A pilot case-controlled study. World J. Oncol. 2015, 6, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Yanez, A.; Coetzee, S.G.; Olsson, A.; Muench, D.E.; Berman, B.P.; Hazelett, D.J.; Salomonis, N.; Grimes, H.L.; Goodridge, H.S. Granulocyte-monocyte progenitors and monocyte-dendritic cell progenitors independently produce functionally distinct monocytes. Immunity 2017, 47, 890–902.e4. [Google Scholar] [CrossRef] [PubMed]
- Kondo, M.; Oshita, F.; Kato, Y.; Yamada, K.; Nomura, I.; Noda, K. Early monocytopenia after chemotherapy as a risk factor for neutropenia. Am. J. Clin. Oncol. 1999, 22, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Oguz, A.; Karadeniz, C.; Ckitak, E.C.; Cil, V. Which one is a risk factor for chemotherapy-induced febrile neutropenia in childhood solid tumors: Early lymphopenia or monocytopenia? Pediatr. Hematol. Oncol. 2006, 23, 143–151. [Google Scholar] [CrossRef]
- Chenaille, P.J.; Steward, S.A.; Ashmun, R.A.; Jackson, C.W. Prolonged thrombocytosis in mice after 5-fluorouracil results from failure to down-regulate megakaryocyte concentration. An experimental model that dissociates regulation of megakaryocyte size and DNA content from megakaryocyte concentration. Blood 1990, 76, 508–515. [Google Scholar] [CrossRef]
- Bomfin, L.E.; Braga, C.M.; Oliveira, T.A.; Martins, C.S.; Foschetti, D.A.; Santos, A.; Costa, D.V.S.; Leitao, R.F.C.; Brito, G.A.C. 5-fluorouracil induces inflammation and oxidative stress in the major salivary glands affecting salivary flow and saliva composition. Biochem. Pharmacol. 2017, 145, 34–45. [Google Scholar] [CrossRef]
- Sommer, J.; Mahli, A.; Freese, K.; Schiergens, T.S.; Kuecuekoktay, F.S.; Teufel, A.; Thasler, W.E.; Muller, M.; Bosserhoff, A.K.; Hellerbrand, C. Analysis of molecular mechanisms of 5-fluorouracil-induced steatosis and inflammation in vitro and in mice. Oncotarget 2017, 8, 13059–13072. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.T.; Ho, T.Y.; Lin, H.; Liang, J.A.; Huang, H.C.; Li, C.C.; Lo, H.Y.; Wu, S.L.; Huang, Y.F.; Hsiang, C.Y. 5-fluorouracil induced intestinal mucositis via nuclear factor-kappab activation by transcriptomic analysis and in vivo bioluminescence imaging. PLoS ONE 2012, 7, e31808. [Google Scholar]
- Ferreira, J.N.; Correia, L.; Oliveira, R.M.; Watanabe, S.N.; Possari, J.F.; Lima, A.F.C. Managing febrile neutropenia in adult cancer patients: An integrative review of the literature. Rev. Bras. Enferm. 2017, 70, 1301–1308. [Google Scholar] [CrossRef] [Green Version]
- Kostic, I.; Gurrieri, C.; Piva, E.; Semenzato, G.; Plebani, M.; Caputo, I.; Vianello, F. Comparison of presepsin, procalcitonin, interleukin-8 and c-reactive protein in predicting bacteraemia in febrile neutropenic adult patients with haematological malignancies. Mediterr. J. Hematol. Infect. Dis. 2019, 11, e2019047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shilpakar, R.; Paudel, B.D.; Neupane, P.; Shah, A.; Acharya, B.; Dulal, S.; Wood, L.A.; Shahi, R.; Khanal, U.; Poudyal, B.S. Procalcitonin and c-reactive protein as markers of bacteremia in patients with febrile neutropenia who receive chemotherapy for acute leukemia: A prospective study from nepal. J. Glob. Oncol. 2019, 5, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Crawford, J.; Dale, D.C.; Lyman, G.H. Chemotherapy-induced neutropenia: Risks, consequences, and new directions for its management. Cancer 2004, 100, 228–237. [Google Scholar] [CrossRef]
- Munshi, H.G.; Montgomery, R.B. Severe neutropenia: A diagnostic approach. West. J. Med. 2000, 172, 248–252. [Google Scholar] [CrossRef] [Green Version]
- Bleeker, J.S.; Hogan, W.J. Thrombocytosis: Diagnostic evaluation, thrombotic risk stratification, and risk-based management strategies. Thrombosis 2011, 2011, 536062. [Google Scholar] [CrossRef]
- Kopp, H.G.; Avecilla, S.T.; Hooper, A.T.; Shmelkov, S.V.; Ramos, C.A.; Zhang, F.; Rafii, S. Tie2 activation contributes to hemangiogenic regeneration after myelosuppression. Blood 2005, 106, 505–513. [Google Scholar] [CrossRef] [Green Version]
- Marcelino, G.; Hiane, P.A.; Freitas, K.C.; Santana, L.F.; Pott, A.; Donadon, J.R.; Guimaraes, R.C.A. Effects of olive oil and its minor components on cardiovascular diseases, inflammation, and gut microbiota. Nutrients 2019, 11, 1826. [Google Scholar] [CrossRef] [Green Version]
- Alves, A.Q.; da Silva, V.A., Jr.; Goes, A.J.S.; Silva, M.S.; de Oliveira, G.G.; Bastos, I.; de Castro Neto, A.G.; Alves, A.J. The fatty acid composition of vegetable oils and their potential use in wound care. Adv. Skin Wound Care 2019, 32, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Montserrat-de la Paz, S.; Naranjo, M.C.; Millan-Linares, M.C.; Lopez, S.; Abia, R.; Biessen, E.A.L.; Muriana, F.J.G.; Bermudez, B. Monounsaturated fatty acids in a high-fat diet and niacin protect from white fat dysfunction in the metabolic syndrome. Mol. Nutr. Food Res. 2019, 63, e1900425. [Google Scholar] [CrossRef]
- Venereau, E.; Ceriotti, C.; Bianchi, M.E. Damps from cell death to new life. Front. Immunol. 2015, 6, 422. [Google Scholar] [CrossRef] [Green Version]
- Roh, J.S.; Sohn, D.H. Damage-associated molecular patterns in inflammatory diseases. Immune Netw. 2018, 18, e27. [Google Scholar] [CrossRef] [PubMed]
- Serhan, C.N.; Savill, J. Resolution of inflammation: The beginning programs the end. Nat. Immunol. 2005, 6, 1191–1197. [Google Scholar] [CrossRef] [PubMed]
- Vourc’h, M.; Roquilly, A.; Asehnoune, K. Trauma-induced damage-associated molecular patterns-mediated remote organ injury and immunosuppression in the acutely ill patient. Front. Immunol. 2018, 9, 1330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Groeningen, C.J.; Peters, G.J.; Leyva, A.; Laurensse, E.; Pinedo, H.M. Reversal of 5-fluorouracil-induced myelosuppression by prolonged administration of high-dose uridine. J. Natl. Cancer Inst. 1989, 81, 157–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaikh, A.; Bhartiya, D.; Kapoor, S.; Nimkar, H. Delineating the effects of 5-fluorouracil and follicle-stimulating hormone on mouse bone marrow stem/progenitor cells. Stem Cell Res. Ther. 2016, 7, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, H.O.; Park, J.S.; Cho, S.H.; Yoon, J.Y.; Kim, M.G.; Jhon, G.J.; Han, S.Y.; Kim, S.H. Stimulatory effects of monoacetyldiglycerides on hematopoiesis. Biol. Pharm. Bull. 2004, 27, 1121–1125. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.R.; Yoo, N.; Jeong, J.; Sohn, K.Y.; Yoon, S.Y.; Kim, J.W. Plag alleviates chemotherapy-induced thrombocytopenia via promotion of megakaryocyte/erythrocyte progenitor differentiation in mice. Thromb. Res. 2018, 161, 84–90. [Google Scholar] [CrossRef]
- Batzoglou, S.; Pachter, L.; Mesirov, J.P.; Berger, B.; Lander, E.S. Human and mouse gene structure: Comparative analysis and application to exon prediction. Genome Res. 2000, 10, 950–958. [Google Scholar] [CrossRef] [Green Version]
- Yue, F.; Cheng, Y.; Breschi, A.; Vierstra, J.; Wu, W.; Ryba, T.; Sandstrom, R.; Ma, Z.; Davis, C.; Pope, B.D.; et al. A comparative encyclopedia of DNA elements in the mouse genome. Nature 2014, 515, 355–364. [Google Scholar] [CrossRef] [Green Version]
- O’Connell, K.E.; Mikkola, A.M.; Stepanek, A.M.; Vernet, A.; Hall, C.D.; Sun, C.C.; Yildirim, E.; Staropoli, J.F.; Lee, J.T.; Brown, D.E. Practical murine hematopathology: A comparative review and implications for research. Comp. Med. 2015, 65, 96–113. [Google Scholar]
- Van der Veldt, A.A.; Lammertsma, A.A.; Smit, E.F. Scheduling of anticancer drugs: Timing may be everything. Cell Cycle 2012, 11, 4339–4343. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment | Mean First Day of Neutropenia (±SE, Range) | Mean Duration of Neutropenia in Days (±SE, Range) | Mean First Day of Monocytopenia (±SE, Range) | Mean Duration of Monocytopenia in Days (±SE, Range) | Mean First Day of Thrombocytopenia (±SE, Range) | Mean Duration of Thrombocytopenia in Days (±SE, Range) |
|---|---|---|---|---|---|---|
| Control | 4.7 ± 0.2 (3–5) | 6.0 ± 0.4 (5–7) | 3.7 ± 0.4 (3–5) | 7.5 ± 0.6 (5–9) | 4.2 ± 0.4 (3–5) | 2.1 ± 0.3 (1–3) |
| PLAG 50 | 5.1 ± 0.1 (5–6) | 5.3 ± 0.3 (4–7) | 5.1 ± 0.1 (5–6) | 5.6 ± 0.4 (4–7) | 3.7 ± 0.7 (3–5) | 1.7 ± 0.3 (1–2) |
| PLAG 100 | 5.0 ± 0.0 (5–5) | 4.6 ± 0.4 (2–5) | 4.2 ± 0.4 (3–5) | 4.5 ± 0.8 (2–7) | 3.0 ± 0.0 (3–3) | 2.0 ± 0.0 (2–2) |
| PLAG 200 | 5.0 ± 0.0 (5–5) | 3.1 ± 0.7 (1–5) | 5.8 ± 0.2 (5–6) | 1.2 ± 0.2 (1–2) | 3.0 ± 0.0 (3–3) | 2.0 ± 0.0 (2–2) |
| PLAG 400 | 4.7 ± 0.0 (3–5) | 2.9 ± 0.7 (1–5) | 6.0 ± 0.0 (6–6) | 1.0 ± 0.0 (1–1) | 3.0 ± 0.0 (3–3) | 2.0 ± 0.0 (2–2) |
| Two-sided p values (control vs. PLAG 50) | 0.5333 | 0.2168 | 0.0326 * | 0.0089 ** | 0.5455 | 0.6667 |
| Two-sided p values (control vs. PLAG 100) | >0.9999 | 0.0513 | 0.0131 * | 0.0006 *** | 0.0808 | 0.7394 |
| Two-sided p values (control vs. PLAG 200) | >0.9999 | 0.0109 * | 0.0002 *** | 0.0003 *** | N/A | N/A |
| Two-sided p values (control vs. PLAG 400) | 1 | 0.0054 ** | 0.0002 *** | 0.0003 *** | N/A | N/A |
| Treatment | Number of Mice of Severe Neutropenia | Mean First Day Severe Neutropenia (±SE, Range) | Mean Duration of Severe Neutropenia (±SE, Range) |
|---|---|---|---|
| Control | 8/8 | 5.0 ± 0.0 (5–5) | 5.1 ± 0.5 (2–7) |
| PLAG 50 | 8/8 | 5.4 ± 0.2 (5–6) | 3.2 ± 0.6 (1–5) |
| PLAG 100 | 8/8 | 5.4 ± 0.2 (5–6) | 2.1 ± 0.6 (1–5) |
| PLAG 200 | 0/8 | None | N/A |
| PLAG 400 | 0/8 | None | N/A |
| Two-sided p values (Control vs. PLAG 50) | N/A | 0.2 | 0.0177 |
| Two-sided p values (Control vs. PLAG 100) | N/A | 0.2 | 0.0079 |
| Two-sided p values (Control vs. PLAG 200) | N/A | N/A | N/A |
| Two-sided p values (Control vs. PLAG 400) | N/A | N/A | N/A |
| Treatment | Nadir of ANC (cells/μL) | Mean Number of Days to Recovery—ANC ≥ 500/μL (± SE, Range) | Nadir of Monocytes (MON) (cells/μL) | Mean Number of Days to Recovery—MON ≥ 150/μL (±SE, Range) | Nadir of Platelets (PLT) (cells/nL) | Mean Number of Days to Recovery—PLT ≥ 1000 × 103/μL (±SE, Range) |
|---|---|---|---|---|---|---|
| Control | 3.2 ± 1.4 | 11.0 ± 0.4 (10–12) | 2.1 ± 1.1 | 11.2 ± 0.4 (10–12) | 409.6 ± 12.2 | 8.5 ± 0.6 (7–10) |
| PLAG 50 | 17.6 ± 5.2 | 10.5 ± 0.3 (10–12) | 16.4 ± 5.6 | 10.7 ± 0.4 (10–12) | 689.5 ± 28.5 | 5.7 ± 0.2 (5–7) |
| PLAG 100 | 27.5 ± 6.7 | 9.6 ± 0.4 (7–10) | 32.5 ± 4.1 | 8.9 ± 0.5 (7–10) | 660.6 ± 19.8 | 6.4 ± 0.6 (5–10) |
| PLAG 200 | 236.2 ± 36.4 | 8.1 ± 0.7 (6–10) | 106.2 ± 22.6 | 7.0 ± 0.0 (7–7) | 786.1 ± 37.7 | 4.9 ± 0.3 (3–6) |
| PLAG 400 | 245 ± 19.8 | 8.1 ± 0.7 (6–10) | 142.5 ± 26.2 | 7.0 ± 0.0 (7–7) | 813.1 ± 48.7 | 5.4 ± 0.2 (5–6) |
| Two-sided p values (control vs. PLAG 50) | 0.0123 * | 0.6084 | 0.0076 ** | 0.2104 | 0.0002 *** | 0.0008 *** |
| Two-sided p values (control vs. PLAG 100) | 0.0016 ** | 0.0513 | 0.0002 *** | 0.0011 * | 0.0002 *** | 0.0194 * |
| Two-sided p values (control vs. PLAG 200) | 0.0002 *** | 0.0109 * | 0.0002 *** | 0.0009 *** | 0.0002 *** | 0.0002 *** |
| Two-sided p values (control vs. PLAG 400) | 0.0002 *** | 0.0109 * | 0.0002 *** | 0.0007 *** | 0.0002 *** | 0.0002 *** |
| Title | Treatment | Two-Sided p Values (Control vs.) | |||||
|---|---|---|---|---|---|---|---|
| Control | PLAG | Olive Oil | PLH | PLAG | Olive Oil | PLH | |
| Mean First Day of Neutropenia | 5.0 ± 0.0 (5–5) | 5.0 ± 0.0 (5–5) | 5.0 ± 0.0 (5–5) | 5.0 ± 0.0 (5–5) | 1 | 1 | 1 |
| Mean Duration of Neutropenia | 5.0 ± 0.0 (5–5) | 2.0 ± 0.0 (2–2) | 8.0 ± 1.2 (5–10) | 7.0 ± 0.0 (7–7) | 0.06 | 0.0269 * | 0.1824 |
| Number of mice of Severe Neutropenia | 5/5 | 0/5 | 5/5 | 5/5 | N/A | N/A | N/A |
| Mean First Day of Severe Neutropenia | 5.0 ± 0.0 (5–5) | N/A | 5.0 ± 0.0 (5–5) | 5.0 ± 0.0 (5–5) | N/A | 1 | 1 |
| Mean Duration of Severe Neutropenia | 5.0 ± 0.0 (5–5) | N/A | 5.0 ± 0.0 (5–5) | 5.0 ± 0.0 (5–5) | N/A | 1 | 1 |
| Nadir of ANC (cells/μL) | 28.0 ± 7.3 | 344.0 ± 90.8 | 18.0 ± 2.0 | 8.2 ± 1.8 | 0.0008 *** | 0.9986 | 0.9896 |
| Mean Number of Days to Recovery ANC ≥ 500 μL (±SE, range) | 10.0 ± 0.0 (10–10) | 7.0 ± 0.0 (7–7) | 12.4 ± 1.2 (10–15) | 12.0 ± 0.0 (12–12) | 0.0375 * | 0.0577 | 0.132 |
| Mean First Day of Monocytopenia | 4.2 ± 0.5 (3–5) | 6.0 ± 1.0 (5–7) | 4.2 ± 0.5 (3–5) | 3.8 ± 0.8 (1–5) | 0.4274 | 1 | 0.9661 |
| Mean Duration of Monocytopenia | 6.2 ± 0.8 (5–9) | 2.5 ± 0.5 (2–3) | 7.6 ± 1.7 (5–12) | 6.2 ± 0.5 (5–7) | 0.1327 | 0.6458 | >0.9999 |
| Nadir of MON | 20.2 ± 8.2 | 198.0 ± 37.5 | 20.0 ± 3.2 | 16.0 ± 2.5 | <0.0001 *** | >0.9999 | 0.9986 |
| Mean Number of Days to Recovery MON ≥ 150/μL (±SE, range) | 10.4 ± 0.4 (10–12) | 8.5 ± 1.5 (7–10) | 10.8 ± 0.5 (10–12) | 10.8 ± 0.5 (10–12) | 0.2488 | 0.9454 | 0.9454 |
| Mean First Day of Thrombocytopenia | 4.6 ± 0.4 (3–5) | 3.0 ± 0.0 (3–3) | 4.6 ± 0.4 (3–5) | 4.6 ± 0.4 (3–5) | 0.3979 | >0.9999 | >0.9999 |
| Mean Duration of Thrombocytopenia | 2.4 ± 0.4 (2–4) | 2.0 ± 0.0 (2–2) | 2.4 ± 0.4 (2–4) | 2.4 ± 0.4 (2–4) | 0.976 | >0.9999 | >0.9999 |
| Nadir of PLT | 509.0 ± 13.2 | 868.8 ± 70.2 | 518.8 ± 50.3 | 462.8 ± 17.8 | 0.0002 *** | 0.9986 | 0.8826 |
| Mean Number of Days to Recovery PLT ≥ 1000 × 103/μL (±SE, range) | 8.8 ± 0.7 (7–10) | 5.0 ± 0.0 (5–5) | 7.6 ± 0.6 (7–10) | 8.2 ± 0.7 (7–10) | 0.0048 ** | 0.5361 | 0.9013 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, J.; Kim, Y.-J.; Lee, D.Y.; Sohn, K.-Y.; Yoon, S.Y.; Kim, J.W. Mitigating Effect of 1-Palmitoyl-2-Linoleoyl-3-Acetyl-Rac-Glycerol (PLAG) on a Murine Model of 5-Fluorouracil-Induced Hematological Toxicity. Cancers 2019, 11, 1811. https://doi.org/10.3390/cancers11111811
Jeong J, Kim Y-J, Lee DY, Sohn K-Y, Yoon SY, Kim JW. Mitigating Effect of 1-Palmitoyl-2-Linoleoyl-3-Acetyl-Rac-Glycerol (PLAG) on a Murine Model of 5-Fluorouracil-Induced Hematological Toxicity. Cancers. 2019; 11(11):1811. https://doi.org/10.3390/cancers11111811
Chicago/Turabian StyleJeong, Jinseon, Yong-Jae Kim, Do Young Lee, Ki-Young Sohn, Sun Young Yoon, and Jae Wha Kim. 2019. "Mitigating Effect of 1-Palmitoyl-2-Linoleoyl-3-Acetyl-Rac-Glycerol (PLAG) on a Murine Model of 5-Fluorouracil-Induced Hematological Toxicity" Cancers 11, no. 11: 1811. https://doi.org/10.3390/cancers11111811