Rapid Simultaneous Determination of Paraquat and Creatinine in Human Serum Using a Piece of Paper


Abstract
:1. Introduction
2. Materials and Methods
2.1. Reagents
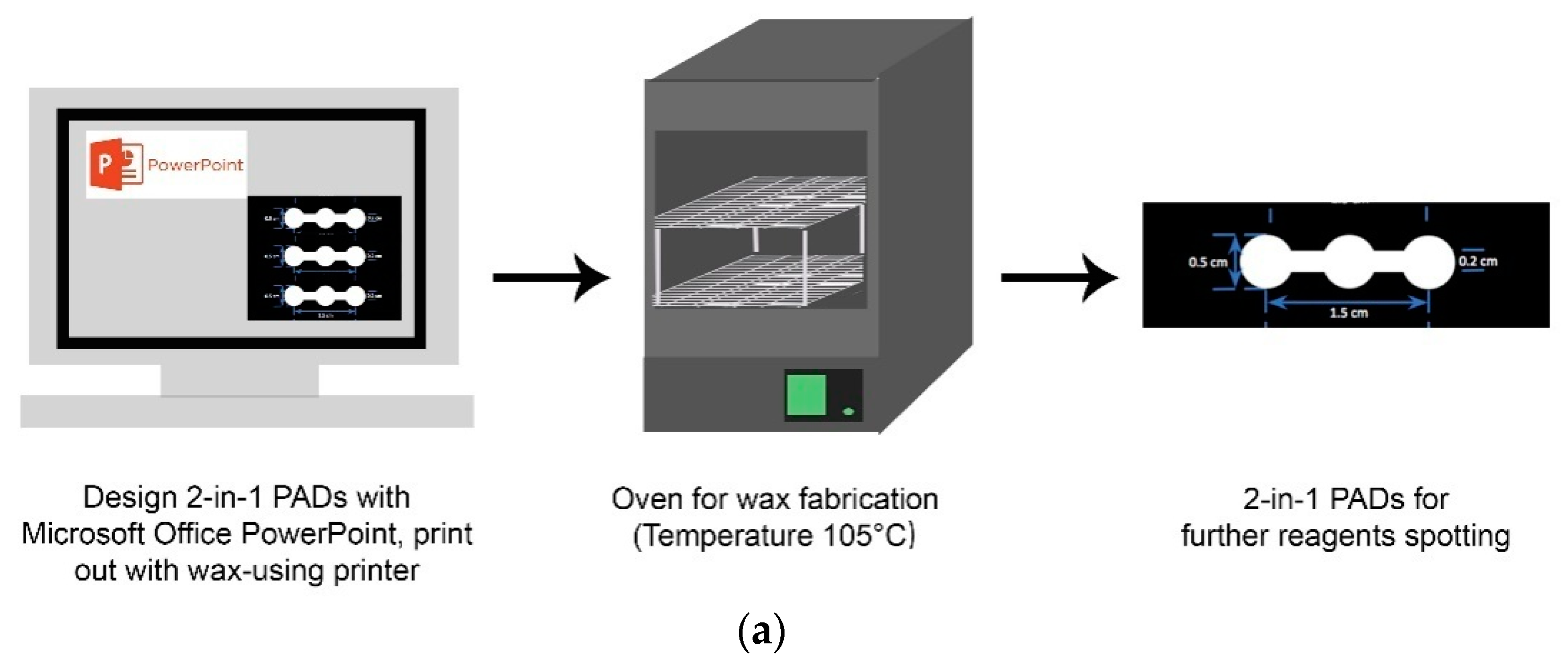
2.2. Fabrication of 2-in-1 PADs
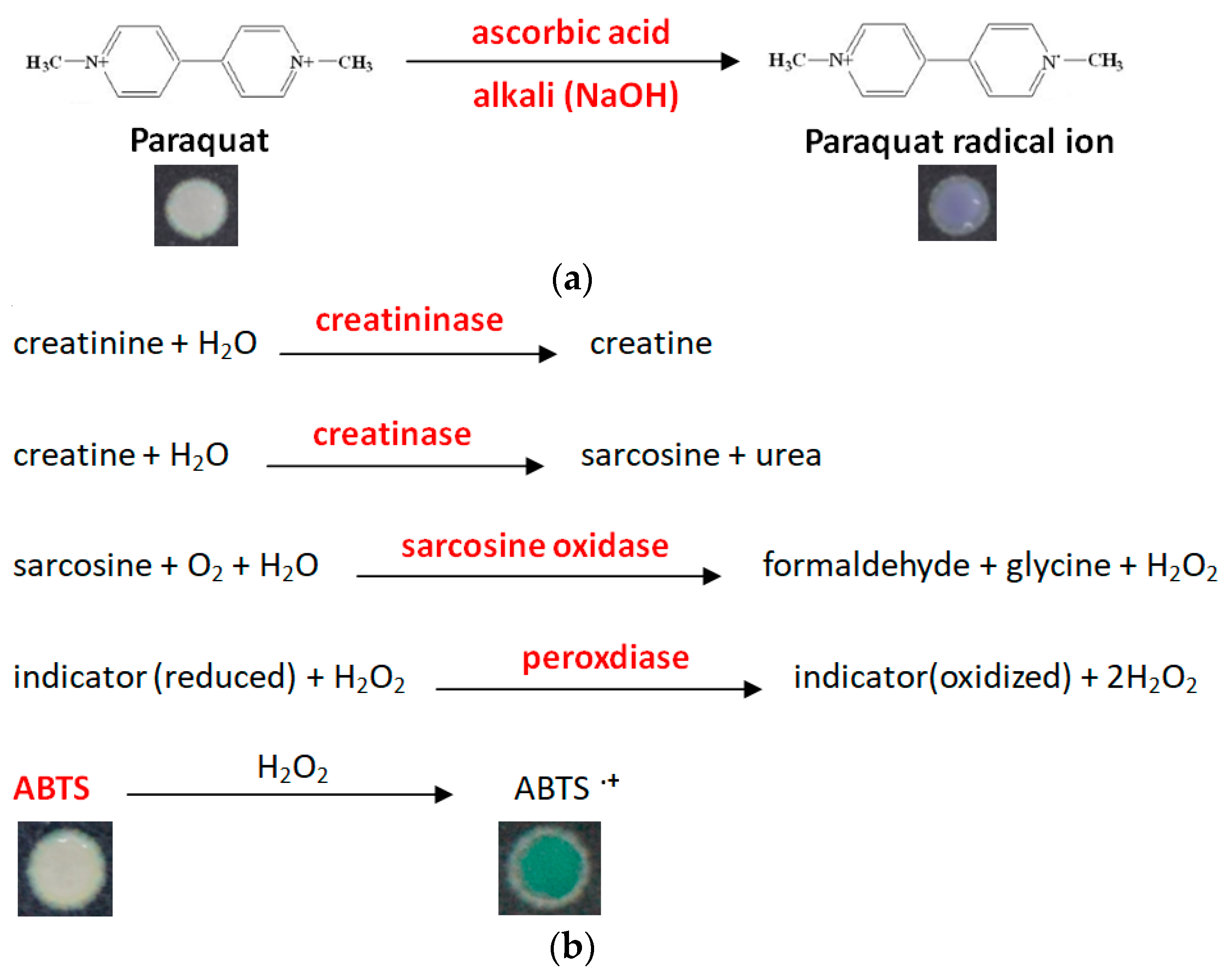
2.3. Colorimetric Assays
2.4. Image Analysis
2.5. Clinical Samples
3. Results and Discussion
3.1. PQ Standard Curve in Serum and Buffer Systems
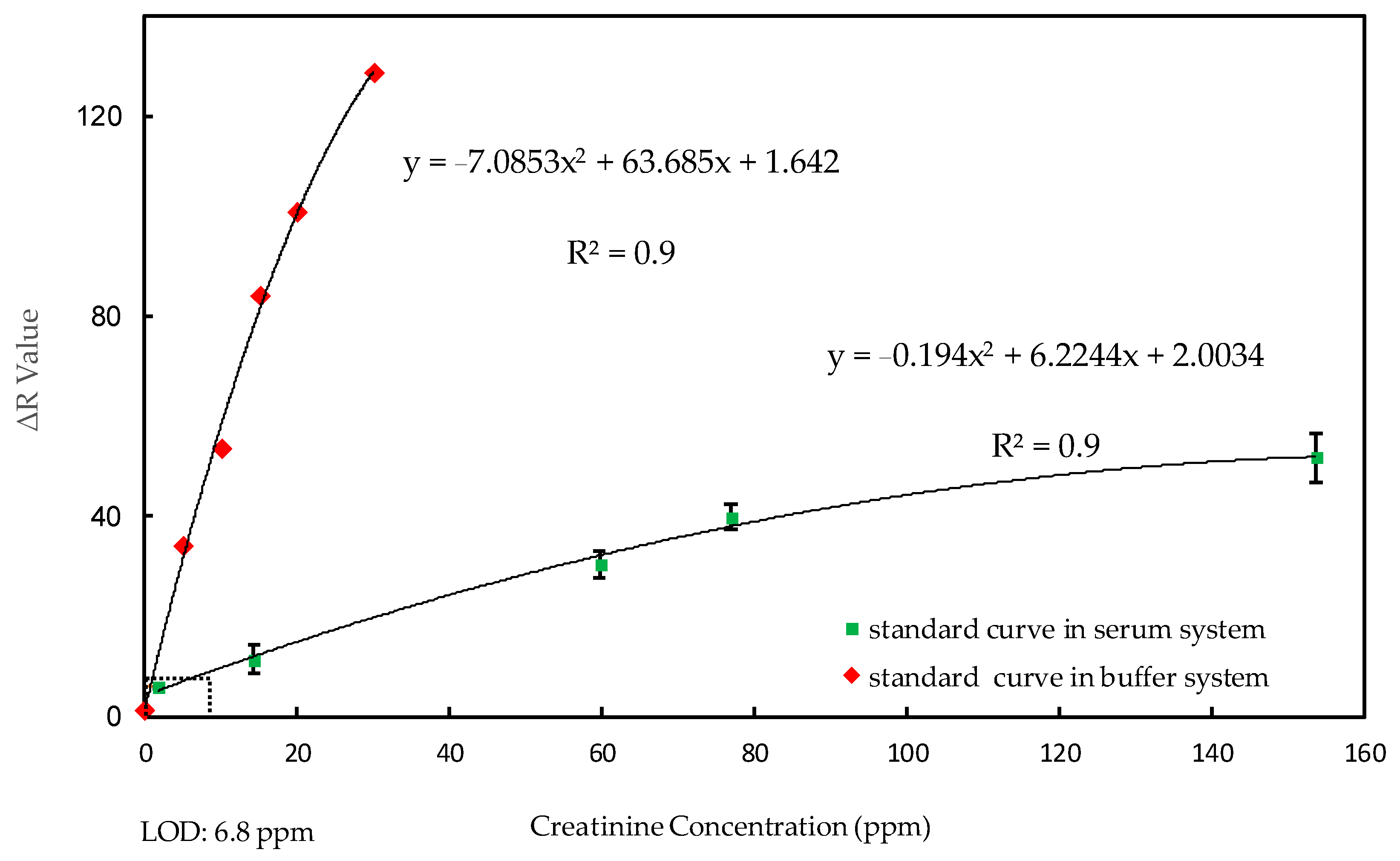
3.2. Creatinine Standard Curve in Serum and Buffer Systems
3.3. 2-in-1 PADs Performance
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wesseling, C.; De Joode, B.V.W.; Ruepert, C.; León, C.; Monge, P.; Hermosillo, H.; Partanen, L.J. Paraquat in developing countries. Int. J. Occup. Environ. Health 2001, 7, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Wesseling, C.; Corriols, M.; Bravo, V. Acute pesticide poisoning and pesticide registration in central America. Toxicol. Appl. Pharmacol. 2005, 207, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.W.; Lin, J.L.; Lin-Tan, D.T.; Chen, K.H.; Yen, T.H.; Wu, M.S.; Lin, S.C. Early hemoperfusion may improve survival of severely paraquat-poisoned patients. PLoS ONE 2012, 7, e48397. [Google Scholar] [CrossRef] [PubMed]
- Wei, T.Y.; Yen, T.H.; Cheng, C.M. Point-of-care testing in the early diagnosis of acute pesticide intoxication: The example of paraquat. Biomicrofluidics 2018, 12, 011501. [Google Scholar] [CrossRef] [PubMed]
- Seok, S.J.; Gil, H.W.; Jeong, D.S.; Yang, J.O.; Lee, E.Y.; Hong, S.Y. Paraquat intoxication in subjects who attempt suicide: Why they chose paraquat. Korean J. Int. Med. 2009, 24, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Kuan, C.M.; Lin, S.T.; Yen, T.H.; Wang, Y.L.; Cheng, C.M. Paper-based diagnostic devices for clinical paraquat poisoning diagnosis. Biomicrofluidics 2016, 10, 034118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weng, C.H.; Hu, C.C.; Lin, J.L.; Lin-Tan, D.T.; Hsu, C.W.; Yen, T.H. Predictors of acute respiratory distress syndrome in patients with paraquat intoxication. PLoS ONE 2013, 8, e82695. [Google Scholar] [CrossRef] [PubMed]
- Sittipunt, C. Paraquat poisoning. Respir. Care 2005, 50, 383–385. [Google Scholar] [PubMed]
- Pond, S.M.; Rivory, L.P.; Hampson, E.C.; Roberts, M.S. Kinetics of toxic doses of paraquat and the effects of hemoperfusion in the dog. J. Toxicol. Clin. Toxicol. 1993, 31, 229–246. [Google Scholar] [CrossRef] [PubMed]
- Suntres, Z.E. Role of antioxidants in paraquat toxicity. Toxicology 2002, 180, 65–77. [Google Scholar] [CrossRef]
- Weng, C.H.; Chen, H.H.; Hu, C.C.; Huang, W.H.; Hsu, C.W.; Fu, J.F.; Lin, W.R.; Wang, I.K.; Yen, T.H. Predictors of acute kidney injury after paraquat intoxication. Oncotarget 2017, 8, 51345–51354. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.L.; Lin-Tan, D.T.; Chen, K.H.; Huang, W.H.; Hsu, C.W.; Hsu, H.H.; Yen, T.H. Improved survival in severe paraquat poisoning with repeated pulse therapy of cyclophosphamide and steroids. Intensiv. Care Med. 2011, 37, 1006–1013. [Google Scholar] [CrossRef] [PubMed]
- Lanaro, R.; Costa, J.L.; Fernandes, L.C.; Resende, R.R.; Tavares, M.F. Detection of paraquat in oral fluid, plasma, and urine by capillary electrophoresis for diagnosis of acute poisoning. J. Anal. Toxicol. 2011, 35, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Proudfoot, A.T.; Stewart, M.S.; Levitt, T.; Widdop, B. Paraquat poisoning: Significance of plasma-paraquat concentrations. Lancet 1979, 2, 330–332. [Google Scholar] [CrossRef]
- Sawada, Y.; Yamamoto, I.; Hirokane, T.; Nagai, Y.; Satoh, Y.; Ueyama, M. Severity index of paraquat poisoning. Lancet 1988, 1, 1333. [Google Scholar] [CrossRef]
- Li, C.B.; Li, X.H.; Wang, Z.; Jiang, C.H.; Peng, A. Serum paraquat concentration detected by spectrophotometry in patients with paraquat poisoning. World J. Emerg. Med. 2011, 2, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Koo, J.R.; Yoon, J.W.; Han, S.J.; Choi, M.J.; Park, I.I.; Lee, Y.K.; Kim, S.G.; Oh, J.E.; Seo, J.W.; Kim, H.J.; et al. Rapid analysis of plasma paraquat using sodium dithionite as a predictor of outcome in acute paraquat poisoning. Am. J. Med. Sci. 2009, 338, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Croes, K.; Martens, F.; Desmet, K. Quantitation of paraquat in serum by HPLC. J. Anal. Toxicol. 1993, 17, 310–312. [Google Scholar] [CrossRef] [PubMed]
- De Almeida, R.M.; Yonamine, M. Gas chromatographic-mass spectrometric method for the determination of the herbicides paraquat and diquat in plasma and urine samples. J. Chromatogr. B 2007, 853, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Vinner, E.; Stievenart, M.; Humbert, L.; Mathieu, D.; Lhermitte, M. Separation and quantification of paraquat and diquat in serum and urine by capillary electrophoresis. Biomed. Chromatogr. 2001, 15, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Koivunen, M.E.; Gee, S.J.; Park, E.K.; Lee, K.; Schenker, M.B.; Hammock, B.D. Application of an enzyme-linked immunosorbent assay for the analysis of paraquat in human-exposure samples. Arch. Environ. Contam. Toxicol. 2005, 48, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Gao, R.; Choi, N.; Chang, S.I.; Kang, S.H.; Song, J.M.; Cho, S.I.; Lim, D.W.; Choo, J. Highly sensitive trace analysis of paraquat using a surfaceenhanced Raman scattering microdroplet sensor. Anal. Chim. Acta 2010, 681, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.R.; Li, Q.Q.; Ren, Y.L.; Geng, J.P.; Cao, P.; Sui, T.; Wang, X.; Du, Y.P. Surface enhanced Raman spectroscopy signals of mixed pesticides and their identification. Chin. Chem. Lett. 2011, 22, 1477–1480. [Google Scholar] [CrossRef]
- Fang, H.; Zhang, X.; Zhang, S.J.; Liu, L.; Zhao, Y.M.; Xu, H.J. Ultrasensitive and quantitative detection of paraquat on fruits skins via surface-enhanced Raman spectroscopy. Sens. Actuators B Chem. 2015, 213, 452–456. [Google Scholar] [CrossRef] [Green Version]
- Dao, T.C.; Luong, T.Q.N.; Cao, T.A.; Nguyen, N.H.; Kieu, N.M.; Luong, T.T. Trace detection of herbicides by SERS technique, using SERS-active substrates fabricated from different silver nanostructures deposited on silicon. Adv. Nat. Sci. Nanosci. Nanotechnol. 2015, 6, 035012. [Google Scholar] [CrossRef] [Green Version]
- Randviir, E.P.; Banks, C.E. Analytical methods for quantifying creatinine within biological media. Sens. Actuators B Chem. 2013, 183, 239–252. [Google Scholar] [CrossRef]
- Cappuccio, F.P.; Buchanan, L.A.; Ji, C.; Siani, A.; Miller, M.A. Systematic review and meta-analysis of randomised controlled trials on the effects of potassium supplements on serum potassium and creatinine. BMJ Open 2016, 6, e011716. [Google Scholar] [CrossRef] [PubMed]
- Pavan, M. Acute kidney injury following Paraquat poisoning in India. Iran. J. Kidney Dis. 2013, 7, 64–66. [Google Scholar] [PubMed]
- Gil, H.W.; Hong, J.R.; Jang, S.H.; Hong, S.Y. Diagnostic and therapeutic approach for acute paraquat intoxication. J. Korean Med. Sci. 2014, 29, 1441–1449. [Google Scholar] [CrossRef] [PubMed]
- Yetisen, A.K.; Akram, M.S.; Lowe, C.R. Paper-based microfluidic point-of care diagnostic devices. Lab Chip 2013, 13, 2210–2251. [Google Scholar] [CrossRef] [PubMed]
- Pollock, N.R.; Rolland, J.P.; Kumar, S.; Beattie, P.D.; Jain, S.; Noubary, F.; Wong, V.L.; Pohlmann, R.A.; Ryan, U.S.; Whitesides, G.M. A paper-based multiplexed transaminase test for low cost, point-of-care liver function testing. Sci. Trans. Med. 2012, 4, 152ra129. [Google Scholar] [CrossRef] [PubMed]
- Hsu, M.Y.; Yang, C.Y.; Hsu, W.H.; Lin, K.H.; Wang, C.Y.; Shen, Y.C.; Chen, Y.C.; Chau, S.F.; Cheng, C.M. Monitoring the VEGF level in aqueous humor of patients with ophthalmologically relevant diseases via ultrahigh sensitive paper-based ELISA. Biomaterials 2014, 35, 3729–3735. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.K.; Huang, H.Y.; Chen, W.R.; Nishie, W.; Ujiie, H.; Natsuga, K.; Fanll, S.T.; Wang, H.K.; Lee, J.Y.Y.; Tsai, W.L.; et al. Paper-based ELISA for the detection of autoimmune antibodies in body fluid-the case of bullous pemphigoid. Anal. Chem. 2014, 86, 4605–4610. [Google Scholar] [CrossRef] [PubMed]
- Murdock, R.C.; Shen, L.; Griffin, D.K.; Kelley-Loughnane, N.; Papautsky, I.; Hagen, J.A. Optimization of a paper-based ELISA for a human performance biomarker. Anal. Chem. 2013, 85, 11634–11642. [Google Scholar] [CrossRef] [PubMed]
- Evans, G.O. The use of an enzymatic kit to measure plasma creatinine in the mouse and 3 other species. Comp. Biochem. Phys. B 1986, 85, 193–195. [Google Scholar] [CrossRef]
- Young, D.S.; Pestaner, L.C.; Gibberman, V. Effects of drugs on clinical laboratory tests. Ann. Clin. Chem. 1997, 34, 579–581. [Google Scholar] [CrossRef] [PubMed]
- Nilghaz, A.; Guan, L.; Tan, W.; Shen, W. Advances of paper-based microfluidics for diagnostics—The original motivation and current status. ACS Sens. 2016, 1, 1382–1393. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2-in-1 μPADs | Paraquat (ppm) | Creatinine (ppm) | |||
|---|---|---|---|---|---|
| Our Value | Hospital | Our Value | Hospital | ||
| T1 |  | 22.59 | >10 | 16.10 | 19.3 |
| T2 |  | 5.99 | 5.1 | 12.92 | 13.3 |
| T3 |  | 26.52 | >10 | 13.82 | 14.4 |
| T4 |  | 35.19 | >10 | 13.58 | 14.3 |
| T5 |  | 25.0 | >10 | 12.20 | 12.6 |
| Patient Number | Age | Sex | Time between Paraquat Ingestion and Hospital Arrival (h) | Blood Paraquat Level (ppm) | Severiry Index of Paraquat Poisoning (ppm) | Blood Creatinine Level (ppm) | Treatment | Duration of Hospitalization (day) | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| T1 | 50 | M | 6 | 10 | 60 | 19.3 | Hemoperfusion cytotoxic agent, glucocorticoid | 1 | Dead |
| T2 | 62 | M | 6 | 5.11 | 30.66 | 13.3 | Hemoperfusion cytotoxic agent, glucocorticoid | 1 | Dead |
| T3 | 43 | M | 2 | 10 | 20 | 14.4 | Hemoperfusion cytotoxic agent, glucocorticoid | 1 | Dead |
| T4 | 87 | M | 2 | 10 | 20 | 14.3 | Hemoperfusion cytotoxic agent, glucocorticoid | 1 | Dead |
| T5 | 50 | M | 24 | 10 | 240 | 12.6 | Hemoperfusion cytotoxic agent, glucocorticoid | 3 | Dead |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, T.-H.; Tung, K.-H.; Gu, P.-W.; Yen, T.-H.; Cheng, C.-M. Rapid Simultaneous Determination of Paraquat and Creatinine in Human Serum Using a Piece of Paper. Micromachines 2018, 9, 586. https://doi.org/10.3390/mi9110586
Chang T-H, Tung K-H, Gu P-W, Yen T-H, Cheng C-M. Rapid Simultaneous Determination of Paraquat and Creatinine in Human Serum Using a Piece of Paper. Micromachines. 2018; 9(11):586. https://doi.org/10.3390/mi9110586
Chicago/Turabian StyleChang, Tsui-Hsuan, Kuo-Hao Tung, Po-Wen Gu, Tzung-Hai Yen, and Chao-Min Cheng. 2018. "Rapid Simultaneous Determination of Paraquat and Creatinine in Human Serum Using a Piece of Paper" Micromachines 9, no. 11: 586. https://doi.org/10.3390/mi9110586