
High−Accuracy Film−Integrated Optical Sensor for Real−Time Intraocular Pressure Monitoring

Abstract
:1. Introduction
2. Principle and Design
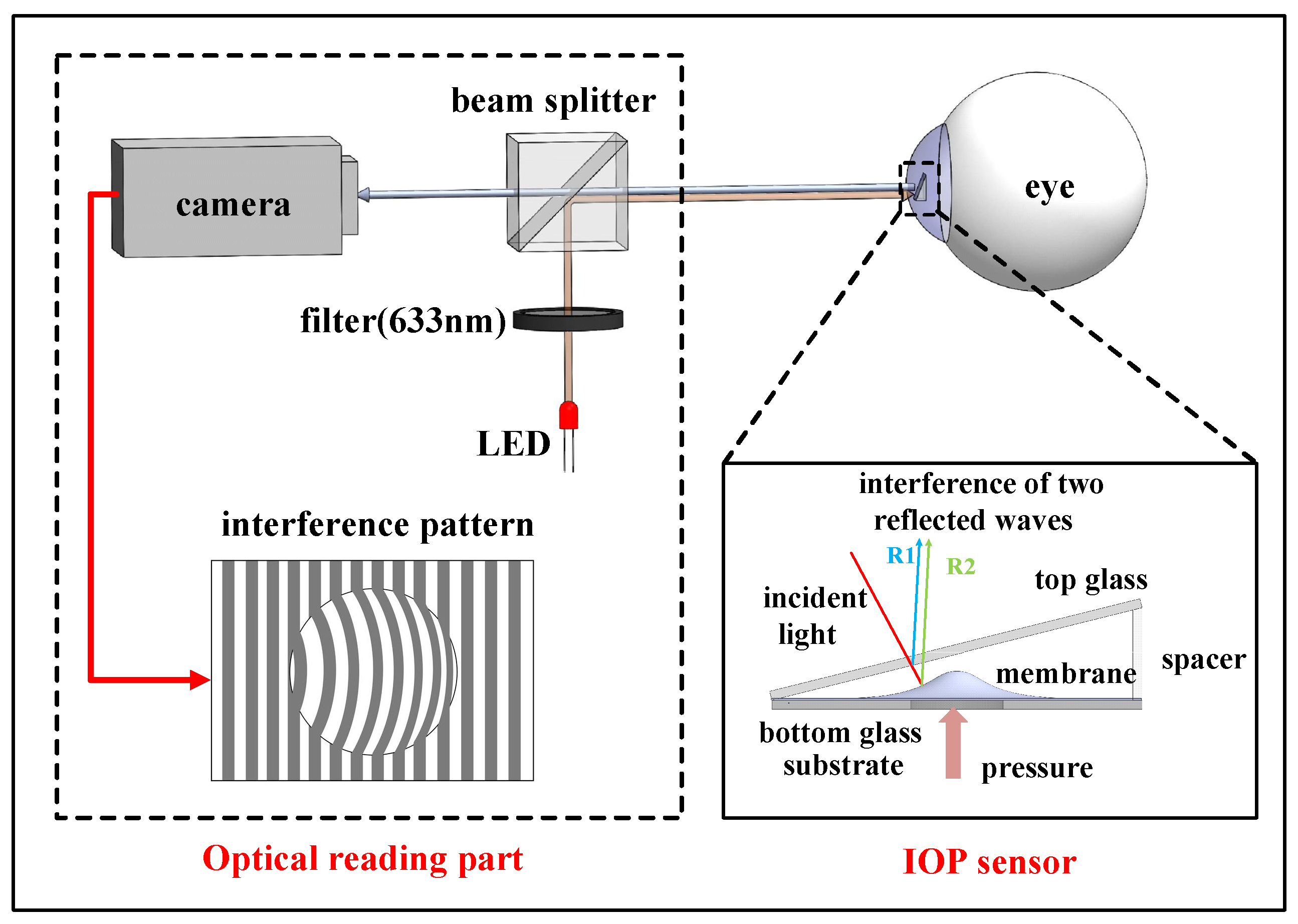
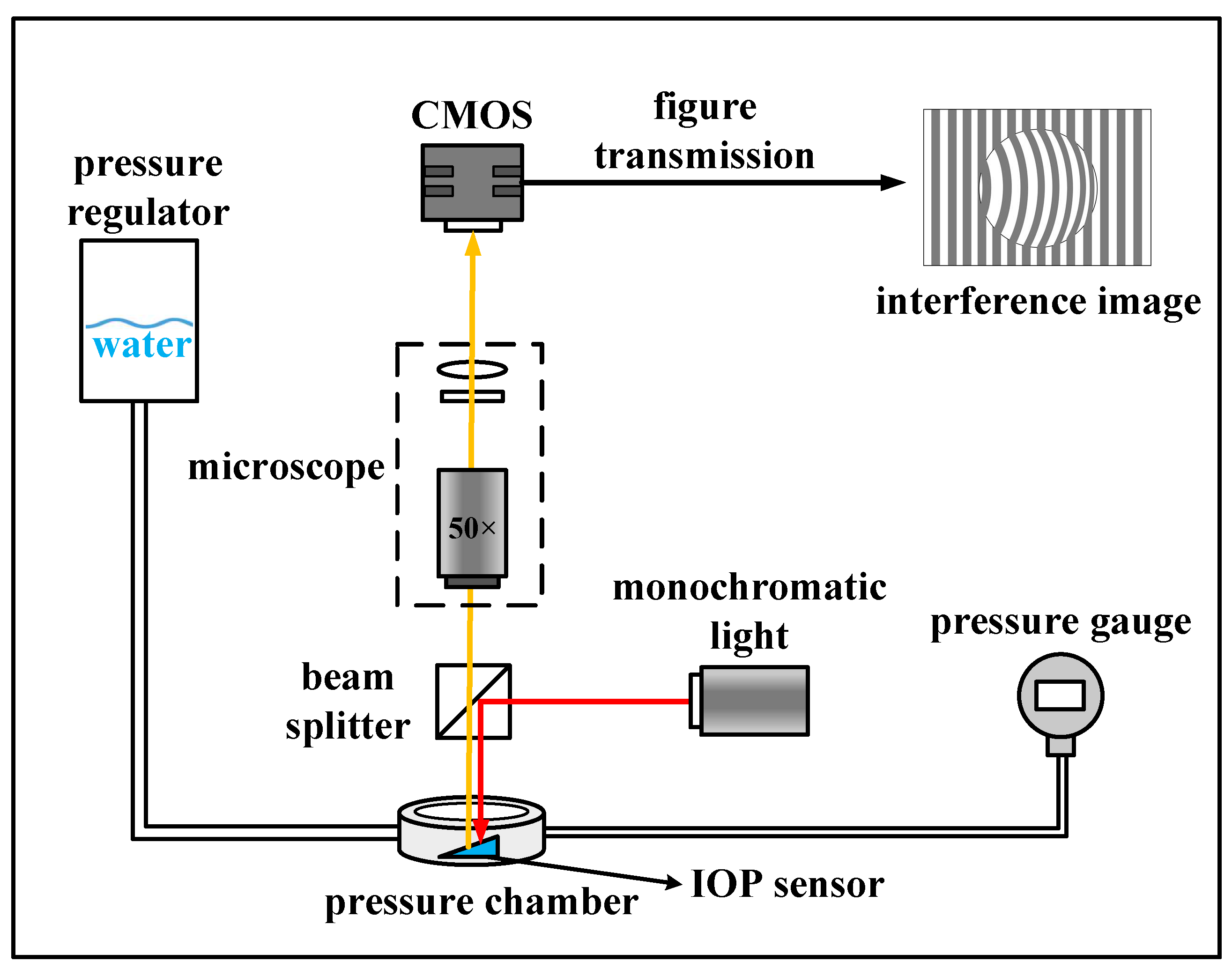
2.1. System Operating Principle
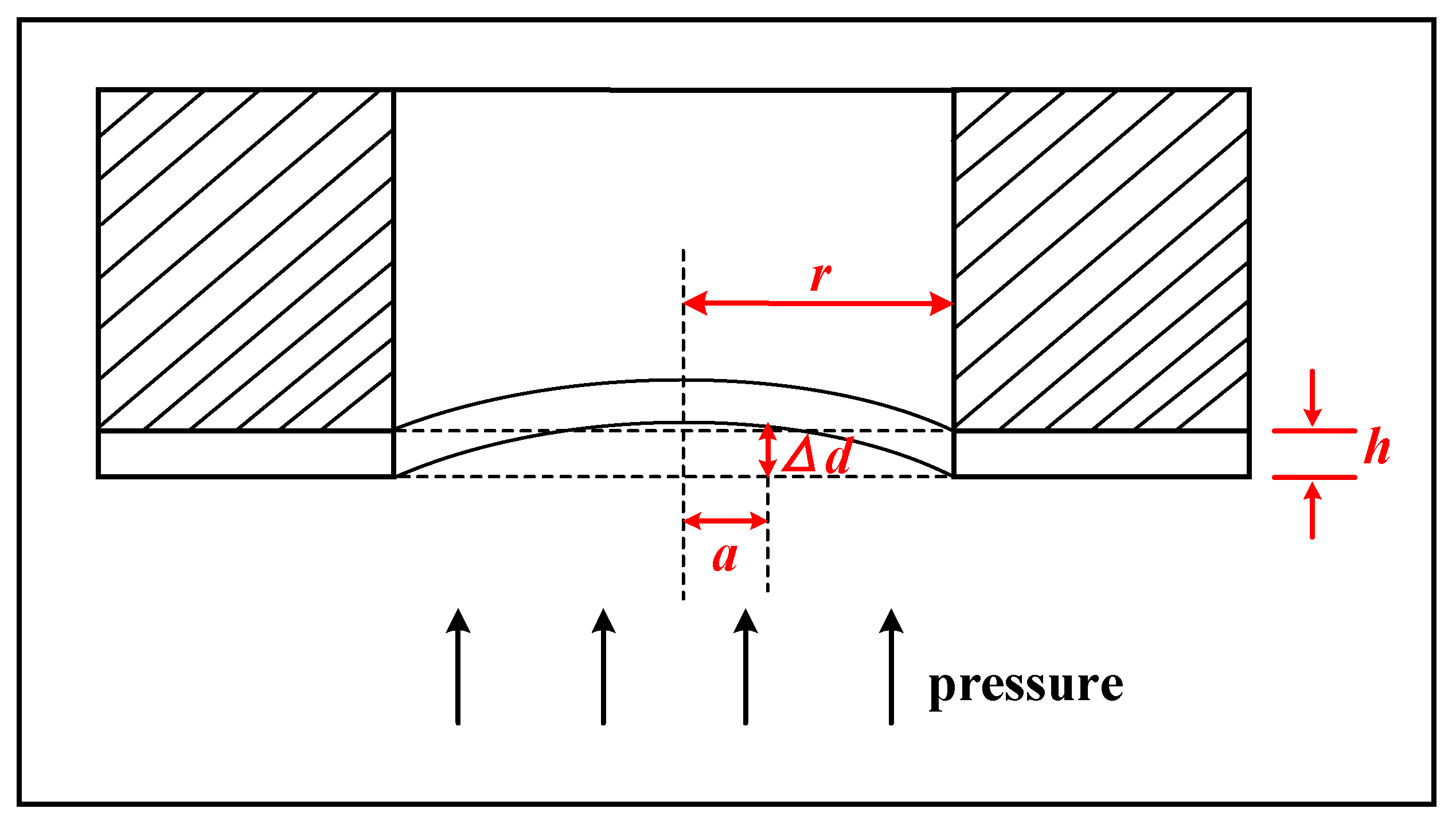
2.2. Design of the IOP Sensor
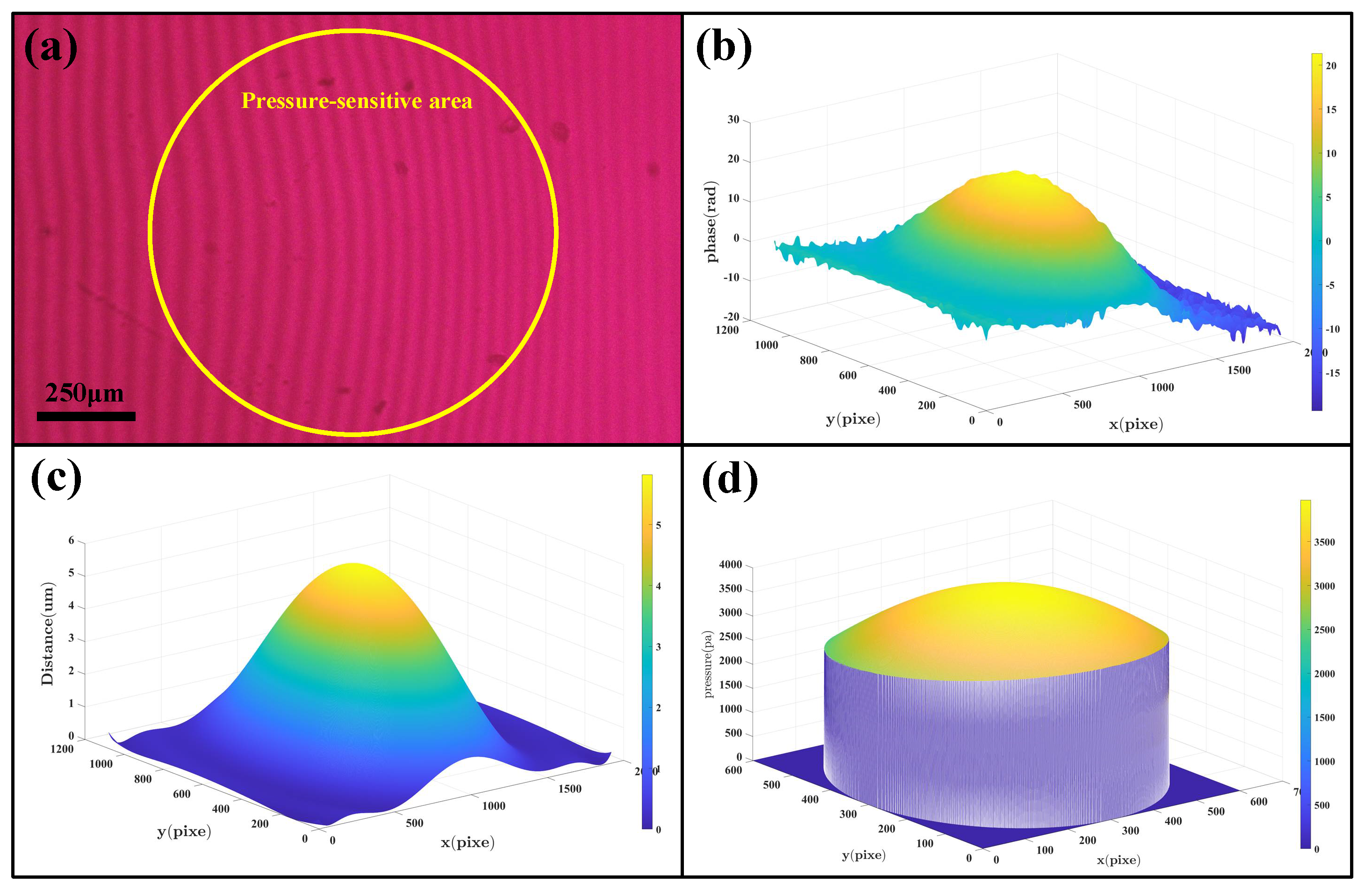
2.3. Algorithm
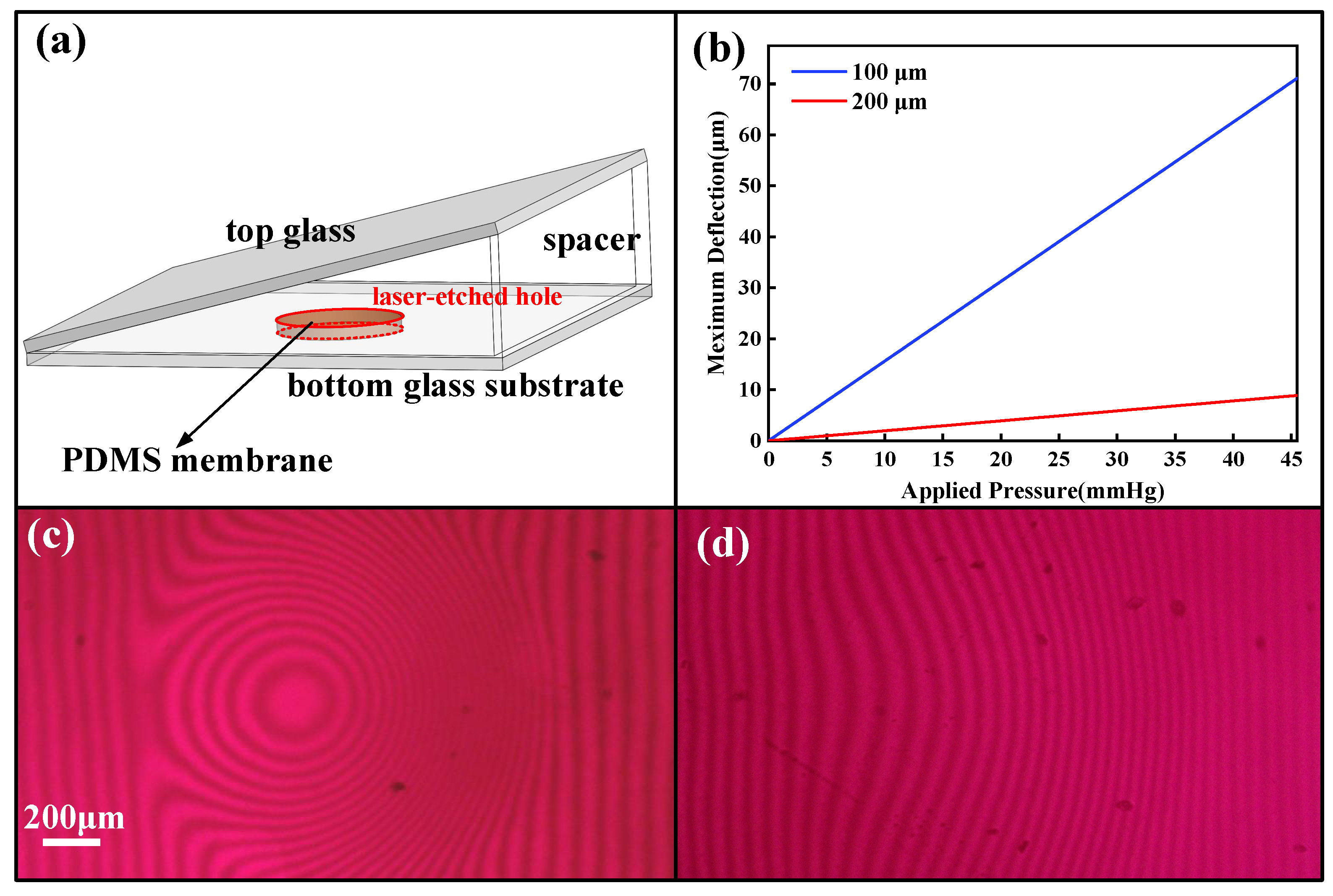
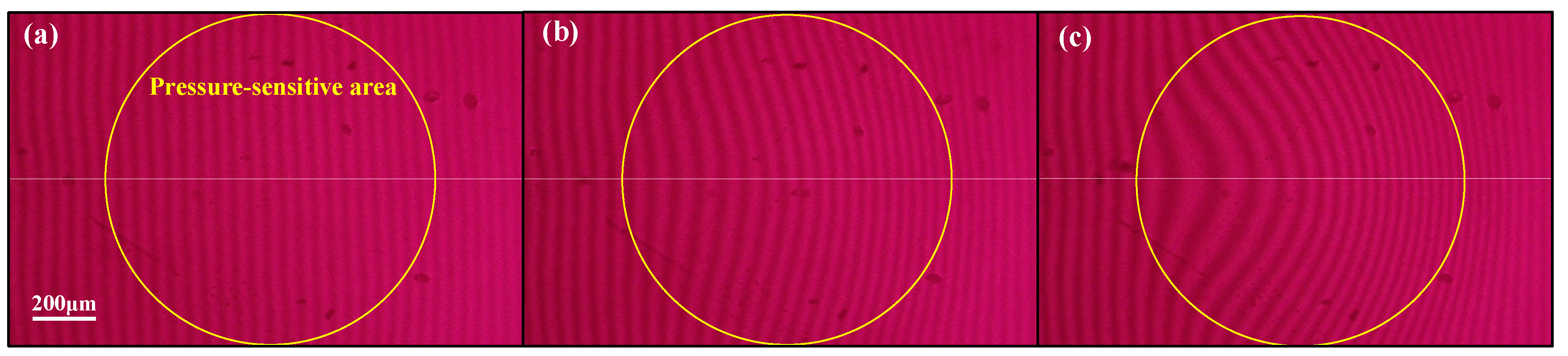
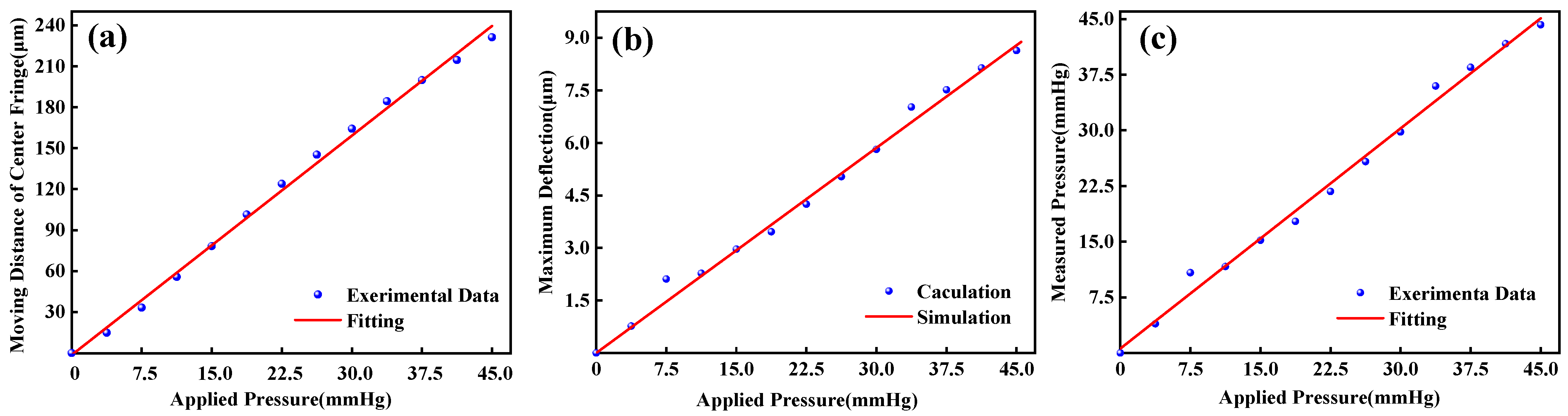
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Flaxman, S.R.; Bourne, R.R.A.; Resnikoff, S.; Ackland, P.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, J.B.; Keeffe, J.; Kempen, J.H.; et al. Global causes of blindness and distance vision impairment 1990–2020: A systematic review and meta−analysis. Lancet Glob. Health 2017, 5, e1221–e1234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta−analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- De Moraes, C.G.V.; Juthani, V.J.; Liebmann, J.M.; Teng, C.C.; Tello, C.; Susanna, R., Jr.; Ritch, R. Risk factors for visual field progression in treated glaucoma. Arch. Ophthalmol. 2011, 129, 562–568. [Google Scholar] [CrossRef] [Green Version]
- Bengtsson, B.; Leske, M.C.; Hyman, L.; Heijl, A.; Early Manifest Glaucoma Trial, G. Fluctuation of intraocular pressure and glaucoma progression in the early manifest glaucoma trial. Ophthalmology 2007, 114, 205–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.W.L.L.H. Application progress of tonometer in clinic. Chin. J. Mod. Nurs. 2017, 23, 292–296. [Google Scholar]
- Bhan, A.; Browning, A.C.; Shah, S.; Hamilton, R.; Dave, D.; Dua, H.S. Effect of corneal thickness on intraocular pressure measurements with the pneumotonometer, Goldmann applanation tonometer, and Tono−Pen. Investig. Ophthalmol. Vis. Sci. 2002, 43, 1389–1392. [Google Scholar]
- Mosaed, S.; Liu, J.H.K.; Weinreb, R.N. Correlation between office and peak nocturnal intraocular pressures in healthy subjects and glaucoma patients. Am. J. Ophthalmol. 2005, 139, 320–324. [Google Scholar] [CrossRef]
- Yang, C.; Huang, X.; Li, X.; Yang, C.; Zhang, T.; Wu, Q.; Liu, D.; Lin, H.; Chen, W.; Hu, N.; et al. Wearable and Implantable Intraocular Pressure Biosensors: Recent Progress and Future Prospects. Adv. Sci. 2021, 8, 2002971. [Google Scholar] [CrossRef]
- Kotecha, A.; Elsheikh, A.; Roberts, C.R.; Zhu, H.; Garway−Heath, D.F. Corneal thickness− and age−related biomechanical properties of the cornea measured with the ocular response analyzer. Investig. Ophthalmol. Vis. Sci. 2006, 47, 5337–5347. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Kim, M.; Lee, M.S.; Kim, K.; Ji, S.; Kim, Y.T.; Park, J.; Na, K.; Bae, K.H.; Kyun Kim, H.J.N.C. Wearable smart sensor systems integrated on soft contact lenses for wireless ocular diagnostics. Nat. Commun. 2017, 8, 14997. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.J.; Saati, S.; Varma, R.; Humayun, M.S.; Tai, Y.C.J.J.o.M.S. Wireless Intraocular Pressure Sensing Using Microfabricated Minimally Invasive Flexible−Coiled LC Sensor Implant. J. Microelectromech. Syst. 2010, 19, 721–734. [Google Scholar] [CrossRef] [Green Version]
- Chen, G.Z.; Chan, I.S.; Lam, D.J.S.; Physical, A.A. Capacitive contact lens sensor for continuous non−invasive intraocular pressure monitoring. Sens. Actuators A Phys. 2013, 203, 112–118. [Google Scholar] [CrossRef]
- Chen, P.J.; Rodger, D.C.; Saati, S.; Humayun, M.S.; Tai, Y.C. Microfabricated Implantable Parylene−Based Wireless Passive Intraocular Pressure Sensors. J. Microelectromech. Syst. 2008, 17, 1342–1351. [Google Scholar] [CrossRef]
- Chen, G.Z.; Chan, I.S.; Leung, L.K.; Lam, D.C. Soft wearable contact lens sensor for continuous intraocular pressure monitoring. Med. Eng. Phys. 2014, 36, 1134–1139. [Google Scholar] [CrossRef] [PubMed]
- Katuri, K. Design and Optimization of Passive Wireless Intraocular Pressure Sensor; North Carolina State University: Raleigh, NC, USA, 2012. [Google Scholar]
- Kouhani, M.H.M.; Weber, A.; Li, W. Wireless intraocular pressure sensor using stretchable variable inductor. In Proceedings of the 2017 IEEE 30th International Conference on Micro Electro Mechanical Systems (MEMS), Las Vegas, NV, USA, 22–26 January 2017; pp. 557–560. [Google Scholar]
- Akar, O.; Akin, T.; Najafi, K. A wireless batch sealed absolute capacitive pressure sensor. Sens. Actuators A Phys. 2001, 95, 29–38. [Google Scholar] [CrossRef]
- Kouhani, M.H.M.; Wu, J.; Tavakoli, A.; Weber, A.J.; Li, W. Wireless, passive strain sensor in a doughnut−shaped contact lens for continuous non−invasive self−monitoring of intraocular pressure. Lab Chip 2020, 20, 332–342. [Google Scholar] [CrossRef]
- Li, B.C.W. Parylene−based fold−and−bond wireless pressure sensor. In Proceedings of the 8th Annual IEEE International Conference on Nano/Micro Engineered and Molecular Systems, Suzhou, China, 7–10 April 2013. [Google Scholar]
- Chen, P.J.; Rodger, D.C.; Saati, S.; Humayun, M.S.; Tai, Y.C. Implantable parylene−based wireless intraocular pressure sensor. In Proceedings of the IEEE 2008 IEEE 21st International Conference on Micro Electro Mechanical Systems, Tucson, AZ, USA, 13–17 January 2008. [Google Scholar]
- Todani, A.; Behlau, I.; Fava, M.A.; Cade, F.; Cherfan, D.G.; Zakka, F.R.; Jakobiec, F.A.; Gao, Y.; Dohlman, C.H.; Melki, S.A. Intraocular pressure measurement by radio wave telemetry. Investig. Ophthalmol. Vis. Sci. 2011, 52, 9573–9580. [Google Scholar] [CrossRef]
- Araci, I.E.; Su, B.; Quake, S.R.; Mandel, Y. An implantable microfluidic device for self−monitoring of intraocular pressure. Nat. Med. 2014, 20, 1074–1078. [Google Scholar] [CrossRef]
- Lee, J.O.; Park, H.; Du, J.; Balakrishna, A.; Chen, O.; Sretavan, D.; Choo, H. A microscale optical implant for continuous in vivo monitoring of intraocular pressure. Microsyst. Nanoeng. 2017, 3, 17057. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, J.; Kwon, Y.H.; Kim, J.J.; Liu, H.; Jiang, H. High Contrast Grating Based Strain Sensor for Intraocular Applications. J. Microelectromech. Syst. 2018, 27, 599–601. [Google Scholar] [CrossRef]
- Phan, A.; Truong, P.; Trumpp, J.; Talke, F.E. Design of an Optical Pressure Measurement System for Intraocular Pressure Monitoring. IEEE Sens. J. 2018, 18, 61–68. [Google Scholar] [CrossRef]
- Giovanni, M. Flat and Corrugated Diaphragm Design Handbook; Marcel Dekker: New York, NY, USA, 1982; pp. 130–154. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Wearable IOP Sensors | Implantable IOP Sensors | ||
|---|---|---|---|
| Ref. | Sensitivity | Ref. | Sensitivity |
| [10] | ~2.2 MHz mmHg−1 | [11] | 243 kHz mmHg−1 |
| [12] | 23 kHz mmHg−1 | [13] | 1.14 MHz mmHg−1 |
| [14] | 8 kHz mmHg−1 | [15] | 119.88 kHz mmHg−1 |
| [16] | 57 kHz mmHg−1 | [17] | 120 kHz mmHg−1 |
| [18] | 35.1 kHz mmHg−1 | [19] | 156 kHz mmHg−1 |
| Ref. | Working Principle | Sensitivity | Accuracy | Merit and Demerit |
|---|---|---|---|---|
| [20] | Inductive | 7000 ppm/mmHg | Not mentioned | Merit: high sensitivity Demerit: non−portability of the external reading device |
| [21] | Capacitive | Not mentioned | 0.81 mmHg | Merit: long−term implantation of IOP detector in animal experimentations will not produce inflammation. Demerit: the size is too large to be implanted in humans’ eye |
| [22] | Microfluidic | 106 μm/mm Hg | 0.5 mmHg | Merit: simple and low−cost Demerit: it is difficult to read out the pressure optically through a hazy cornea |
| [23] | Spectral reflectance | Not mentioned | 0.29 mmHg | Merit: high accuracy Demerit: more complicated and higher−cost fabrication |
| [25] | interferometry | 31 nm/mmHg | 0.3 mmHg | Merit: high accuracy and sensitivity Demerit: more complicated fabrication |
| This work | interferometry | 0.19 μm/mmHg | 0.84 mmHg | Merit: easy fabrication process and low cost |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, X.; Liu, Z.; Wang, L.; Huang, Y.; Yang, H. High−Accuracy Film−Integrated Optical Sensor for Real−Time Intraocular Pressure Monitoring. Micromachines 2023, 14, 353. https://doi.org/10.3390/mi14020353
Xu X, Liu Z, Wang L, Huang Y, Yang H. High−Accuracy Film−Integrated Optical Sensor for Real−Time Intraocular Pressure Monitoring. Micromachines. 2023; 14(2):353. https://doi.org/10.3390/mi14020353
Chicago/Turabian StyleXu, Xiaobin, Zixuan Liu, Liqiang Wang, Yifei Huang, and He Yang. 2023. "High−Accuracy Film−Integrated Optical Sensor for Real−Time Intraocular Pressure Monitoring" Micromachines 14, no. 2: 353. https://doi.org/10.3390/mi14020353