
Design and Development of a Smart IoT-Based Robotic Solution for Wrist Rehabilitation

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Methodology
2.1. Mechanical Design
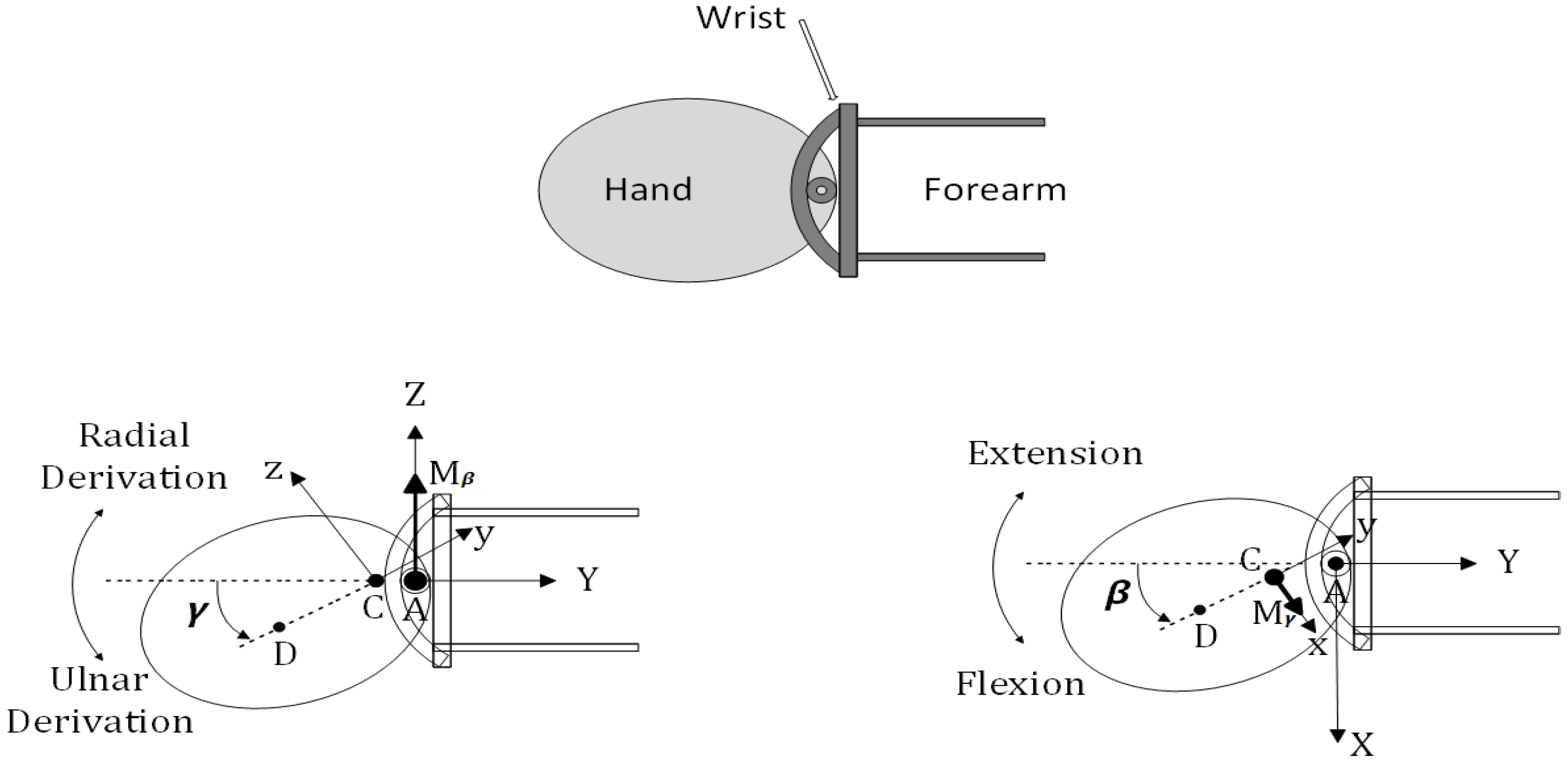
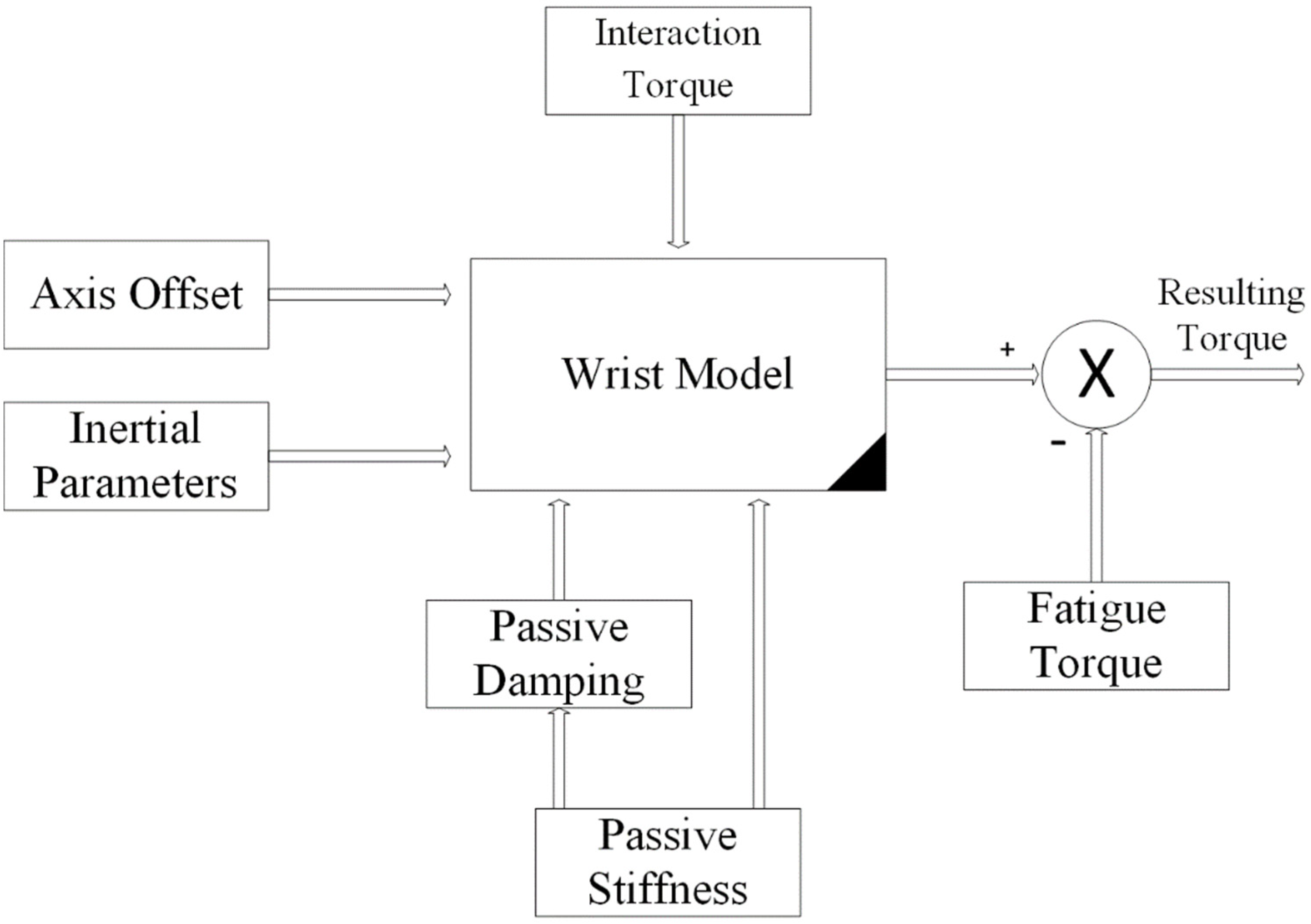
2.2. Second-Order Mechanical Impedance Model of Wrist Rotations
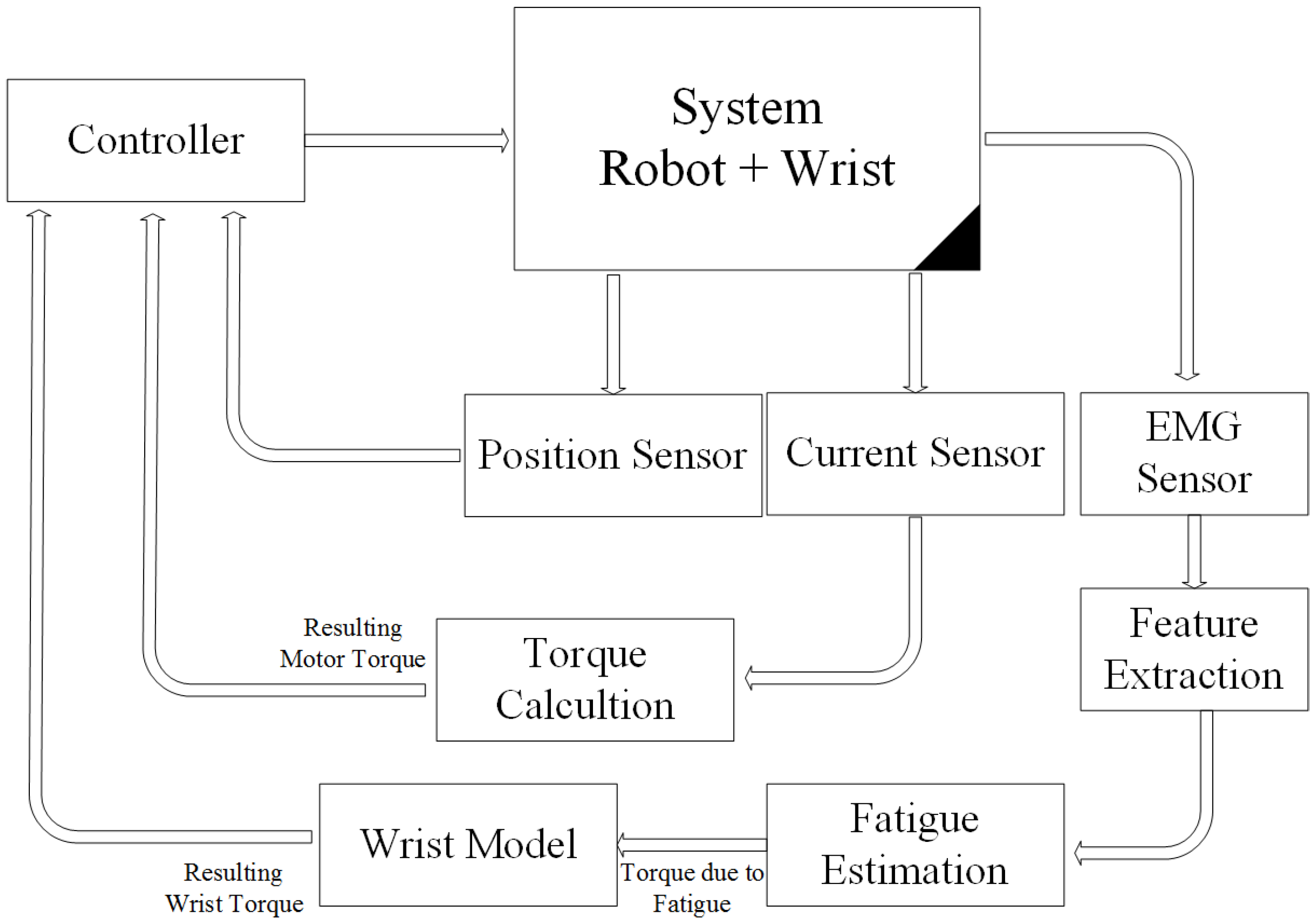
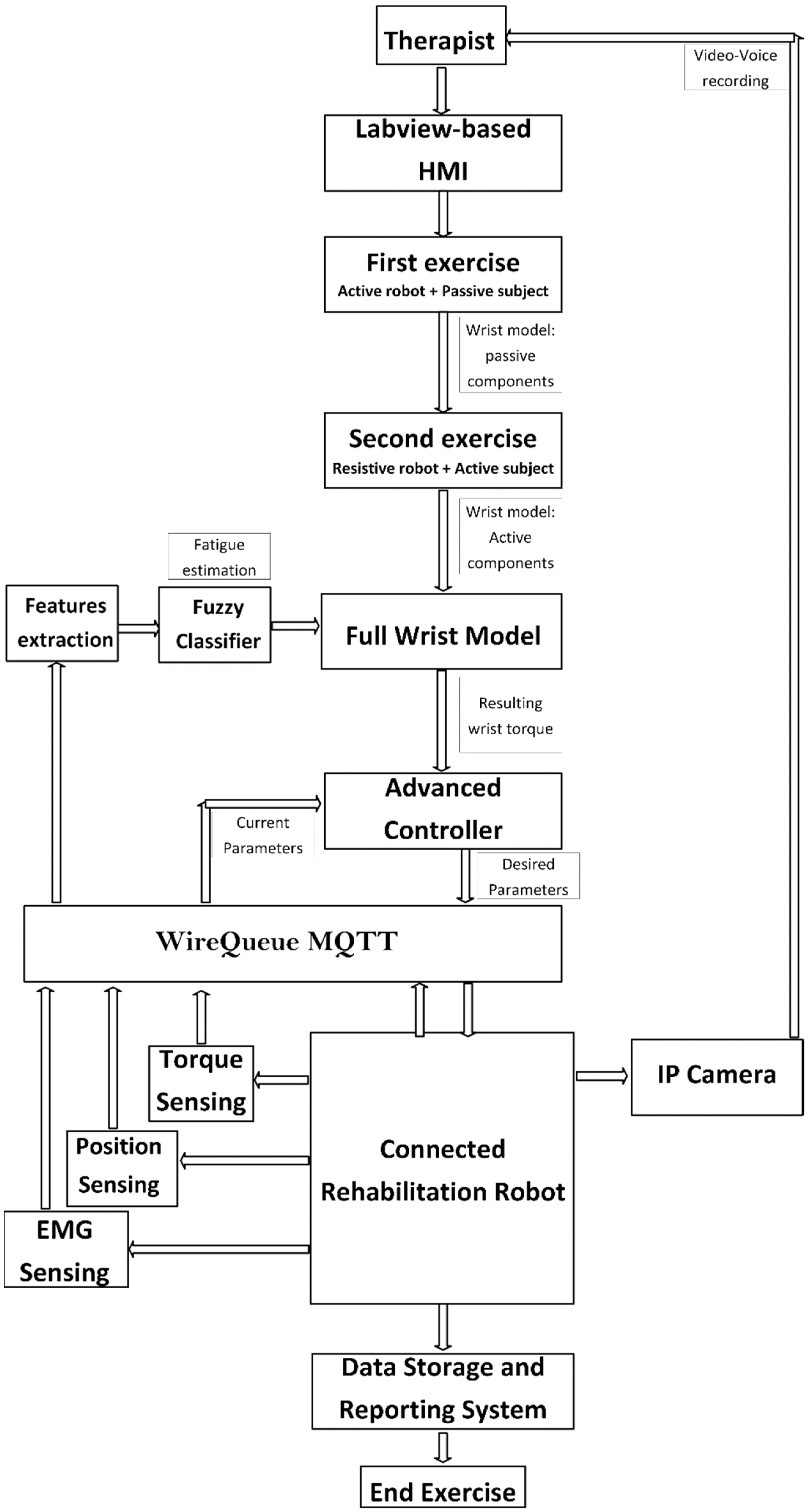
2.3. Control Architecture Design
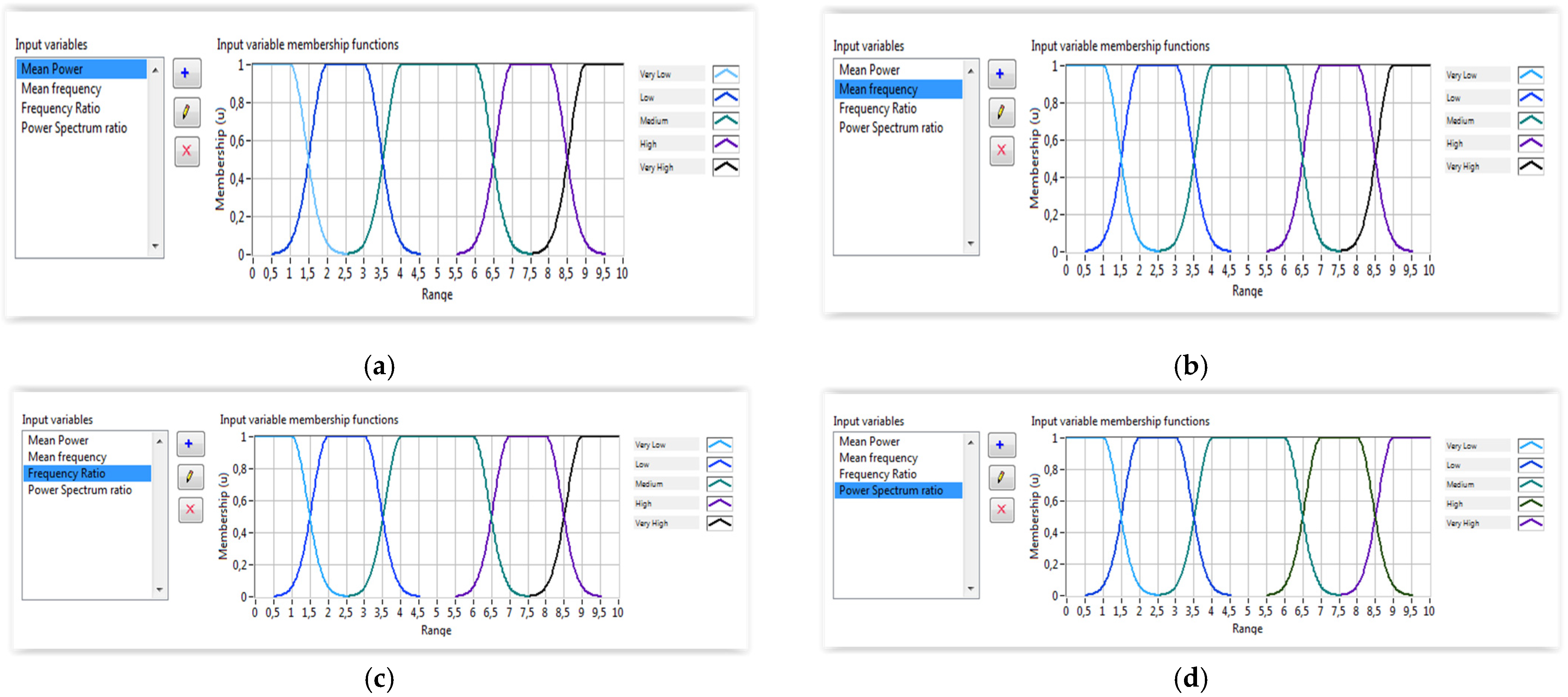
2.3.1. EMG Feature Extraction
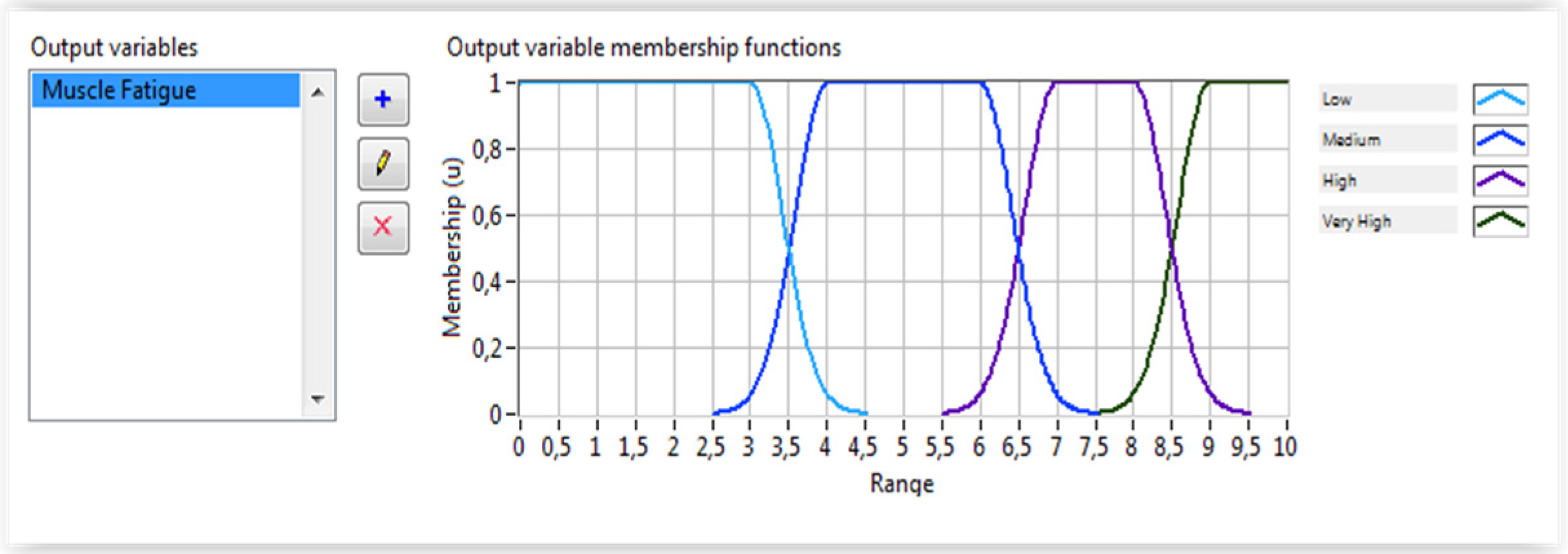
2.3.2. Fuzzy Classifier Algorithm for Fatigue Estimation
2.3.3. Protocol Description
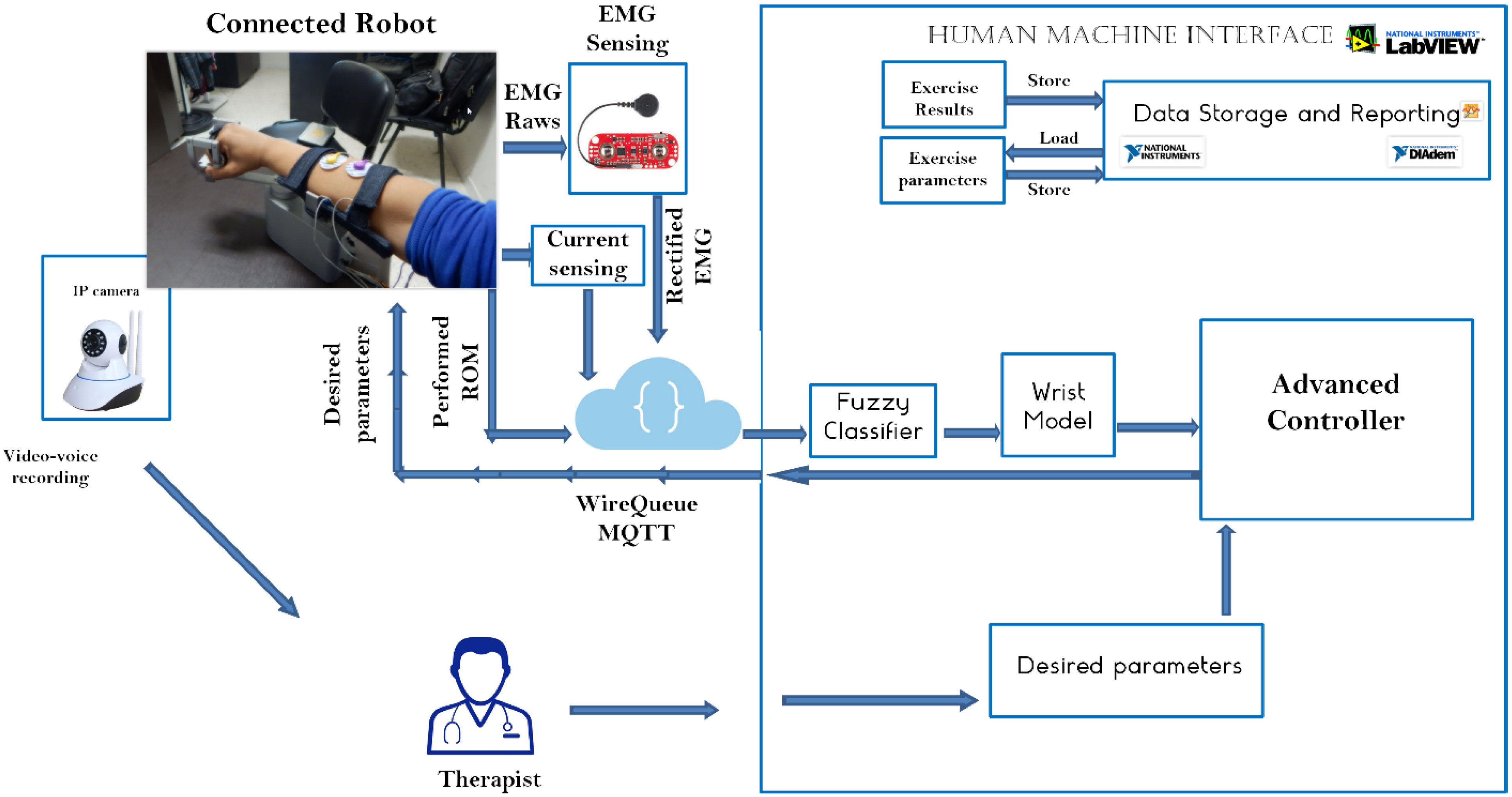
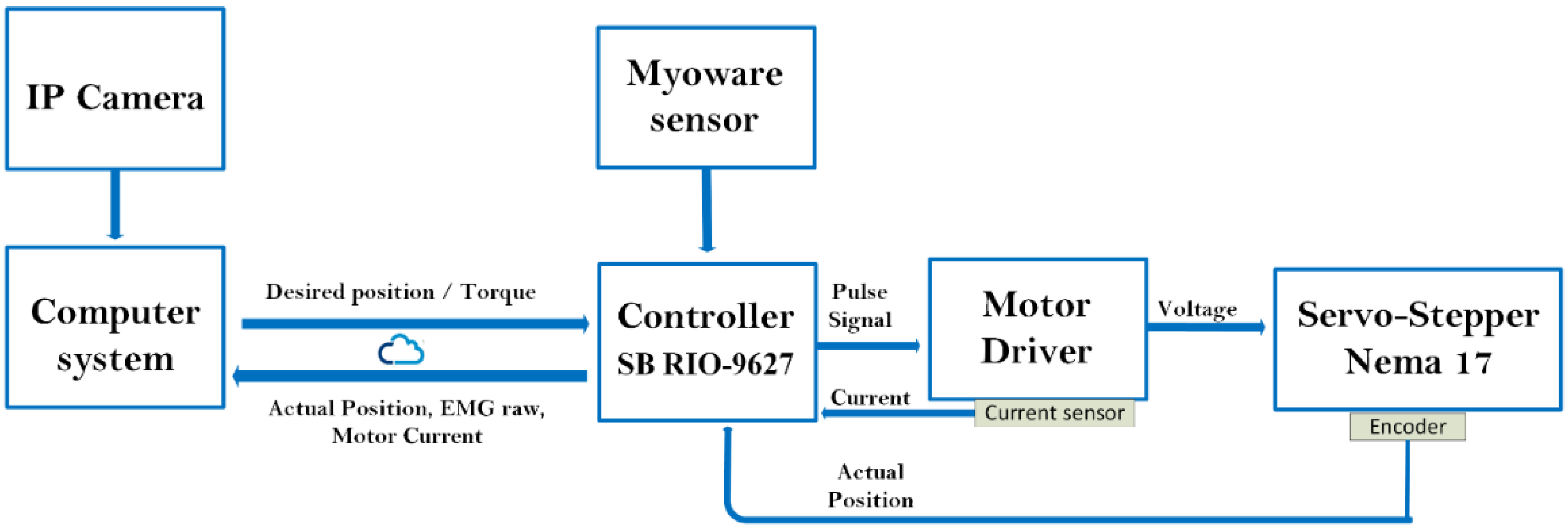
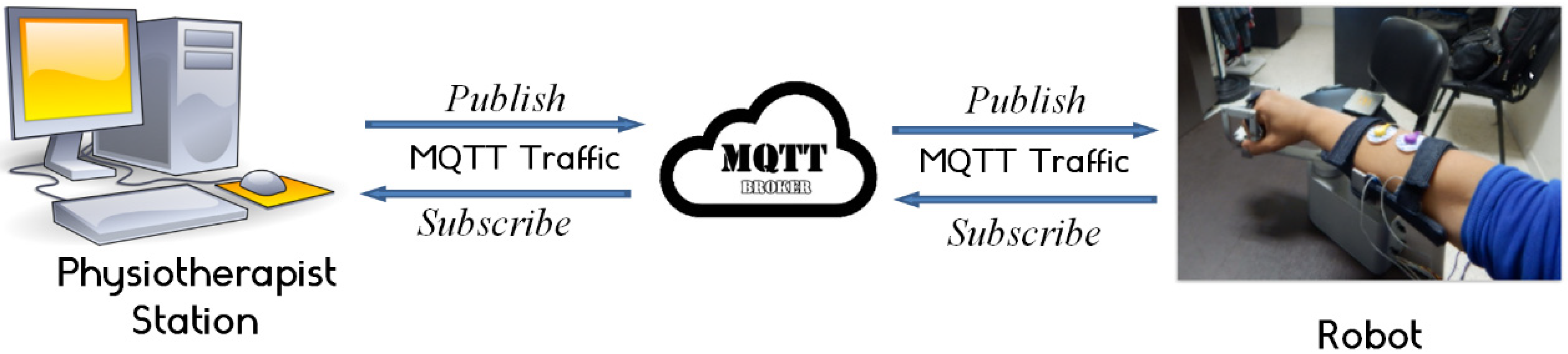
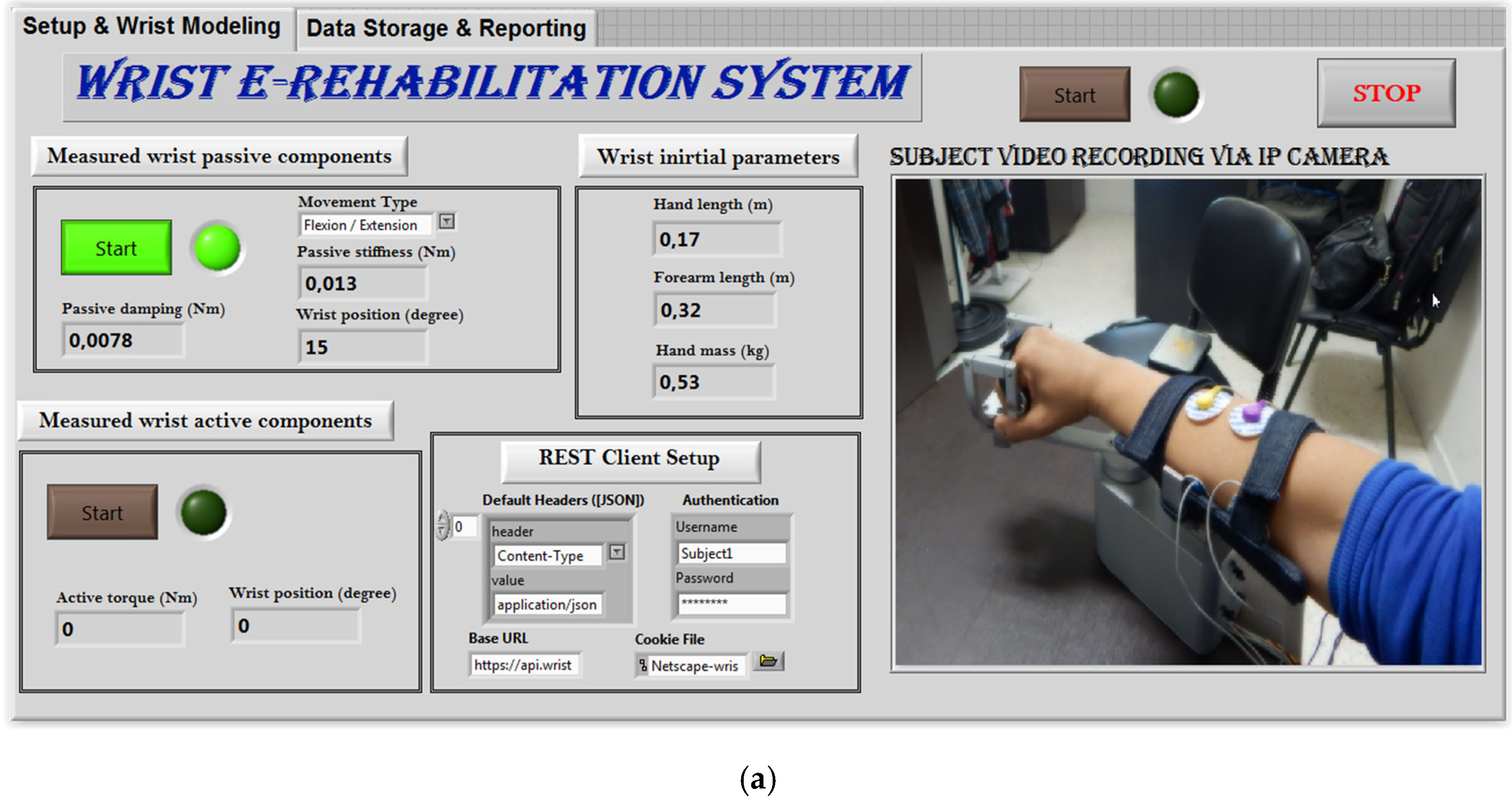
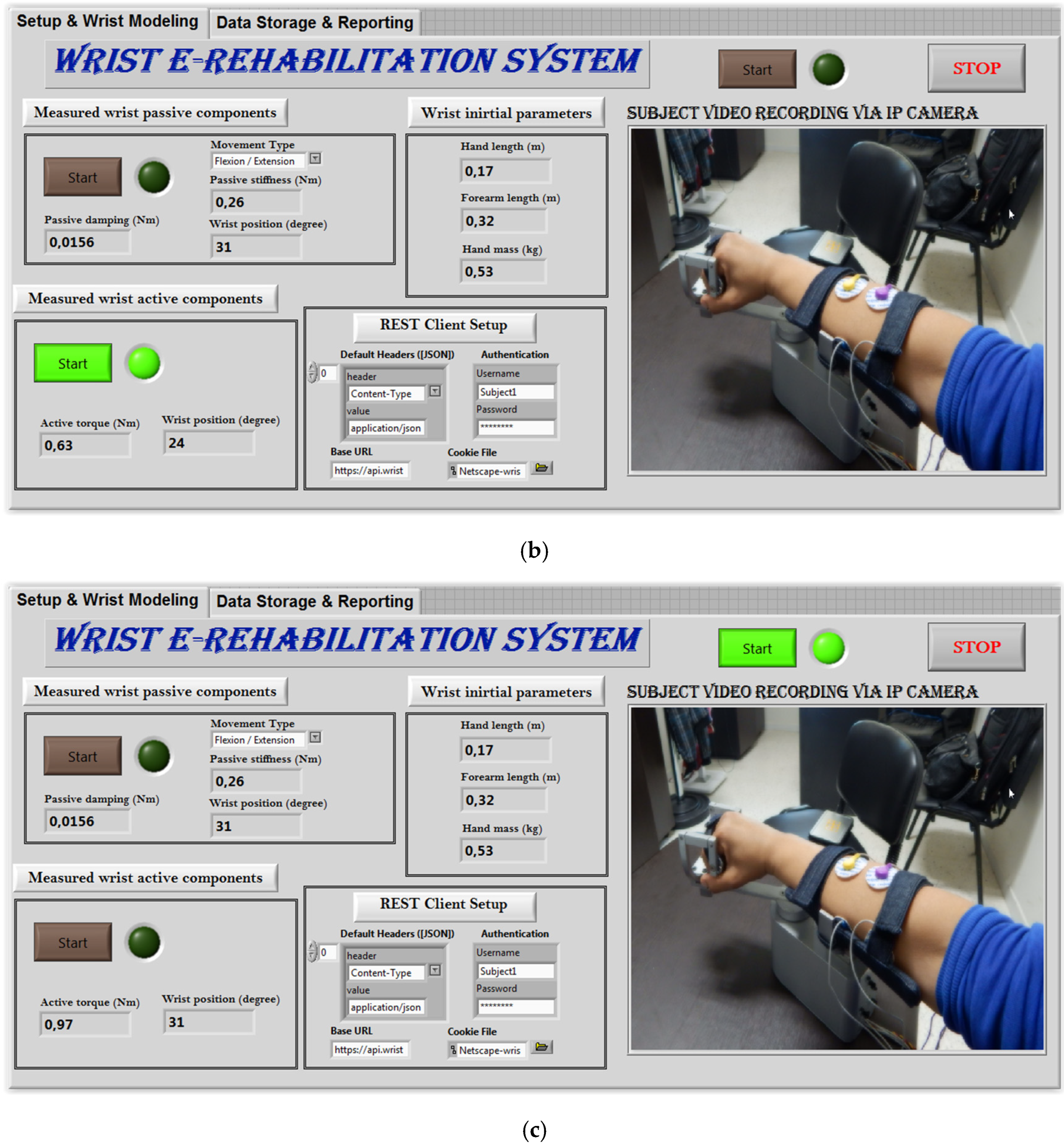
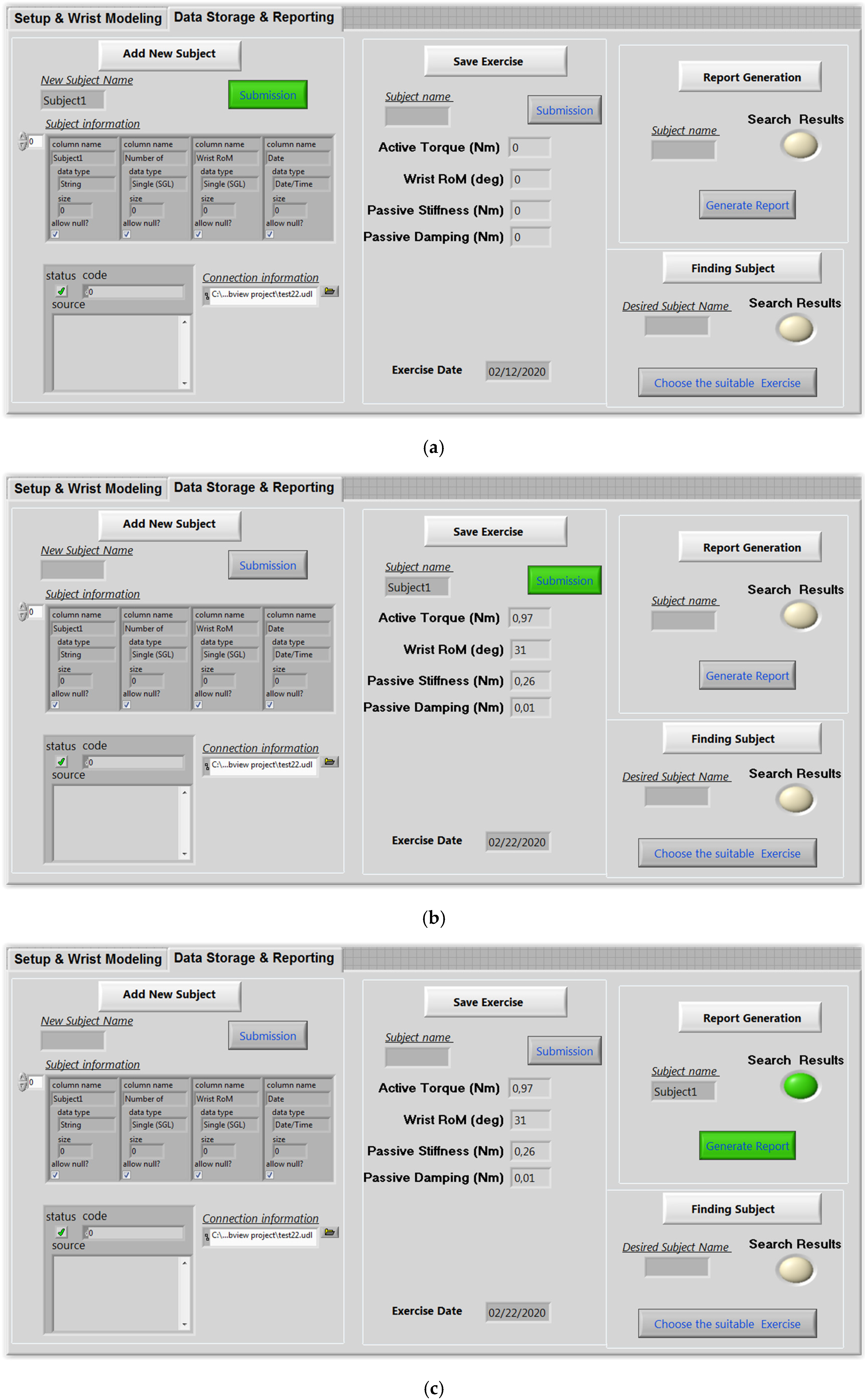
2.3.4. IoT-Based Control Architecture
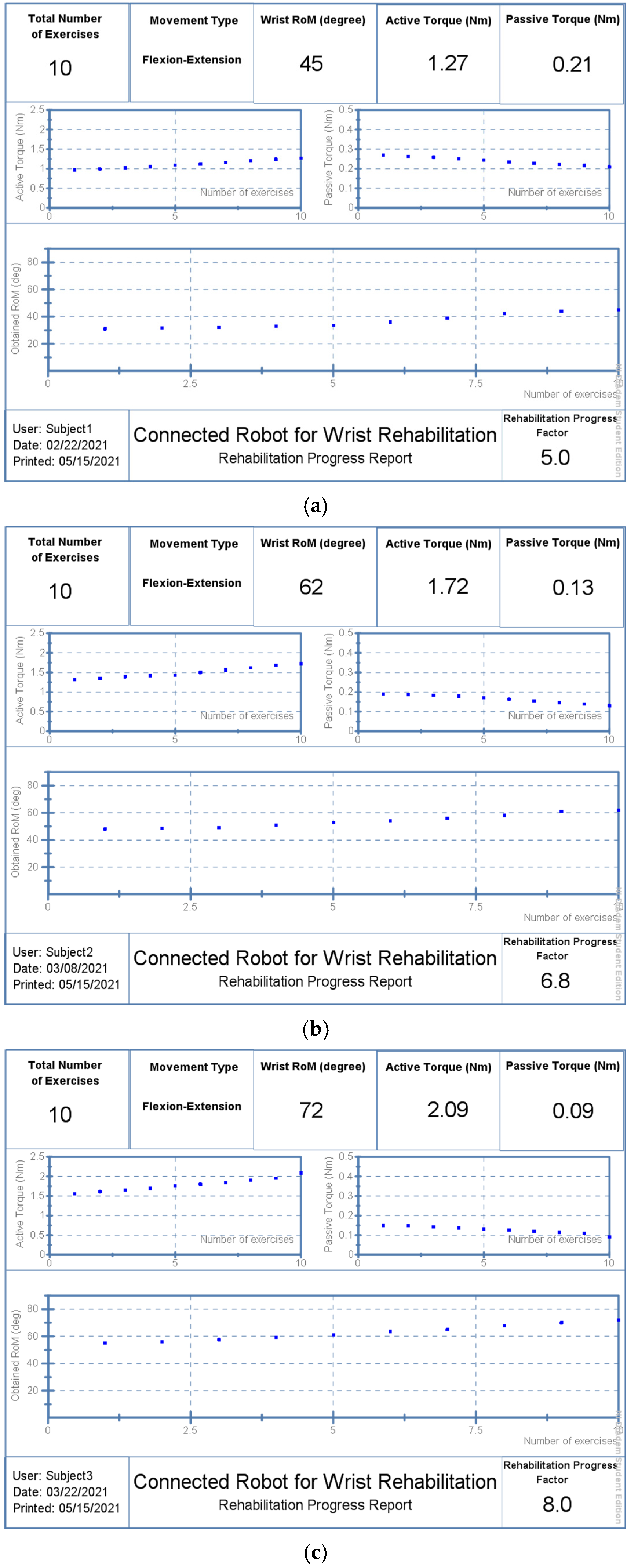
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GWorld Health Organization. Stroke, Cerebrovascular Accident. Available online: http://www.emro.who.int/health-topics/strokecerebrovascularaccident/index.html (accessed on 3 August 2020).
- Samaee, S.; Kobravi, H.R. Predicting the occurrence of wrist tremor based on electromyography using a hidden Markov model and entropy based learning algorithm. Biomed. Signal Process. Control 2019, 57, 101739. [Google Scholar] [CrossRef]
- Moghaddam, M.M.; Moshaii, A.A.; Niestanak, V.D. Fuzzy sliding mode control of a wearable rehabilitation robot for wrist and finger. Ind. Robot. 2019, 46. Available online: https://www.emerald.com/insight/content/doi/10.1108/IR-05-2019-0110/full/html (accessed on 1 June 2022).
- Tran, V.D.; Dario, P.; Mazzoleni, S.; Posteraro, F. Wrist robot-assisted rehabilitation treatment in subacute and chronic stroke patients: From distal-to-proximal motor recovery. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1889–1896. [Google Scholar]
- Islam, R.; Zaman, A.U.; Brahmi, B.; Bouteraa, Y.; Wang, I.; Rahman, M. Design and Development of an Upper Limb Rehabilitative Robot with Dual Functionality. Micromachines 2021, 12, 870. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, I.; Bouteraa, Y.; Rekik, C. Web-based robot control for wrist telerehabilitation. In Proceedings of the IEEE 4th International Conference on Control Engineering Information Technology (CEIT), Hammamet, Tunisia, 16–18 December 2016; pp. 1–6. [Google Scholar]
- Charles, S.K.; Hogan, N. Dynamics of wrist rotations. J. Biomech. 2010, 44, 614–621. [Google Scholar] [CrossRef]
- Peaden, A.W.; Charles, S.K. Dynamics of wrist and forearm rotations. J. Biomech. 2014, 47, 2779–2785. [Google Scholar] [CrossRef]
- Kooij, H.; Keemink, Q.; Stienen, A. Admittance control for physical human-robot interaction. Int. J. Robot. Res. 2018, 37, 1421–1444. [Google Scholar]
- Ben Abdallah, I.; Bouteraa, Y.; Rekik, C. Kinect-Based Sliding Mode Control for Lynxmotion Robotic Arm. Adv. Hum.-Comput. Interact. 2016, 2016, 7921295. [Google Scholar] [CrossRef] [Green Version]
- Bouteraa, Y.; Ben Abdallah, I.; Alnowaiser, K.; Ibrahim, A. Smart solution for pain detection in remote rehabilitation. Alex. Eng. J. 2021, 60, 3485–3500. [Google Scholar] [CrossRef]
- Zhang, J.; Meng, Q.; Yang, X. Virtual rehabilitation training system based on surface emg feature extraction and analysis. J. Med. Syst. 2019, 43, 48. [Google Scholar]
- Foroutannia, A.; Akbarzadeh, T.M.-R.; Akbarzadeh, A. A deep learning strategy for EMG-based joint position prediction in hip exoskeleton assistive robots. Biomed. Signal Process. Control 2022, 75, 103557. [Google Scholar] [CrossRef]
- Bednarczyk, M.; Omran, H.; Bayle, B. EMG-Based Variable Impedance Control With Passivity Guarantees for Collaborative Robotics. IEEE Robot. Autom. Lett. 2022, 7, 4307–4312. [Google Scholar] [CrossRef]
- Bouteraa, Y.; Abdallah, I.B.; Elmogy, A. Design and control of an exoskeleton robot with emg-driven electrical stimulation for upper limb rehabilitation. Ind. Robot. 2020, 47. Available online: https://www.emerald.com/insight/content/doi/10.1108/IR-02-2020-0041/full/html (accessed on 1 June 2022). [CrossRef]
- Aabdallah, I.B.; Bouteraa, Y.; Rekik, C. Design of smart robot for wrist rehabilitation. Int. J. Smart Sens. Intell. Syst. 2016, 9, 1029–1053. [Google Scholar] [CrossRef] [Green Version]
- Matsui, M.; Higashi, T.; Iso, N.; Hachisuka, K.; Yamamoto, I.; Hachisuka, A. Wrist rehabilitation robot system and its effectiveness for patients. Sens. Mater. 2018, 30, 1825–1830. [Google Scholar]
- Telegenov, K.; Zeinullin, M.; Tursynbek, I.; Omarkulov, N.; Shintemirov, A. Preliminary mechanical design of NU-Wrist: A 3-DOF selfaligning Wrist rehabilitation robot. In Proceedings of the IEEE International Conference on Biomedical Robotics and Biomechatronics (BioRob), Singapore, 26–29 June 2016; pp. 962–967. [Google Scholar]
- Kim, J.P.; Kim, K.; Hwang, C.H.; Phan, H.L.; Koo, K.I. Wrist rehabilitation system using augmented reality for hemiplegic stroke patient rehabilitation: A feasibility study. Appl. Sci. 2019, 9, 2892. [Google Scholar]
- Merzouk, A.; Choquet, D.; Gayda, M.; Ahmaidi, S. Assessment of skeletal muscle fatigue in men with coronary artery disease using surface electromyography during isometric contraction of quadriceps muscles. Arch. Phys. Med. Rehabil. 2005, 86, 210–215. [Google Scholar]
- Bouteraa, Y.; Ben Abdallah, I.; ElMogy, A.; Ibrahim, A.; Tariq, U.; Ahmad, T. A Fuzzy Logic Architecture for Rehabilitation Robotic Systems. Int. J. Comput. Commun. Control 2020, 15, 1841–9844. [Google Scholar] [CrossRef]
- De Leva, P. Adjustments to Zatsiorsky-Seluyanov’s segment inertia parameters. J. Biomech. 1996, 29, 1223–1230. [Google Scholar] [CrossRef]
- Krebs, H.I.; Volpe, B.T.; Williams, D.; Celestino, J.; Charles, S.K.; Lynch, D.; Hogan, N. Robot-Aided Neurorehabilitation: A Robot for Wrist Rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 327–335. [Google Scholar] [CrossRef] [Green Version]
- Gielen, C.C.; Houk, J.C. Nonlinear viscosity of human wrist. J. Neurophysiol. 1984, 52, 553–569. [Google Scholar] [CrossRef] [PubMed]
- Perreault, E.J.; Kirsch, R.; Crago, P.E. Multijoint dynamics and postural stability of the human arm. Exp. Brain Res. 2004, 157, 507–517. [Google Scholar] [CrossRef] [PubMed]
- Oskoei, M.A.; Hu, H. Support Vector Machine-Based Classification Scheme for Myoelectric Control Applied to Upper Limb. IEEE Trans. Biomed. Eng. 2008, 55, 1956–1965. [Google Scholar] [CrossRef] [PubMed]
- Neu, C.P.; Crisco, J.; Wolfe, S.W. In vivo kinematic behavior of the radio-capitate joint during wrist flexion–extension and radio-ulnar deviation. J. Biomech. 2001, 34, 1429–1438. [Google Scholar] [CrossRef]
- Oskoei, M.A.; Hu, H. GA-based feature subset selection for myoelectric classification. In Proceedings of the IEEE International Conference on Robotics Biomimetics, Kunming, China, 17–20 December 2006; pp. 1465–1470. [Google Scholar]
- Qingju, Z.; Zhizeng, L. Wavelet de-noising of electromyography. In Proceedings of the IEEE International Conference on Mechatronics Automation, Luoyang, China, 25–28 June 2006; pp. 1553–1558. [Google Scholar]
- Phinyomark, A.; Phukpattaranont, P.; Limsakul, C. Feature reduction and selection for emg signal classification. Expert Syst. Appl. 2012, 8, 7420–7431. [Google Scholar] [CrossRef]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
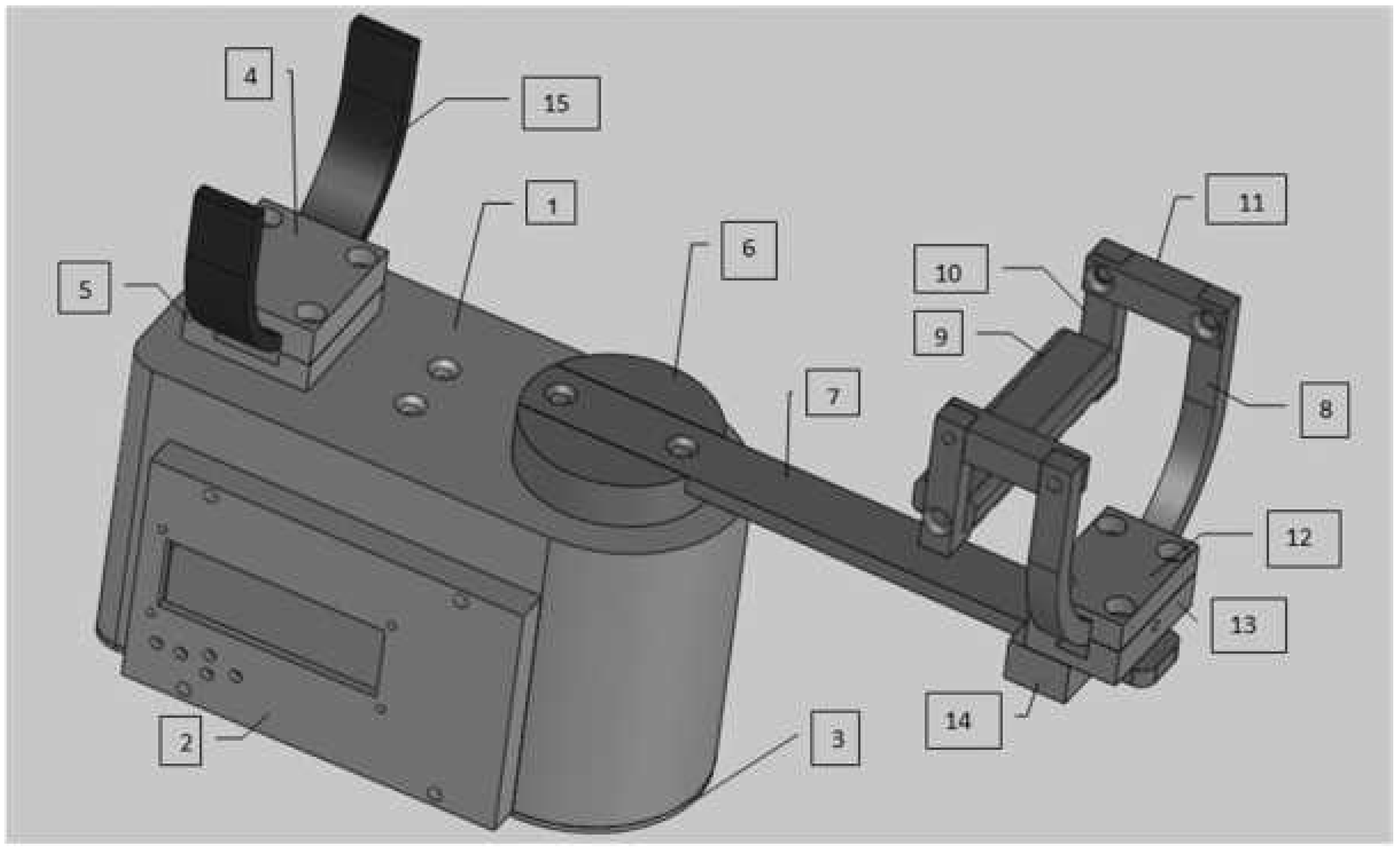
| Block | Article Number | Piece Name | Metal | Quantity |
|---|---|---|---|---|
| Block A | 1 | Box | ALU AU4G | 1 |
| 2 | LCD box | Steel C45 | 1 | |
| 3 | Box cover | Steel C45 | 1 | |
| 4 | Higher back arc support | Steel C45 | 1 | |
| 5 | Lower back arc support | Steel C45 | 1 | |
| Block B | 6 | Drive disk | Steel C45 | 1 |
| 7 | Sliding bar | Steel C45 | 1 | |
| Block C | 8 | Forward arc | Steel C45 | 1 |
| 9 | Handhold | Steel C45 | 1 | |
| 10 | Handhold support in L | Steel C45 | 2 | |
| 11 | Handhold support | Steel C45 | 2 | |
| Block D | 12 | Higher front arc support | Steel C45 | 1 |
| 13 | Intermediate front arc support | Steel C45 | 1 | |
| 14 | Lower front arc support | Steel C45 | 1 | |
| Block E | 15 | Back arc | Steel C45 | 1 |
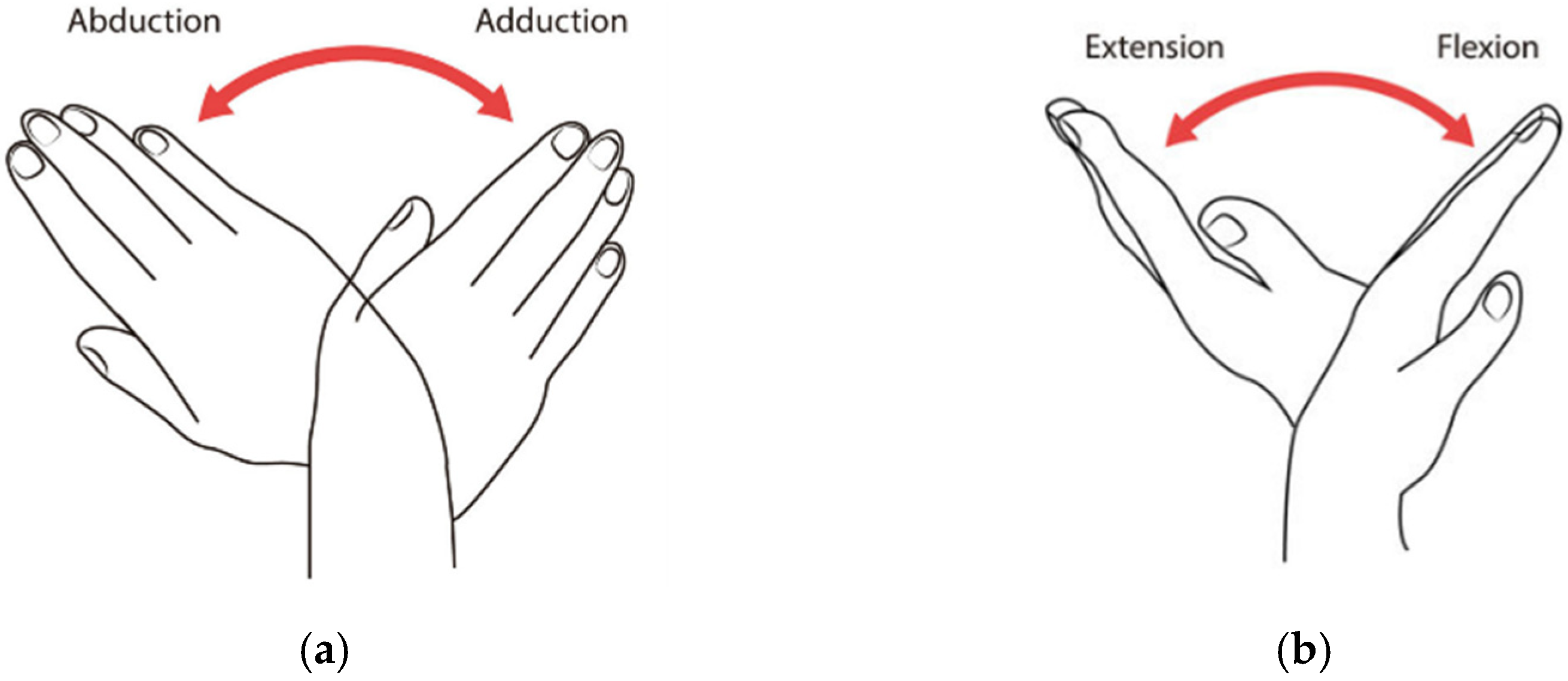
| Mvt Number | Flexion | Extension | Radial | Ulnar |
|---|---|---|---|---|
| RoM | 80–90 | 70–90 | 15 | 30–45 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bouteraa, Y.; Ben Abdallah, I.; Alnowaiser, K.; Islam, M.R.; Ibrahim, A.; Gebali, F. Design and Development of a Smart IoT-Based Robotic Solution for Wrist Rehabilitation. Micromachines 2022, 13, 973. https://doi.org/10.3390/mi13060973
Bouteraa Y, Ben Abdallah I, Alnowaiser K, Islam MR, Ibrahim A, Gebali F. Design and Development of a Smart IoT-Based Robotic Solution for Wrist Rehabilitation. Micromachines. 2022; 13(6):973. https://doi.org/10.3390/mi13060973
Chicago/Turabian StyleBouteraa, Yassine, Ismail Ben Abdallah, Khaled Alnowaiser, Md Rasedul Islam, Atef Ibrahim, and Fayez Gebali. 2022. "Design and Development of a Smart IoT-Based Robotic Solution for Wrist Rehabilitation" Micromachines 13, no. 6: 973. https://doi.org/10.3390/mi13060973