

A Flexible Thermocouple Film Sensor for Respiratory Monitoring

Abstract
:1. Introduction
2. Physical Modeling
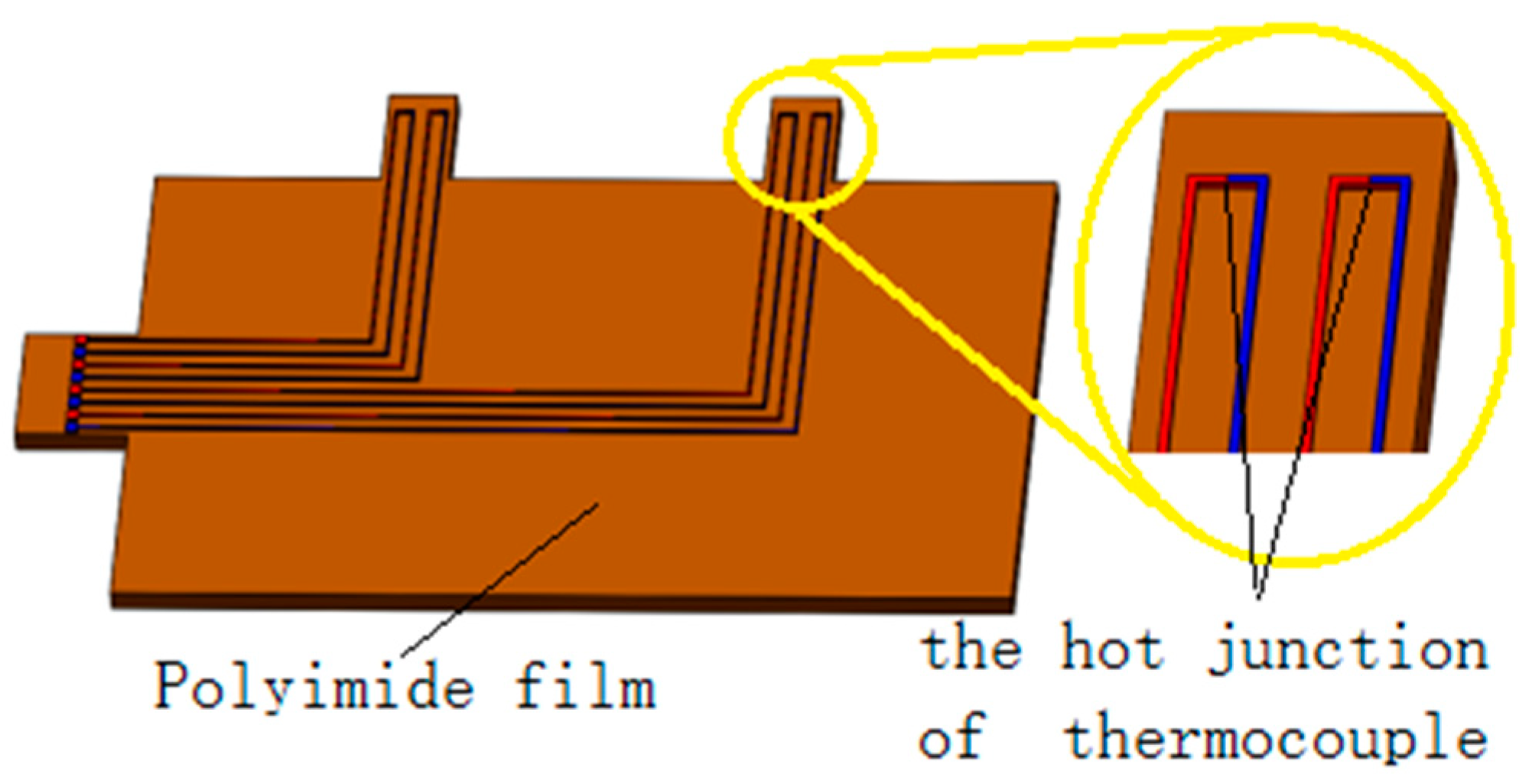
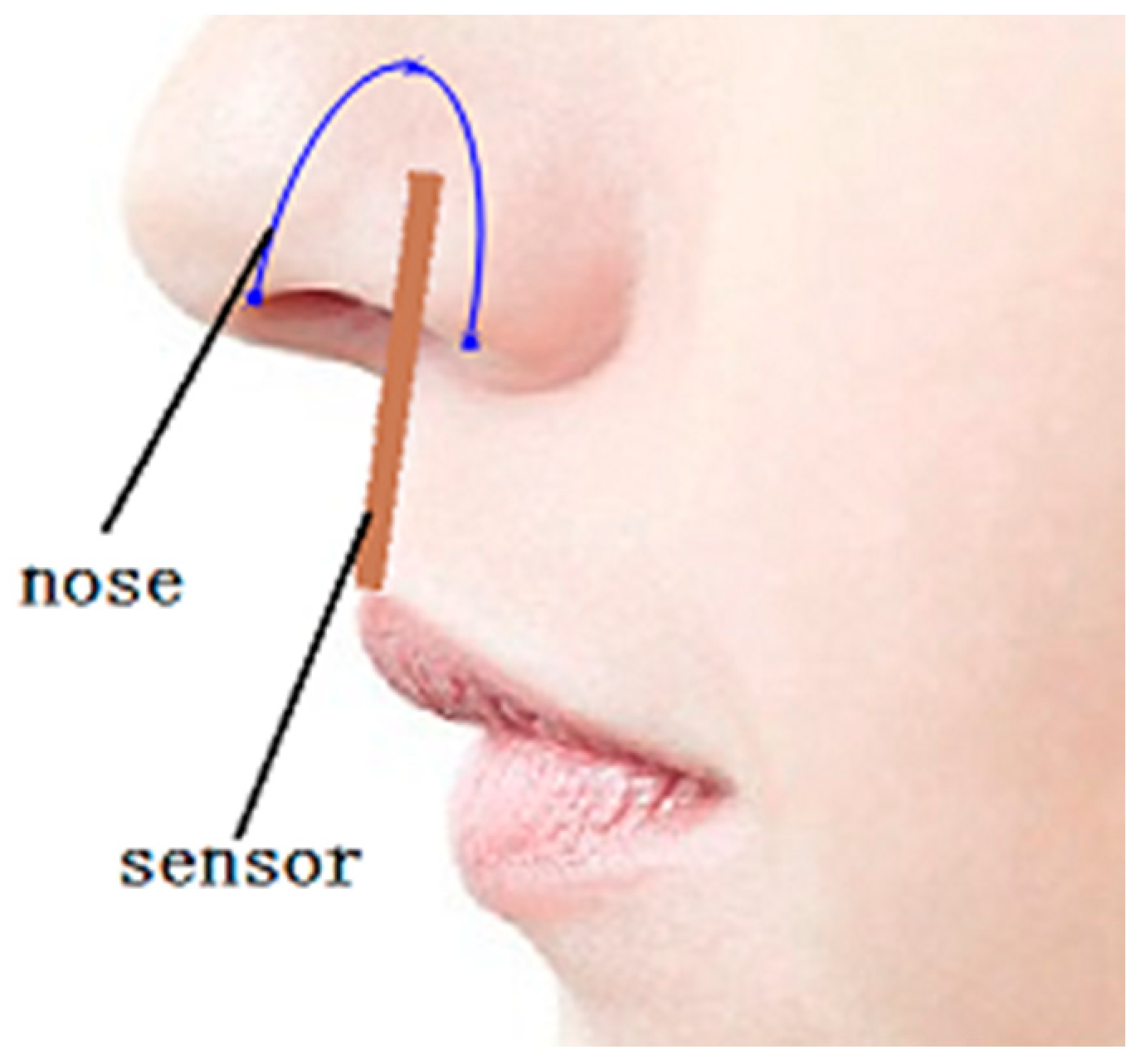
2.1. Physical Model
2.2. Mathematical Model
3. Simulation
3.1. Simulation of the Distribution of the Polyimide Substrate
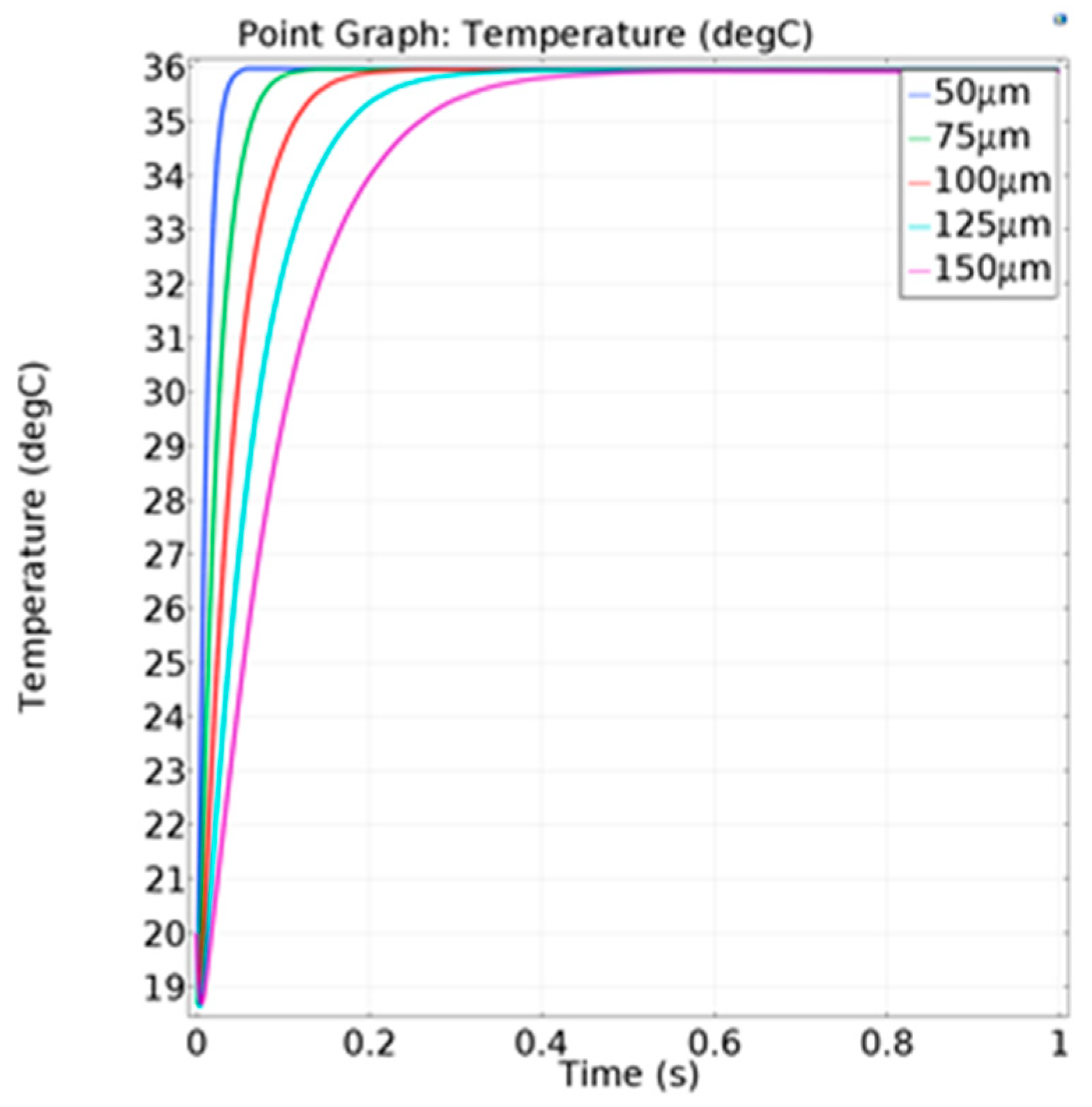
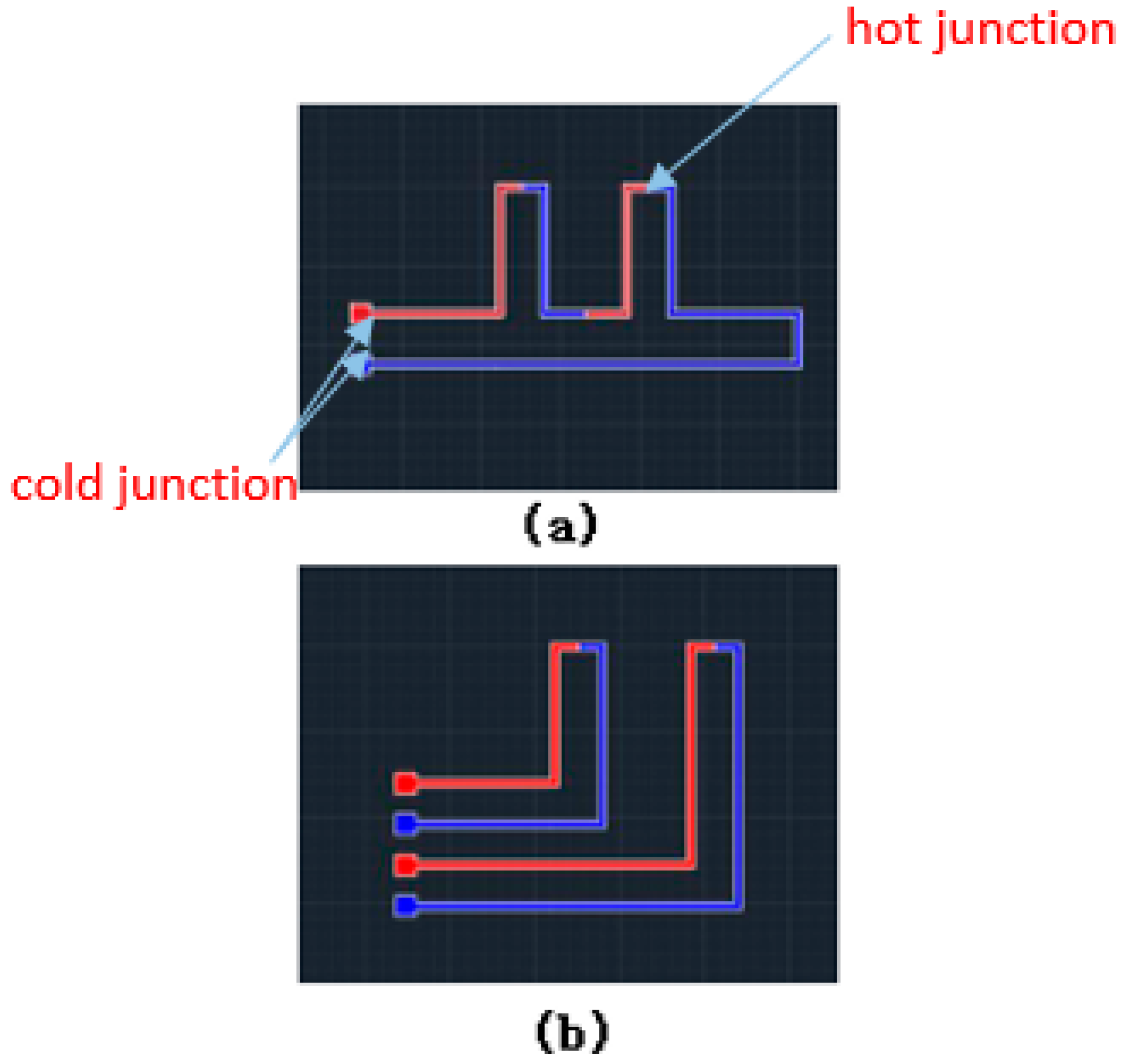
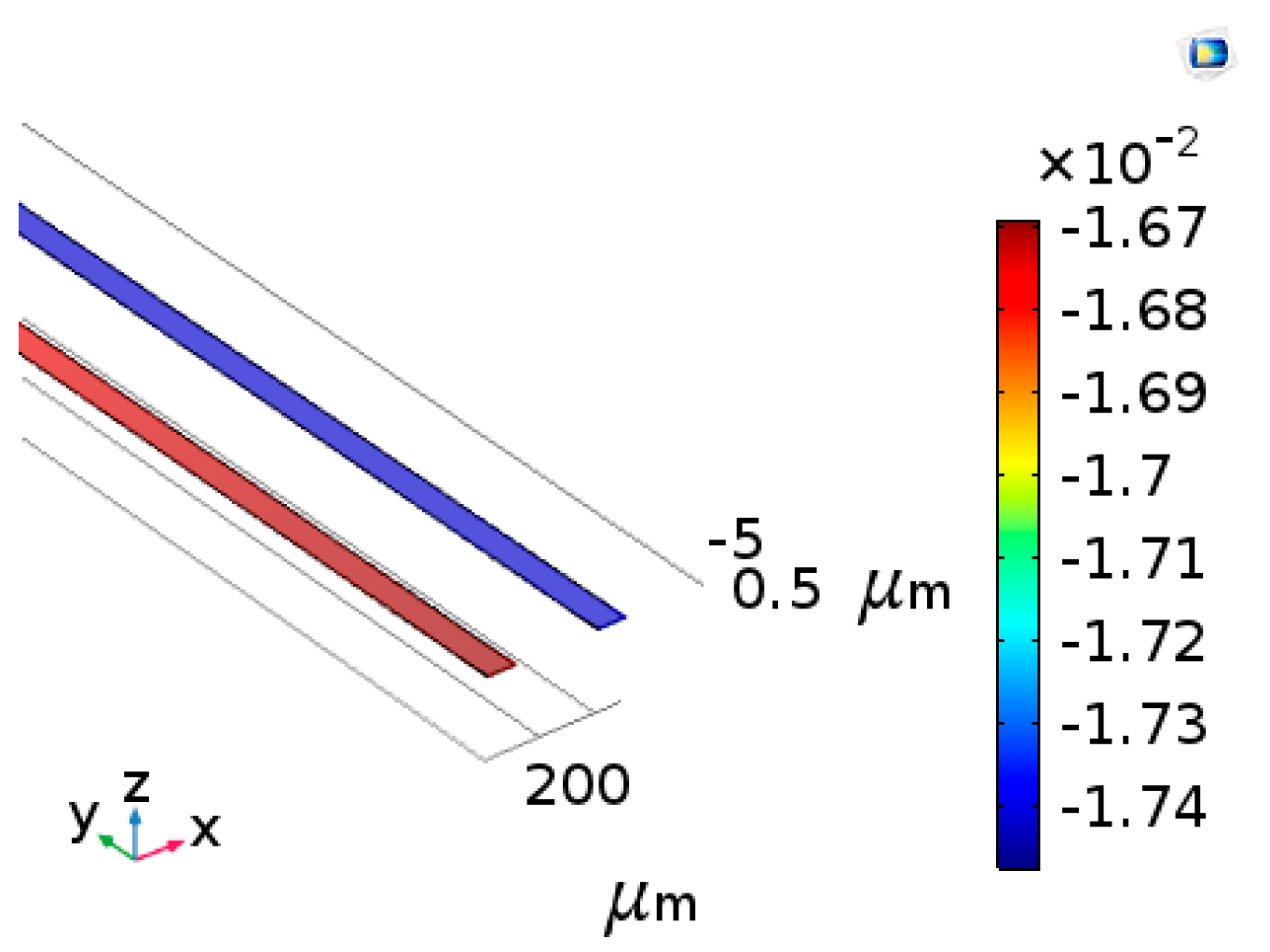
3.2. Simulation of the Single Thermalcouple
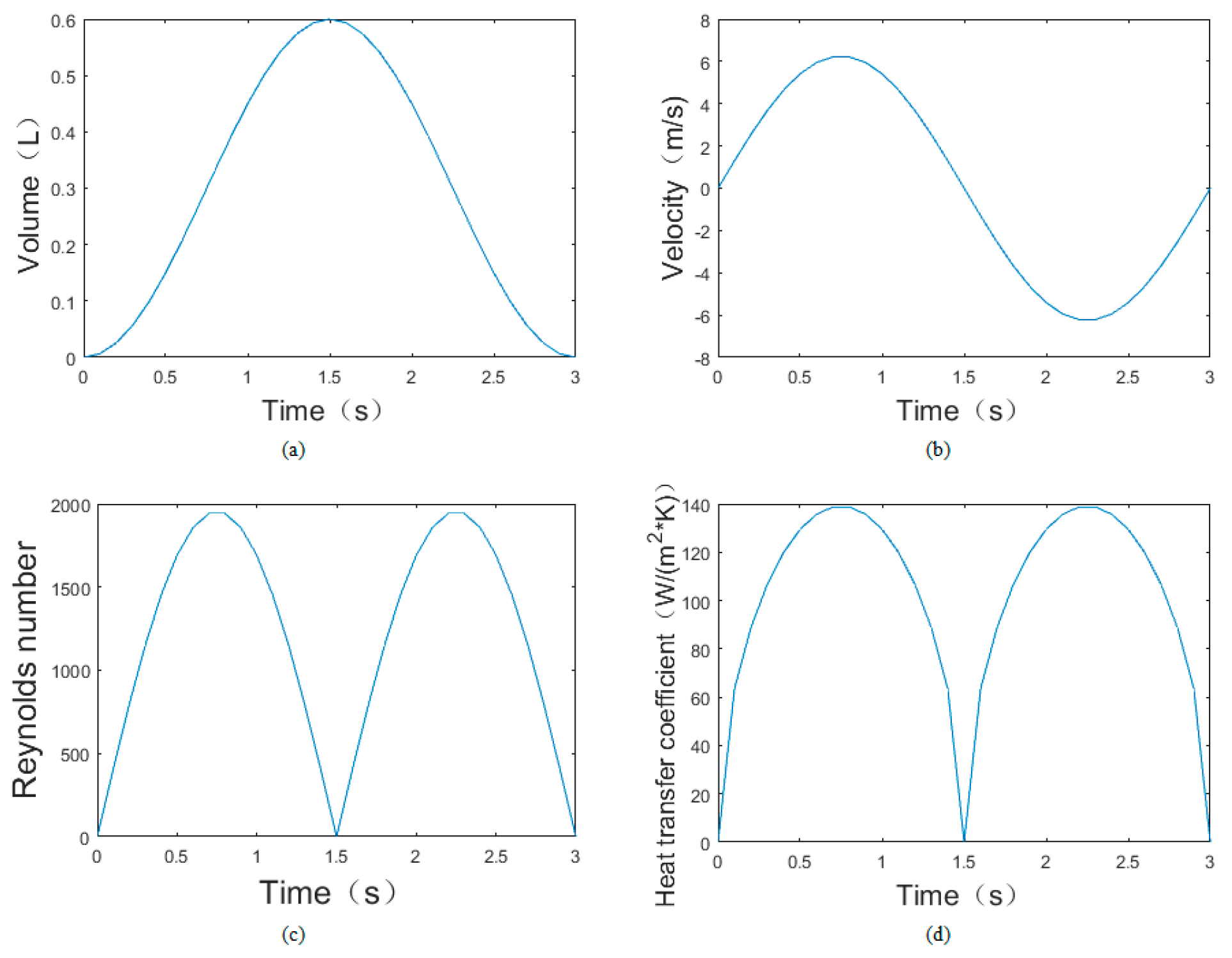
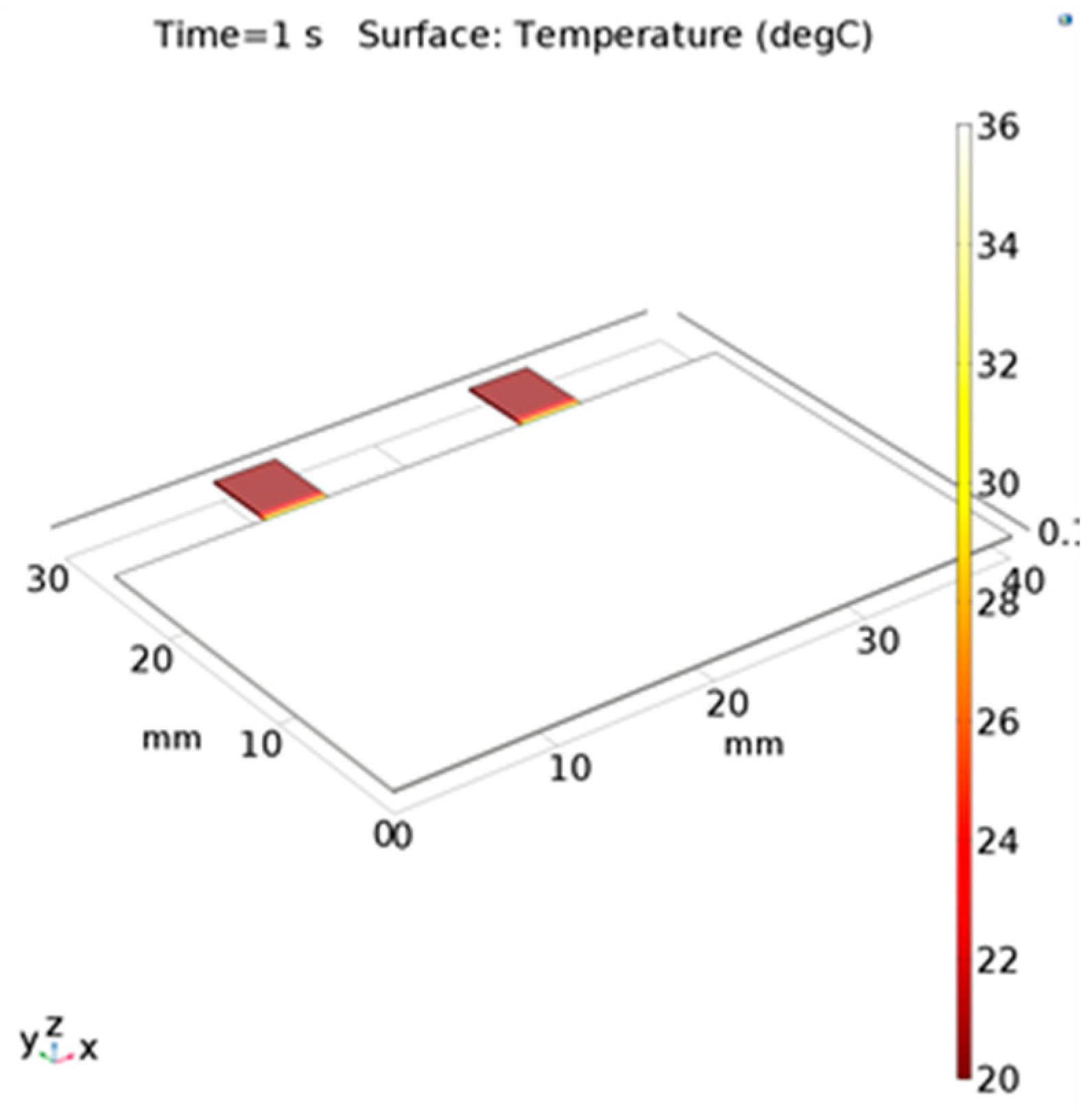
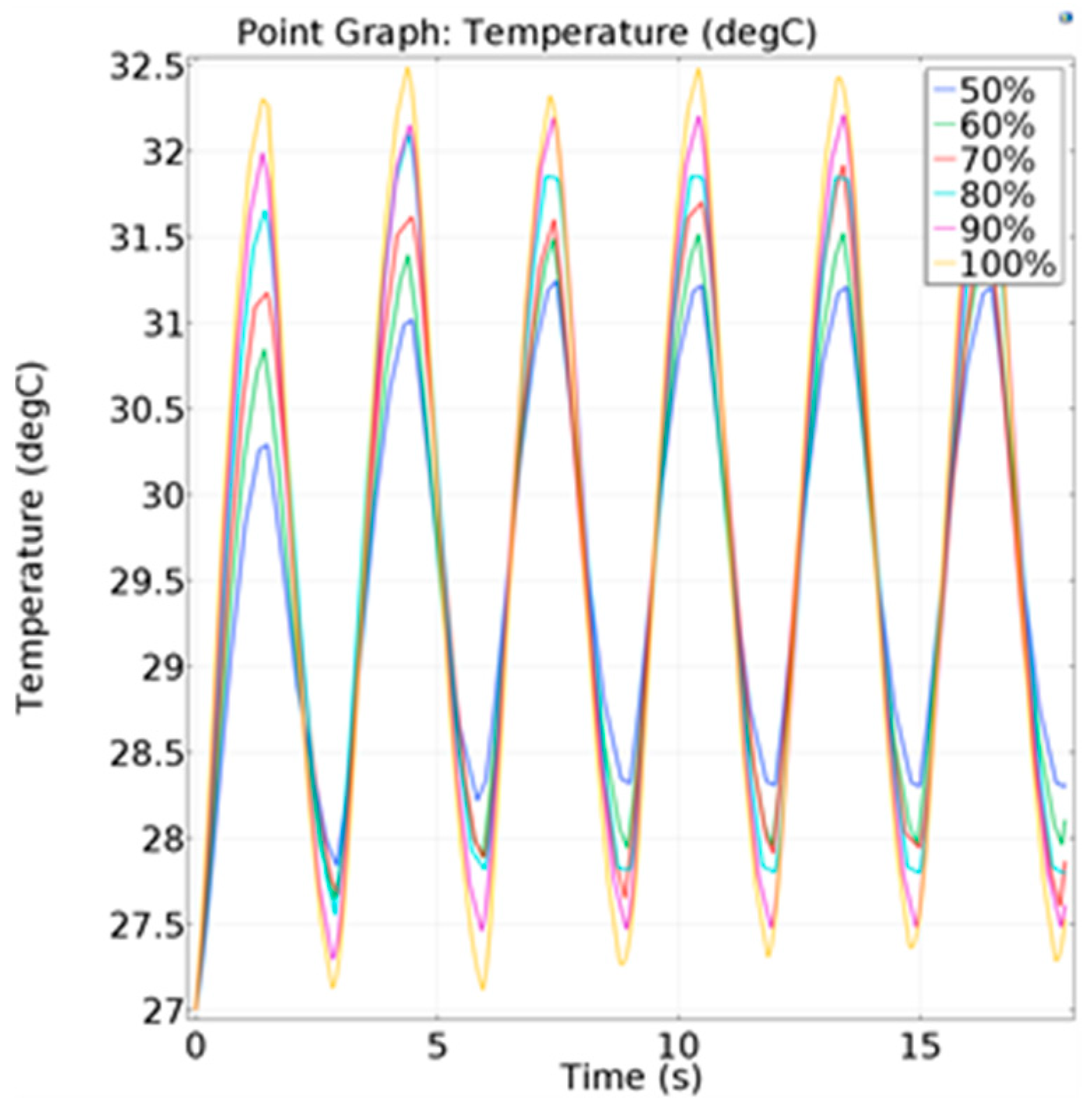
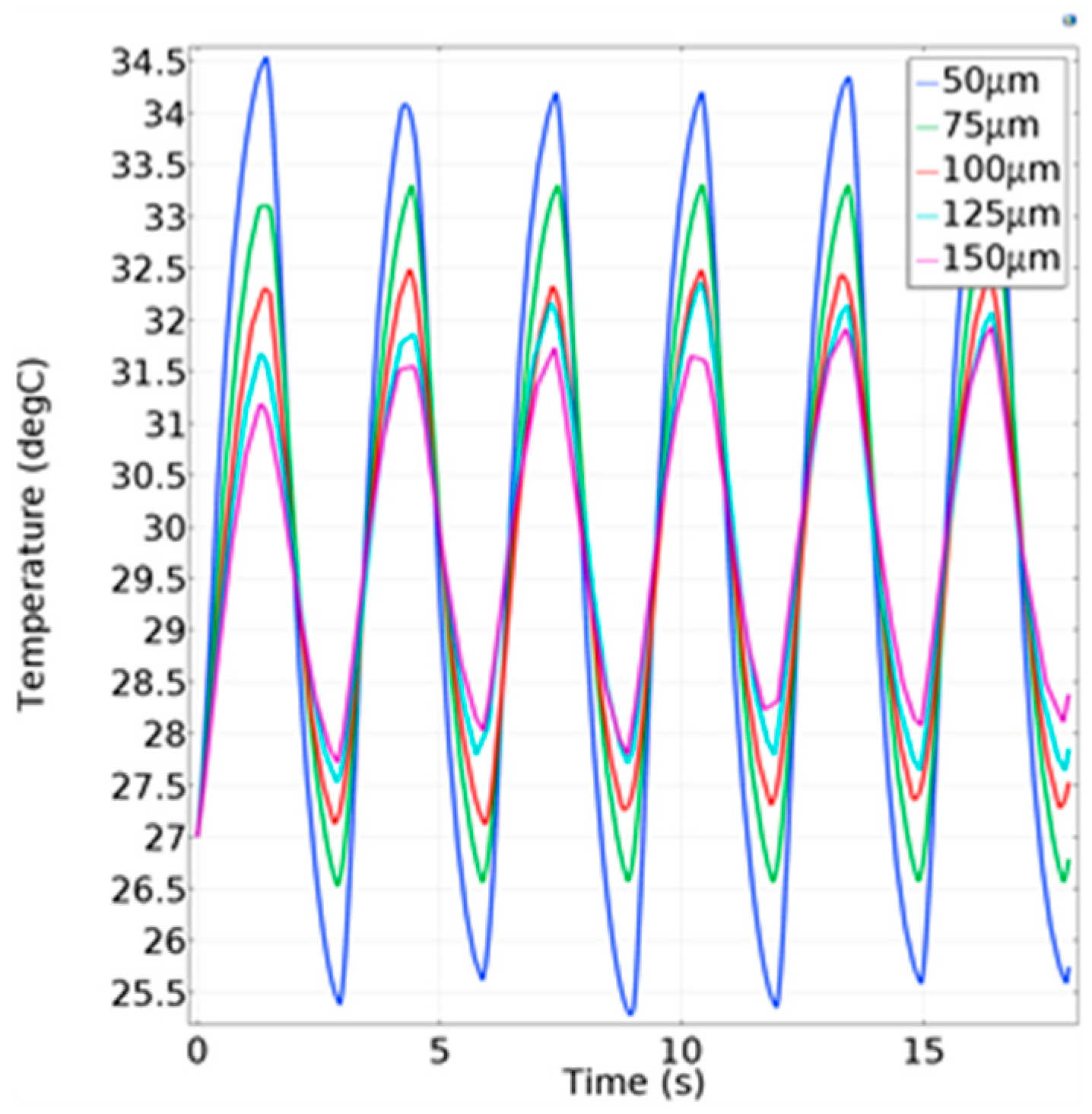
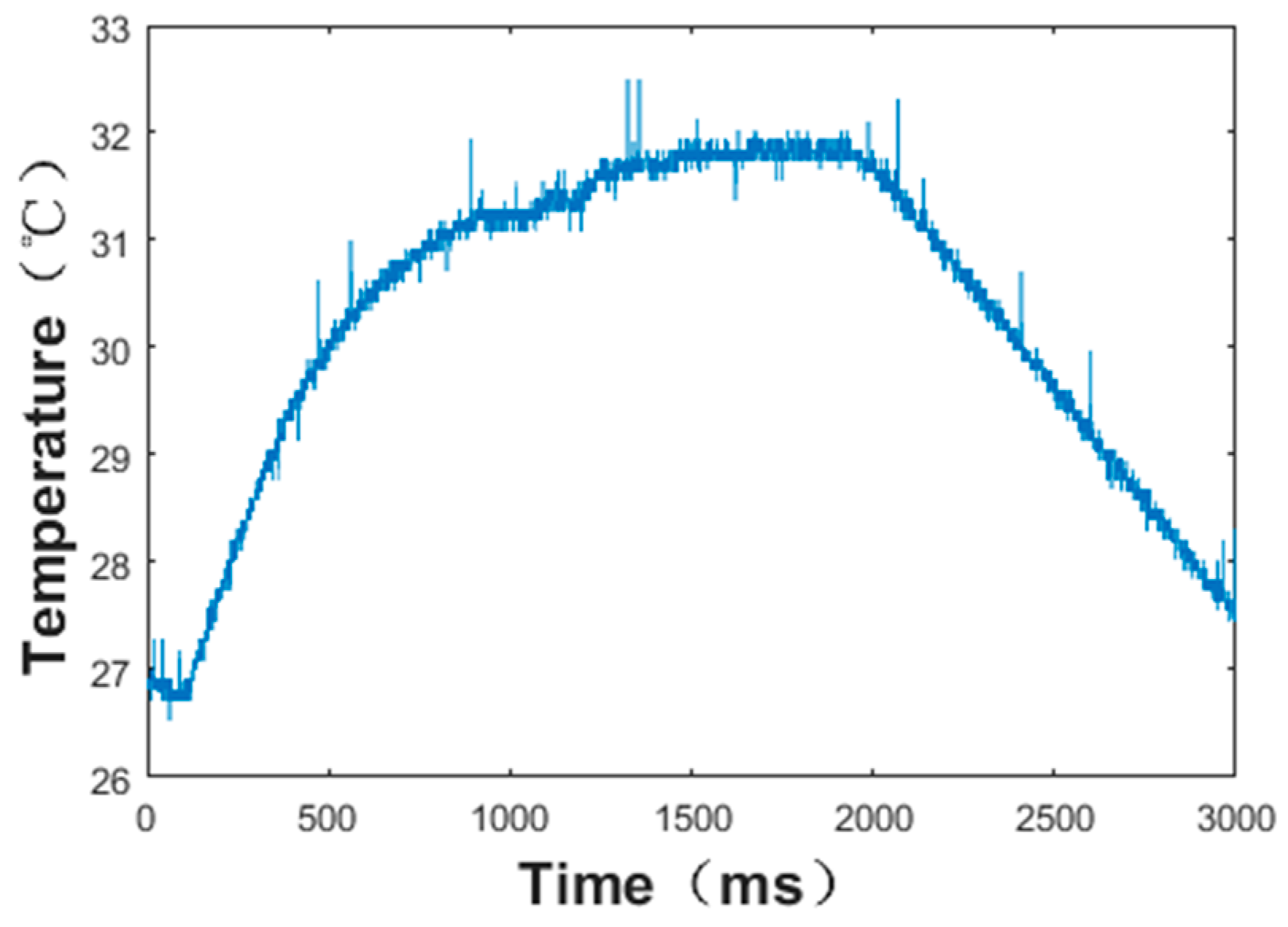
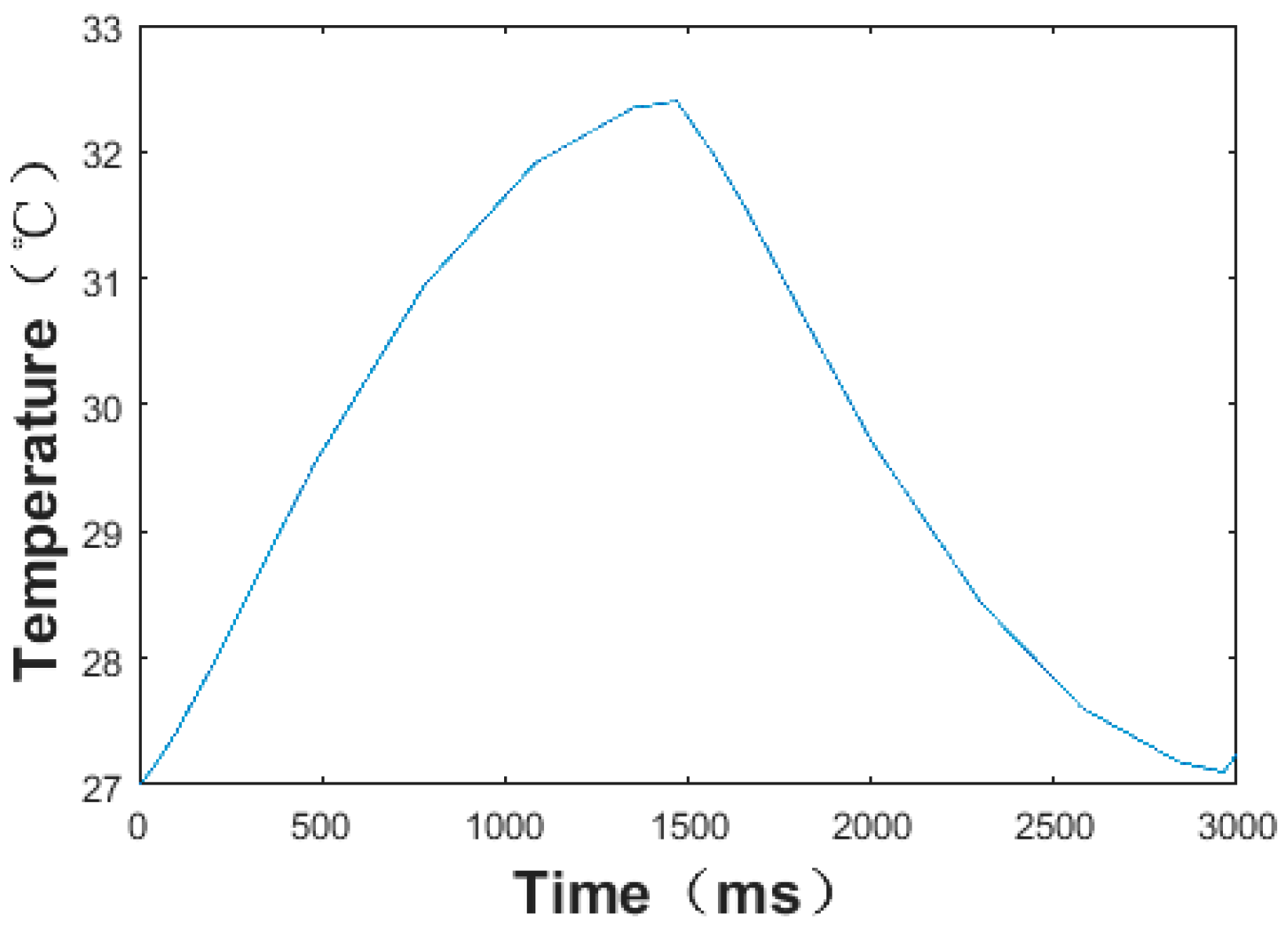
3.3. Simulation of the Sensor under the Working Conditions
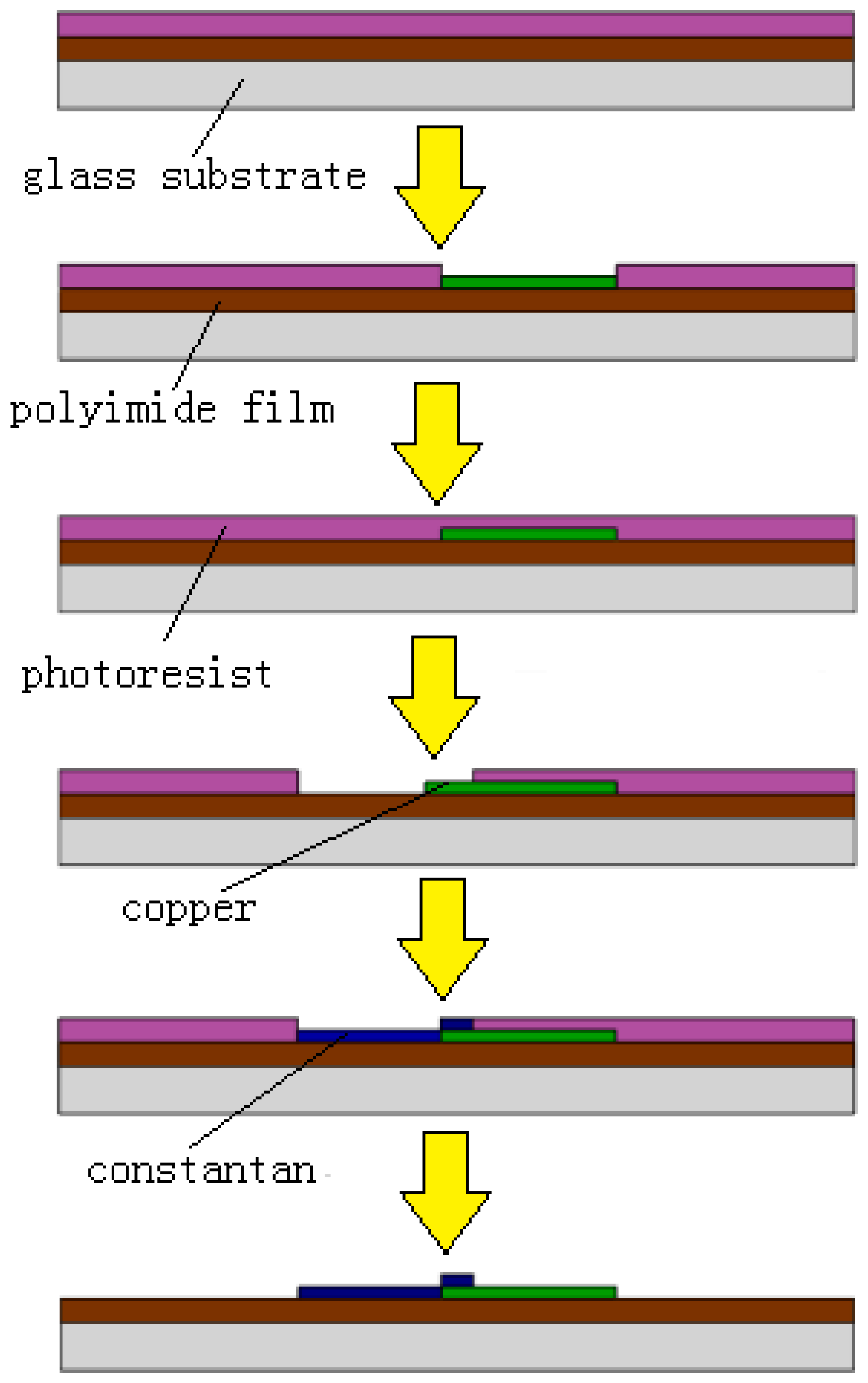
4. Microfabrication
- (1)
- The cleaned PI film was attached to the glass substrate and spin-coated with AZ-4620 positive photoresist with a thickness of 10 μm. Then the glass substrate was heat treated.
- (2)
- The substrate was exposed for 30 s and then developed for 15 s to form the mold of the bottom layer for sputtering.
- (3)
- Then, the chromium seed layer was sputtered at 300 W for 180 s and the copper layer at 300 W for 480 s. The process of sputtering copper was repeated five times.
- (4)
- The photoresist was removed by ultrasonic cleaning in acetone solution for 30 min.
5. Experiment and Results
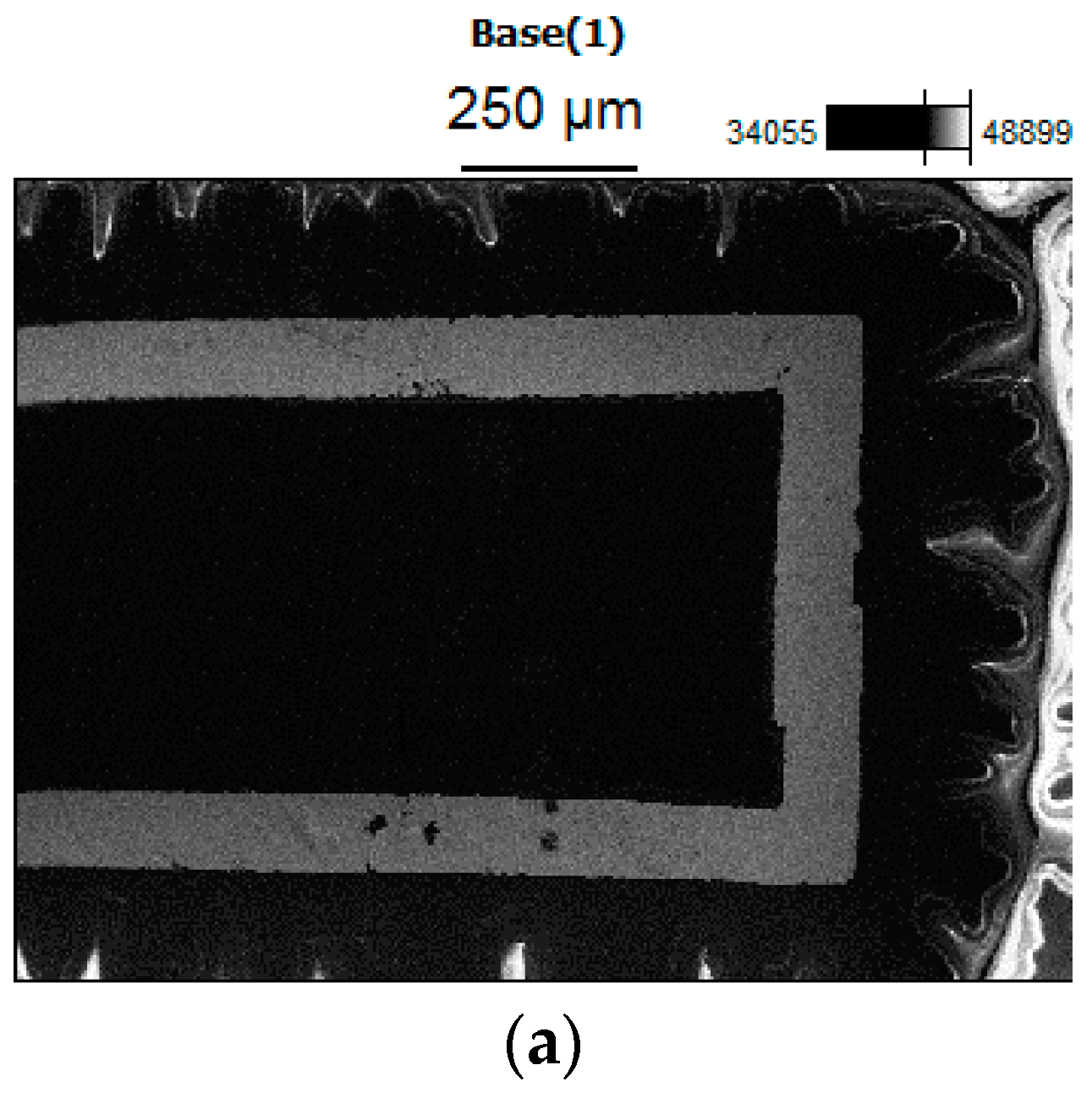
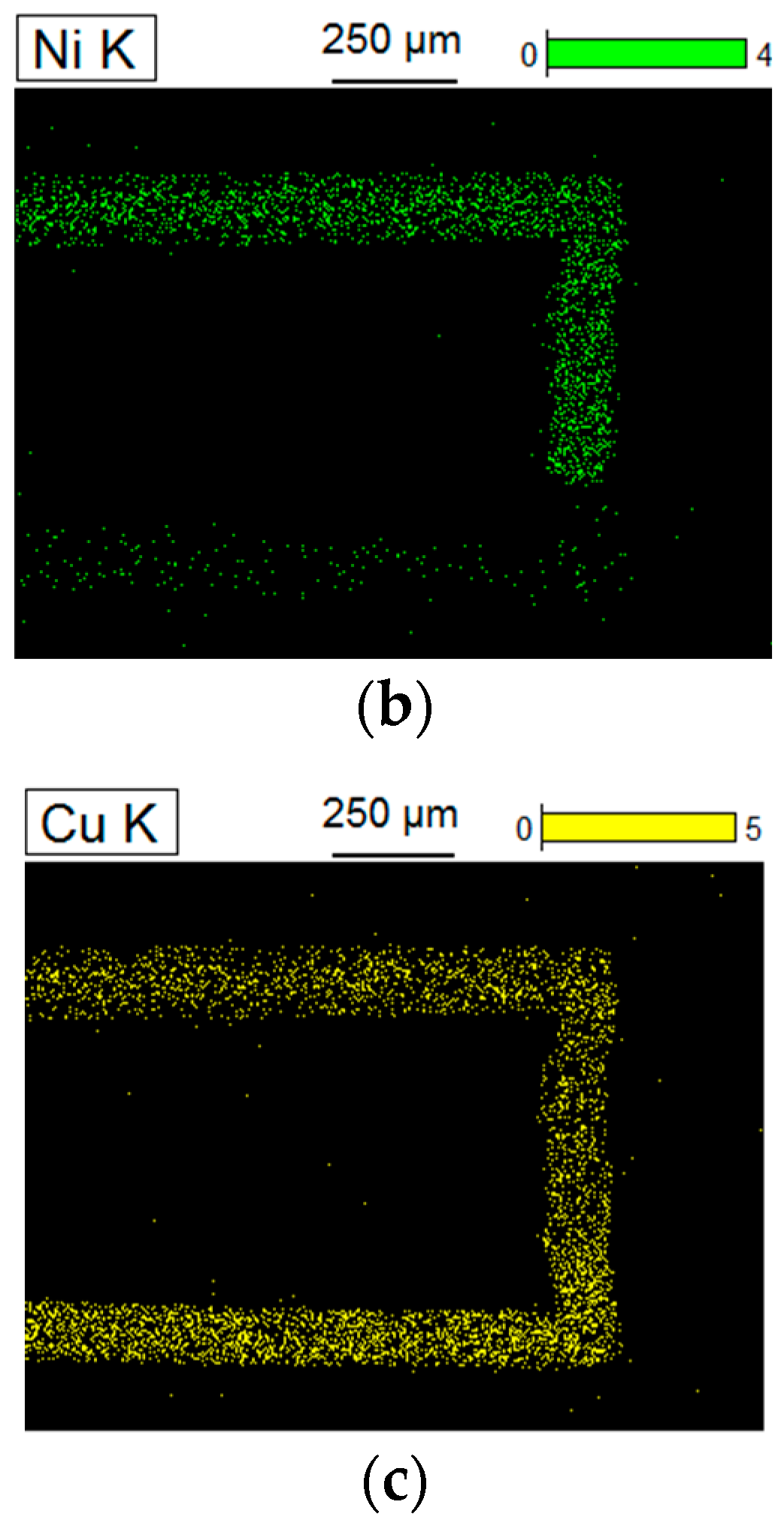
5.1. Microscopic Morphology of the Sensor
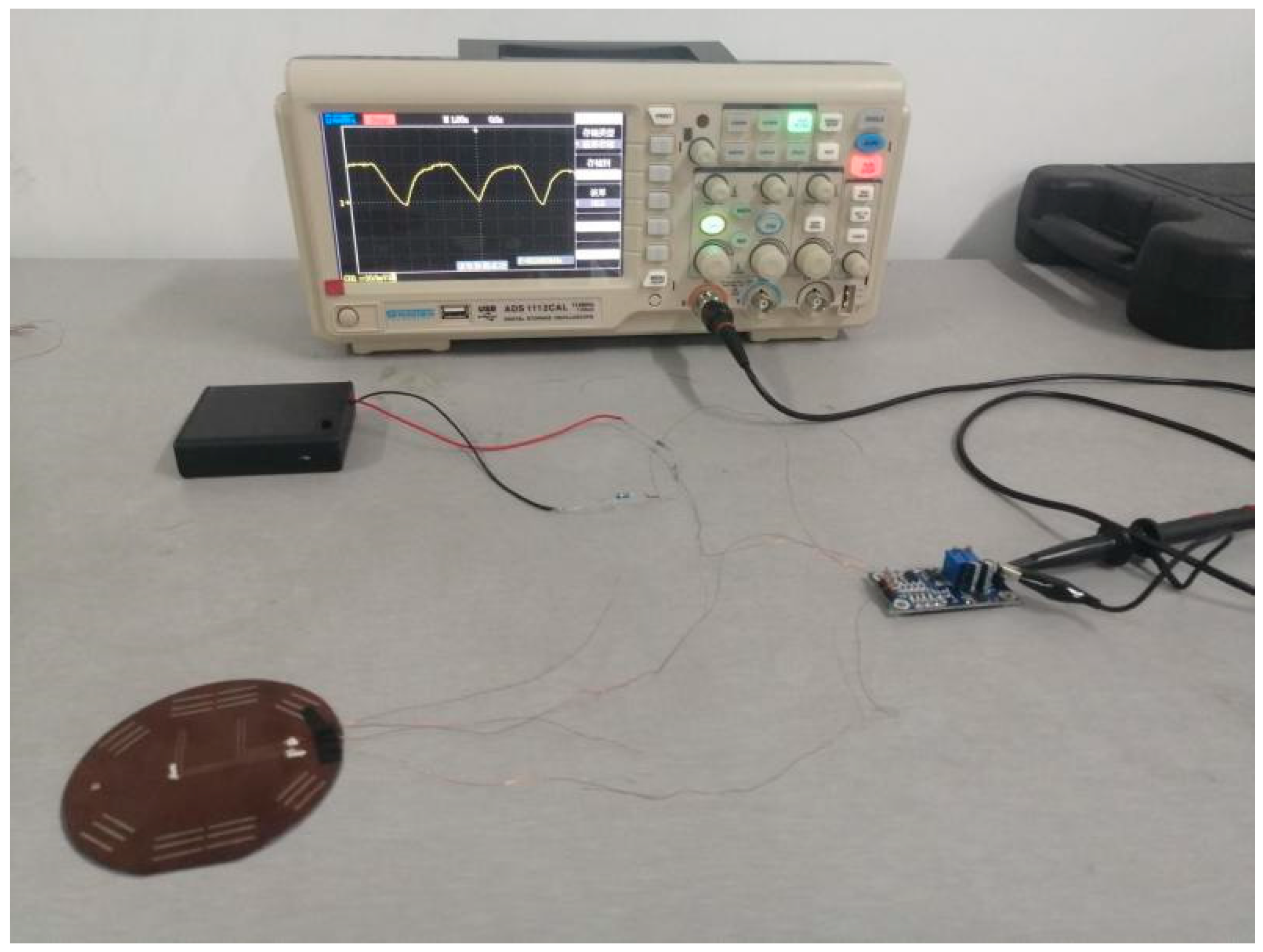
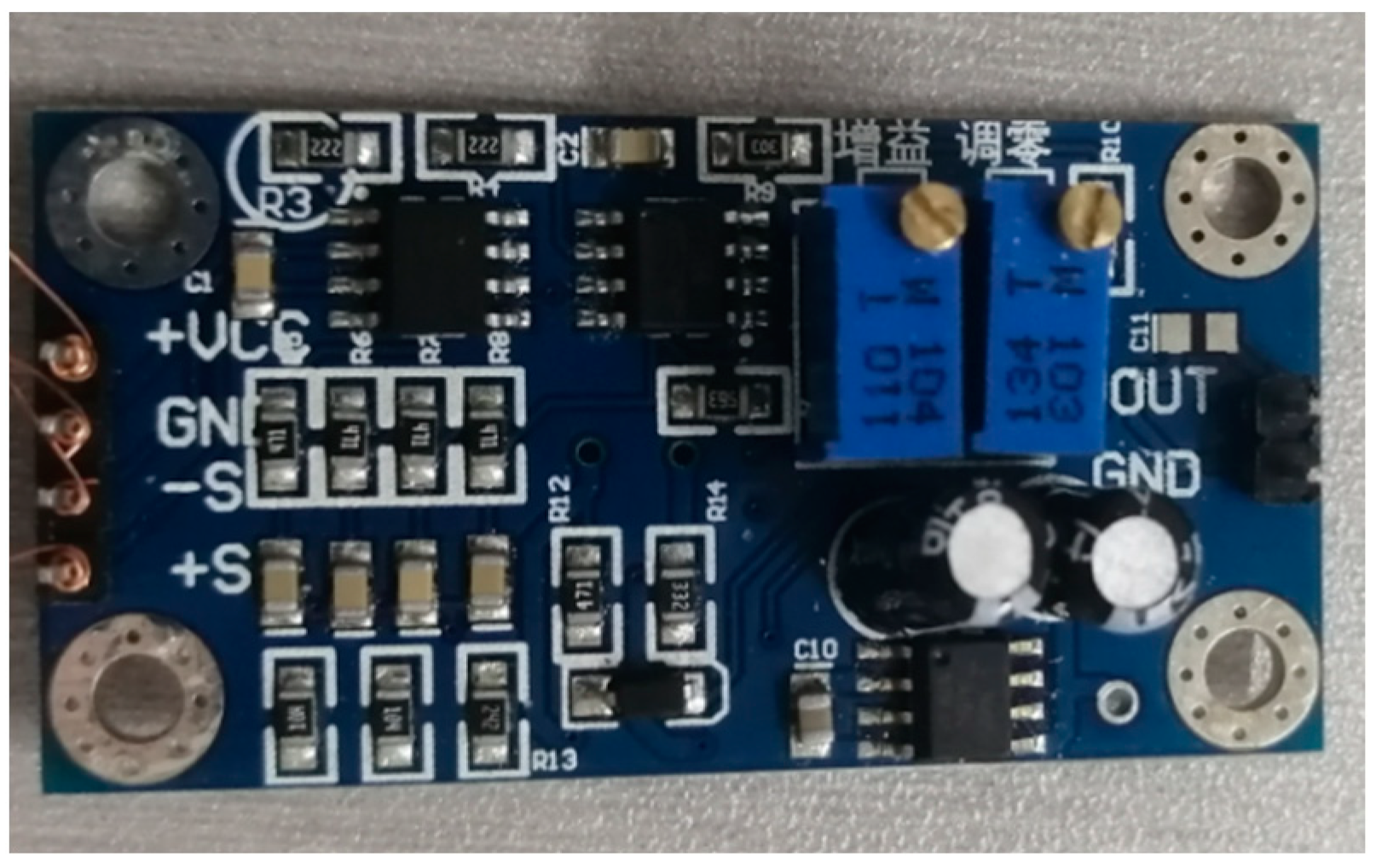
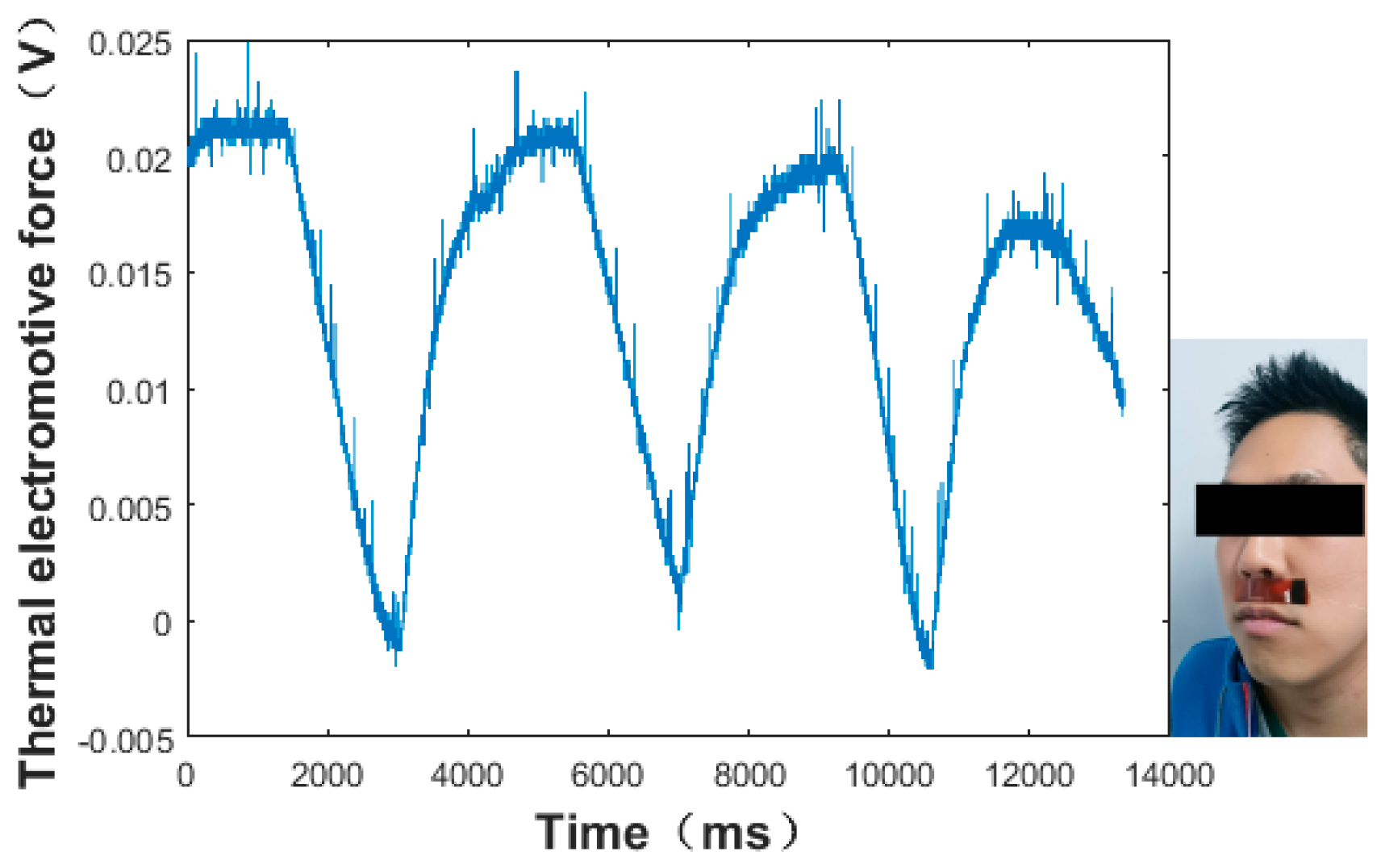
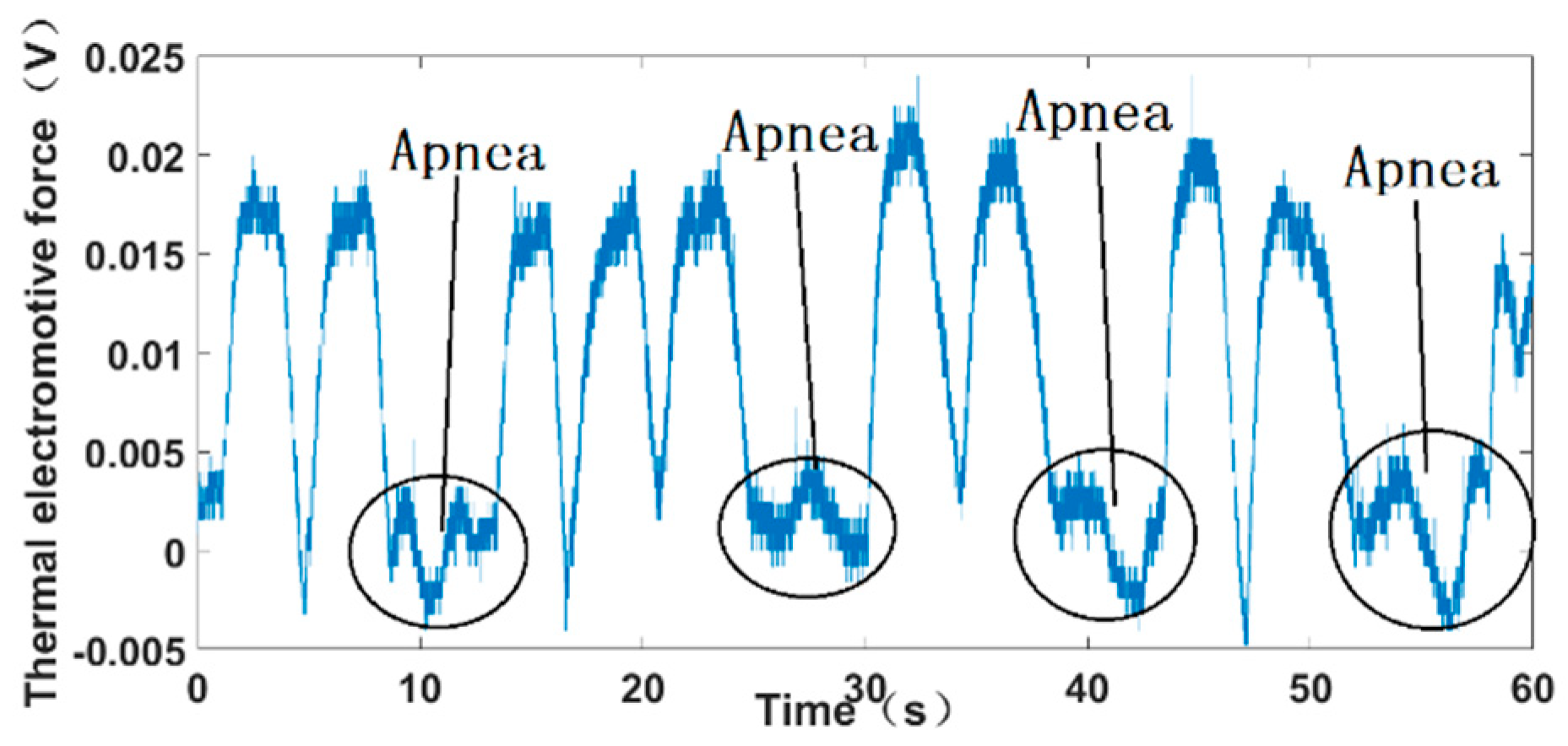
5.2. Sleep Apnea Measurment System and Results
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Buchner, R.; Sosna, C.; Maiwald, M.; Benecke, W.; Lang, W. A high temperature thermopile fabrication process for thermal flow sensors. Sens. Actuators A Phys. 2006, 130–131, 262–266. [Google Scholar] [CrossRef]
- Tang, Z.; Smith, B.; Schild, J.H.; Peckham, P.H. Data transmission from an implantable biotelemeter by load-shift keying using circuit confifiguration modulator. IEEE Trans. Biomed. Eng. 1995, 42, 524–528. [Google Scholar] [CrossRef] [Green Version]
- Yaggi, H.K.; Concato, J.; Kernan, W.N.; Lichtman, J.H.; Brass, L.M.; Mohsenin, V. Obstructive sleep apnea as a risk factor for stroke and death. N. Eng. J. Med. 2005, 353, 2034–2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: An american academy of sleep medicine clinical practice guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef] [PubMed]
- Collop, N.A.; Anderson, W.M.; Boehlecke, B.; Claman, D.; Goldberg, R.; Gottlieb, D.J.; Hudgel, D.; Sateia, M.; Schwab, R. Clinical guidelines for the use of unattended portable monitors in the diagnosis of obstructive sleep apnea in adult patients. J. Clin. Sleep Med. 2007, 3, 737–747. [Google Scholar]
- Collop, N.A.; Tracy, S.L.; Kapur, V.; Mehra, R.; Kuhlmann, D.; Fleishman, S.A.; Ojile, J.M. Obstructive sleep apnea devices for out-of-center (OOC) testing: Technology evaluation. J. Clin. Sleep. Med. 2011, 7, 531–548. [Google Scholar] [CrossRef] [Green Version]
- Marino, M.; Li, Y.; Rueschman, M.N.; Winkelman, J.W.; Ellenbogen, J.M.; Solet, J.M.; Dulin, H.; Berkman, L.F.; Buxton, O.M. Measuring sleep: Accuracy, sensitivity, and specificity of wrist actigraphy compared to polysomnography. Sleep 2013, 36, 1747–1755. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, F.; Lu, B.; Zhang, Y.; Feng, X. Skin-like hybrid integrated circuits conformal to face for continuous respiratory monitoring. Adv. Electron. Mater. 2020, 6, 2000145. [Google Scholar] [CrossRef]
- Jiang, P.; Zhu, R.; Dong, X.; Chang, Y. Combination mode of physiological signals for diagnosis of OSAS using portable monitor. Sleep Breath 2018, 22, 123–129. [Google Scholar] [CrossRef]
- Gupta, H.; Arumuru, V.; Jha, R. Industrial fluid flow measurement using optical fiber sensors: A review. IEEE Sens. J. 2021, 21, 7130–7142. [Google Scholar] [CrossRef]
- Jin, H.; Tao, X.; Dong, S.R. Flexible surface acoustic wave respiration sensor for monitoring obstructive sleep apnea syndrome. J. Micromech. Microeng. 2017, 27, 115006. [Google Scholar] [CrossRef]
- Lin, H.C.; Su, C.L.; Ong, J.H.; Chen, Y.W.; Lin, C.Y.; Chiang, L.L.; Hung, C.H. Pulse oximetry monitor feasible for early screening of Obstructive Sleep Apnea (OSA). J. Med. Biol. Eng. 2020, 40, 62–70. [Google Scholar] [CrossRef]
- Que, R.-Y.; Zhu, R. A compact flexible thermal flow sensor for detecting two-dimensional flow vector. IEEE Sens. J. 2015, 15, 1931–1936. [Google Scholar] [CrossRef]
- Wang, D.F.; Isagawa, K.; Kobayashi, T.; Itoh, T.; Maeda, R. Developing passive piezoelectric MEMS sensor applicable to two-wire DC appliances with current switching. Micro Nano Lett. 2012, 7, 68–71. [Google Scholar] [CrossRef]
- Kottapalli, A.G.P.; Asadnia, M.; Miao, J.M. Polymer MEMS pressure sensor arrays for fish-like underwater sensing applications. Micro Nano Lett. 2012, 7, 1189–1192. [Google Scholar] [CrossRef]
- Kuo, J.T.W.; Yu, L.; Meng, E. Micromachined thermal flow sensors—A review. Micromachines 2012, 3, 550–573. [Google Scholar] [CrossRef] [Green Version]
- Feng, H.L.; Miao, X.D.; Yang, Z.Q. Design, simulation and experimental study of the linear magnetic microactuator. Micromachines 2018, 9, 454. [Google Scholar] [CrossRef] [Green Version]
- Elsheikh, M.H.; Shnawah, D.A.; Sabri, M.F.M.; Said, S.B.M.; Hassan, M.H.; Bashir, M.B.A.; Mohamad, M. A review on thermoelectric renewable energy: Principle parameters that affect their performance. Renew. Sust. Energ. Rev. 2014, 30, 337–355. [Google Scholar] [CrossRef]
- Zhang, X.; Han, Y.; Li, J.; Zhang, L.; Jia, X.; Wang, E. Portable, universal, and visual ion sensing platform based on the light emitting diode-based self-referencing-ion selective field-effect transistor. Anal. Chem. 2014, 86, 1380–1384. [Google Scholar] [CrossRef]
- Lihong, Y.; Yuanshen, Z.; Cenming, F. The influence of size effect on sensitivity of Cu/CuNi thin-film thermocouple. Phys. Procedia 2011, 22, 95–100. [Google Scholar]
- Dalola, S.; Cerimovic, S.; Kohl, F.; Beigelbeck, R.; Schalko, J.; Ferrari, V.; Marioli, D.; Keplinger, F.; Sauter, T. MEMS thermal flow sensor with smart electronic interface circuit. IEEE Sens. J. 2012, 12, 3318–3328. [Google Scholar] [CrossRef]
- Wei, C.-L.; Lin, C.-F.; Tseng, I.-T. A novel MEMS respiratory flow sensor. IEEE Sens. J. 2010, 10, 16–18. [Google Scholar] [CrossRef]
- Wang, X.; Ke, Z.; Liao, G.; Pan, X.; Yang, Y.; Xu, W. Fast-response breathing monitoring system for human respiration disease detection. IEEE Sens. J. 2022, 22, 10411–10419. [Google Scholar] [CrossRef]
- Jiang, T.; Deng, L.R.; Liang, J.; Wu, Y.; Shao, Z.; Wang, D. Wearable breath monitoring via a hot-film/calorimetric airflow sensing system. Biosens. Bielectronics 2020, 163, 112288. [Google Scholar] [CrossRef]
- Hwang, B.; Han, Y.; Matteini, P. Bending fatigue behavior of Ag nanowire/Cu thin-film hybrid interconnects for wearable electronics. Facta Univ. Ser. Mech. Eng. 2022. [Google Scholar] [CrossRef]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
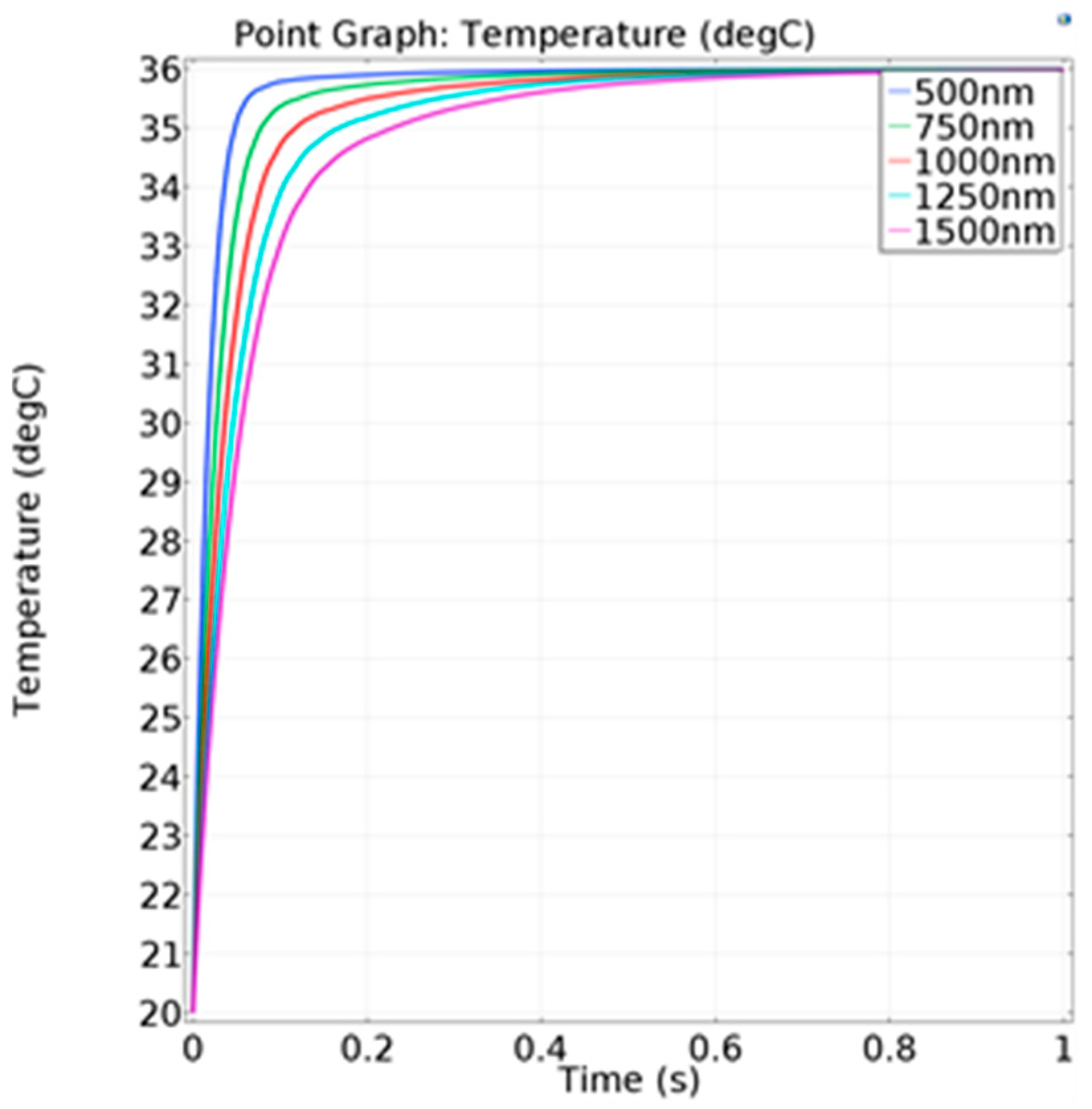
| Thickness of Thermocouple (nm) | Response Time (ms) |
|---|---|
| 500 | 40 |
| 750 | 57 |
| 1000 | 79 |
| 1250 | 104 |
| 1500 | 134 |
| Respiratory Flow (%) | Average Temperature Difference (°C) |
|---|---|
| 100 | 5.17 |
| 90 | 4.70 |
| 80 | 4.10 |
| 70 | 3.50 |
| 60 | 3.21 |
| 50 | 2.45 |
| Thin-Film Thickness (μm) | Average Temperature Difference (°C) |
|---|---|
| 50 | 8.47 |
| 75 | 6.74 |
| 100 | 5.17 |
| 125 | 4.07 |
| 150 | 3.52 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miao, X.; Gao, X.; Su, K.; Li, Y.; Yang, Z. A Flexible Thermocouple Film Sensor for Respiratory Monitoring. Micromachines 2022, 13, 1873. https://doi.org/10.3390/mi13111873
Miao X, Gao X, Su K, Li Y, Yang Z. A Flexible Thermocouple Film Sensor for Respiratory Monitoring. Micromachines. 2022; 13(11):1873. https://doi.org/10.3390/mi13111873
Chicago/Turabian StyleMiao, Xiaodan, Xiang Gao, Kaiming Su, Yahui Li, and Zhuoqing Yang. 2022. "A Flexible Thermocouple Film Sensor for Respiratory Monitoring" Micromachines 13, no. 11: 1873. https://doi.org/10.3390/mi13111873