Passive Wireless Pressure Sensing for Gastric Manometry

Abstract
:1. Introduction
2. Methods and Modeling
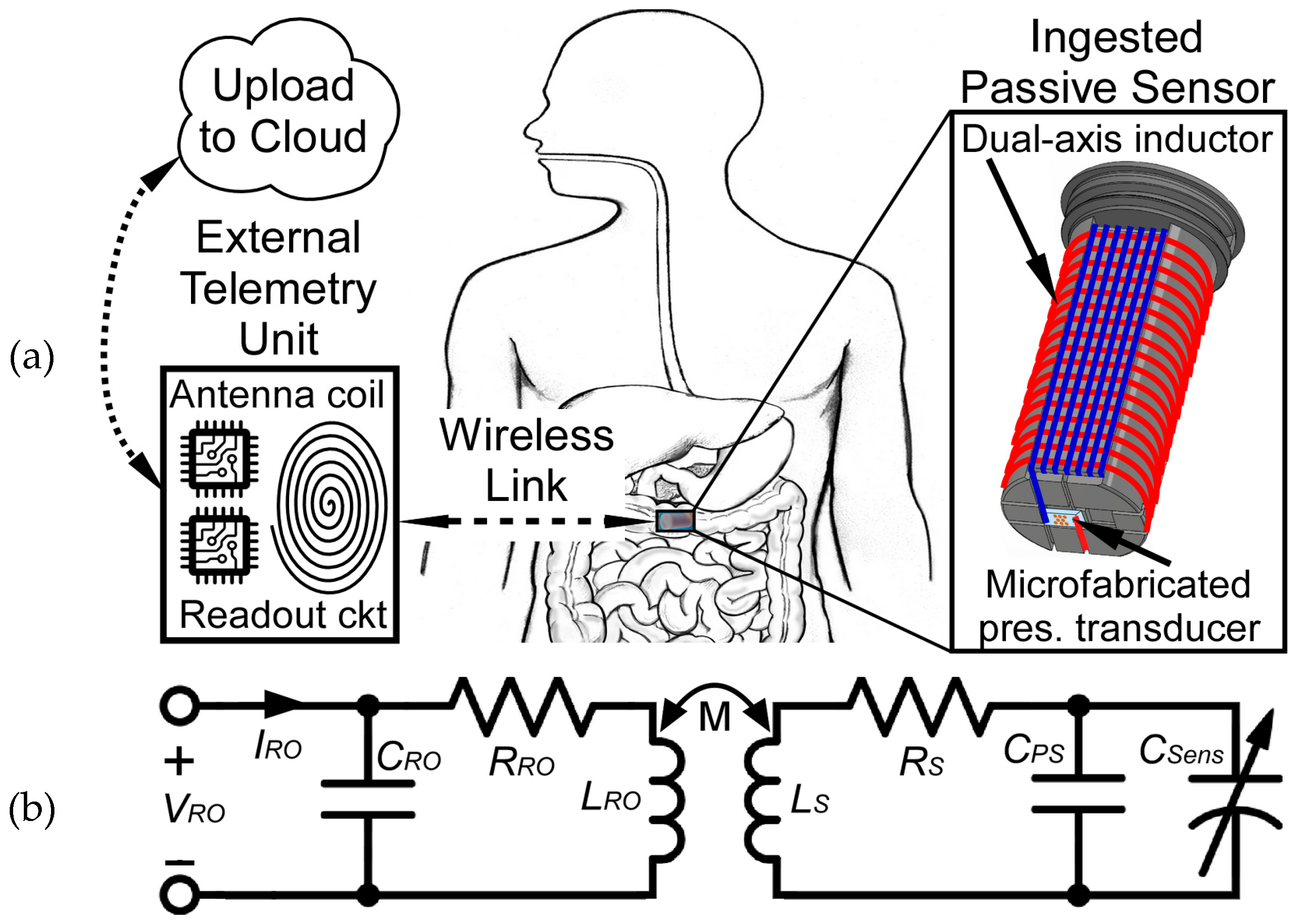
2.1. Inductive Coupling Analysis
2.2. System Design and Fabrication
2.2.1. Sensor and Readout Antenna
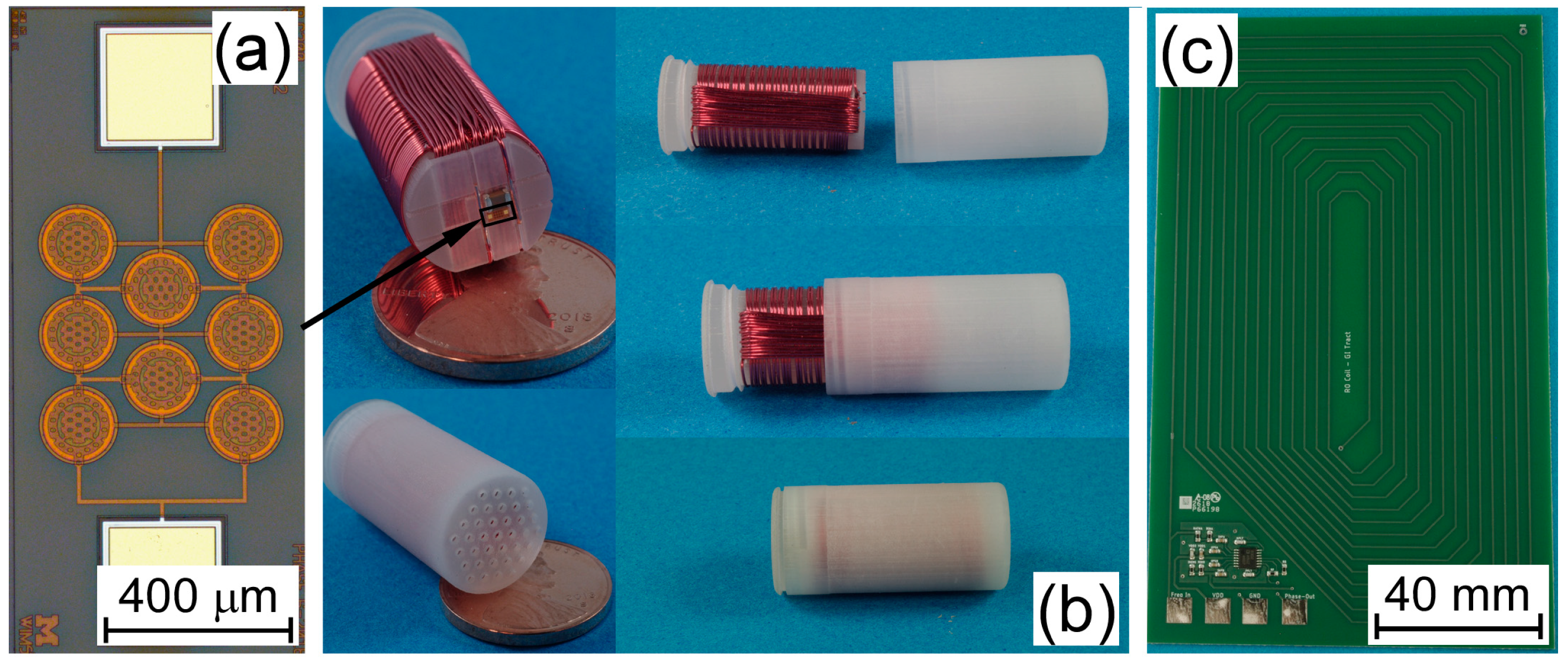
2.2.2. Fabrication
3. Results and Discussions
3.1. Interrogation System
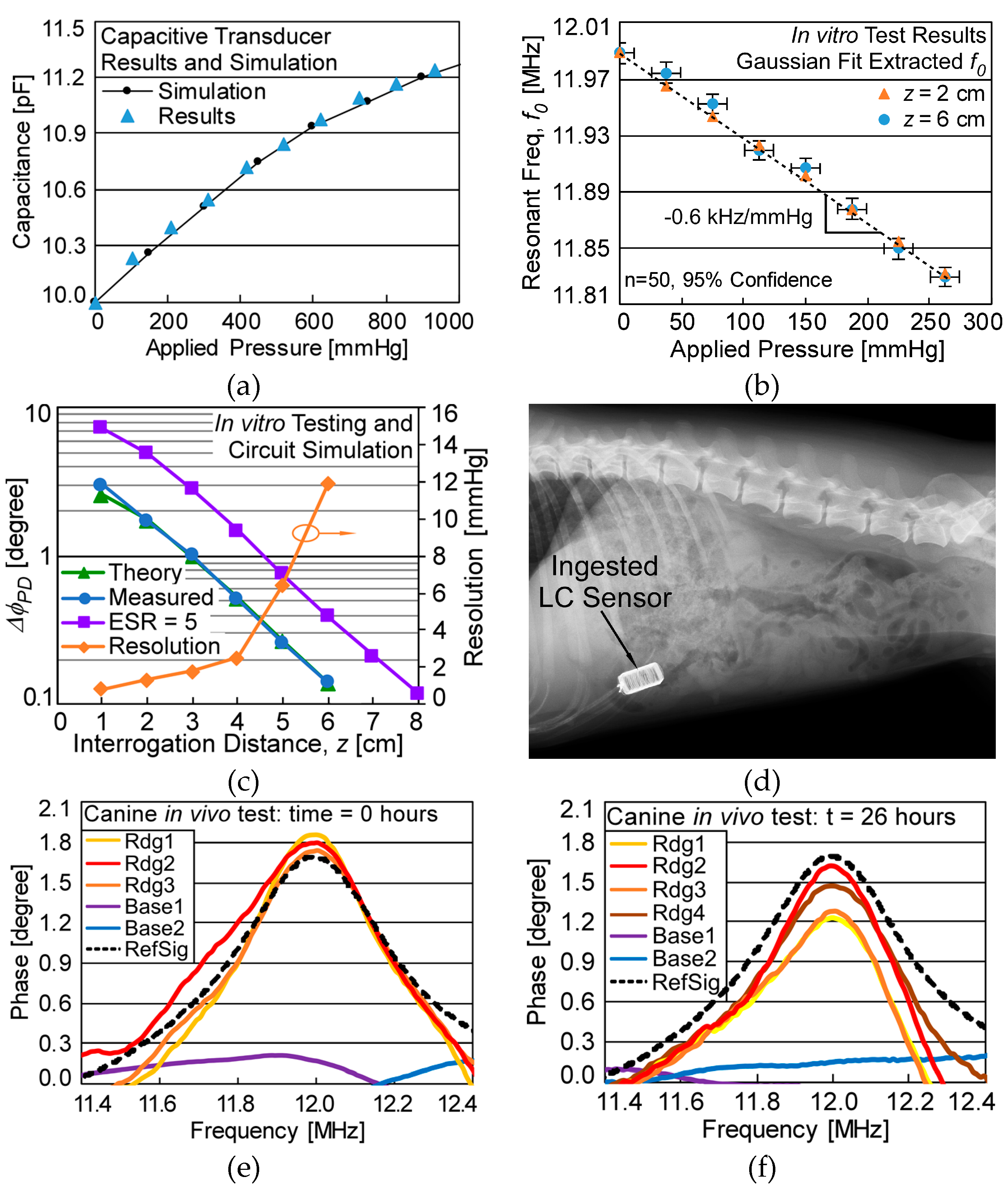
3.2. Measurement Results
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- Wise, K.D. Wireless implantable microsystems: Coming breakthroughs in health care. In Proceedings of the IEEE VLSI Circuit Symposium, Honolulu, HI, USA, 13–15 June 2002; pp. 106–109. [Google Scholar]
- Hasler, W.L.; Wilson, L.A.; Parkman, H.P.; Koch, K.L.; Abell, T.L.; Nguyen, L.; Pasricha, P.J.; Snape, W.J.; McCallum, R.W.; Sarosiek, I.; et al. Factors related to abdominal pain in gastroparesis: Contrast to patients with predominant nausea and vomiting. Neurogastroenterol. Motil. 2013, 25, 427–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abell, T.; Camilleri, M.; Donohoe, K.; Hasler, W.L.; Lin, H.; Maurer, A.; Nowak, T.; Nusynowitz, M.; Parkman, H.; Shreve, P. Consensus recommendations for gastric emptying scintigraphy. Am. J. Gastroenterol. 2008, 103, 753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciuti, G.; Menciassi, A.; Dario, P. Capsule endoscopy: From current achievements to open challenges. IEEE Rev. Biomed. Eng. 2011, 4, 59–72. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.; Yan, G.; Zhao, K.; Lu, L.; Gao, J.; Liu, G. A wireless capsule system with ASIC for monitoring the physiological signals of the human gastrointestinal tract. IEEE Trans. Biomed. Circuits Syst. 2014, 8, 871–880. [Google Scholar] [CrossRef] [PubMed]
- Adler, S.N.; Metzger, Y.C. PillCam COLON capsule endoscopy: Recent advances and new insights. Ther. Adv. Gastroenterol. 2011, 4, 265–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, S.; Camilleri, M.; Hasler, W.L.; Simren, M.; Soffer, E.; Szarka, L. Evaluation of gastrointestinal transit in clinical practice. Neurogastroenterol. Motil. 2011, 23, 8–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalantar-Zadeh, K.; Berean, K.J.; Ha, N.; Chrimes, A.F.; Xu, K.; Grando, D.; Ou, J.Z.; Pillai, N.; Campbell, J.L.; Brkljača, R.; et al. A human pilot trial of ingestible electronic capsules capable of sensing different gases in the gut. Nat. Electron. 2018, 1, 79. [Google Scholar] [CrossRef]
- Collins, C.C. Miniature passive pressure transensor for implanting in the eye. IEEE Trans. Biomed. Eng. 1967, 2, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Takahata, K.; Gianchandani, Y.B.; Wise, K.D. Micromachined antenna stents and cuffs for monitoring intraluminal pressure and flow. IEEE/ASME J. Microelectromech. Syst. 1289. [Google Scholar] [CrossRef] [Green Version]
- Allen, M.G. Micromachined endovascularly-implantable wireless aneurysm pressure sensors: From concept to clinic. In Proceedings of the IEEE International Conference on Solid State Sensors, Actuators, and Microsystem (Transducers), Seoul, Korea, 5–9 June 2005. [Google Scholar]
- DeHennis, A.; Wise, K.D. A double-sided single-chip wireless pressure sensor. In Proceedings of the IEEE/ASME International Conference on Micro Electro Mechanical Systems (MEMS ’02), Las Vegas, NV, USA, 24 January 2002. [Google Scholar]
- Pichorim, S.; Abatti, P. Design of coils for millimeter-and submillimeter-sized biotelemetry. IEEE Trans. Biomed. Eng. 2004, 51, 1487–1489. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, H.A. Formulas for the skin effect. Proc. IRE 1942, 30, 412–424. [Google Scholar] [CrossRef]
- Ferreira, J.A. Improved analytical modeling of conductive losses in magnetic components. IEEE Trans. Power Electron. 1994, 9, 127–131. [Google Scholar] [CrossRef]
- Mohan, S.; Hershenson, M.; Boyd, S.; Lee, T.H. Simple accurate expressions for planar spiral inductances. IEEE J. Solid-State Circuits 1999, 34, 1419–1424. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.H.; Yu, Y.; Yang, Z.; Yu, W.Z.; Chen, W.L.; Yu, H.; Kim, M.J.M.; Huang, M.; Tan, S.; Luo, H.; et al. Intraluminal pressure patterns in the human colon assessed by high-resolution manometry. Sci. Rep. 2017, 7, 41436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- 3D Systems: ProJet MJP 3600 Series. Available online: https://www.3dsystems.com/3d-printers/projet-mjp-3600-series (accessed on 26 October 2018).
- Benken, A. A High-Yield Microfabrication Process for Sapphire Substrate Pressure Sensors with Low Parasitic Capacitances and 200 °C Tolerance. Ph.D. Thesis, University of Michigan, Ann Arbor, MI, USA, 2019. [Google Scholar]
- Analog Devices. LF–2.7 GHz RF/IF Gain and Phase Detector: AD8302 Datasheet; Analog Devices: Norwood, MA, USA, 2002; Revised April 2018. [Google Scholar]
- Candy, J.C.; Temes, G.C. Oversampling methods for data conversion. In Proceedings of the IEEE Pacific Rim Conference on Communications, Computers and Signal Processing Conference, Victoria, BC, Canada, 9–10 May 1991; pp. 498–502. [Google Scholar]
- Abdalla, S.; Al-Ameer, S.S.; Al-Magaishi, S.H. Electrical properties with relaxation through human blood. Biomicrofluidics 2010, 4, 034101. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Equation | |
|---|---|---|
| Complex input impedance | (1) | |
| Input impedance phase | (2) | |
| Phase-dip size at f0, small RRO, CRO | (3) | |
| Quality factor | (4) | |
| Coupling factor | (5) | |
| Resonant frequency | (6) | |
| Parameter | Value |
|---|---|
| z-axis coil dimensions | ø 10 mm × 20 mm |
| z-axis: nS,z, SS,z | 42 turns, 0.16 mm |
| z-axis: LS,z | 6.3 µH (RS,z ≈ 4.5 Ω) |
| x-axis coil dimensions | 9 mm × 19 mm × 5 mm |
| x-axis: nS,x, SS,x | 15 turns, 0.05 mm |
| x-axis: LS,x | 4.7 µH (RS,x ≈ 6.5 Ω) |
| Capacitive transducer, CSens | C0 = 10 pF, (ESR ≈ 50 Ω), ΔC = 1.8 fF/mmHg |
| Low-ESR Cap., CPS | C0 = 5 pF (ESR ≈ 0 Ω) |
| Parasitic Cap., Cpar | ≈1 pF |
| Inductor-capacitor (LC) sensor RS | 30.5 Ω |
| LC sensor response | −0.6 kHz/mmHg |
| Readout coil size | 9 cm × 15 cm |
| nRO, SRO | 14 turns, 2.5 mm |
| Readout coil inductance, LRO | 17.3 µH |
| System resolution, z = 1 cm | 0.8 mmHg |
| t = 0 h | Measured f0 | Interpreted Pressure |
|---|---|---|
| Rdg1 | 11.9892 MHz | −0.8 ± 0.4 mmHg |
| Rdg2 | 11.9902 MHz | −2.6 ± 0.4 mmHg |
| Rdg3 | 11.9880 MHz | 1.2 ± 0.4 mmHg |
| t = 26 h | Measured f0 | Interpreted Pressure |
| Rdg1 | 11.9879 MHz | 1.4 ± 0.6 mmHg |
| Rdg2 | 11.9872 MHz | 2.5 ± 0.5 mmHg |
| Rdg3 | 11.9870 MHz | 2.9 ± 0.6 mmHg |
| Rdg4 | 11.9870 MHz | 2.9 ± 0.5 mmHg |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benken, A.; Gianchandani, Y. Passive Wireless Pressure Sensing for Gastric Manometry. Micromachines 2019, 10, 868. https://doi.org/10.3390/mi10120868
Benken A, Gianchandani Y. Passive Wireless Pressure Sensing for Gastric Manometry. Micromachines. 2019; 10(12):868. https://doi.org/10.3390/mi10120868
Chicago/Turabian StyleBenken, Alexander, and Yogesh Gianchandani. 2019. "Passive Wireless Pressure Sensing for Gastric Manometry" Micromachines 10, no. 12: 868. https://doi.org/10.3390/mi10120868