Development of a Generic PBK Model for Human Biomonitoring with an Application to Deoxynivalenol

 , and
, and
Abstract
:1. Introduction
2. Results
2.1. The DON PBK Model


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Poorly Perfused Organs | Richly Perfused Organs |
|---|---|---|
| Relative volume | 0.58 | 0.09 |
| Relative flow | 0.35 | 0.18 |
2.2. Calculation and Estimation of DON-Related Parameters

2.2.1. Calculation of DON-Related Parameters Based on Data from the Literature
| Parameters | DON | DON-3-GlcA | DON-15-GlcA |
|---|---|---|---|
| Log (Kow) | −9.7 | −5.75 | −5.75 |
| Water solubility | 5.5 × 104 | 5.5 × 104 | 5.5 × 104 |
| Compartment | DON | DON-3-GlcA | DON-15-GlcA |
|---|---|---|---|
| Adipose tissue | 0.1 | 0.1 | 0.1 |
| Poorly perfused | 0.74 | 0.74 | 0.74 |
| Richly perfused | 0.78 | 0.78 | 0.78 |
| Kidney | 0.77 | 0.77 | 0.77 |
| Intestine | 0.52 | 0.52 | 0.52 |
| Liver | 0.52 | 0.52 | 0.52 |
| Lung | 0.74 | 0.74 | 0.74 |
2.2.2. Estimation of DON-Related Parameters by Fitting
| Parameter | DON | DON-3GlcA | DON-15GlcA |
|---|---|---|---|
| Absorption rate constant | 22 (per hour) | ||
| Renal excretion fraction | 0.97 | 3.28 | 3.28 |

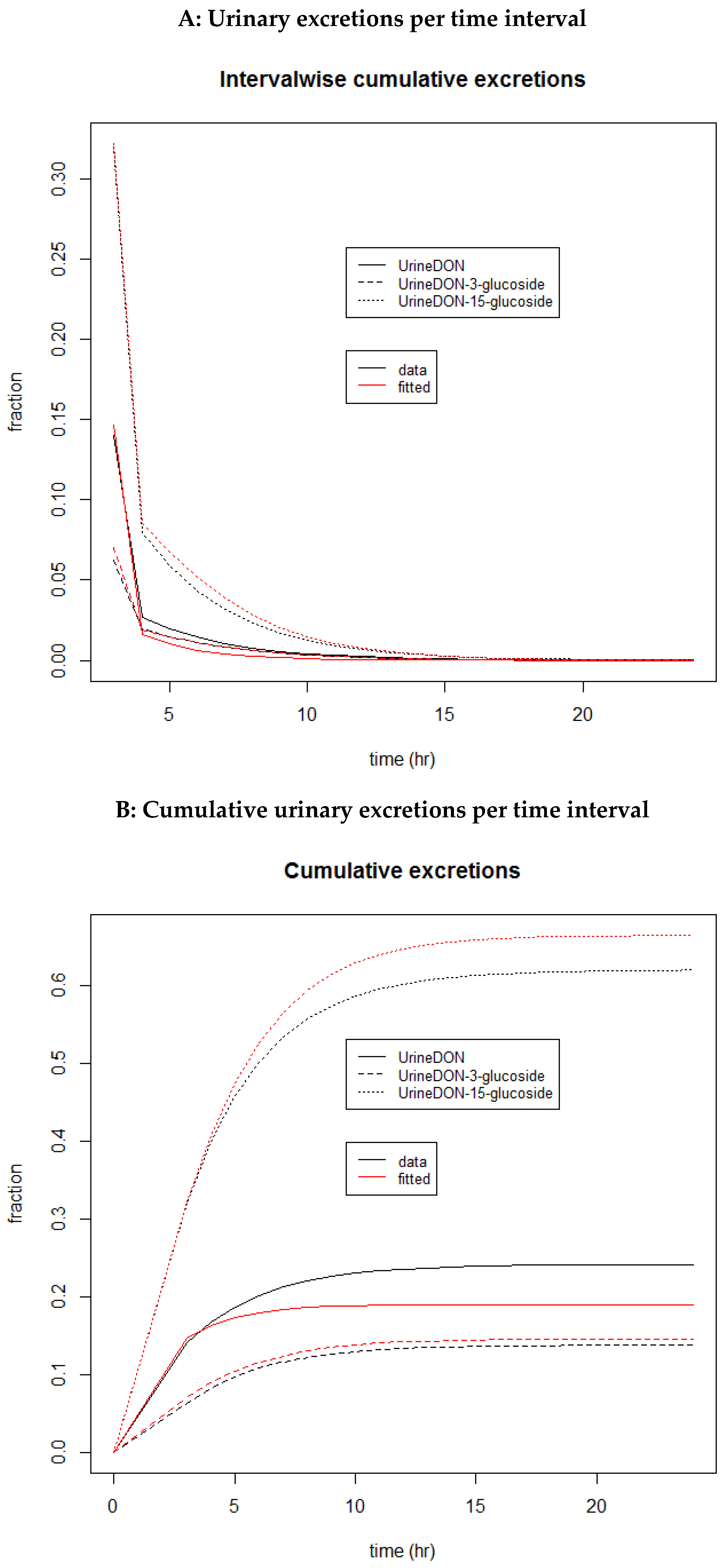
2.3. Illustration of the DON PBK Model

3. Discussion
4. Conclusions
5. Materials and Methods
5.1. General Description of the PBK Model
5.2. DON-Related Parameters
5.2.1. Deriving DON-Related Parameters from the Literature
5.2.2. Deriving DON-Related Parameters by Fitting of ICF Model: Calculation of the PBK-Model Absorption and Renal Excretion Parameters
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- EFSA Panel on Contaminants in the Food Chain. Scientific Opinion on the risks for human and animal health related to the presence of modified forms of certain mycotoxins in food and feed. EFSA J. 2014, 12, 3916. [Google Scholar] [CrossRef]
- Halstensen, A.S.; Nordby, K.C.; Eduard, W.; Klemsdal, S.S. Real-time PCR detection of toxigenic Fusarium in airborne and settled grain dust and associations with trichothecene mycotoxins. J. Environ. Monit. 2006, 8, 1235–1241. [Google Scholar] [CrossRef] [PubMed]
- Straumfors, A.; Mundra, S.; Foss, O.A.H.; Mollerup, S.K.; Kauserud, H. The airborne mycobiome and associations with mycotoxins and inflammatory markers in the Norwegian grain industry. Sci. Rep. 2021, 11, 9357. [Google Scholar] [CrossRef] [PubMed]
- Tangni, E.K.; Pussemier, L. Ergosterol and mycotoxins in grain dusts from fourteen Belgian cereal storages: A preliminary screening survey. J. Sci. Food Agric. 2007, 87, 1263–1270. [Google Scholar] [CrossRef]
- Viegas, C.; Fleming, G.T.A.; Kadir, A.; Almeida, B.; Caetano, L.A.; Quintal Gomes, A.; Twarużek, M.; Kosicki, R.; Viegas, S.; Coggins, A.M. Occupational Exposures to Organic Dust in Irish Bakeries and a Pizzeria Restaurant. Microorganisms 2020, 8, 118. [Google Scholar] [CrossRef]
- Ndaw, S.; Remy, A.; Jargot, D.; Antoine, G.; Denis, F.; Robert, A. Mycotoxins Exposure of French Grain Elevator Workers: Biomonitoring and Airborne Measurements. Toxins 2021, 13, 382. [Google Scholar] [CrossRef]
- EFSA Panel on Contaminants in the Food Chain; Knutsen, H.K.; Alexander, J.; Barregård, L.; Bignami, M.; Brüschweiler, B.; Ceccatelli, S.; Cottrill, B.; Dinovi, M.; Grasl-Kraupp, B.; et al. Risks to human and animal health related to the presence of deoxynivalenol and its acetylated and modified forms in food and feed. EFSA J. 2017, 15, e04718. [Google Scholar] [CrossRef]
- Iverson, F.; Armstrong, C.; Nera, E.; Truelove, J.; Fernie, S.; Scott, P.; Stapley, R.; Hayward, S.; Gunner, S. Chronic feeding study of deoxynivalenol in B6C3F1 male and female mice. Teratog. Carcinog. Mutagen. 1995, 15, 283–306. [Google Scholar] [CrossRef]
- Viegas, S.; Viegas, C.; Martins, C.; Assunção, R. Occupational Exposure to Mycotoxins-Different Sampling Strategies Telling a Common Story Regarding Occupational Studies Performed in Portugal (2012–2020). Toxins 2020, 12, 513. [Google Scholar] [CrossRef]
- Ndaw, S.; Jargot, D.; Antoine, G.; Denis, F.; Melin, S.; Robert, A. Investigating Multi-Mycotoxin Exposure in Occupational Settings: A Biomonitoring and Airborne Measurement Approach. Toxins 2021, 13, 54. [Google Scholar] [CrossRef]
- Brera, C.; de Santis, B.; Debegnach, F.; Miano, B.; Moretti, G.; Lanzone, A.; Del Sordo, G.; Buonsenso, D.; Chiaretti, A.; Hardie, L.; et al. Experimental study of deoxynivalenol biomarkers in urine. EFSA Support. Publ. 2015, 12, 818E. [Google Scholar] [CrossRef]
- Mengelers, M.; Zeilmaker, M.; Vidal, A.; De Boevre, M.; De Saeger, S.; Hoogenveen, R. Biomonitoring of Deoxynivalenol and Deoxynivalenol-3-glucoside in Human Volunteers: Renal Excretion Profiles. Toxins 2019, 11, 466. [Google Scholar] [CrossRef] [PubMed]
- van den Brand, A.D.; Hoogenveen, R.; Mengelers, M.J.B.; Zeilmaker, M.; Eriksen, G.S.; Uhlig, S.; Brantsæter, A.L.; Dirven, H.; Husøy, T. Modelling the Renal Excretion of the Mycotoxin Deoxynivalenol in Humans in an Everyday Situation. Toxins 2021, 13, 675. [Google Scholar] [CrossRef]
- Jongeneelen, F.J.; Berge, W.F. A generic, cross-chemical predictive PBTK model with multiple entry routes running as application in MS Excel; design of the model and comparison of predictions with experimental results. Ann. Occup. Hyg. 2011, 55, 841–864. [Google Scholar] [CrossRef]
- Pletz, J.; Blakeman, S.; Paini, A.; Parissis, N.; Worth, A.; Andersson, A.M.; Frederiksen, H.; Sakhi, A.K.; Thomsen, C.; Bopp, S.K. Physiologically based kinetic (PBK) modelling and human biomonitoring data for mixture risk assessment. Environ. Int. 2020, 143, 105978. [Google Scholar] [CrossRef] [PubMed]
- Jongeneelen, F.; ten Berge, W. Simulation of urinary excretion of 1-hydroxypyrene in various scenarios of exposure to polycyclic aromatic hydrocarbons with a generic, cross-chemical predictive PBTK-model. Int. Arch. Occup. Environ. Health 2012, 85, 689–702. [Google Scholar] [CrossRef] [PubMed]
- Fragki, S.; Piersma, A.H.; Rorije, E.; Zeilmaker, M.J. In vitro to in vivo extrapolation of effective dosimetry in developmental toxicity testing: Application of a generic PBK modelling approach. Toxicol. Appl. Pharmacol. 2017, 332, 109–120. [Google Scholar] [CrossRef]
- OECD. Guidance Document on the Characterisation, Validation and Reporting of PBK Models for Regulatory Purposes. OECD series on Testing and Assessment No. 331; Environment, Health and Safety, Environment Directorate, OECD: Paris, France, 2021. [Google Scholar]
- International Programme on Chemical Safety Inter-Organization Programme for the Sound Management of Chemicals. Characterization and Application of Physiologically Based Pharmacokinetic Models in Risk Assessment; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Paini, A.; Tan, Y.M.; Sachana, M.; Worth, A. Gaining acceptance in next generation PBK modelling approaches for regulatory assessments—An OECD international effort. Comput. Toxicol. 2021, 18, 100163. [Google Scholar] [CrossRef]
- Jongeneelen, F.; Ten Berge, W. IndusChemFate: A Multi-Chemical PBTK-Model in MS-Excel Applicable for Workers, Consumers and Experimental Animals User Manual; Version 2.00; IndusTox Consult: Nijmegen, The Netherlands, 2011. [Google Scholar]
- Maresca, M. From the gut to the brain: Journey and pathophysiological effects of the food-associated trichothecene mycotoxin deoxynivalenol. Toxins 2013, 5, 784–820. [Google Scholar] [CrossRef]
- Fæste, C.K.; Ivanova, L.; Sayyari, A.; Hansen, U.; Sivertsen, T.; Uhlig, S. Prediction of deoxynivalenol toxicokinetics in humans by in vitro-to-in vivo extrapolation and allometric scaling of in vivo animal data. Arch. Toxicol. 2018, 92, 2195–2216. [Google Scholar] [CrossRef]
- EFSA Panel on Contaminants in the Food Chain; Arcella, D.; Gergelova, P.; Innocenti, M.L.; Steinkellner, H. Human and animal dietary exposure to T-2 and HT-2 toxin. EFSA J. 2017, 15, e04972. [Google Scholar] [CrossRef] [PubMed]
- Burdorf, A.; Lillienberg, L.; Brisman, J. Characterization of exposure to inhalable flour dust in Swedish bakeries. Ann. Occup. Hyg. 1994, 38, 67–78. [Google Scholar] [CrossRef] [PubMed]
- Giesecke, A. Air Emission Calculation for Particulate Matter: Flour. Available online: https://www.bakingbusiness.com/articles/26149-air-emission-calculation-for-particulate-matter-flour (accessed on 5 December 2021).
- Laurière, M.; Gorner, P.; Bouchez-Mahiout, I.; Wrobel, R.; Breton, C.; Fabriès, J.F.; Choudat, D. Physical and biochemical properties of airborne flour particles involved in occupational asthma. Ann. Occup. Hyg. 2008, 52, 727–737. [Google Scholar] [CrossRef] [PubMed]
- Miller, F.J.; Asgharian, B.; Schroeter, J.D.; Price, O. Improvements and additions to the multiple path particle dosimetry model. J. Aerosol Sci. 2016, 99, 14–26. [Google Scholar] [CrossRef]
- Barnes, H.; Troy, L.; Lee, C.T.; Sperling, A.; Strek, M.; Glaspole, I. Hypersensitivity pneumonitis: Current concepts in pathogenesis, diagnosis, and treatment. Allergy 2022, 77, 442–453. [Google Scholar] [CrossRef]
- Sorenson, W.G. Fungal spores: Hazardous to health? Environ. Health Perspect. 1999, 107 (Suppl. 3), 469–472. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Notenboom, S.; Hoogenveen, R.T.; Zeilmaker, M.J.; Van den Brand, A.D.; Assunção, R.; Mengelers, M.J.B. Development of a Generic PBK Model for Human Biomonitoring with an Application to Deoxynivalenol. Toxins 2023, 15, 569. https://doi.org/10.3390/toxins15090569
Notenboom S, Hoogenveen RT, Zeilmaker MJ, Van den Brand AD, Assunção R, Mengelers MJB. Development of a Generic PBK Model for Human Biomonitoring with an Application to Deoxynivalenol. Toxins. 2023; 15(9):569. https://doi.org/10.3390/toxins15090569
Chicago/Turabian StyleNotenboom, Sylvia, Rudolf T. Hoogenveen, Marco J. Zeilmaker, Annick D. Van den Brand, Ricardo Assunção, and Marcel J. B. Mengelers. 2023. "Development of a Generic PBK Model for Human Biomonitoring with an Application to Deoxynivalenol" Toxins 15, no. 9: 569. https://doi.org/10.3390/toxins15090569