Botulinum Toxin—A High-Dosage Effect on Functional Outcome and Spasticity-Related Pain in Subjects with Stroke

 , and
, and
Abstract
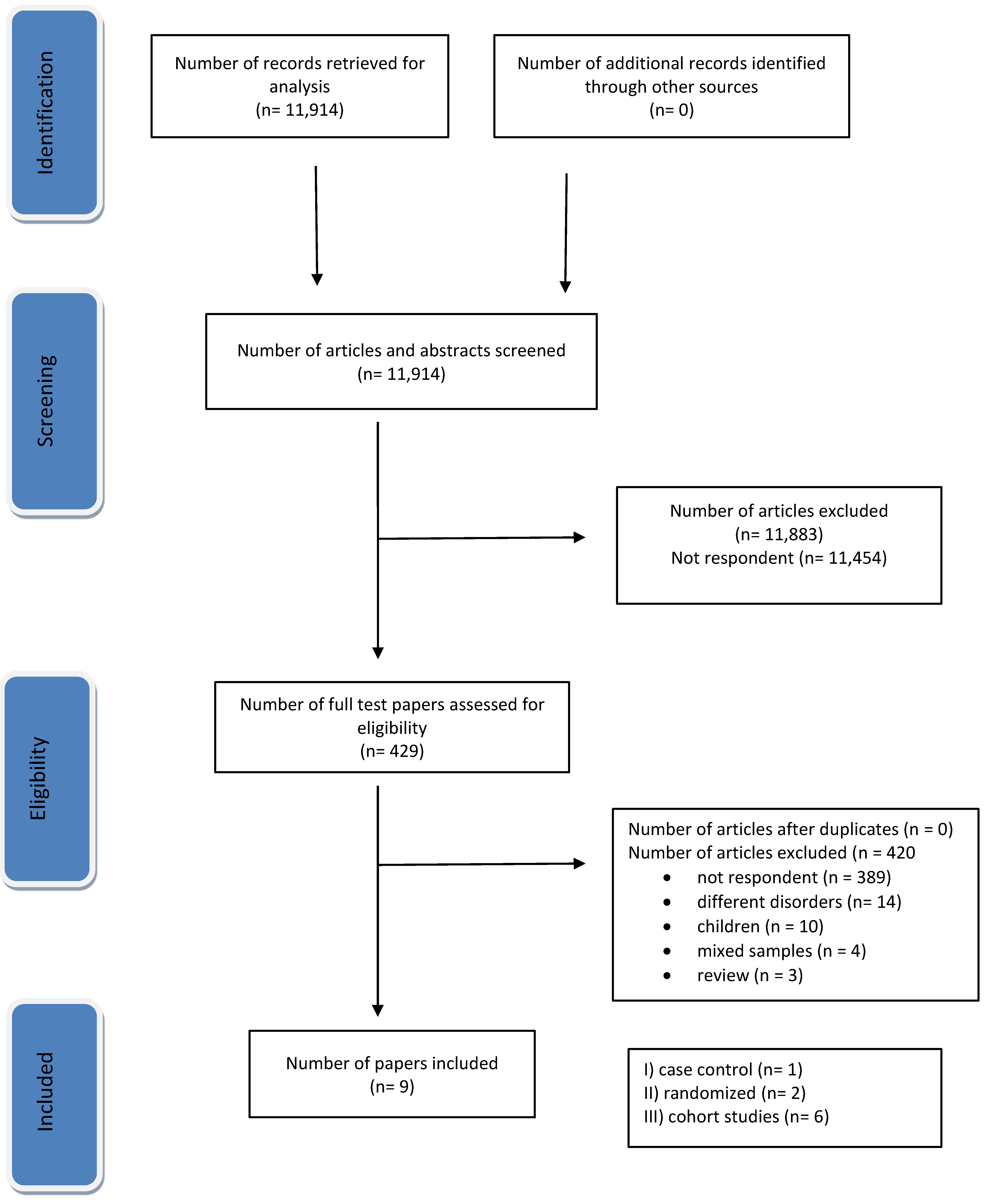
:1. Introduction
2. Results
2.1. Functional Outcome
2.2. Spasticity-Related Pain

{kind=link}
| Study | Design | Patients/Sex/ Age | BTX-A Doses and Guidance/Follow-Up | Functional Measures and SRP Evaluation | Effect on Spasticity-Related Pain | Effect on Spasticity and Functional Outcome |
|---|---|---|---|---|---|---|
| Mancini et al., 2005 [25] | randomized, double-blind, study | N = 45 pts; N = 15 pts with onaBTX-A high dosage; (M 8, F 7) mean age 63.2 ± 10.1 | onaBTX-A (Botox) 540 ± 124.2 U; EMG; 4 months | MRC; MAS; VAS GT; GV; | improvement of pain | prolonged effect of BTX on spasticity, GV, gait function, pain, and presence of clonus |
| Santamato et al., 2013 [26] | prospective | N = 25 12 F, 8 M; age (range 45–71 years) | incoBTX-A (Xeomin) 840 U (ranged from 750 to 840 U) in both UL and LL; UL muscles received a dosage of a maximum of 540 U; 340 U was administered in LL (range 250–340 U); US; 3 months | AS; DAS; GATR; VAS | improvement of SRP was observed for all patients | improvement of disability and muscle tone. Significant decrease evaluated after 30 and 90 days from the treatment (p < 0.05) to functional measures |
| Invernizzi et al., 2014 [27] | case control | N = 11; 5 M, 6 F; age from 44 to 72 years | incoBTX-A (Xeomin) higher 600 U; 12 U/kg (range 600–800); NR | AS > 2; ECG for HRV (RR interval) | N/A | N/A |
| Baricich et al., 2015 [28] | cohort; retrospective | N = 26; M 13, F 13; mean age 54.7 ± 11.6 | onaBTX-A (Botox) 600 IU; 13 pts > 700 IU; mean dose 676.9 ± 86.3 IU; US; 23 pts were treated at both upper and lower limbs; 3 months | MAS; DAS; GAE | N/A | significant reduction of spasticity (p < 0.0001). Improvement in DAS and GAE |
| Santamato et al., 2017 [29] | cohort; prospective | 25 pts; 20 (12 F, 8 M); mean age 60.8 ± 7.8 | incoBTX-A (Xeomin); 830 U (ranged from 750 U to 830 U) in both upper and lower limb; US; UL received a dosage of a maximum of 560 U and LL a dosage of a maximum of 460 U (ranged from 260 U to 460 U); 2 years | AS; DAS GATR | the rate of patients that chose pain as the primary target of DAS was increased compared to the baseline: 39% and 24%, respectively | improvements as assessed on clinical scales for spasticity (AS), disability (DAS), and global assessment of treatment response (GATR) |
| Wissel et al., 2017 [30] | prospective, single-arm, dose-titration study | mixed sample N = 155 pts M 104; F 51; mean age 53.7 ± 13.1 N = 132 with stroke; N = 23 other causes ^ | incoBTX-A (Xeomin); 400 to 800 IU; 36–48 weeks | AS; REPAS; GAS; | N/A | dosage up to 800 U was associated with increased treatment efficacy, improved muscle tone, and goal attainment |
| Baricich et al., 2017 [31] | single-blind randomized controlled crossover study design | 10 pts; 7 M, 3 F; age 69 ± 10.5 | N = 5 onaBTX-A (Botox) 600 U (670 ± 83.67); N = 5 incoBTX-A (Xeomin) (660 ± 89.44); doses below 12 U/Kg | AS; BI; MI; FAC | N/A | N/A |
| Ianieri et al., 2018 [32] | cohort, retrospective | mixed sample ° N = 120 N = 58 M 28, F 22; mean age 66 ± 3.2 | incoBTX-A (Xeomin) N = 58 received 700–1000 U (from 775.65 ± 30.45 to 986.65 ± 13.67); NR; 2 years | AS; FIM; MyotonPRO | N/A | reduction of spasticity and statistical improvement of FIM in 10 patients treated by 100–400 UI when the dosage increased up to 700 U |
| Chiu SY et al., 2020 [33] | cohort, retrospective | mixed sample N = 68 pts F 43, M 25; N = 24 with spasticity *, N = 44 with dystonia | onaBTX-A (Botox) > 400 U receiving doses up to 800 U (range 425–800); 12 up 86 months | CGIS | N/A | all patients had a reduction of spasticity after the first treatment and the duration of benefit was 8.8 weeks ± 3.1 |
3. Discussion
4. Conclusions
5. Materials and Methods
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kong, K.H.; Lee, J.; Chua, K.S. Occurrence and Temporal Evolution of Upper Limb Spasticity in Stroke Patients Admitted to a Rehabilitation Unit. Arch. Phys. Med. Rehabil. 2012, 93, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Lance, J.W.; Feldman, R.G.; Young, R.R.; Koeller, C. Spasticity: Disordered Motor Control; Yearbook Medical: Chicago, IL, USA, 1980; pp. 485–494. [Google Scholar]
- Andringa, A.; van Wegen, E.; van de Port, I.; Kwakkel, G.; Meskers, C. Measurement Properties of the NeuroFlexor Device for Quantifying Neural and Non-neural Components of Wrist Hyper-Resistance in Chronic Stroke. Front. Neurol. 2019, 10, 730. [Google Scholar] [CrossRef]
- Brashear, A.; Gordon, M.F.; Elovic, E.; Kassicieh, V.D.; Marciniak, C.; Do, M.; Lee, C.-H.; Jenkins, S.; Turkel, C. Intramuscular Injection of Botulinum Toxin for the Treatment of Wrist and Finger Spasticity after a Stroke. N. Engl. J. Med. 2002, 347, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Pirazzini, M.; Azarnia Tehran, D.; Zanetti, G.; Megighian, A.; Scorzeto, M.; Fillo, S.; Shone, C.C.; Binz, T.; Rossetto, O.; Lista, F.; et al. Thioredoxin and its reductase are present on synaptic vesicles, and their inhibition prevents the paralysis induced by botulinum neurotoxins. Cell Rep. 2014, 8, 1870–1878. [Google Scholar] [CrossRef]
- Tehran, D.A.; Pirazzini, M.; Leka, O.; Mattarei, A.; Lista, F.; Binz, T.; Rossetto, O.; Montecucco, C. Hsp90 is involved in the entry of clostridial neurotoxins into the cytosol of nerve terminals. Cell. Microbiol. 2017, 19, e12647. [Google Scholar] [CrossRef] [PubMed]
- Kaya, C.S.; Yılmaz, E.O.; Akdeniz-Doğan, Z.D.; Yucesoy, C.A. Long-Term effects with potential clinical importance of Botulinum Toxin Type-A on mechanics of muscles exposed. Front. Bioeng. Biotechnol. 2020, 8, 738. [Google Scholar] [CrossRef]
- Zhang, S.; Masuyer, G.; Zhang, J.; Shen, Y.; Lundin, D.; Henriksson, L.; Miyashita, S.-I.; Martínez-Carranza, M.; Dong, M.; Stenmark, P. Identification and characterization of a novel botulinum neurotoxin. Nat. Commun. 2017, 8, 14130. [Google Scholar] [CrossRef]
- Zornetta, I.; Tehran, D.A.; Arrigoni, G.; Anniballi, F.; Bano, L.; Leka, O.; Zanotti, G.; Binz, T.; Montecucco, C. The first non Clostridial botulinum-like toxin cleaves VAMP within the juxtamembrane domain. Sci. Rep. 2016, 6, 30257. [Google Scholar] [CrossRef]
- Azarnia Terhan, D.; Pirazzini, M. Novel Botulinum Neurotoxins: Exploring Underneath the Iceberg Tip. Toxins 2018, 10, 190. [Google Scholar]
- Francisco, G.E. Botulinum toxin: Dosing and dilution. Am. J. Phys. Med. Rehabil. 2004, 83, S30–S37. [Google Scholar] [CrossRef]
- Wissel, J.; Ward, A.B.; Erztgaard, P.; Bensmail, D.; Hecht, M.J.; Lejeune, T.M.; Schnider, P.; Altavista, M.C.; Cavazza, S.; Deltombe, T.; et al. European consensus table on the use of botulinum toxin type A in adult spasticity. J. Rehabil. Med. 2009, 41, 13–25. [Google Scholar] [CrossRef]
- Rekand, T.; Biering-Sörensen, B.; He, J.; Vilholm, O.J.; Christensen, P.B.; Ulfarsson, T.; Belusa, R.; Ström, T.; Myrenfors, P.; Maisonobe, P.; et al. Botulinum toxin treatment of spasticity targeted to muscle endplates: An international, randomised, evaluator-blinded study comparing two different botulinum toxin injection strategies for the treatment of upper limb spasticity. BMJ Open 2019, 9, e024340. [Google Scholar] [CrossRef] [PubMed]
- Dressler, D.; Saberi, F.A.; Kollewe, K.; Schrader, C. Safety aspects of incobotulinum toxinA high-dose therapy. J. Neural Transm. 2015, 122, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Intiso, D.; Simone, V.; Di Rienzo, F.; Iarossi, A.; Pazienza, L.; Santamato, A.; Maruzzi, G.; Basciani, M. High doses of a new botulinum toxin type A (NT-201) in adult patients with severe spasticity following brain injury and cerebral palsy. Neurorehabilitation 2014, 34, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Santamato, A.; Micello, M.F.; Ranieri, M.; Valeno, G.; Albano, A.; Baricich, A.; Cisari, C.; Intiso, D.; Pilotto, A.; Logroscino, G.; et al. Employment of higher doses of botulinum toxin type A to reduce spasticity after stroke. J. Neurol. Sci. 2015, 350, 1–6. [Google Scholar] [CrossRef]
- Intiso, D.; Simone, V.; Bartolo, M.; Santamato, A.; Ranieri, M.; Gatta, M.T.; Di Rienzo, F. High Dosage of Botulinum Toxin Type A in Adult Subjects with Spasticity Following Acquired Central Nervous System Damage: Where Are We at? Toxins 2020, 12, 315. [Google Scholar] [CrossRef]
- Asan, F.; Gündüz, A.; Tütüncü, M.; Uygunoğlu, U.; Savrun, F.K.; Saip, S.; Siva, A. Treatment of multiple sclerosis–related trigeminal neuralgia with onabotulinumtoxinA. Headache 2022, 62, 1322–1328. [Google Scholar] [CrossRef]
- Lippi, L.; de Sire, A.; Folli, A.; D’abrosca, F.; Grana, E.; Baricich, A.; Carda, S.; Invernizzi, M. Multidimensional Effectiveness of Botulinum Toxin in Neuropathic Pain: A Systematic Review of Randomized Clinical Trials. Toxins 2022, 14, 308. [Google Scholar] [CrossRef]
- Hary, V.; Schitter, S.; Martinez, V. Efficacy and safety of botulinum A toxin for the treatment of chronic peripheral neuropathic pain: A systematic review of randomized controlled trials and meta-analysis. Eur. J. Pain 2022, 26, 980–990. [Google Scholar] [CrossRef]
- Gupta, A.D.; Edwards, S.; Smith, J.; Snow, J.; Visvanathan, R.; Tucker, G.; Wilson, D. A Systematic Review and Meta-Analysis of Efficacy of Botulinum Toxin A for Neuropathic Pain. Toxins 2022, 14, 36. [Google Scholar] [CrossRef]
- Baker, J.A.; Pereira, G. The efficacy of Botulinum Toxin A for spasticity and pain in adults: A systematic review and meta-analysis using the Grades of Recommendation, Assessment, Development and Evaluation approach. Clin. Rehabil. 2013, 27, 1084–1096. [Google Scholar] [CrossRef]
- Wissel, J.; Camões-Barbosa, A.; Comes, G.; Althaus, M.; Scheschonka, A.; Simpson, D.M. Pain Reduction in Adults with Limb Spasticity Following Treatment with IncobotulinumtoxinA: A Pooled Analysis. Toxins 2021, 13, 887. [Google Scholar] [CrossRef]
- Brown, E.A.; Schütz, S.G.; Simpson, D.M. Botulinum toxin for neuropathic pain and spasticity: An overview. Pain Manag. 2014, 4, 129–151. [Google Scholar] [CrossRef] [PubMed]
- Mancini, F.; Sandrini, G.; Moglia, A.; Nappi, G.; Pacchetti, C. A randomised, double-blind, dose-ranging study to evaluate efficacy and safety of three doses of botulinum toxin type A (Botox) for the treatment of spastic foot. Neurol. Sci. 2015, 26, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Santamato, A.; Panza, F.; Ranieri, M.; Frisardi, V.; Micello, M.F.; Filoni, S.; Fortunato, F.; Intiso, D.; Basciani, M.; Logroscino, G.; et al. Efficacy and safety of higher doses of botulinum toxin type A NT 201 free from complexing proteins in the upper and lower limb spasticity after stroke. J. Neural Transm. 2013, 120, 469–476. [Google Scholar] [CrossRef]
- Invernizzi, M.; Carda, S.; Molinari, C.; Stagno, D.; Cisari, C.; Baricich, A. Heart Rate Variability (HRV) modifications in adult hemiplegic patients after botulinum toxin type A (nt-201) injection. Eur. J. Phys. Rehabil. Med. 2015, 51, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Baricich, A.; Grana, E.; Carda, S.; Santamato, A.; Cisari, C.; Invernizzi, M. High doses of onabotulinumtoxinA in post-stroke spasticity: A retrospective analysis. J. Neural Transm. 2015, 122, 1283–1287. [Google Scholar] [CrossRef]
- Santamato, A.; Panza, F.; Intiso, D.; Baricich, A.; Picelli, A.; Smania, N.; Fortunato, F.; Seripa, D.; Fiore, P.; Ranieri, M. Long-term safety of repeated high doses of incobotulinumtoxinA injections for the treatment of upper and lower limb spasticity after stroke. J. Neurol. Sci. 2017, 378, 182–186. [Google Scholar] [CrossRef]
- Wissel, J.; Bensmail, D.; Ferreira, J.J.; Molteni, F.; Satkunam, L.; Moraleda, S.; Rekand, T.; McGuire, J.; Scheschonka, A.; Flatau-Baqué, B.; et al. Tower study investigators. Safety and efficacy of incobotulinumtoxinA doses up to 800 U in limb spasticity: The TOWER study. Neurology 2017, 88, 1321–1328. [Google Scholar] [CrossRef]
- Baricich, A.; Grana, E.; Carda, S.; Santamato, A.; Molinari, C.; Cisari, C.; Invernizzi, M. Heart Rate Variability modifications induced by high doses of incobotulinumtoxinA and onabotulinumtoxinA in hemiplegic chronic stroke patients: A single blind randomized controlled, crossover pilot study. Toxicon 2017, 138, 145–150. [Google Scholar] [CrossRef]
- Ianieri, G.; Marvulli, R.; Gallo, G.A.; Fiore, P.; Megna, M. “Appropriate Treatment” and Therapeutic Window in Spasticity Treatment with IncobotulinumtoxinA: From 100 to 1000 Units. Toxins 2018, 10, 140. [Google Scholar] [CrossRef] [PubMed]
- Chiu, S.Y.; Patel, B.; Burns, M.R.; Legacy, J.; Shukla, A.W.; Ramirez-Zamora, A.; Deeb, W.; Malaty, I.A. High-dose Botulinum Toxin Therapy: Safety, Benefit, and Endurance of Efficacy. Tremor Other Hyperkinetic Mov. 2020, 10. [Google Scholar] [CrossRef]
- Dressler, D. Routine use of Xeomin® in patients previously treated with Botox®: Long term results. Eur. J. Neurol. 2009, 16 (Suppl. S2), 2–5. [Google Scholar] [CrossRef] [PubMed]
- Kirshblum, S.; Solinsky, R.; Jasey, N.; Hampton, S.; Didesch, M.; Seidel, B.; Botticello, A. Adverse Event Profiles of High Dose Botulinum Toxin Injections for Spasticity. PM&R 2020, 12, 349–355. [Google Scholar] [CrossRef]
- Pavone, V.; Testa, G.; Restivo, D.A.; Cannavo, L.; Condorelli, G.; Portinaro, N.M.; Sessa, G. Botulinumtoxin treatment for limb spasticity in childhood cerebral palsy. Front. Pharmacol. 2016, 7, 29. [Google Scholar] [CrossRef]
- Bethoux, F. Spasticity Management after Stroke. Phys. Med. Rehabil. Clin. N. Am. 2015, 26, 625–639. [Google Scholar] [CrossRef]
- Intiso, D.; Simone, V.; Di Rienzo, F.; Santamato, A.; Russo, M.; Tolfa, M.; Basciani, M. Does Spasticity Reduction by Botulinum Toxin Type A Improve Upper Limb Functionality in Adult Post-Stroke Patients? A Systematic Review of Relevant Studies. J. Neurol. Neurophysiol. 2013, 4, 1–12. [Google Scholar] [CrossRef]
- Foley, N.; Pereira, S.; Salter, K.; Fernandez, M.M.; Speechley, M.; Sequeira, K.; Miller, T.; Teasell, R. Treatment with Botulinum Toxin Improves Upper-Extremity Function Post Stroke: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2013, 94, 977–989. [Google Scholar] [CrossRef]
- Santamato, A.; Ranieri, M.; Solfrizzi, V.; Lozupone, M.; Vecchio, M.; Daniele, A.; Greco, A.; Seripa, D.; Logroscino, G.; Panza, F. High doses of incobotulinumtoxinA for the treatment of post-stroke spasticity: Are they safe and effective? Expert Opin. Drug Metab. Toxicol. 2016, 12, 843–846. [Google Scholar] [CrossRef]
- Baricich, A.; Picelli, A.; Santamato, A.; Carda, S.; de Sire, A.; Smania, N.; Cisari, C.; Invernizzi, M. Safety Profile of High-Dose Botulinum Toxin Type A in Post-Stroke Spasticity Treatment. Clin. Drug Investig. 2018, 38, 991–1000. [Google Scholar] [CrossRef]
- López de Munain, L.; Valls-Solé, J.; Garcia Pascual, I.; Maisonobe, P.; on behalf of the VALGAS investigators group. Botulinum Toxin Type A Improves Function According to Goal Attainment in Adults with Poststroke Lower Limb Spasticity in Real Life Practice. Eur. Neurol. 2019, 82, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Picelli, A.; Baricich, A.; Cisari, C.; Paolucci, S.; Smania, N.; Sandrini, G. The Italian real-life post-stroke spasticity survey: Unmet needs in the management of spasticity with botulinum toxin type A. Funct. Neurol. 2017, 32, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Woldag, H.; Hummelsheim, H. Is the reduction of spasticity by botulinum toxin a beneficial for the recovery of motor function of arm and 528 hand in stroke patients? Eur. Neurol. 2003, 50, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Lazzaro, C.; Baricich, A.; Picelli, A.; Caglioni, P.; Ratti, M.; Santamato, A. AbobotulinumtoxinA and rehabilitation vs rehabilitation alone in post-stroke spasticity: An cost-utility analysis. J. Rehabil. Med. 2020, 52, jrm00016. [Google Scholar] [CrossRef] [PubMed]
- Shackley, P.; Shaw, L.; Price, C.; Van Wijck, F.; Barnes, M.; Graham, L.; Ford, G.A.; Steen, N.; Rodgers, H. Cost-Effectiveness of Treating Upper Limb Spasticity Due to Stroke with Botulinum Toxin Type A: Results from the Botulinum Toxin for the Upper Limb after Stroke (BoTULS) Trial. Toxins 2012, 4, 1415–1426. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Intiso, D.; Centra, A.M.; Gravina, M.; Chiaramonte, A.; Bartolo, M.; Di Rienzo, F. Botulinum Toxin—A High-Dosage Effect on Functional Outcome and Spasticity-Related Pain in Subjects with Stroke. Toxins 2023, 15, 509. https://doi.org/10.3390/toxins15080509
Intiso D, Centra AM, Gravina M, Chiaramonte A, Bartolo M, Di Rienzo F. Botulinum Toxin—A High-Dosage Effect on Functional Outcome and Spasticity-Related Pain in Subjects with Stroke. Toxins. 2023; 15(8):509. https://doi.org/10.3390/toxins15080509
Chicago/Turabian StyleIntiso, Domenico, Antonello Marco Centra, Michele Gravina, Angelo Chiaramonte, Michelangelo Bartolo, and Filomena Di Rienzo. 2023. "Botulinum Toxin—A High-Dosage Effect on Functional Outcome and Spasticity-Related Pain in Subjects with Stroke" Toxins 15, no. 8: 509. https://doi.org/10.3390/toxins15080509