Long-Term Muscular Atrophy and Weakness Following Cessation of Botulinum Toxin Type A Injections in the Flexor Digitorum Muscle of Musicians with Focal Hand Dystonia


Abstract
:1. Introduction
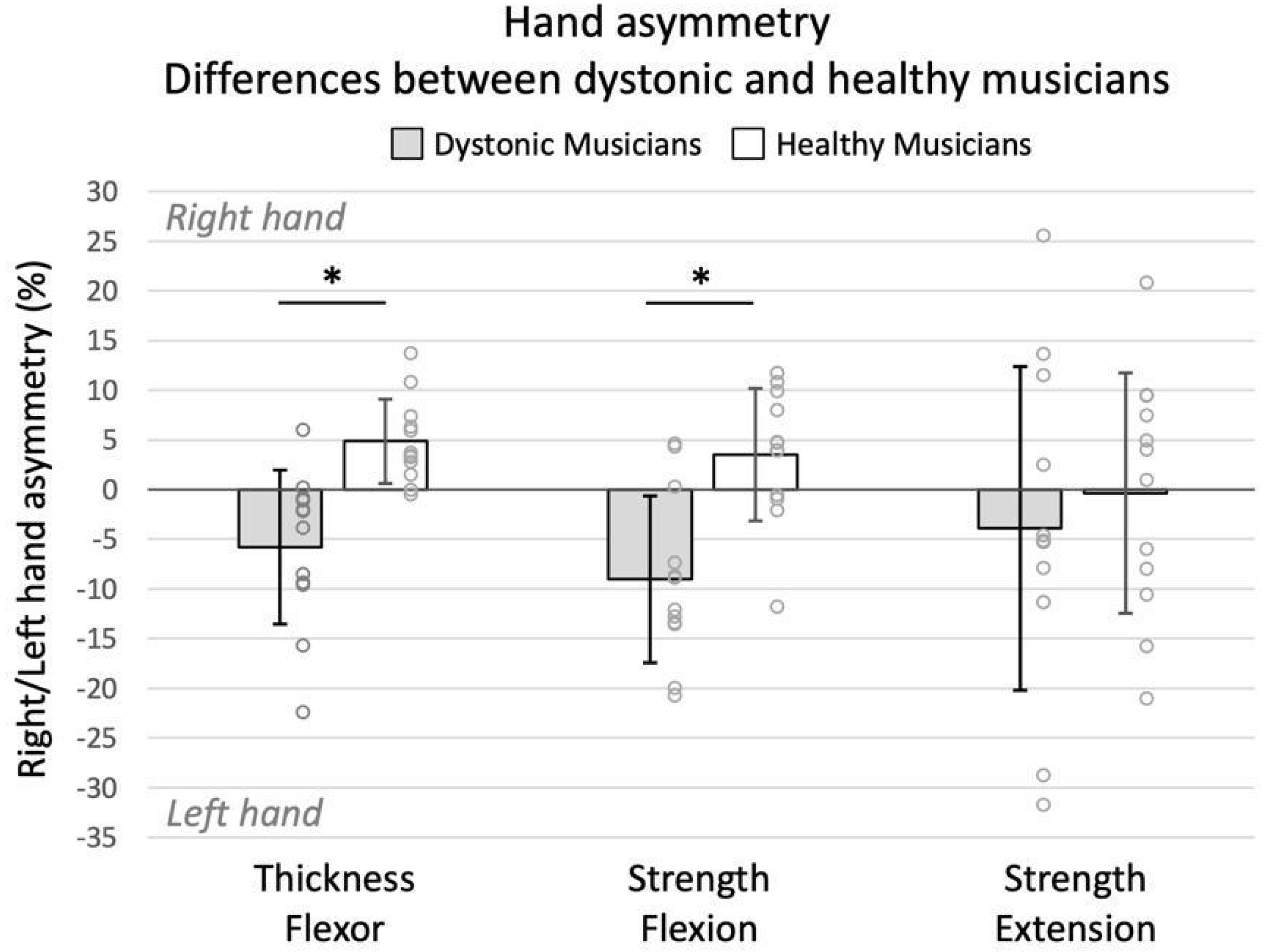
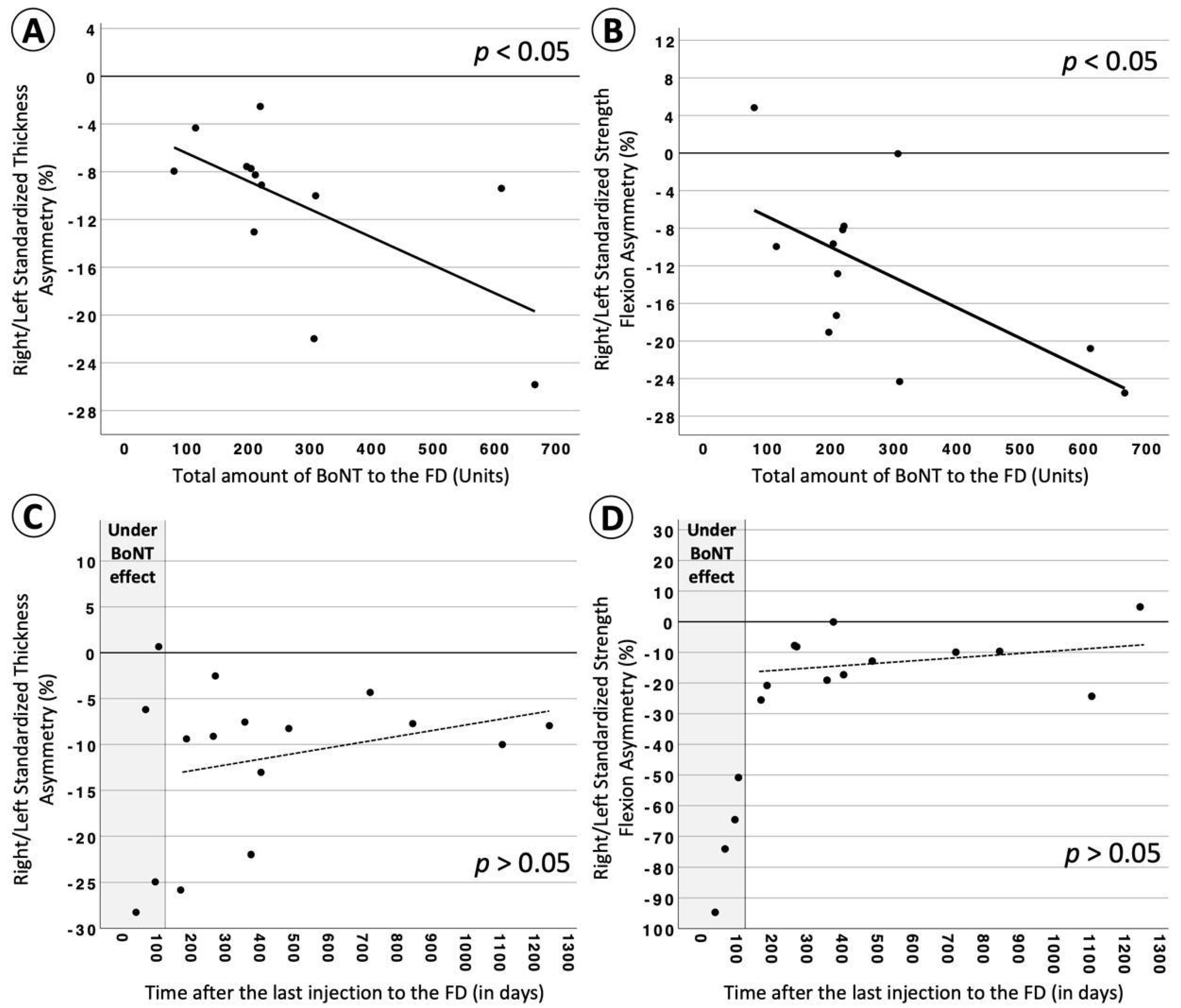
2. Results
3. Discussion
4. Conclusions
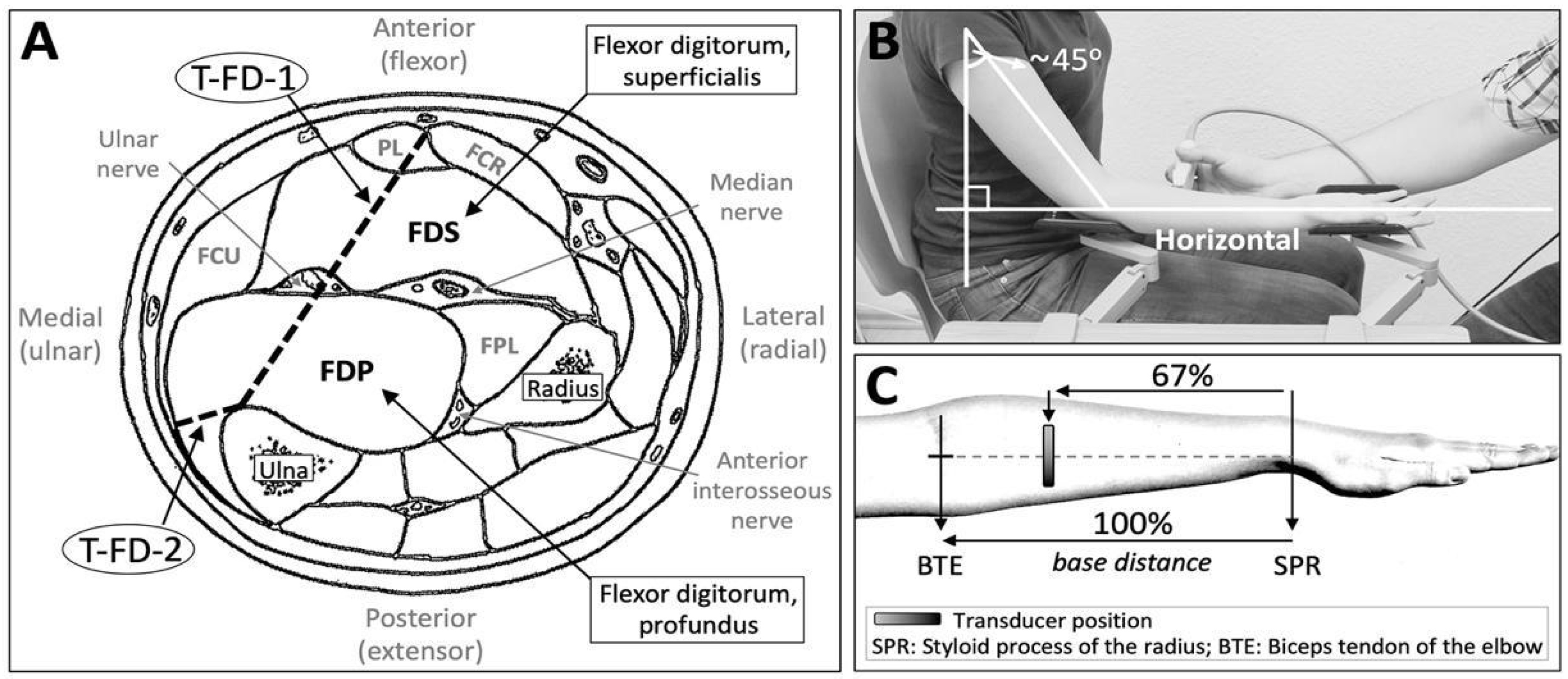
5. Methods
5.1. Participants
5.2. Assessments
5.3. Procedure
5.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Altenmüller, E.; Jabusch, H.C. Focal dystonia in musicians: Phenomenology, pathophysiology and triggering factors. Eur. J. Neurol. 2010, 17, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Torres-Russotto, D.; Perlmutter, J.S. Task-specific Dystonias. Ann. N. Y. Acad. Sci. 2008, 1142, 179–199. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Yoo, S.-Y.; Kim, J.-S. Task-Specific Dystonia in a Professional Billiard Player. J. Mov. Disord. 2022, 15, 86–88. [Google Scholar] [CrossRef]
- Clarke, P.; Sheffield, D.; Akehurst, S. The yips in sport: A systematic review, International Review of Sport and Exercise. Psychology 2015, 8, 156–184. [Google Scholar] [CrossRef]
- Schuele, S.; Jabusch, H.C.; Lederman, R.J.; Altenmüller, E. Botulinum toxin injections in the treatment of musician’s dystonia. Neurology 2005, 64, 341–343. [Google Scholar] [CrossRef]
- Foran, P.G.; Davletov, B.; Meunier, F.A. Getting muscles moving again after botulinum toxin: Novel therapeutic challenges. Trends Mol. Med. 2003, 9, 291–299. [Google Scholar] [CrossRef]
- Stahl, C.M.; Frucht, S.J. Focal task specific dystonia: A review and update. J. Neurol. 2017, 264, 1536–1541. [Google Scholar] [CrossRef]
- Guo, Y.; Pan, L.; Liu, W.; Pan, Y.; Nie, Z.; Jin, L. Polyclonal neural cell adhesion molecule antibody prolongs the effective duration time of botulinum toxin in decreasing muscle strength. Neurol. Sci. 2015, 36, 2019–2025. [Google Scholar] [CrossRef]
- Truong, D.; Hallett, M.; Zachary, C.B.; Dressler, D. Manual of Botulinum Toxin Therapy, 2nd ed.; Cambridge University Press: Cambridge, UK, 2013. [Google Scholar]
- Jochim, A.; Meindl, T.; Mantel, T.; Zwirner, S.; Zech, M.; Castrop, F.; Haslinger, B. Treatment of cervical dystonia with abo- and onabotulinumtoxinA: Long-term safety and efficacy in daily clinical practice. J. Neurol. 2019, 266, 1879–1886. [Google Scholar] [CrossRef]
- Jochim, A.; Meindl, T.; Huber, C.; Mantel, T.; Zwirner, S.; Castrop, F.; Haslinger, B. Treatment of blepharospasm and Meige’s syndrome with abo- and onabotulinumtoxinA: Long-term safety and efficacy in daily clinical practice. J. Neurol. 2020, 267, 267–275. [Google Scholar] [CrossRef]
- Ramirez-Castaneda, J.; Jankovic, J. Long-Term efficacy and safety of botulinum toxin injections in dystonia. Toxins 2013, 5, 249–266. [Google Scholar] [CrossRef] [PubMed]
- Cole, R.; Hallett, M.; Cohen, L.G. Double-Blind Trial of Botulinum Toxin for Treatment of Focal Hand Dystonia. Mov. Disord. 1995, 10, 466–471. [Google Scholar] [CrossRef]
- Compston, A. Aids to the Investigation of Peripheral Nerve Injuries. Medical Research Council: Nerve Injuries Research Committee. His Majesty’s Stationery Office: 1942; pp. 48 (iii) and 74 figures and 7 diagrams; with Aids to the Examination of the Peripheral Nervous System. By Michael O’Brien for the Guarantors of Brain; Saunders Elsevier: 2010; pp. [8] 64 and 94 Figures. Brain 2010, 133, 2838–2844. [Google Scholar] [CrossRef] [PubMed]
- Lungu, C.; Karp, B.I.; Alter, K.; Zolbrod, R.; Hallett, M. Long-Term Follow-up of Botulinum Toxin Therapy for Focal Hand Dystonia: Outcome at 10 Years or More. Mov. Disord. 2011, 26, 750–753. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, A.S.; Ertl-Wagner, B.; Britsch, S. Muscle Biopsy Substantiates Long-Term MRI Alterations One Year After a Single Dose of Botulinum Toxin Injected into the Lateral Gastrocnemius Muscle of Healthy Volunteers. Mov. Disord. 2009, 24, 1494–1503. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Park, Y.W.; Ji, Y.J.; Park, S.W.; Kim, S.G. Effects of a botulinum toxin type A injection on the masseter muscle: An animal model study. Maxillofac. Plast. Reconstr. Surg. 2015, 37, 10. [Google Scholar] [CrossRef]
- Fortuna, R.; Horisberger, M.; Vaz, M.A.; Herzog, W. Do skeletal muscle properties recover following repeat onabotulinum toxin A injections? J. Biomech. 2013, 46, 2426–2433. [Google Scholar] [CrossRef]
- Fortuna, R.; Vaz, M.A.; Youssef, A.R.; Longino, D.; Herzog, W. Changes in contractile properties of muscles receiving repeat injections of botulinum toxin (Botox). J. Biomech. 2011, 44, 39–44. [Google Scholar] [CrossRef]
- Frick, C.G.; Richtsfeld, M.; Sahani, N.D.; Kaneki, M.; Blobner, M.; Martyn, J.A.J. Long-term Effects of Botulinum Toxin on Neuromuscular Function. Anesthesiology 2007, 106, 1139–1146. [Google Scholar] [CrossRef]
- Billante, C.; Zaelear, D.; Billante, M.; Reyes, J.H.; Sant’Anna, G.; Rodriguez, R.; Stone, R.E. Comparison of neuromuscular blockade and recovery with botulinum toxins A and F. Muscle Nerve 2002, 26, 395–403. [Google Scholar] [CrossRef]
- Ma, J.; Elsaidi, G.A.; Smith, T.L.; Walker, F.O.; Tan, K.H.; Martin, E.; Koman, A.L.; Paterson Smith, B.P. Time Course of Recovery of Juvenile Skeletal Muscle After Botulinum Toxin A Injection An Animal Model Study. J. Phys. Med. Rehabil. 2004, 83, 774–780. [Google Scholar] [CrossRef]
- Hammoud, N.; Jankovic, J. Botulinum Toxin in the Treatment of Cervical Dystonia: Evidence-Based Review. Dystonia 2022, 1, 10655. [Google Scholar] [CrossRef]
- Ioannou, C.I.; Hodde-Chriske, F.L.; Avraamides, M.N.; Altenmüller, E. Novel Ultrasonographic Thickness and Strength Assessments of the Flexor Digitorum: A Reliability Analysis. Med. Probl. Perform. Art. 2021, 36, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Salari, M.; Sharma, S.; Jog, M.S. Botulinum toxin induced atrophy: An uncharted territory. Toxins 2018, 10, 313. [Google Scholar] [CrossRef] [PubMed]
- Dressler, D.; Saberi, F.A. Botulinum Toxin: Mechanisms of Action. Eur. Neurol. 2005, 53, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Stone, A.V.; Ma, J.; Whitlock, P.W.; Koman, A.; Smith, T.L.; Smith, B.P.; Callahan, M.F. Effects of Botox1 and Neuronox1 on Muscle Force Generation in Mice. J. Orthop. Res. 2007, 25, 1658–1664. [Google Scholar] [CrossRef]
- Rollnik, J.D.; Matzke, M.; Wohlfarth, K.; Dengler, R.; Bigalke, H. Low-dose treatment of cervical dystonia, blepharospasm and facial hemispasm with albumin-diluted botulinum toxin type A under EMG guidance. Eur. Neurol. 2000, 43, 9–12. [Google Scholar] [CrossRef]
- Oldfield, R.C. The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef]
- Arts, I.M.P.; Overeem, S.; Pillen, S.; Kleine, B.U.; Broekestein, A.; Zwarts, M.J.; Schelhaas, H.J. Muscle ultrasonography: A diagnostic tool for amyotrophic lateral sclerosis. Clin. Neurophysiol. 2012, 123, 1662–1667. [Google Scholar] [CrossRef]
- Harris-Love, M.O.; Seamon, B.A.; Teixeira, C.; Ismail1, C. Ultrasound estimates of muscle quality in older adults: Reliability and comparison of Photoshop and ImageJ for the grayscale analysis of muscle echogenicity. PeerJ 2016, 4, e1721. [Google Scholar] [CrossRef]
- Matak, I.; Riederer, P.; Lacković, Z. Botulinum toxin’s axonal transport from periphery to the spinal cord. Neurochem. Int. 2012, 61, 236–239. [Google Scholar] [CrossRef] [PubMed]
- Hortobágyi, T.; Dempsey, L.; Fraser, D.; Zheng, D.; Hamilton, G.; Lambert, J.; Dohm, L. Changes in muscle strength, muscle fibre size and myofibrillar gene expression after immobilization and retraining in humans. J. Physiol. 2000, 524, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.W.; Chen, H.L.; Chang, Y.C.; Chen, C.M. Molecular Mechanisms of Treadmill Therapy on Neuromuscular Atrophy Induced via Botulinum Toxin A. Neural. Plast. 2013, 2013, 593271. [Google Scholar] [CrossRef] [PubMed]
- Ahtiainen, J.P.; Pakarinen, A.; Alen, M.; Kraemer, W.J.; Häkkinen, K. Muscle hypertrophy, hormonal adaptations and strength development during strength training in strength-trained and untrained men. Eur. J. Appl. Physiol. 2003, 89, 555–563. [Google Scholar] [CrossRef]
- Hubal, M.J.; Gordish-Dressman, H.; Thompson, P.D.; Price, T.B.; Hoffman, E.P.; Angelopoulos, T.J.; Gordon, P.M.; Moyna, N.M.; Pescatello, L.S.; Visich, P.S.; et al. Variability in Muscle Size and Strength Gain after Unilateral Resistance Training. Med. Sci. Sports Exerc. 2005, 37, 964–972. [Google Scholar]
- Enoka, R.M. Muscle strength and its development. New perspectives. Sports Med. 1988, 6, 146–168. [Google Scholar] [CrossRef]
- Folland, J.P.; Williams, A.G. The adaptations to strength training: Morphological and neurological contributions to increased strength. Sports Med. 2007, 37, 145–168. [Google Scholar] [CrossRef]
- Jabusch, H.C.; Zschucke, D.; Schmidt, A.; Schuele, S.; Altenmüller, E. Focal Dystonia in Musicians: Treatment Strategies and Long-Term Outcome in 144 Patients. Mov. Disord. 2005, 20, 1623–1626. [Google Scholar] [CrossRef]
- Brashear, A.; Wooten Watts, M.; Marchetti, A.; Magar, R.; Lau, H.; Wang, L. Duration of Effect of Botulinum Toxin Type A in Adult Patients with Cervical Dystonia: A Retrospective Chart Review. Clin. Ther. 2000, 22, 1516–1524. [Google Scholar] [CrossRef]
- Dressler, D.; Tacik, P.; Saberi, F.A. Botulinum toxin therapy of cervical dystonia: Duration of therapeutic effects. J. Neural Transm. 2015, 122, 297–300. [Google Scholar] [CrossRef]
- Scaglione, F. Conversion Ratio between Botox®, Dysport®, and Xeomin® in Clinical Practice. Toxins 2016, 8, 65. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Thiebaud, R.S.; Loenneke, P.; Ogawa, M.; Mitsukawa, N. Association between Forearm Muscle Thickness and Age-related Loss of Skeletal Muscle Mass, Handgrip and Knee Extension Strength and Walking Performance in Old Men and Women: A Pilot Study. Ultrasound Med. Biol. 2014, 40, 2069–2075. [Google Scholar] [CrossRef] [PubMed]
- Hodde, F.L.; Ioannou, C.I.; Altenmüller, E. Mapping of finger fascicles within the flexor digitorum superficialis and profundus muscles. Muscle Nerve 2019, 60, 579–582. [Google Scholar] [CrossRef] [PubMed]
- Sklerov, M.; Pullman, S.L. Treatment of Musician’s Dystonia with Botulinum Toxin. In Treatment of Dystonia; Dressler, D., Altenmüller, E., Krauss, J.K., Eds.; Cambridge University Press: Cambridge, UK, 2018; pp. 206–209. [Google Scholar]
- Perotto, A.O. Anatomical Guide for the Electromyographer: The Limbs and Trunk, 5th ed.; Charles C Thomas Publisher: Springfield, IL, USA, 2011. [Google Scholar]
- MacDermid, J.C.; Kramer, J.F.; Woodbury, M.G.; McFarlane, R.M.; Roth, J.H. Interrater reliability of pinch and grip strength measurements in patients with cumulative trauma disorders. J. Hand Ther. 1994, 7, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Mathiowetz, V.; Weber, K.; Volland, G.; Kashman, N. Reliability and validity of grip and pinch strength evaluations. J. Hand Surg. 1984, 9, 222–226. [Google Scholar] [CrossRef]
- Błażkiewicz, M.; Wiszomirska, I.; Wit, A. Comparison of four methods of calculating the symmetry of spatial-temporal parameters of gait. Acta Bioeng. Biomech. 2014, 16, 29–35. [Google Scholar] [CrossRef]
- Bangert, M.; Peschel, T.; Schlaug, G.; Rotte, M.; Drescher, D.; Hinrichs, H.; Heinze, H.-J.; Altenmüller, E. Shared networks for auditory and motor processing in professional pianists: Evidence from fmri conjunction. NeuroImage 2006, 30, 917–926. [Google Scholar] [CrossRef]
- Ioannou, C.I.; Hodde-Chriske, F.L.; Altenmüller, E. Flexor digitorum thickness and strength asymmetry between dominant and non-dominant hands: The effect of playing a musical instrument. Hum. Mov. Sci. 2023; under revision. [Google Scholar]
- Schlaug, G. Musicians and Music Making as a Model for the Study of Brain Plasticity. Prog. Brain Res. 2015, 217, 37–55. [Google Scholar] [CrossRef]
- Sarabon, N.; Kozinc, Z.; Bishop, C.; Maffiuletti, N.A. Factors influencing bilateral deficit and inter-limb asymmetry of maximal and explosive strength: Motor task, outcome measure and muscle group. Eur. J. Appl. Physiol. 2020, 120, 1681–1688. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Constant | IVs | ||||||
|---|---|---|---|---|---|---|---|
| Variables | R2 | B | SE B | B | SE B | β | |
| Outcome: Standardized Thickness Asymmetry of FD (%) | |||||||
| Total amount of BoNT (Units) | 0.387 | −4.088 | 3.063 | −0.023 | 0.009 | −0.622 * | |
| Outcome: Standardized Strength Asymmetry of FD (%) | |||||||
| Total amount of BoNT (Units) | 0.391 | −3.507 | 4.198 | −0.032 | 0.013 | −0.625 * | |
| Variables | a. | b. | c. | d. | e. | f. | g. | h. | |
|---|---|---|---|---|---|---|---|---|---|
| a. | Standardized Thickness Asymmetry of FD (%) | ||||||||
| b. | Standardized Strength Asymmetry of FD (%) | 0.343 | |||||||
| c. | Standardized Strength Asymmetry of Ext. Digitorum (%) | 0.308 | 0.422 | ||||||
| d. | Total amount of BoNT to the FD (units) | −0.678 * | −0.483 | −0.294 | |||||
| e. | Total Number of Injections to the FD | −0.449 | −0.502 | −0.651 * | 0.710 * | ||||
| f. | Averaged time between injections to the FD (days) | 0.112 | 0.341 | 0.014 | −0.119 | −0.096 | |||
| g. | Total treatment time from first to last BoNT injection to the FD (days) | −0.399 | −0.28 | −0.696 * | 0.531 | 0.942 ** | 0.111 | ||
| h. | Time after last BoNT injection to the FD (until day of experiment) (days) | 0.266 | 0.322 | 0.326 | −0.622 * | −0.097 | 0.056 | 0.021 | |
| i. | Averaged BoNT dosage per injection to the FD (units) | −0.14 | −0.287 | 0.329 | 0.063 | −0.465 | 0.102 | −0.533 | −0.414 |
| Characteristics | Dystonic Musicians (n = 12) | Healthy Musicians (n = 12) | Dystonic Musicians (under BTX, n = 4) | Healthy Musicians (n = 4) |
|---|---|---|---|---|
| Age in years (M±SD) | 56.5 ± 8 | 57.4 ± 7 | 50 ± 6 | 51.5 ±2.5 |
| Main instrument: piano/guitar/clarinet-oboe (n) | 7/4/1 | 7/4/1 | piano/guitar/trumpet/contrabass | piano/guitar/trumpet/contrabass |
| Handedness 1 (%) | 90 ± 16 | 88 ± 17 | 93 ± 8 | 93 ± 9 |
| Gender: Male / Female (n) | 9 / 3 | 9 / 3 | 4 / 0 | 4 / 0 |
| Dystonic symptoms onset (age, years: M ± SD) | 39 ± 12 | - | 36 ± 6 | |
| Motor skills after diagnosis 2 (out of 100%) | 56 ± 31 | - | 52.5 ± 17 | |
| Motor skills today 2 (out of 100%) | 58 ± 30 | - | 70 ± 21 | |
| Cumulative hours of practicing | 33,413 ± 21,272 | 45,855 ± 26,075 | 41,769 ± 13,188 | 43,481 ± 19,584 |
| Age started playing in years (M ± SD) | 10.4 ± 3.1 | 9.7 ± 4.3 | 13 ± 5 | 9 ± 2 |
| Years of experience (M ± SD) | 46 ± 8 | 48 ± 7 | 37 ± 2 | 43 ± 3 |
| Body Mass Index (kg/m2) | 26.5 ± 3.8 | 29.2 ± 4.6 | 25 ± 4 | 25 ± 2 |
| Total (sum) and averaged (M ± SD) amount of BoNT (units) to the FD | 3357, 280 ± 180 | - | 2571, 642 ± 322 | - |
| Total number of injections to the FD (M ± SD) | 16.5 ± 11 | - | 27 ± 17 | - |
| Total treatment time (days) from first to last BoNT injection to the FD (M ± SD) | 2801 ± 1877 | - | 2588 ± 1532 | - |
| Averaged time between injections to the FD (days, M ± SD) | 173 ± 29 | - | 113 ± 51 | - |
| Time (days) after last BoNT (units) injection to the FD (until day of experiment) (M ± SD) | 531 ± 361 | - | 73 ± 30 | - |
| Average BoNT dosage (units) per injection to the FD (M ± SD) | 20 ± 10 | - | 26 ± 6 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ioannou, C.I.; Hodde-Chriske, F.L.; Altenmüller, E. Long-Term Muscular Atrophy and Weakness Following Cessation of Botulinum Toxin Type A Injections in the Flexor Digitorum Muscle of Musicians with Focal Hand Dystonia. Toxins 2023, 15, 296. https://doi.org/10.3390/toxins15040296
Ioannou CI, Hodde-Chriske FL, Altenmüller E. Long-Term Muscular Atrophy and Weakness Following Cessation of Botulinum Toxin Type A Injections in the Flexor Digitorum Muscle of Musicians with Focal Hand Dystonia. Toxins. 2023; 15(4):296. https://doi.org/10.3390/toxins15040296
Chicago/Turabian StyleIoannou, Christos I., Franziska L. Hodde-Chriske, and Eckart Altenmüller. 2023. "Long-Term Muscular Atrophy and Weakness Following Cessation of Botulinum Toxin Type A Injections in the Flexor Digitorum Muscle of Musicians with Focal Hand Dystonia" Toxins 15, no. 4: 296. https://doi.org/10.3390/toxins15040296