Assessing the Significance of the Circadian Time of Administration on the Effectiveness and Tolerability of OnabotulinumtoxinA for Chronic Migraine Prophylaxis




Abstract
:1. Introduction
2. Results
2.1. Within Group Comparison of Efficacy Headache Outcomes According to BoNTA Time of Administration
2.1.1. AM-Treated Patients (n = 50)
2.1.2. PM-Treated Patients (n = 50)
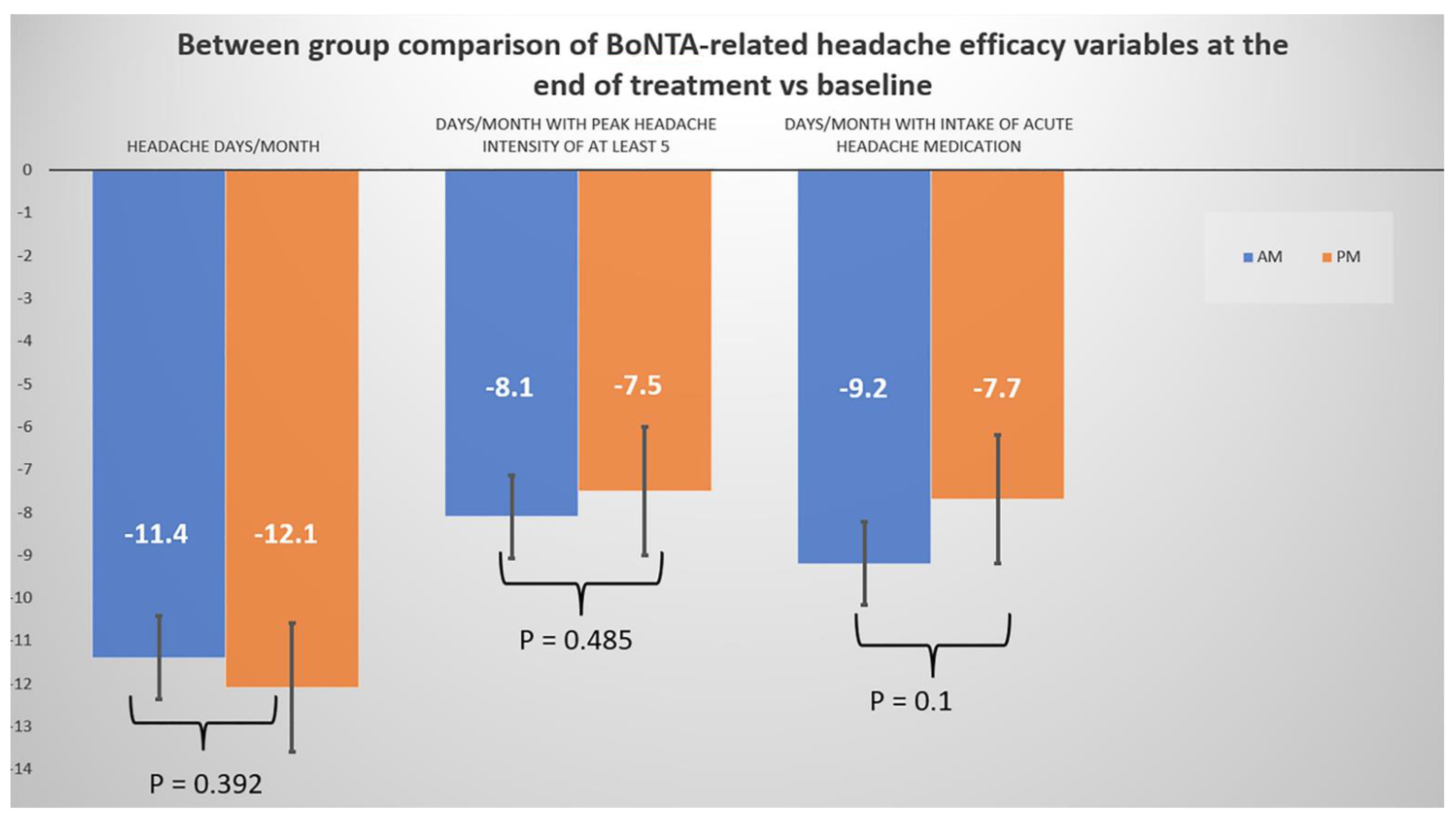
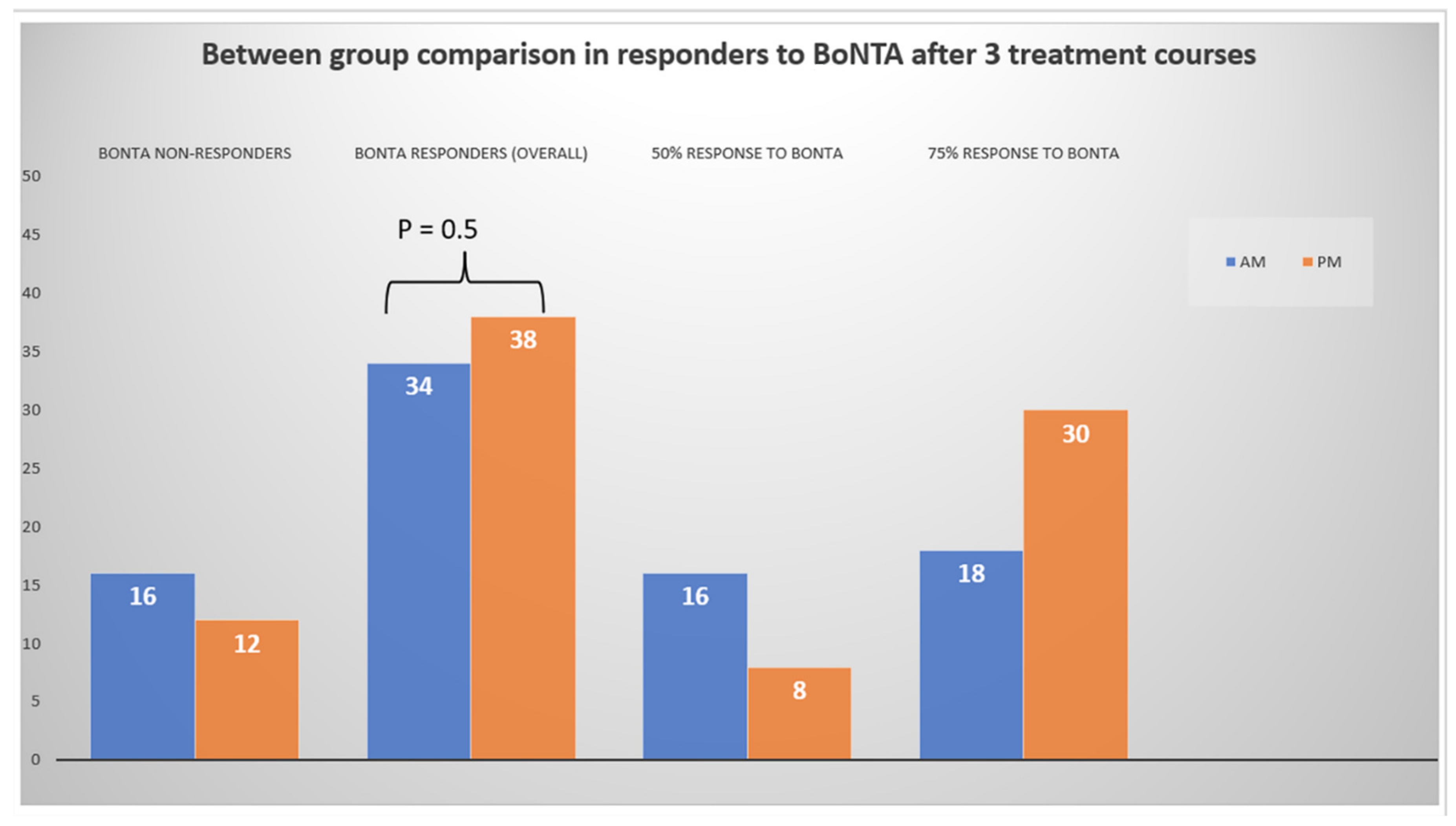
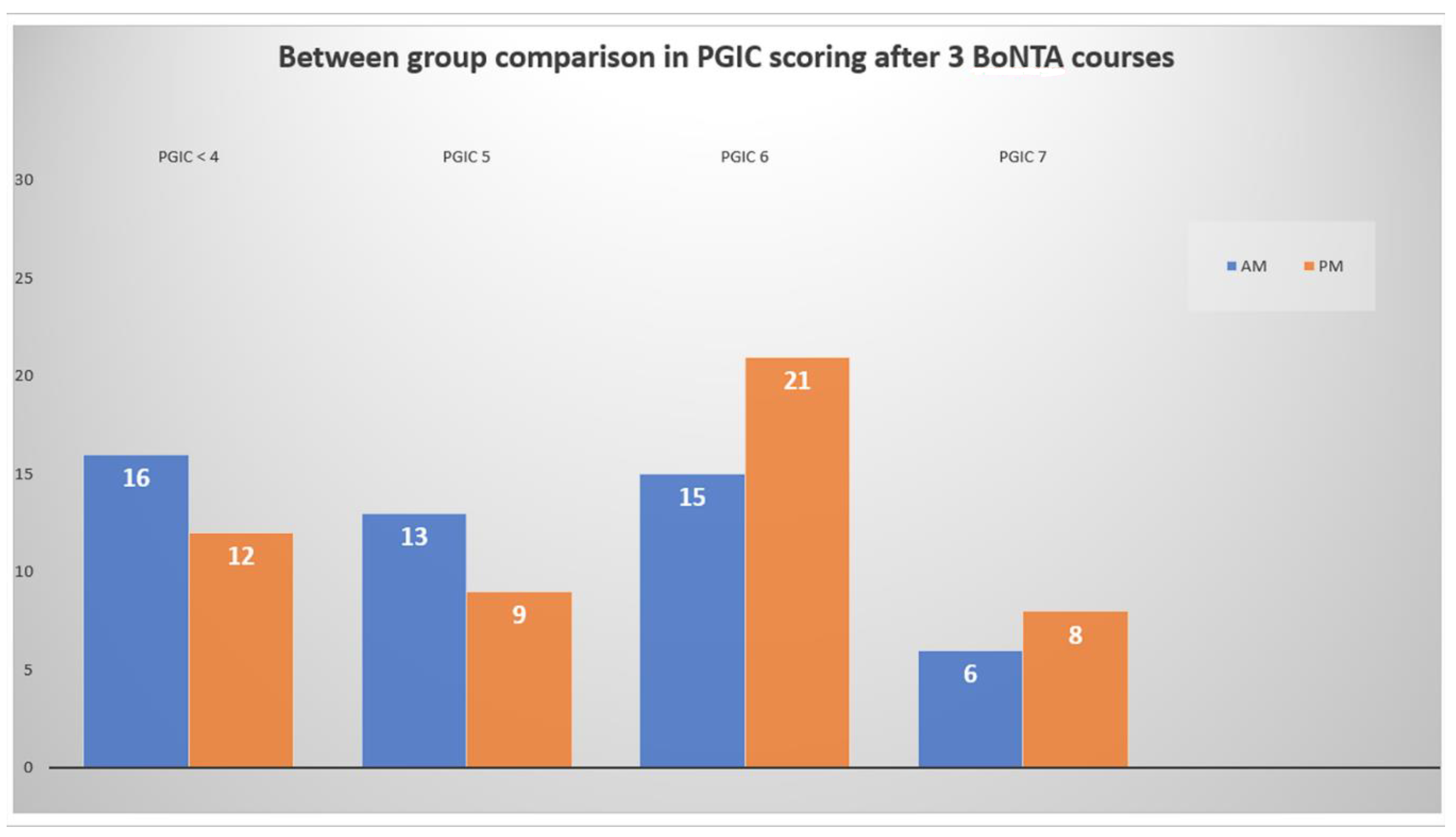
2.2. Between Group Comparison of Efficacy Headache Outcomes According to BoNTA Time of Administration (AM vs. PM)
3. Discussion
4. Conclusions
5. Materials and Methods
Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sumelahti, M.L.; Sumanen, M.; Sumanen, M.S.; Tuominen, S.; Vikkula, J.; Honkala, S.M.; Rosqvist, S.; Korolainen, M.A. My Migraine Voice survey: Disease impact on healthcare resource utilization, personal and working life in Finland. J. Headache Pain 2020, 21, 118. [Google Scholar] [CrossRef] [PubMed]
- Buse, D.C.; Greisman, J.D.; Baigi, K.; Lipton, R.B. Migraine Progression: A Systematic Review. Headache 2019, 59, 306–338. [Google Scholar] [CrossRef] [PubMed]
- Katsarava, Z.; Buse, D.C.; Manack, A.N.; Lipton, R.B. Defining the differences between episodic migraine and chronic migraine. Curr. Pain Headache Rep. 2012, 16, 86–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreou, A.P.; Edvinsson, L. Mechanisms of migraine as a chronic evolutive condition. J. Headache Pain 2019, 20, 117. [Google Scholar] [CrossRef] [PubMed]
- Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Aurora, S.K.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F.; PREEMPT Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Pooled results from the double-blind, randomized, placebo-controlled phases of the PREEMPT clinical program. Headache 2010, 50, 921–936. [Google Scholar] [CrossRef] [PubMed]
- Argyriou, A.A.; Mitsikostas, D.D.; Mantovani, E.; Vikelis, M.; Tamburin, S. Beyond chronic migraine: A systematic review and expert opinion on the off-label use of botulinum neurotoxin type-A in other primary headache disorders. Expert Rev. Neurother. 2021, 21, 923–944. [Google Scholar] [CrossRef]
- Barbanti, P.; Egeo, G.; Fofi, L.; Aurilia, C.; Piroso, S. Rationale for use of onabotulinum toxin A (BOTOX) in chronic migraine. Neurol. Sci. 2015, 36 (Suppl. S1), 9–32. [Google Scholar] [CrossRef]
- Jakubowski, M.; McAllister, P.J.; Bajwa, Z.H.; Ward, T.N.; Smith, P.; Burstein, R. Exploding vs. imploding headache in migraine prophylaxis with Botulinum Toxin A. Pain 2006, 125, 286–295. [Google Scholar] [CrossRef]
- Ravichandran, E.; Gong, Y.; Al Saleem, F.H.; Ancharski, D.M.; Joshi, S.G.; Simpson, L.L. An initial assessment of the systemic pharmacokinetics of botulinum toxin. J. Pharmacol. Exp. Ther. 2006, 318, 1343–1351. [Google Scholar] [CrossRef]
- Pellett, S.; Tepp, W.H.; Whitemarsh, R.C.; Bradshaw, M.; Johnson, E.A. In vivo onset and duration of action varies for botulinum neurotoxin A subtypes 1–5. Toxicon 2015, 107, 37–42. [Google Scholar] [CrossRef] [Green Version]
- Packard, A.; Arciniegas, A.A.; Smotherman, C. Effectiveness of preventive onabotulinumtoxin A injections for migraine headaches is dependent on the circadian time of administration. Chronobiol. Int. 2021, 38, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Packard, A.; Smotherman, C.; Jovanovic, N. Effect of circadian rhythm on the pain associated with preventive onabotulinumtoxinA injections for migraines. Chronobiol. Int. 2020, 37, 1766–1771. [Google Scholar] [CrossRef] [PubMed]
- Vikelis, M.; Argyriou, A.A.; Dermitzakis, E.V.; Spingos, K.C.; Mitsikostas, D.D. Onabotulinumtoxin-A treatment in Greek patients with chronic migraine. J. Headache Pain 2016, 17, 84. [Google Scholar] [CrossRef] [Green Version]
- Vikelis, M.; Argyriou, A.A.; Dermitzakis, E.V.; Spingos, K.C.; Makris, N.; Kararizou, E. Sustained onabotulinumtoxinA therapeutic benefits in patients with chronic migraine over 3 years of treatment. J. Headache Pain 2018, 19, 87. [Google Scholar] [CrossRef] [PubMed]
- Argyriou, A.A.; Dermitzakis, E.V.; Vlachos, G.S.; Vikelis, M. Long-term adherence, safety, and efficacy of repeated onabotulinumtoxinA over five years in chronic migraine prophylaxis. Acta Neurol. Scand. 2022; in press. [Google Scholar] [CrossRef]
- Zaki, N.; Yousif, M.; BaHammam, A.S.; Spence, D.W.; Bharti, V.K.; Subramanian, P.; Pandi-Perumal, S.R. Chronotherapeutics: Recognizing the Importance of Timing Factors in the Treatment of Disease and Sleep Disorders. Clin. Neuropharmacol. 2019, 42, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Ballesta, A.; Innominato, P.F.; Dallmann, R.; Rand, D.A.; Lévi, F.A. Systems Chronotherapeutics. Pharmacol. Rev. 2017, 69, 161–199. [Google Scholar] [CrossRef] [Green Version]
- Dallaspezia, S.; Suzuki, M.; Clara, L.; Colombo, C.; Benedetti, F. Chronotype influences response to antidepressant chronotherapeutics in bipolar patients. Chronobiol. Int. 2018, 35, 1319–1325. [Google Scholar] [CrossRef]
- Ruben, M.D.; Hogenesch, J.B.; Smith, D.F. Sleep and circadian medicine: Time of day in the Neurologic clinic. Neurol. Clin. 2019, 37, 615–629. [Google Scholar] [CrossRef]
- Brückmann, K.F.; Hennig, J.; Müller, M.J.; Fockenberg, S.; Schmidt, A.M.; Cabanel, N.; Kundermann, B. Influence of chronotype on daily mood fluctuations: Pilot study in patients with depression. BJPsych Open 2020, 6, e17. [Google Scholar] [CrossRef]
- Viticchi, G.; Falsetti, L.; Paolucci, M.; Altamura, C.; Buratti, L.; Salvemini, S.; Brunelli, N.; Bartolini, M.; Vernieri, F.; Silvestrini, M. Influence of chronotype on migraine characteristics. Neurol. Sci. 2019, 40, 1841–1848. [Google Scholar] [CrossRef]
- Liampas, I.; Siokas, V.; Brotis, A.; Vikelis, M.; Dardiotis, E. Endogenous melatonin levels and therapeutic use of exogenous melatonin in migraine: Systematic review and meta-analysis. Headache 2020, 60, 1273–1299. [Google Scholar] [CrossRef]
- Segal, J.P.; Tresidder, K.A.; Bhatt, C.; Gilron, I.; Ghasemlou, N. Circadian control of pain and neuroinflammation. J. Neurosci. Res. 2018, 96, 1002–1020. [Google Scholar] [CrossRef]
- Negro, A.; Curto, M.; Lionetto, L.; Martelletti, P. A two years open-label prospective study of OnabotulinumtoxinA 195 U in medication overuse headache: A real-world experience. J. Headache Pain 2015, 17, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurst, H.; Bolton, J. Assessing the clinical significance of change scores recorded on subjective outcome measures. J. Manip. Physiol. Ther. 2004, 27, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; Turk, D.C.; Wyrwich, K.W.; Beaton, D.; Cleeland, C.S.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Kerns, R.D.; Ader, D.N.; et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J. Pain 2008, 9, 105–121. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | AM-Treated Patients | PM-Treated Patients | ||
|---|---|---|---|---|
| Participants | n = 50 | n = 50 | ||
| n = 100 | N | % | N | % |
| Gender | ||||
| Females | 42 | 84 | 47 | 94 |
| Males | 8 | 16 | 3 | 6 |
| Age ± SD (range) | 42.7 ± 10.2 (21–60) | 44.6 ± 9.3 (30–60) | ||
| Number of previously used preventative medications | ||||
| Median value (range) | 3 (1–7) | 3 (1–7) | ||
| Years± SD (range) with chronic migraine | 10.1 ± 3.7 (6–16) | 10.4 ± 3.6 (6–18) | ||
| Psychiatric comorbidities | 35 | 70 | 39 | 78 |
| Anxiety disorder | 13 | 14 | ||
| Depression | 10 | 12 | ||
| Mixed anxiety and depression disorder | 10 | 10 | ||
| Bipolar disorder | 2 | 3 | ||
| Medication overuse headache | ||||
| Yes | 33 | 66 | 36 | 72 |
| No | 17 | 34 | 14 | 28 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dermitzakis, E.V.; Vikelis, M.; Vlachos, G.S.; Argyriou, A.A. Assessing the Significance of the Circadian Time of Administration on the Effectiveness and Tolerability of OnabotulinumtoxinA for Chronic Migraine Prophylaxis. Toxins 2022, 14, 296. https://doi.org/10.3390/toxins14050296
Dermitzakis EV, Vikelis M, Vlachos GS, Argyriou AA. Assessing the Significance of the Circadian Time of Administration on the Effectiveness and Tolerability of OnabotulinumtoxinA for Chronic Migraine Prophylaxis. Toxins. 2022; 14(5):296. https://doi.org/10.3390/toxins14050296
Chicago/Turabian StyleDermitzakis, Emmanouil V., Michail Vikelis, George S. Vlachos, and Andreas A. Argyriou. 2022. "Assessing the Significance of the Circadian Time of Administration on the Effectiveness and Tolerability of OnabotulinumtoxinA for Chronic Migraine Prophylaxis" Toxins 14, no. 5: 296. https://doi.org/10.3390/toxins14050296