Treatment Outcomes of Intravesical Botulinum Toxin A Injections on Patients with Interstitial Cystitis/Bladder Pain Syndrome


Abstract
:1. Introduction
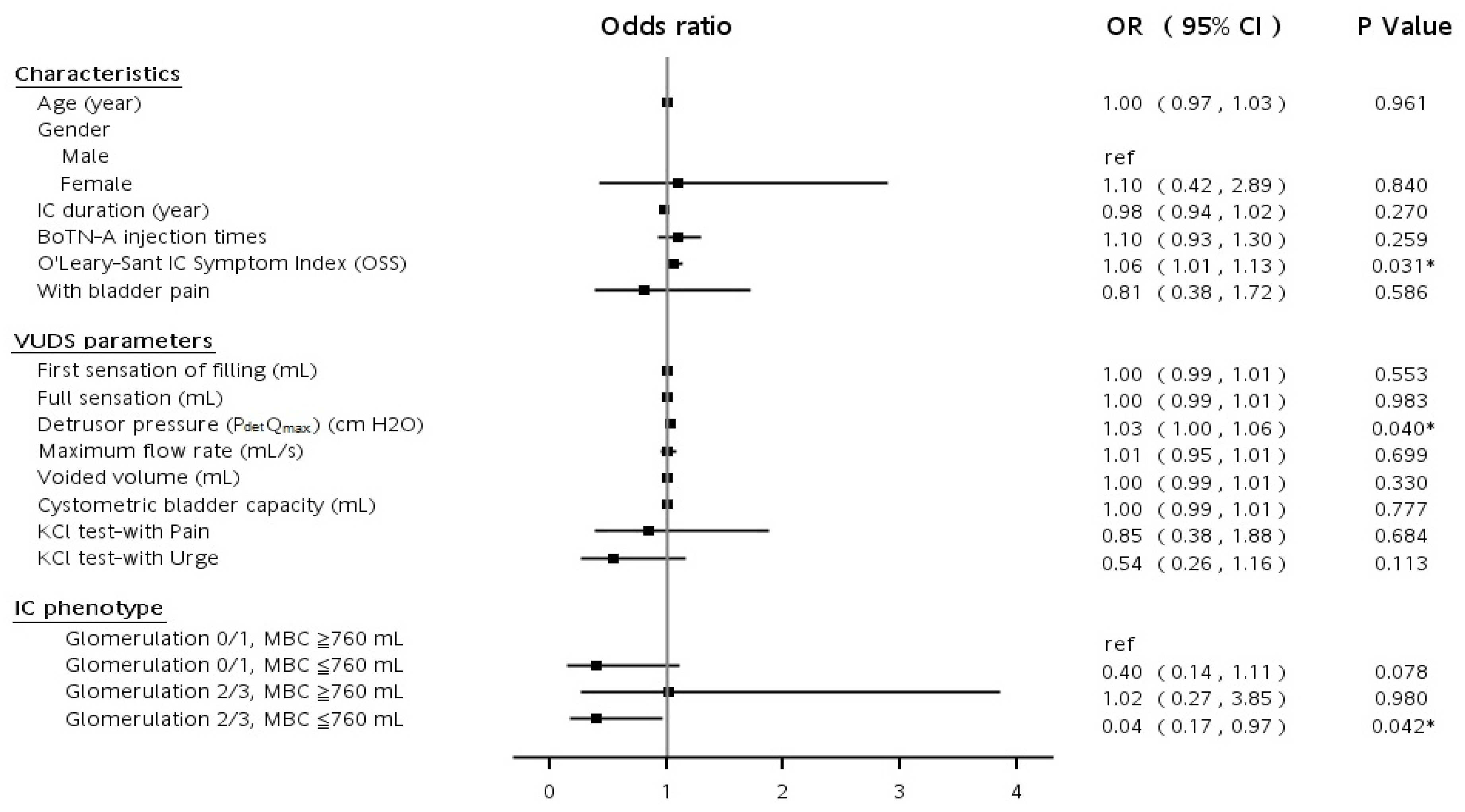
2. Results
3. Discussion
4. Conclusions
5. Materials and Methods
Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. The Inclusion and Exclusion Criteria of Intravesical BoNT-A Injection for IC/BPS
| Patient Inclusion Criteria |
|
| Patient Exclusion Criteria |
|
References
- Homma, Y.; Akiyama, Y.; Tomoe, H.; Furuta, A.; Ueda, T.; Maeda, D.; Lin, A.T.; Kuo, H.C.; Lee, M.H.; Oh, S.J.; et al. Clinical guidelines for interstitial cystitis/bladder pain syndrome. Int. J. Urol. 2020, 27, 578–589. [Google Scholar] [CrossRef] [PubMed]
- Jhang, J.F.; Jiang, Y.H.; Kuo, H.C. Current understanding of the pathophysiology and novel treatments of interstitial cystitis/bladder pain syndrome. Biomedicines 2022, 10, 2380. [Google Scholar] [CrossRef] [PubMed]
- Balsara, Z.R.; Li, X. Sleeping beauty: Awakening urothelium from its slumber. Am. J. Physiol. Ren. Physiol. 2017, 312, F732–F743. [Google Scholar] [CrossRef] [Green Version]
- Clemens, J.Q.; Erickson, D.R.; Varela, N.P.; Lai, H.H. Diagnosis and treatment of interstitial cystitis/bladder pain syndrome. J. Urol. 2022, 208, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Cox, A.; Golda, N.; Nadeau, G.; Nickel, J.C.; Carr, L.; Corcos, J.; Teichman, J. CUA guideline: Diagnosis and treatment of interstitial cystitis/bladder pain syndrome. Can. Urol. Assoc. J. 2016, 10, E136–E155. [Google Scholar] [CrossRef] [PubMed]
- Malde, S.; Palmisani, S.; Al-Kaisy, A.; Sahai, A. Guideline of guidelines: Bladder pain syndrome. BJU Int. 2018, 122, 729–743. [Google Scholar] [CrossRef] [Green Version]
- Hanno, P.M.; Burks, D.A.; Clemens, J.Q.; Dmochowski, R.R.; Erickson, D.; FitzGerald, M.P.; Forrest, J.B.; Gordon, B.; Gray, M.; Mayer, R.D.; et al. AUA guideline for the diagnosis and treatment of interstitial cystitis/bladder pain syndrome. J. Urol. 2011, 185, 2162–2170. [Google Scholar] [CrossRef]
- Jiang, Y.H.; Yu, W.R.; Kuo, H.C. Therapeutic effect of botulinum toxin A on sensory bladder disorders—from bench to bedside. Toxins 2020, 12, 166. [Google Scholar] [CrossRef] [Green Version]
- Kuo, H.C.; Jiang, Y.H.; Tsai, Y.C.; Kuo, Y.C. Intravesical botulinum toxin-A injections reduce bladder pain of interstitial cystitis/bladder pain syndrome refractory to conventional treatment—a prospective, multicenter, randomized, double-blind, placebo-controlled clinical trial. Neurourol. Urodyn. 2016, 35, 609–614. [Google Scholar] [CrossRef]
- Chiu, B.; Tai, H.C.; Chung, S.D.; Birder, L.A. Botulinum toxin A for bladder pain syndrome/interstitial cystitis. Toxins 2016, 8, 201. [Google Scholar] [CrossRef]
- Wang, H.J.; Yu, W.R.; Ong, H.L.; Kuo, H.C. Predictive factors for a satisfactory treatment outcome with intravesical botulinum toxin A injection in patients with interstitial cystitis/bladder pain syndrome. Toxins 2019, 11, 676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keller, J.J.; Chen, Y.K.; Lin, H.C. Comorbidities of bladder pain syndrome/interstitial cystitis: A population-based study. BJU Int. 2012, 110, E903–E909. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.R.; Jiang, Y.H.; Jhang, J.F.; Kuo, H.C. Use of urinary cytokine and chemokine levels for identifying bladder conditions and predicting treatment outcomes in patients with interstitial cystitis/bladder pain syndrome. Biomedicines 2022, 10, 1149. [Google Scholar] [CrossRef] [PubMed]
- Yamany, T.; Van Batavia, J.; Mendelsohn, C. Formation and regeneration of the urothelium. Curr. Opin. Organ Transplant 2014, 19, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Wiessner, G.B.; Plumber, S.A.; Xiang, T.; Mendelsohn, C.L. Development, regeneration and tumorigenesis of the urothelium. Development 2022, 149, dev198184. [Google Scholar] [CrossRef]
- Choudhury, S.; Baker, M.R.; Chatterjee, S.; Kumar, H. Botulinum toxin: An update on pharmacology and newer products in development. Toxins 2021, 13, 58. [Google Scholar] [CrossRef]
- Moore, D.C.; Cohn, J.A.; Dmochowski, R.R. Use of botulinum toxin A in the treatment of lower urinary tract disorders: A review of the literature. Toxins 2016, 8, 88. [Google Scholar] [CrossRef] [Green Version]
- Kuo, H.C. Preliminary results of suburothelial injection of botulinum a toxin in the treatment of chronic interstitial cystitis. Urol. Int. 2005, 75, 170–174. [Google Scholar] [CrossRef]
- Kuo, H.C. Repeated onabotulinumtoxin-a injections provide better results than single injection in treatment of painful bladder syndrome. Pain. Phys. 2013, 16, E15–E23. [Google Scholar] [CrossRef]
- Hanno, P.M.; Erickson, D.; Moldwin, R.; Faraday, M.M. Diagnosis and treatment of interstitial cystitis/bladder pain syndrome: AUA guideline amendment. J. Urol. 2015, 193, 1545–1553. [Google Scholar] [CrossRef]
- Shatkin-Margolis, A.; White, J.; Jedlicka, A.E.; Tam, T.; Hill, A.; Yeung, J.; Crisp, C.C.; Pauls, R.N. The effect of mindfulness-based stress reduction on the urinary microbiome in interstitial cystitis. Int. Urogynecol. J. 2022, 33, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Shie, J.H.; Liu, H.T.; Kuo, H.C. Increased cell apoptosis of urothelium mediated by inflammation in interstitial cystitis/painful bladder syndrome. Urology 2012, 79, 484.e7-13. [Google Scholar] [CrossRef] [PubMed]
- Hanno, P.M.; Landis, J.R.; Matthews-Cook, Y.; Kusek, J.; Nyberg, L. The diagnosis of interstitial cystitis revisited: Lessons learned from the National Institutes of Health Interstitial Cystitis Database study. J. Urol. 1999, 161, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Van de Merwe, J.P.; Nordling, J.; Bouchelouche, P.; Bouchelouche, K.; Cervigni, M.; Daha, L.K.; Elneil, S.; Fall, M.; Hohlbrugger, G.; Irwin, P.; et al. Diagnostic criteria, classification, and nomenclature for painful bladder syndrome/interstitial cystitis: An ESSIC proposal. Eur. Urol. 2008, 53, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Grinberg, K.; Sela, Y.; Nissanholtz-Gannot, R. New insights about chronic pelvic pain syndrome (CPPS). Int. J. Environ. Res. Public Health 2020, 17, 3005. [Google Scholar] [CrossRef]
- Esen, B.; Obaid, K.; Süer, E.; Gökçe, M.İ.; Gökmen, D.; Bedük, Y.; Gülpınar, Ö. Reliability and validity of Turkish versions of the interstitial cystitis symptom index and interstitial cystitis problem index. Neurourol. Urodyn. 2020, 39, 2338–2343. [Google Scholar] [CrossRef]
- O’Leary, M.P.; Sant, G.R.; Fowler, F.J.; Whitmore, K.E.; Spolarich-Kroll, J. The interstitial cystitis symptom index and problem index. Urology 1997, 49, 58–63. [Google Scholar] [CrossRef]
- Abrams, P.; Cardozo, L.; Fall, M.; Griffiths, D.; Rosier, P.; Ulmsten, U.; Van Kerrebroeck, P.; Victor, A.; Wein, A. The standardisation of terminology of lower urinary tract function: Report from the Standardisation Sub-committee of the International Continence Society. Am. J. Obstet. Gynecol. 2002, 187, 116–126. [Google Scholar] [CrossRef] [Green Version]
- Hsiao, S.M.; Lin, H.H.; Kuo, H.C. Videourodynamic studies of women with voiding dysfunction. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Parsons, C.L.; Stein, P.C.; Bidair, M.; Lebow, D. Abnormal sensitivity to intravesical potassium in interstitial cystitis and radiation cystitis. Neurourol. Urodyn. 1994, 13, 515–520. [Google Scholar] [CrossRef]
- Kuo, H.C. Potential urine and serum biomarkers for patients with bladder pain syndrome/interstitial cystitis. Int. J. Urol. 2014, 21, 34–41. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Total (n = 220) | Unsatisfactory Outcome GRA ≤ 1 (n = 133) | Satisfactory Outcome GRA ≥ 2 (n = 87) | p Value | ||
|---|---|---|---|---|---|---|
| Characteristics | ||||||
| Age (years) | 54.1 ± 13.4 | 53.9 ± 14.2 | 55.2 ± 12.3 | 0.499 | ||
| Gender (%) | Men | 40 (18%) | 25 (19%) | 15 (17%) | 0.458 | |
| Women | 180 (82%) | 108 (81%) | 72 (83%) | |||
| IC duration (years) | 13.8 ± 10.1 | 14.5 ± 10.9 | 12.6 ± 8.6 | 0.176 | ||
| Numerical rating pain scale | 5.1 ± 2.7 | 4.9 ± 2.7 | 5.3 ± 2.6 | 0.332 | ||
| IC symptoms index (ICSI) | 12.7 ± 3.7 | 12.5 ± 3.7 | 13.1 ± 3.8 | 0.307 | ||
| IC problem index (ICPI) | 12.0 ± 3.3 | 11.6 ± 3.2 | 12.5 ± 3.4 | 0.052 | ||
| O’Leary-Sant IC Symptom Index (OSS) | 24.7 ± 6.6 | 24.1 ± 6.5 | 25.6 ± 6.8 | 0.118 | ||
| VUDS parameters | ||||||
| First sensation of filling (mL) | 117 ± 52.4 | 116 ± 51.9 | 118 ± 53.4 | 0.751 | ||
| Full sensation (mL) | 182 ± 73.5 | 180 ± 74.7 | 184 ± 71.9 | 0.719 | ||
| Cystometric bladder capacity (mL) | 276 ± 114 | 267 ± 105 | 289 ± 126 | 0.167 | ||
| Detrusor pressure (PdetQmax) (cm H2O) | 20.8 ± 12.8 | 20.8 ± 12.3 | 21.0 ± 13.3 | 0.572 | ||
| Maximum flow rate (mL/s) | 12.3 ± 5.7 | 11.8 ± 5.5 | 13.1 ± 6.0 | 0.572 | ||
| Voided-volume (mL) | 251 ± 121 | 236 ± 111 | 273 ± 130 | 0.026 * | ||
| Post-void residual (mL) | 25.9 ± 51.6 | 28.8 ± 53.6 | 21.5 ± 48.4 | 0.308 | ||
| KCl test—Pain (%) | 167 (77.3%) | 101 (76%) | 66 (76%) | 0.531 | ||
| KCl test—Urge (%) | 68 (31.5%) | 47 (35%) | 21 (24%) | 0.056 | ||
| Maximum bladder capacity (mL) | 652 ± 204 | 635 ± 199 | 680 ± 209 | 0.113 | ||
| Glomerulation grade | Grade 1 | 86 (39.5%) | 48 (36%) | 38 (44%) | 0.173 | |
| Grade 2 | 83 (37.3%) | 55 (41%) | 28 (32%) | |||
| Grade 3 | 31 (14.1%) | 20 (15%) | 11 (13%) | |||
| Hunner’s lesion IC | 20 (9.1%) | 11 (8%) | 9 (10%) | |||
| Variable | Total (n = 220) | Unsatisfactory Outcome GRA ≤ 1 (n = 133) | Satisfactory Outcome GRA ≥ 2 (n = 87) | p Value |
|---|---|---|---|---|
| Bladder condition (%) | ||||
| Maximal bladder capacity < 760 (mL) | 156 (70.9%) | 103 (77%) | 53 (61%) | 0.007 * |
| Glomerulation grade 2/3 | 114 (51.8%) | 75 (56%) | 39 (45%) | 0.062 |
| Hunner’s lesion IC | 20 (9.1%) | 11 (8%) | 9 (10%) | 0.097 |
| Glomerulation 0/1, MBC ≥ 760 mL | 45 (20.5%) | 20 (15%) | 25 (29%) | |
| Glomerulation 0/1, MBC < 760 mL | 38 (17.3%) | 26 (20%) | 12 (14%) | |
| Glomerulation 2/3, MBC ≥ 760 mL | 18 (8.2%) | 10 (8%) | 8 (10%) | |
| Glomerulation 2/3, MBC < 760 mL | 99 (45%) | 66 (47%) | 33 (38%) | |
| Urine biomarker (exclude HIC) | ||||
| IL-8 | 23.7 ± 71.2 | 18.2 ± 24.2 | 31.6 ± 108 | 0.291 |
| CXCL 10 | 16.4 ± 13.2 | 19.7 ± 46.7 | 11.5 ± 37.2 | 0.289 |
| MCP-1 | 318 ± 436 | 379 ± 517 | 229 ± 259 | 0.029 * |
| BDNF | 1.48 ± 9.35 | 2.04 ± 12.1 | 0.64 ± 0.29 | 0.398 |
| Eotaxin | 7.05 ± 7.63 | 7.83 ± 8.04 | 5.92 ± 6.89 | 0.157 |
| IL-6 | 8.54 ± 53.7 | 11.2 ± 67.5 | 4.71 ± 19.0 | 0.496 |
| MIP-1β | 1.70 ± 8.88 | 1.79 ± 2.61 | 1.56 ± 5.23 | 0.728 |
| RANTES | 10.6 ± 61.1 | 15.5 ± 79 | 3.59 ± 5.06 | 0.273 |
| TNF-α | 6.91 ± 35.6 | 8.77 ± 44.6 | 4.19 ± 14.7 | 0.468 |
| PGE2 | 329 ± 346 | 370 ± 382 | 269 ± 278 | 0.100 |
| 8-OHdG | 34.3 ± 26.5 | 36.9 ± 29.6 | 30.5 ± 20.9 | 0.168 |
| 8-Isoprostane | 86.5 ± 194 | 115 ± 245 | 44.8 ± 48.1 | 0.015 * |
| TAC | 1214 ± 1203 | 1323 ± 1288 | 1058 ± 1063 | 0.218 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, W.-R.; Jiang, Y.-H.; Jhang, J.-F.; Chang, W.-C.; Kuo, H.-C. Treatment Outcomes of Intravesical Botulinum Toxin A Injections on Patients with Interstitial Cystitis/Bladder Pain Syndrome. Toxins 2022, 14, 871. https://doi.org/10.3390/toxins14120871
Yu W-R, Jiang Y-H, Jhang J-F, Chang W-C, Kuo H-C. Treatment Outcomes of Intravesical Botulinum Toxin A Injections on Patients with Interstitial Cystitis/Bladder Pain Syndrome. Toxins. 2022; 14(12):871. https://doi.org/10.3390/toxins14120871
Chicago/Turabian StyleYu, Wan-Ru, Yuan-Hong Jiang, Jia-Fong Jhang, Wei-Chuan Chang, and Hann-Chorng Kuo. 2022. "Treatment Outcomes of Intravesical Botulinum Toxin A Injections on Patients with Interstitial Cystitis/Bladder Pain Syndrome" Toxins 14, no. 12: 871. https://doi.org/10.3390/toxins14120871