Hormonal and Thirst Modulated Maintenance of Fluid Balance in Young Women with Different Levels of Habitual Fluid Consumption


 ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Subject Screening and Selection
2.2. Study Design
2.3. Statistical Analysis
3. Results
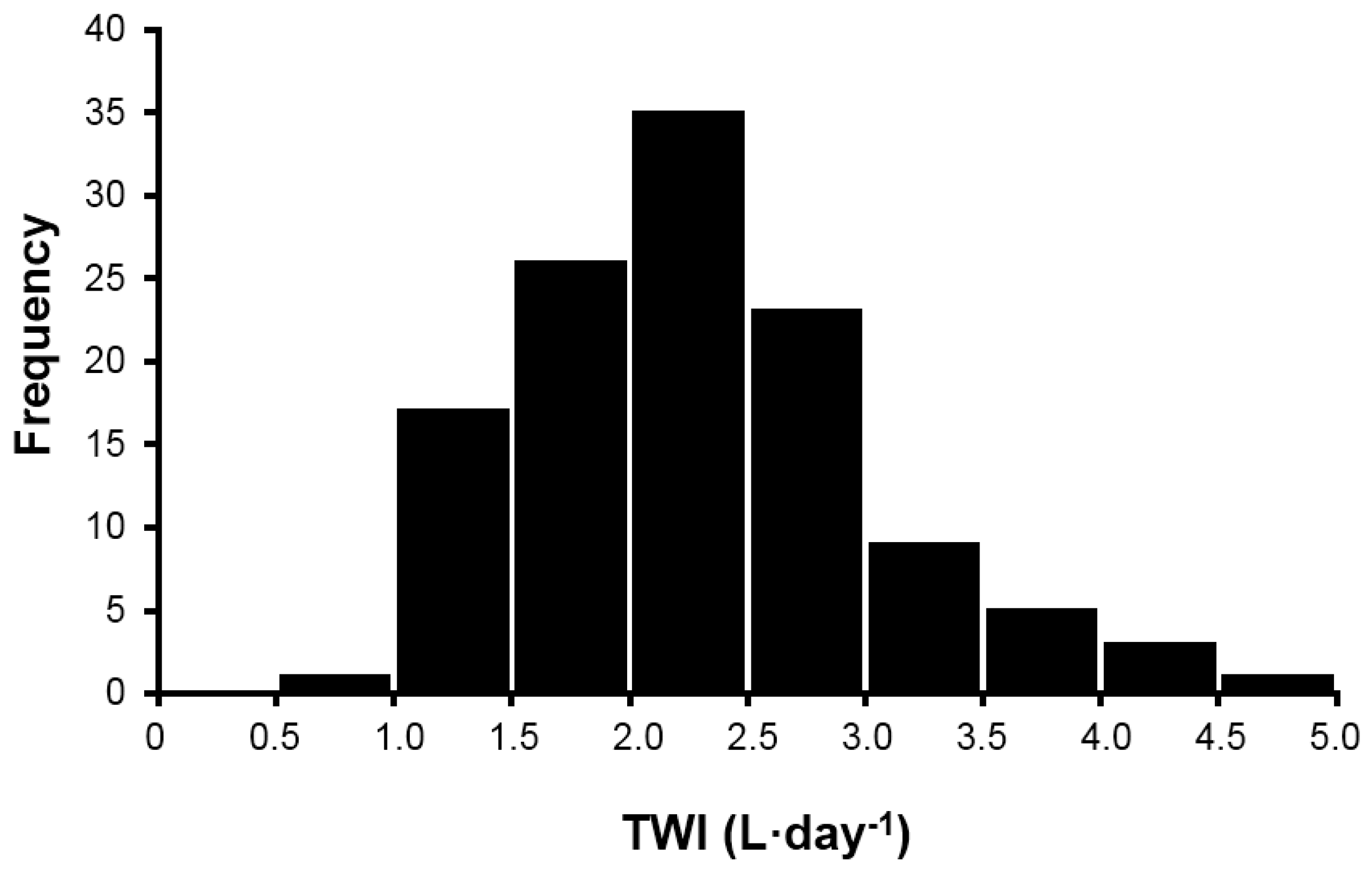
3.1. Full Sample Fluid Intake
3.2. Treatment Fluid Intake
3.3. Hydration Markers
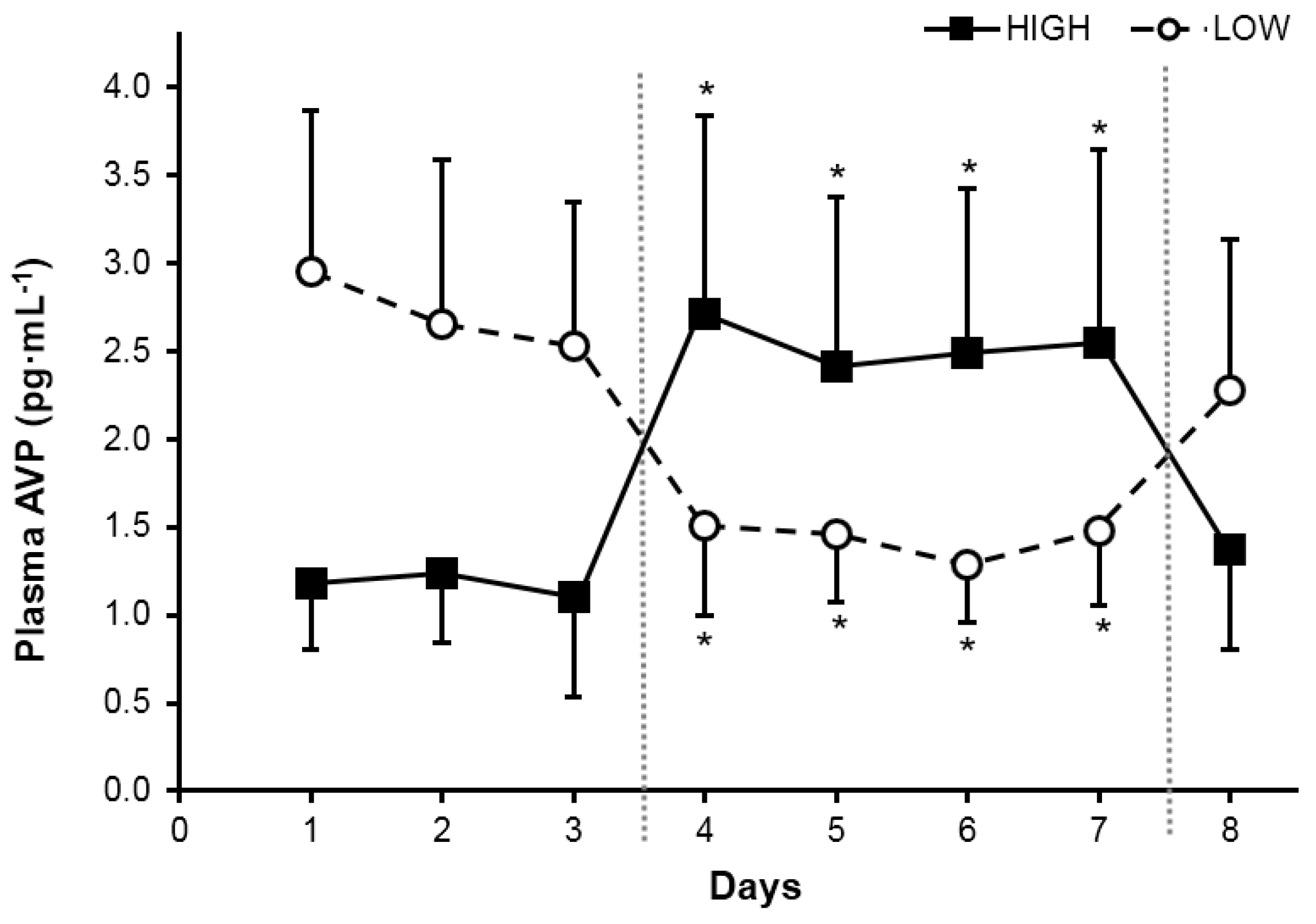
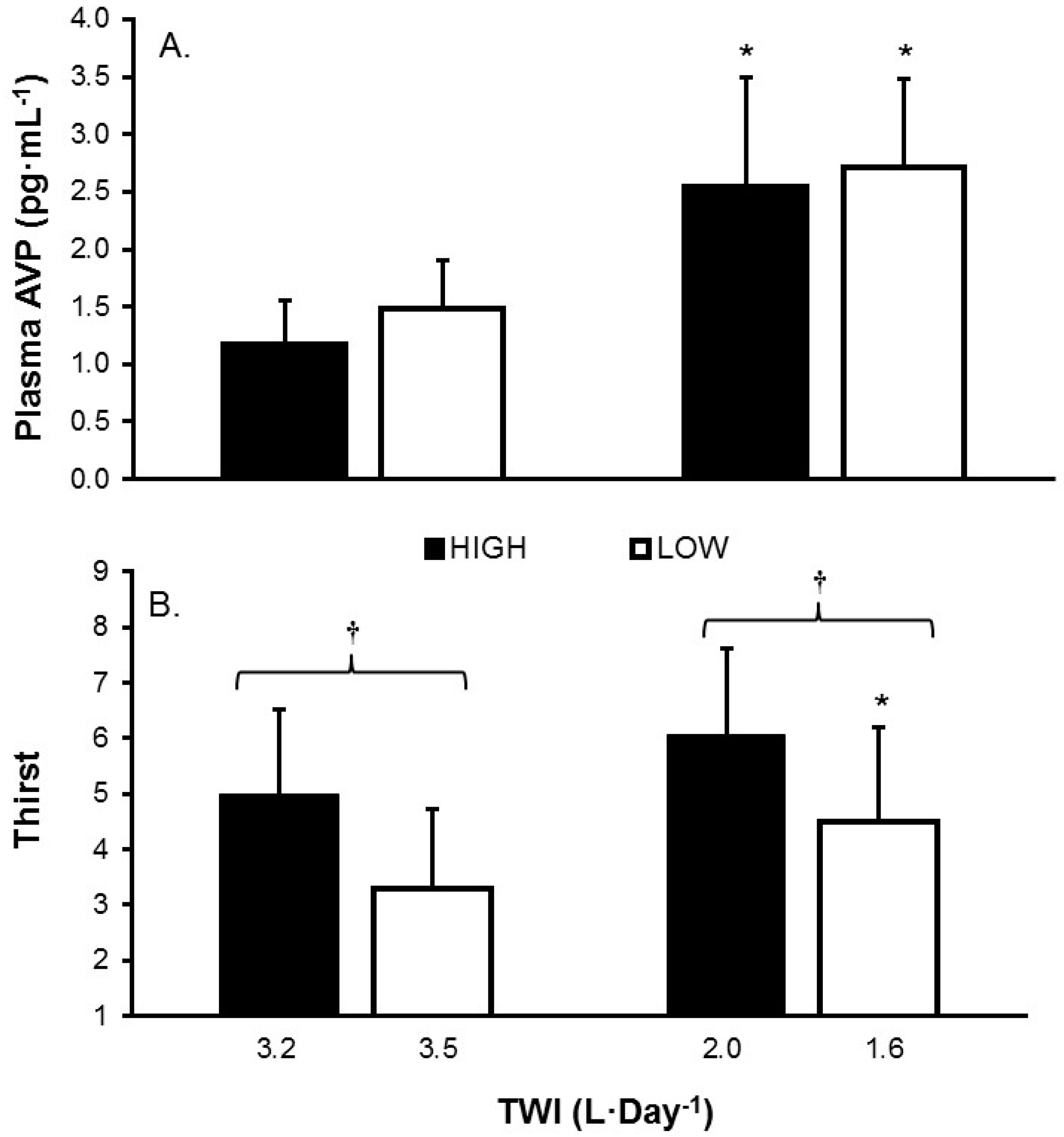
3.4. Hormone Response
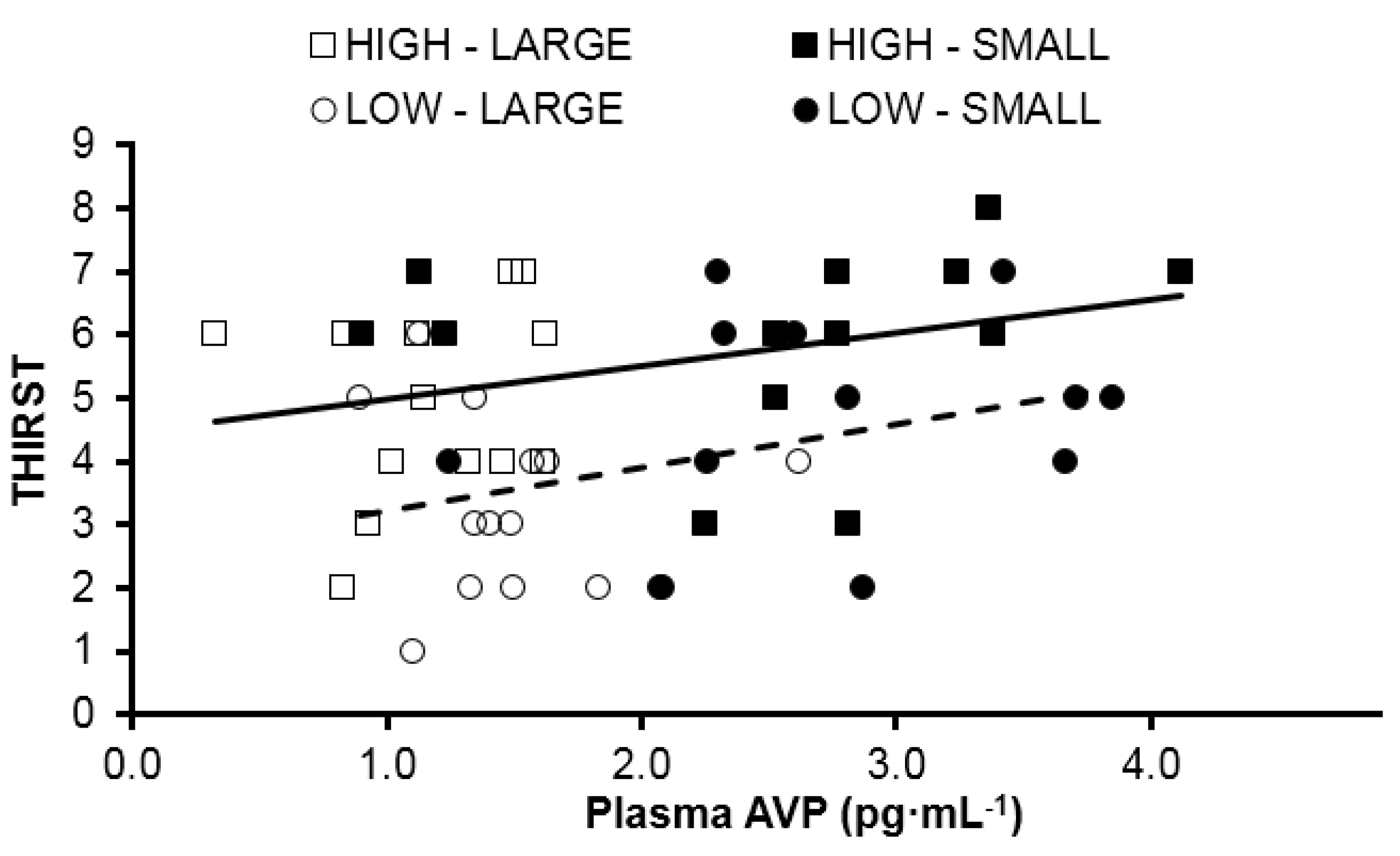
3.5. Perception of Thirst
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- McKinley, M.J.; Johnson, A.K. The Physiological Regulation of Thirst and Fluid Intake. News Physiol. Sci. 2004, 19, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Stricker, E.M.; Sved, A.F. Thirst. Nutrition 2000, 16, 821–826. [Google Scholar] [CrossRef]
- Shore, A.C.; Markandu, N.D.; Sagnella, G.A.; Singer, D.R.; Forsling, M.L.; Buckley, M.G.; Sugden, A.L.; MacGregor, G.A. Endocrine and renal response to water loading and water restriction in normal man. Clin. Sci. 1988, 75, 171–177. [Google Scholar] [CrossRef] [PubMed]
- United States Department of Health and Human Services; Centers for Disease Control and Prevention; National Center for Health Statistics. The Third National Health and Nutrition Examination Survey (NHANES III); Inter-university Consortium for Political and Social Research: Ann Arbor, MI, USA, 1998.
- Food and Nutrition Board, Institute of Medicine. Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate; National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- Perrier, E.; Vergne, S.; Klein, A.; Poupin, M.; Rondeau, P.; Le Bellego, L.; Armstrong, L.E.; Lang, F.; Stookey, J.; Tack, I. Hydration biomarkers in free-living adults with different levels of habitual fluid consumption. Br. J. Nutr. 2013, 109, 1678–1687. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products, Nutrition, and Allergies. Scientific Opinion on Dietary Reference Values for Water. EFSA J. 2010, 8. [Google Scholar]
- Valtin, H. “Drink at least eight glasses of water a day”. Really? Is there scientific evidence for “8 × 8”? Am. J. Physiol. 2002, 283, R993–R1004. [Google Scholar] [CrossRef] [PubMed]
- Noakes, T.D. Waterlogged: The Serious Problem of Overhydration in Endurance Sports; Human Kinetics: Champaign, IL, USA, 2012; p. 448. [Google Scholar]
- Harrison, M.H.; Geelen, G.; Keil, L.C.; Wade, C.A.; Hill, L.C.; Kravik, S.E.; Greenleaf, J.E. Effect of hydration on plasma vasopressin, renin, and aldosterone responses to head-up tilt. Aviat. Space Environ. Med. 1986, 57, 420–425. [Google Scholar] [PubMed]
- Ramsay, D.J.; Rolls, B.J.; Wood, R.J. Body fluid changes which influence drinking in the water deprived rat. J. Physiol. 1977, 266, 453–469. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, D.J.; Rolls, B.J.; Wood, R.J. Thirst following water deprivation in dogs. Am. J. Physiol. 1977, 232, R93–R100. [Google Scholar] [PubMed]
- Czaczkes, J.W.; Kleeman, C.R. The Effect of various States of Hydration and the Plasma Concentration on the Turnover of Antidiuretic Hormone in Mammals. J. Clin. Investig. 1964, 43, 1649–1658. [Google Scholar] [CrossRef] [PubMed]
- Verbalis, J.G. Whole-body volume regulation and escape from antidiuresis. Am. J. Med. 2006, 119, S21–S29. [Google Scholar] [CrossRef] [PubMed]
- Pross, N.; Demazieres, A.; Girard, N.; Barnouin, R.; Metzger, D.; Klein, A.; Perrier, E.; Guelinckx, I. Effects of changes in water intake on mood of high and low drinkers. PLoS ONE 2014, 9, e94754. [Google Scholar] [CrossRef] [PubMed]
- Munoz, C.X.; Johnson, E.C.; McKenzie, A.L.; Guelinckx, I.; Graverholt, G.; Casa, D.J.; Maresh, C.M.; Armstrong, L.E. Habitual total water intake and dimensions of mood in healthy young women. Appetite 2015, 92, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Benton, D.; Burgess, N. The effect of the consumption of water on the memory and attention of children. Appetite 2009, 53, 143–146. [Google Scholar] [CrossRef] [PubMed]
- Benton, D. Dehydration influences mood and cognition: A plausible hypothesis? Nutrients 2011, 3, 555–573. [Google Scholar] [CrossRef] [PubMed]
- Roussel, R.; Fezeu, L.; Bouby, N.; Balkau, B.; Lantieri, O.; Alhenc-Gelas, F.; Marre, M.; Bankir, L.; D.E.S.I.R. Study Group. Low water intake and risk for new-onset hyperglycemia. Diabetes Care 2011, 34, 2551–2554. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Malik, V.S.; Schulze, M.B.; Manson, J.E.; Willett, W.C.; Hu, F.B. Plain-water intake and risk of type 2 diabetes in young and middle-aged women. Am. J. Clin. Nutr. 2012, 95, 1454–1460. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, L.E. Challenges of linking chronic dehydration and fluid consumption to health outcomes. Nutr. Rev. 2012, 70, S121–S127. [Google Scholar] [CrossRef] [PubMed]
- Negoianu, D.; Goldfarb, S. Just add water. J. Am. Soc. Nephrol. 2008, 19, 1041–1043. [Google Scholar] [CrossRef] [PubMed]
- Lette, F.; Dwyer, J.P. The fluid craze. Lancet 2008, 372, 782–784. [Google Scholar] [CrossRef]
- Perrier, E.; Demazieres, A.; Girard, N.; Pross, N.; Osbild, D.; Metzger, D.; Guelinckx, I.; Klein, A. Circadian variation and responsiveness of hydration biomarkers to changes in daily water intake. Eur. J. Appl. Physiol. 2013, 113, 2143–2151. [Google Scholar] [CrossRef] [PubMed]
- Johnson, E.C.; Munoz, C.X.; Le Bellego, L.; Klein, A.; Casa, D.J.; Maresh, C.M.; Armstrong, L.E. Markers of the hydration process during fluid volume modification in women with habitual high or low daily fluid intakes. Eur. J. Appl. Physiol. 2015, 115, 1057–1074. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, L.E.; Johnson, E.C.; Munoz, C.X.; Swokla, B.; Le Bellego, L.; Jimenez, L.; Casa, D.J.; Maresh, C.M. Hydration biomarkers and dietary fluid consumption of women. J. Acad. Nutr. Diet. 2012, 112, 1056–1061. [Google Scholar] [CrossRef] [PubMed]
- Johnson, E.C.; Munoz, C.X.; Le Bellego, L.; Klein, A.; Jimenez, L.; Casa, D.J.; Maresh, C.M.; Armstrong, L.E. Effects of swithching small and high drinker on physiological markers in free-living conditions. Hydration Health Sci. Conf. 2012, 112, 1056–1061. [Google Scholar]
- Engell, D.B.; Maller, O.; Sawka, M.N.; Francesconi, R.N.; Drolet, L.; Young, A.J. Thirst and fluid intake following graded hypohydration levels in humans. Physiol. Behav. 1987, 40, 229–236. [Google Scholar] [CrossRef]
- Kant, A.K.; Graubard, B.I. Contributors of water intake in US children and adolescents: Associations with dietary and meal characteristics—National Health and Nutrition Examination Survey 2005–2006. Am. J. Clin. Nutr. 2010, 92, 887–896. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, R.S.; Bentzen, H.; Bech, J.N.; Pedersen, E.B. Effect of water deprivation and hypertonic saline infusion on urinary AQP2 excretion in healthy humans. Am. J. Physiol. Renal. Physiol. 2001, 280, F860–F867. [Google Scholar] [PubMed]
- Armitage, P. Statistical Methods in Medical Research, 5th ed.; Blackwell Science Ltd.: Oxford, UK, 1980. [Google Scholar]
- Perrier, E.; Rondeau, P.; Poupin, M.; Le Bellego, L.; Armstrong, L.E.; Lang, F.; Stookey, J.; Tack, I.; Vergne, S.; Klein, A. Relation between urinary hydration biomarkers and total fluid intake in healthy adults. Eur. J. Clin. Nutr. 2013, 67, 939–943. [Google Scholar] [CrossRef] [PubMed]
- Ward, D.T.; Hammond, T.G.; Harris, H.W. Modulation of vasopressin-elicited water transport by trafficking of aquaporin2-containing vesicles. Annu. Rev. Physiol. 1999, 61, 683–697. [Google Scholar] [CrossRef] [PubMed]
- Manz, F.; Wentz, A. 24-h hydration status: Parameters, epidemiology and recommendations. Eur. J. Clin. Nutr. 2003, 57, S10–S18. [Google Scholar] [CrossRef] [PubMed]
- Robertson, G.L. Thirst and vasopressin function in normal and disordered states of water balance. J. Lab. Clin. Med. 1983, 101, 351–371. [Google Scholar] [PubMed]
- Verbalis, J.G. How Does the Brain Sense Osmolality? J. Am. Soc. Nephrol. 2007, 18, 3056–3059. [Google Scholar] [CrossRef] [PubMed]
- Obika, L.F.; Ozoene, J.O. Estimation of Plasma Arginine Vasopressin Concentration Using Thirst Perception and Plasma Osmolality Values. Niger. J. Physiol. Sci. 2014, 29, 119–124. [Google Scholar] [PubMed]
- Swanson, L.W.; Mogenson, G.J. Neural mechanisms for the functional coupling of autonomic, endocrine and somatomotor responses in adaptive behavior. Brain Res. Rev. 1981, 228, 1–34. [Google Scholar] [CrossRef]
- Iwasaki, Y.; Gaskill, M.B.; Robertson, G.L. Adaptive resetting of the volume control of vasopressin secretion during sustained hypovolemia. Am. J. Physiol. 1995, 268, R349–R357. [Google Scholar] [PubMed]
- Robertson, G.L.; Shelton, R.L.; Athar, S. The osmoregulation of vasopressin. Kidney Int. 1976, 10, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Robertson, G.L. Abnormalities of thirst regulation. Kidney Int. 1984, 25, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Dunn, F.L.; Brennan, T.J.; Nelson, A.E.; Robertson, G.L. The role of blood osmolality and volume in regulating vasopressin secretion in the rat. J. Clin. Investig. 1973, 52, 3212–3219. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline: 2 Days Ad Libitum (Days 1–2, 2–3) a | Treatment: 4 Days Modified TWI (Days 3–4, 4–5, 5–6, 6–7) a | Recovery: 1 Day Ad Libitum (Days 7–8) b | |
|---|---|---|---|
| HIGH (n = 14) | 3.2 ± 0.6 *,† | 2.0 ± 0.2 *,† | 3.2 ± 0.9 |
| LOW (n = 14) | 1.6 ± 0.4 *,† | 3.5 ± 0.1 *,† | 1.7 ± 0.5 |
| Variable | Group | Total Water Intake | |
|---|---|---|---|
| 3.2–3.5 L·Day−1 | 1.6–2.0 L·Day−1 | ||
| 24 h Urine Volume (L·day−1) *,† | HIGH | 1.9 ± 0.6 | 1.2 ± 0.2 ‡,§ |
| LOW | 2.2 ± 0.4 | 0.8 ± 0.3 ‡,§ | |
| Urine Osmolality (mOsm·kg−1) *,† | HIGH | 392 ± 129 § | 592 ± 222 ‡,§ |
| LOW | 274 ± 60 § | 766 ± 210 ‡,§ | |
| Serum Osmolality (mOsm·kg−1) | HIGH | 293 ± 3 | 294 ± 2 |
| LOW | 293 ± 2 | 295 ± 4 | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johnson, E.C.; Muñoz, C.X.; Jimenez, L.; Le Bellego, L.; Kupchak, B.R.; Kraemer, W.J.; Casa, D.J.; Maresh, C.M.; Armstrong, L.E. Hormonal and Thirst Modulated Maintenance of Fluid Balance in Young Women with Different Levels of Habitual Fluid Consumption. Nutrients 2016, 8, 302. https://doi.org/10.3390/nu8050302
Johnson EC, Muñoz CX, Jimenez L, Le Bellego L, Kupchak BR, Kraemer WJ, Casa DJ, Maresh CM, Armstrong LE. Hormonal and Thirst Modulated Maintenance of Fluid Balance in Young Women with Different Levels of Habitual Fluid Consumption. Nutrients. 2016; 8(5):302. https://doi.org/10.3390/nu8050302
Chicago/Turabian StyleJohnson, Evan C., Colleen X. Muñoz, Liliana Jimenez, Laurent Le Bellego, Brian R. Kupchak, William J. Kraemer, Douglas J. Casa, Carl M. Maresh, and Lawrence E. Armstrong. 2016. "Hormonal and Thirst Modulated Maintenance of Fluid Balance in Young Women with Different Levels of Habitual Fluid Consumption" Nutrients 8, no. 5: 302. https://doi.org/10.3390/nu8050302