
Implementation of National Nutrition Policies and Strategies to Reduce Unhealthy Diets: An Ecological Analysis of 194 Countries from 2017 to 2021

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data and Measurement
2.3. Statistical Analysis
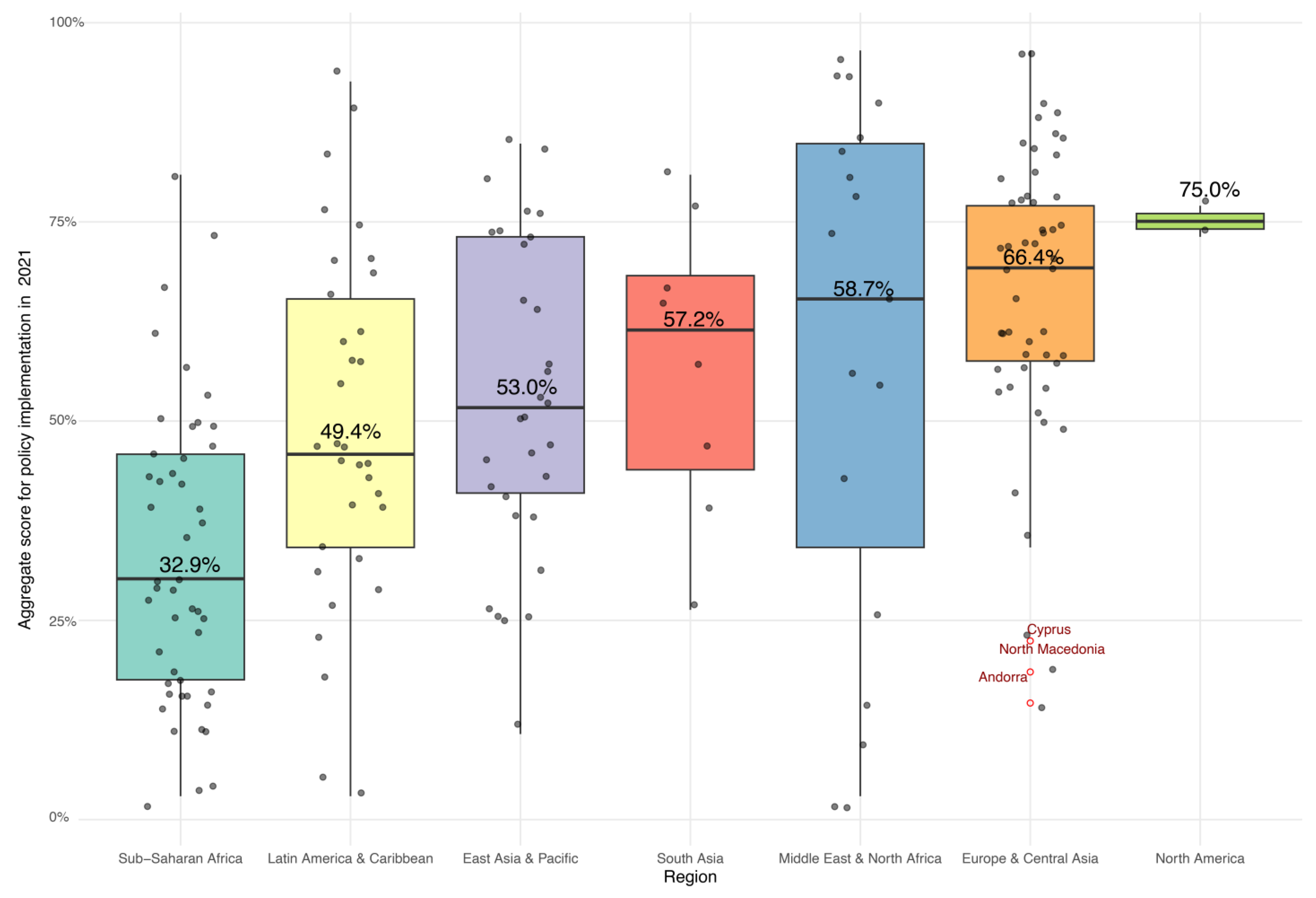
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- World Health Organization. Fact Sheet: Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 16 March 2024).
- Ronto, R.; Wu, J.H.; Singh, G.M. The global nutrition transition: Trends, disease burdens and policy interventions. Public Health Nutr. 2018, 21, 2267–2270. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Development of an Implementation Roadmap 2023–2030 for the Global Action Plan for the Prevention and Control of NCDs 2013–2030. Available online: https://www.who.int/publications/m/item/implementation-roadmap-2023-2030-for-the-who-global-action-plan-for-the-prevention-and-control-of-ncds-2023-2030 (accessed on 3 March 2024).
- Reeve, E.; Thow, A.M.; Huse, O.; Bell, C.; Peeters, A.; Sacks, G. Policy-makers’ perspectives on implementation of cross-sectoral nutrition policies, Western Pacific Region. Bull. World Health Organ. 2021, 99, 865–873. [Google Scholar] [CrossRef] [PubMed]
- Buse, K.; Aftab, W.; Akhter, S.; Phuong, L.B.; Chemli, H.; Dahal, M.; Feroz, A.; Hofiani, S.; Pradhan, N.A.; Anwar, I.; et al. The state of diet-related NCD policies in Afghanistan, Bangladesh, Nepal, Pakistan, Tunisia and Vietnam: A comparative assessment that introduces a ‘policy cube’ approach. Health Policy Plan. 2020, 35, 503–521. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.J.; Cullerton, K.; Herron, L.M. Achieving Food System Transformation: Insights From A Retrospective Review of Nutrition Policy (In)Action in High-Income Countries. Int. J. Health Policy Manag. 2021, 10, 766–783. [Google Scholar] [CrossRef] [PubMed]
- Peeters, A. Obesity and the future of food policies that promote healthy diets. Nat. Rev. Endocrinol. 2018, 14, 430–437. [Google Scholar] [CrossRef]
- European Observatory on Health Systems and Policies. Our Food, Our Health, Our Earth: A Sustainable Future for Humanity (EuroHealth). Available online: https://eurohealthobservatory.who.int/publications/i/our-food-our-health-our-earth-a-sustainable-future-for-humanity-(eurohealth) (accessed on 16 March 2024).
- World Health Organization (WHO). Assessing National Capacity for the Prevention and Control of Noncommunicable Diseases: Report of the 2017 Global Survey. Available online: https://www.who.int/publications/i/item/9789241514781 (accessed on 1 March 2024).
- World Health Organization (WHO). Assessing National Capacity for the Prevention and Control of Noncommunicable Diseases: Report of the 2021 Global Survey. Available online: https://www.who.int/publications/i/item/9789240071698 (accessed on 1 March 2024).
- World Health Organization (WHO). Assessing National Capacity for the Prevention and Control of Noncommunicable Diseases: Report of the 2019 Global Survey. Available online: https://www.who.int/publications/i/item/9789240002319 (accessed on 1 March 2024).
- World Health Organization (WHO). Noncommunicable Diseases Progress Monitor 2020. Available online: https://www.who.int/publications/i/item/9789240000490 (accessed on 1 March 2024).
- World Health Organization (WHO). Noncommunicable Diseases Progress Monitor 2022. Available online: https://www.who.int/publications/i/item/9789240047761 (accessed on 1 March 2024).
- World Health Organization (WHO). Noncommunicable Diseases Progress Monitor 2017. Available online: https://www.who.int/publications/i/item/9789241513029 (accessed on 1 March 2024).
- WHO. On the Road to 2025: The Global NCD Deadline. Available online: https://www.who.int/teams/noncommunicable-diseases/on-the-road-to-2025 (accessed on 3 March 2024).
- World Health Organization (WHO). The Global Health Observatory—Noncommunicable Diseases: National Capacity. Available online: https://www.who.int/data/gho/data/themes/topics/noncommunicable-diseases-national-capacity (accessed on 3 March 2024).
- Allen, L.N.; Nicholson, B.D.; Yeung, B.Y.T.; Goiana-da-Silva, F. Implementation of non-communicable disease policies: A geopolitical analysis of 151 countries. Lancet Glob. Health 2020, 8, e50–e58. [Google Scholar] [CrossRef]
- Allen, L.N.; Wigley, S.; Holmer, H. Implementation of non-communicable disease policies from 2015 to 2020: A geopolitical analysis of 194 countries. Lancet Glob. Health 2021, 9, e1528–e1538. [Google Scholar] [CrossRef]
- World Bank. World Development Indicators (WDI)—Literacy Rate, Adult Total (% of People Ages 15 and Above). Available online: https://data.worldbank.org/indicator/SE.ADT.LITR.ZS (accessed on 1 March 2024).
- United Nations Development Programme (UNDP). Human Development Index (HDI). Available online: https://hdr.undp.org/data-center/human-development-index#/indicies/HDI (accessed on 1 March 2024).
- World Bank. GDP per Capita (Current US$). Available online: https://data.worldbank.org/indicator/NY.GDP.PCAP.CD (accessed on 1 March 2024).
- The Heritage Foundation. 2023 Index of Economic Freedom. Available online: https://indexdotnet.azurewebsites.net/index/explore (accessed on 1 March 2024).
- World Bank. Current Health Expenditure per Capita (current US$). Available online: https://data.worldbank.org/indicator/SH.XPD.CHEX.PC.CD (accessed on 1 March 2024).
- World Health Organization (WHO). Coverage of Essential Health Services. Available online: https://www.who.int/data/gho/data/themes/topics/service-coverage (accessed on 1 March 2024).
- World Bank. Mortality from CVD, Cancer, Diabetes or CRD between Exact Ages 30 and 70 (%). Available online: https://data.worldbank.org/indicator/SH.DYN.NCOM.ZS?end=2019&start=2018 (accessed on 1 March 2024).
- World Bank. Population Ages 65 and above (% of Total Population). Available online: https://data.worldbank.org/indicator/SP.POP.65UP.TO.ZS (accessed on 1 March 2024).
- World Health Organization (WHO). Total NCD Mortality Rate (per 100 000 Population), Age-Standardized. Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/gho-ghe-ncd-mortality-rate (accessed on 1 March 2024).
- Food and Agriculture Organization of the United Nations (FAO). Cost and Affordability of a Healthy Diet (CoAHD). Available online: https://www.fao.org/faostat/en/#data/CAHD (accessed on 1 March 2024).
- World Health Organization (WHO). Prevalence of Obesity among Adults, BMI >= 30 (Age-Standardized Estimate) (%). Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/prevalence-of-obesity-among-adults-bmi-=-30-(age-standardized-estimate)-(-) (accessed on 1 March 2024).
- World Health Organization (WHO). Prevalence of Hypertension among Adults Aged 30–79 Years. Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/prevalence-of-hypertension-among-adults-aged-30-79-years (accessed on 1 March 2024).
- World Bank. Total Alcohol Consumption per Capita (Liters of Pure Alcohol, Projected Estimates, 15+ Years of Age). Available online: https://data.worldbank.org/indicator/SH.ALC.PCAP.LI (accessed on 1 March 2024).
- Global Dietary Database (GDD). GDD 2018 Estimates Dietary Intake for the Global Population. Available online: https://www.globaldietarydatabase.org/data-download (accessed on 1 March 2024).
- Qiao, J.; Lin, X.; Wu, Y.; Huang, X.; Pan, X.; Xu, J.; Wu, J.; Ren, Y.; Shan, P.F. Global burden of non-communicable diseases attributable to dietary risks in 1990–2019. J. Hum. Nutr. Diet 2022, 35, 202–213. [Google Scholar] [CrossRef]
- Ng, S.; Yeatman, H.; Kelly, B.; Sankaranarayanan, S.; Karupaiah, T. Identifying barriers and facilitators in the development and implementation of government-led food environment policies: A systematic review. Nutr. Rev. 2022, 80, 1896–1918. [Google Scholar] [CrossRef]
- Garton, K.; Thow, A.M.; Swinburn, B. International Trade and Investment Agreements as Barriers to Food Environment Regulation for Public Health Nutrition: A Realist Review. Int. J. Health Policy Manag. 2021, 10, 745–765. [Google Scholar] [CrossRef] [PubMed]
- Cullerton, K.; Donnet, T.; Lee, A.; Gallegos, D. Playing the policy game: A review of the barriers to and enablers of nutrition policy change. Public Health Nutr. 2016, 19, 2643–2653. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Nutrition Landscape Information System (NLiS): Nutrition Governance Score. Available online: https://www.who.int/data/nutrition/nlis/info/nutrition-governance-score (accessed on 16 March 2024).
- WHO. The Noncommunicable Disease (NCD) Document Repository. Available online: https://extranet.who.int/ncdccs/documents/default (accessed on 3 March 2024).
- Thow, A.M.; Downs, S.M.; Mayes, C.; Trevena, H.; Waqanivalu, T.; Cawley, J. Fiscal policy to improve diets and prevent noncommunicable diseases: From recommendations to action. Bull. World Health Organ. 2018, 96, 201–210. [Google Scholar] [CrossRef]
- Niebylski, M.L.; Redburn, K.A.; Duhaney, T.; Campbell, N.R. Healthy food subsidies and unhealthy food taxation: A systematic review of the evidence. Nutrition 2015, 31, 787–795. [Google Scholar] [CrossRef]
- Andreyeva, T.; Marple, K.; Marinello, S.; Moore, T.E.; Powell, L.M. Outcomes Following Taxation of Sugar-Sweetened Beverages: A Systematic Review and Meta-analysis. JAMA Netw. Open 2022, 5, e2215276. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.L.; Dono, J.; Wakefield, M.A.; Pettigrew, S.; Coveney, J.; Roder, D.; Durkin, S.J.; Wittert, G.; Martin, J.; Ettridge, K.A. Are Australians ready for warning labels, marketing bans and sugary drink taxes? Two cross-sectional surveys measuring support for policy responses to sugar-sweetened beverages. BMJ Open 2019, 9, e027962. [Google Scholar] [CrossRef] [PubMed]
- Bridge, G.; Lomazzi, M.; Bedi, R. Implementation of a sugar-sweetened beverage tax in low- and middle-income countries: Recommendations for policymakers. J. Public Health Policy 2020, 41, 84–97. [Google Scholar] [CrossRef]
- Shevchenko, O. Environmental and food security as components of ensuring the economic security of Ukraine in a strategic format. Uzhhorod Natl. Univ. Herald. Ser. Law 2022, 68, 110–117. [Google Scholar] [CrossRef]
- Gulich, M.; Petrenko, O. Healthy nutrition as a disease prevention factor: WHO Policy and National Experience (to mark the 75th anniversary of WHO in Ukraine). Medincini Perspekt. 2023, 28, 152–156. [Google Scholar] [CrossRef]
- Candelario, C.M.C. Assessing the Progress of the Philippine Plan of Action for Nutrition From 1974 to 2022: A Narrative Review. Food Nutr. Bull. 2023, 44, 207–220. [Google Scholar] [CrossRef]
- Tee, E.; Florentino, R.; Hardinsyah, H.; Noor, I.; Hlaing, L.; Chotivichien, S.; Hop, L. A review of national plans of action for nutrition in Southeast Asian countries. Malays. J. Nutr. 2020, 26, 501–524. [Google Scholar] [CrossRef]
- Mohapatra, S.C.; Sengupta, P. Health Programs in a Developing Country: Why do we Fail? Health Syst. Policy Res. 2016, 3, 1–7. [Google Scholar] [CrossRef]
- Langlois, E.V.; Mancuso, A.; Elias, V.; Reveiz, L. Embedding implementation research to enhance health policy and systems: A multi-country analysis from ten settings in Latin America and the Caribbean. Health Res. Policy Syst. 2019, 17, 85. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, S.; K Aulakh, B.; Jadeja, N.; Jimenez, M.; Buse, K.; Anwar, I.; Barge, S.; Odubanjo, M.O.; Shukla, A.; Ghaffar, A.; et al. Strengthening capacity to apply health research evidence in policy making: Experience from four countries. Health Policy Plan. 2016, 31, 161–170. [Google Scholar] [CrossRef]
- Jakab, Z.; Selbie, D.; Squires, N.; Mustafa, S.; Saikat, S. Building the evidence base for global health policy: The need to strengthen institutional networks, geographical representation and global collaboration. BMJ Glob. Health 2021, 6, e006852. [Google Scholar] [CrossRef]
- Shawky, S. Geography of Economic Disparities and Global Health Inequality. In Handbook of Global Health; Springer International Publishing: Cham, Switzerland, 2020; pp. 1–14. [Google Scholar]
- Sen, G.; Iyer, A. Beyond Economic Barriers: Intersectionality and Health Policy in Low- and Middle-Income Countries. In The Palgrave Handbook of Intersectionality in Public Policy; The Politics of Intersectionality; Palgrave Macmillan: Cham, Switzerland, 2019; pp. 245–261. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Section | Description |
|---|---|
| Health Information Systems | Functioning system for generating reliable cause-specific mortality data 1 |
| Public Health Infrastructure | Existence of an Operational Unit, Branch, or Department in Ministry of Health with responsibility for NCDs 2 |
| Partnerships and Multisectoral Collaboration | Existence of a national multisectoral commission, agency, or mechanism for NCDs 2 |
| Strategy and Action Plans | Existence of a set of time-bound national targets based on WHO guidance 1 |
| Strategy and Action Plans | Existence of an operational, multisectoral national NCD policy, strategy, or action plan 1 |
| Nutrition Policy | Existence of operational policy/strategy/action plan for unhealthy diet 2 |
| Nutrition Policy | Existence of tax on sugar-sweetened beverages 2 |
| Nutrition Policy | Legislation/regulations fully implementing the International Code of Marketing of Breast Milk Substitutes 1 |
| Nutrition Policy | Existence of any policies on marketing of foods to children 1 |
| Nutrition Policy | Existence of national policies on saturated/ trans fatty acids 1 |
| Nutrition Policy | Existence of any policies to reduce population salt consumption 1 |
| Nutrition Policy | Existence of a tax on foods high in fat, sugars, or salt is implemented in the country. * |
| Nutrition Policy | Existence of price subsidies for healthy foods * |
| Public Education and Awareness | Implementation of a nutrition public awareness program 2 |
| Monitoring and Surveillance | Conduct a STEPS survey or a comprehensive health examination survey every five years 1 |
| Monitoring and Surveillance | A recent national adult risk factor survey is conducted to examine the prevalence of unhealthy diet * |
| Variable | Year | Description | Source | Coverage |
|---|---|---|---|---|
| Literacy Rate | 2018 * | The percentage of people ages 15 and above who can both read and write, and understand a short simple statement about their everyday life. Used as a proxy for the effectiveness of the education system. | World Bank [20] | 135 countries |
| Human Development Index (HDI) | 2021 | A summary measure of average achievement in key dimensions of human development: life expectancy, education, and standard of living. | UNDP [21] | 188 countries |
| GDP per Capita (Thousands) | 2021 | Gross Domestic Product divided by midyear population, in current US dollars. Measures economic output per person, indicating economic prosperity and resource availability. | World Bank [22] | 187 countries |
| Tax Burden | 2021 | Reflects marginal tax rates on income and the overall level of taxation as a percentage of GDP. A composite measure indicating the economic impact of taxation on individuals and corporations. | The Heritage Foundation [23] | 175 countries |
| Current Health Expenditure per Capita (Thousands) | 2020 | Current expenditures on health per capita in current US dollars. Measures the economic resources allocated to health care per person. | World Bank [24] | 185 countries |
| Universal Health Coverage (UHC) Index | 2021 | Coverage index for essential health services (0 to 100). Measures access to essential healthcare services—an aspect of Universal Health Coverage. | WHO [25] | 194 countries |
| Premature Mortality from NCDs | 2019 | The percent of 30-year-old people who would die before their 70th birthday from cardiovascular disease, cancer, diabetes, or chronic respiratory disease. Indicates the burden of major NCDs on the population. | World Bank [26] | 183 countries |
| Population ages 65 and Above | 2022 | The percentage of the total population that is 65 years and above. Indicates the demographic aging of the population and potential NCD burden. | World Bank [27] | 192 countries |
| Total NCD Mortality Rate | 2019 | Age-standardized mortality rate from NCDs per 100,000 persons. Adjusts for differences in the age distribution of the population, indicating the overall NCD mortality burden. | WHO [28] | 183 countries |
| Cost and Affordability of a Healthy Diet | 2021 | The cost of accessing the least expensive locally available foods to meet requirements for a healthy diet. Measures physical and economic access to healthy foods, crucial for preventing NCDs through nutrition. | FAO [29] | 155 countries |
| Prevalence of Obesity among Adults | 2016 | Estimation of age-standardized percentage of adults with a BMI of 30 kg/m2 or higher. Indicates the prevalence of obesity, a major risk factor for several NCDs. | WHO [30] | 190 countries |
| Prevalence of Hypertension among Adults | 2019 | Age-standardized prevalence of raised blood pressure among persons aged 18+ years, defined as systolic blood pressure ≥ 140 and/or diastolic blood pressure ≥90 mmHg. A major risk factor for coronary heart disease and stroke, indicating the burden of NCDs. | WHO [31] | 192 countries |
| Total Alcohol Consumption per Capita | 2019 | Total amount of alcohol consumed per person (15 years of age or older) over a calendar year, in liters of pure alcohol. Associated with the risk of developing health problems such as NCDs. | World Bank [32] | 187 countries |
| Added sugar intake per Capita | 2018 | Estimation of percent of total kcal per day (energy contribution). Represents the energy contribution from added sugars, highlighting diet-related NCD risk. | GDD [33] | 183 countries |
| Sodium intake per Capita | 2018 | Estimation of intake per person in milligrams per day. Quantifies daily sodium intake, critical for understanding dietary risk factors for NCDs. | GDD [33] | 183 countries |
| Saturated fat intake per Capita | 2018 | Estimation of percent of total kcal per day (energy contribution). Assesses energy contribution from saturated fats, which is important for evaluating diet-related NCD risk. | GDD [33] | 183 countries |
| Univariate Linear Regression | Multivariate Linear Regression | |||||
|---|---|---|---|---|---|---|
| Variables of Interest | Effect Size (95% CI) | R2 | p-Value | Effect Size (95% CI) | β | p-Value |
| Literacy Rate | 0.600 (0.487, 0.713) | 0.212 | <0.001 | −0.301 (−0.482, −0.120) | −0.239 | 0.001 |
| HDI | 99.249 (88.780, 109.719) | 0.382 | <0.001 | 14.381 (79.323, 201.438) | 0.843 | <0.001 |
| GDP per Capita | 0.232 (0.161, 0.303) | 0.069 | <0.001 | −0.671 (−1.600, 0.258) | −0.260 | 0.156 |
| Tax Burden | 0.014 (−0.152, 0.180) | 0.000 | 0.866 | −0.183 (−0.428, 0.062) | −0.074 | 0.142 |
| Health Expenditure per Capita | 3.963 (3.020, 4.907) | 0.110 | <0.001 | 2.202 (−1.178, 14.582) | 0.065 | 0.727 |
| UHC Index | 0.908 (0.812, 1.003) | 0.375 | <0.001 | 0.444 (0.087, 0.801) | 0.299 | 0.015 |
| Cost of a Healthy Diet | −4.949 (−7.575, −2.324) | 0.029 | <0.001 | −4.358 (−7.507, −1.210) | −0.128 | 0.007 |
| Inability to Afford Healthy Diet | −0.420 (−0.470, −0.371) | 0.401 | <0.001 | −0.031 (−0.180, 0.118) | −0.046 | 0.682 |
| Population > 65 years (%) | 1.504 (1.246, 1.761) | 0.186 | <0.001 | −0.093 (−0.819, 0.634) | −0.025 | 0.802 |
| NCD Mortality Rate | 0.047 (−0.057, −0.037) | 0.124 | <0.001 | −0.083 (−0.156, −0.010) | −0.532 | 0.026 |
| Premature NCD Mortality | −1.109 (−1.356, −0.863) | 0.125 | <0.001 | 2.348 (0.605, 4.092) | 0.625 | 0.008 |
| Hypertension Prevalence | −0.094 (−0.392, 0.205) | 0.001 | 0.538 | −0.250 (−0.637, 0.137) | −0.069 | 0.205 |
| Obesity Prevalence | 0.427 (0.256, 0.597) | 0.041 | <0.001 | −0.194 (−0.545, 0.157) | −0.071 | 0.277 |
| Alcohol Intake | 1.739 (1.254, 2.223) | 0.082 | <0.001 | −0.322 (−0.953, 0.308) | −0.052 | 0.315 |
| Added Sugars Intake | 0.319 (0.042, 0.596) | 0.009 | 0.024 | 0.027 (−0.265, 0.319) | 0.008 | 0.857 |
| Sodium Intake | 0.012 (0.010, 0.015) | 0.119 | <0.001 | 0.001 (−0.002, 0.004) | 0.034 | 0.459 |
| Saturated Fat Intake | 0.927 (0.297, 1.556) | 0.015 | 0.004 | −0.390 (−1.117, 0.337) | −0.048 | 0.292 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forray, A.I.; Borzan, C.M. Implementation of National Nutrition Policies and Strategies to Reduce Unhealthy Diets: An Ecological Analysis of 194 Countries from 2017 to 2021. Nutrients 2024, 16, 911. https://doi.org/10.3390/nu16060911
Forray AI, Borzan CM. Implementation of National Nutrition Policies and Strategies to Reduce Unhealthy Diets: An Ecological Analysis of 194 Countries from 2017 to 2021. Nutrients. 2024; 16(6):911. https://doi.org/10.3390/nu16060911
Chicago/Turabian StyleForray, Alina Ioana, and Cristina Maria Borzan. 2024. "Implementation of National Nutrition Policies and Strategies to Reduce Unhealthy Diets: An Ecological Analysis of 194 Countries from 2017 to 2021" Nutrients 16, no. 6: 911. https://doi.org/10.3390/nu16060911