

Relative Body Mass Index Improves the BMI Percentile Performance for Detection and Monitoring of Excess Adiposity in Adolescents
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Study Variables
2.3. Definitions
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Baseline Characteristics
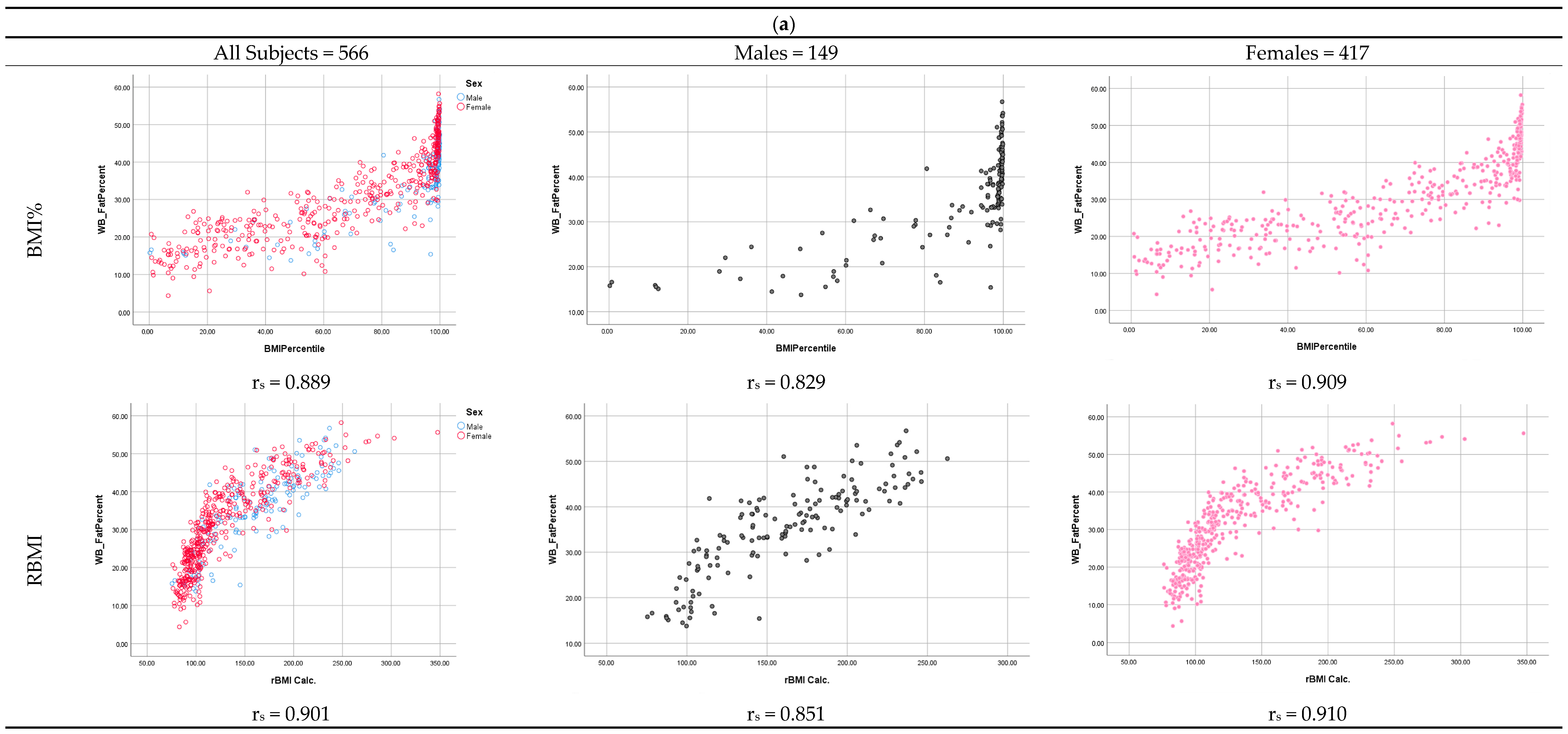
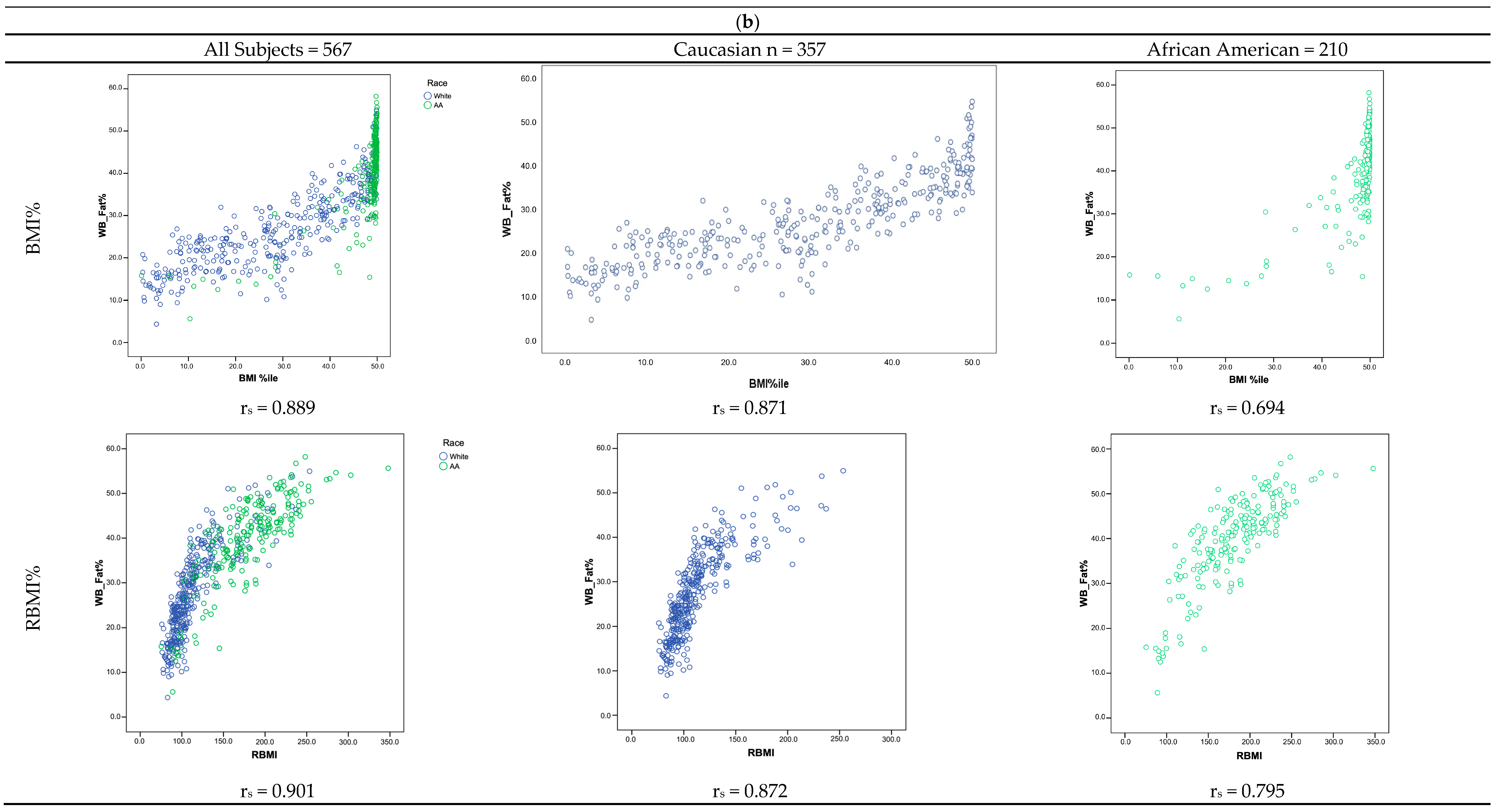
3.2. Correlation of BF% with BMI% and RBMI in Total Sample and by Sex and Race
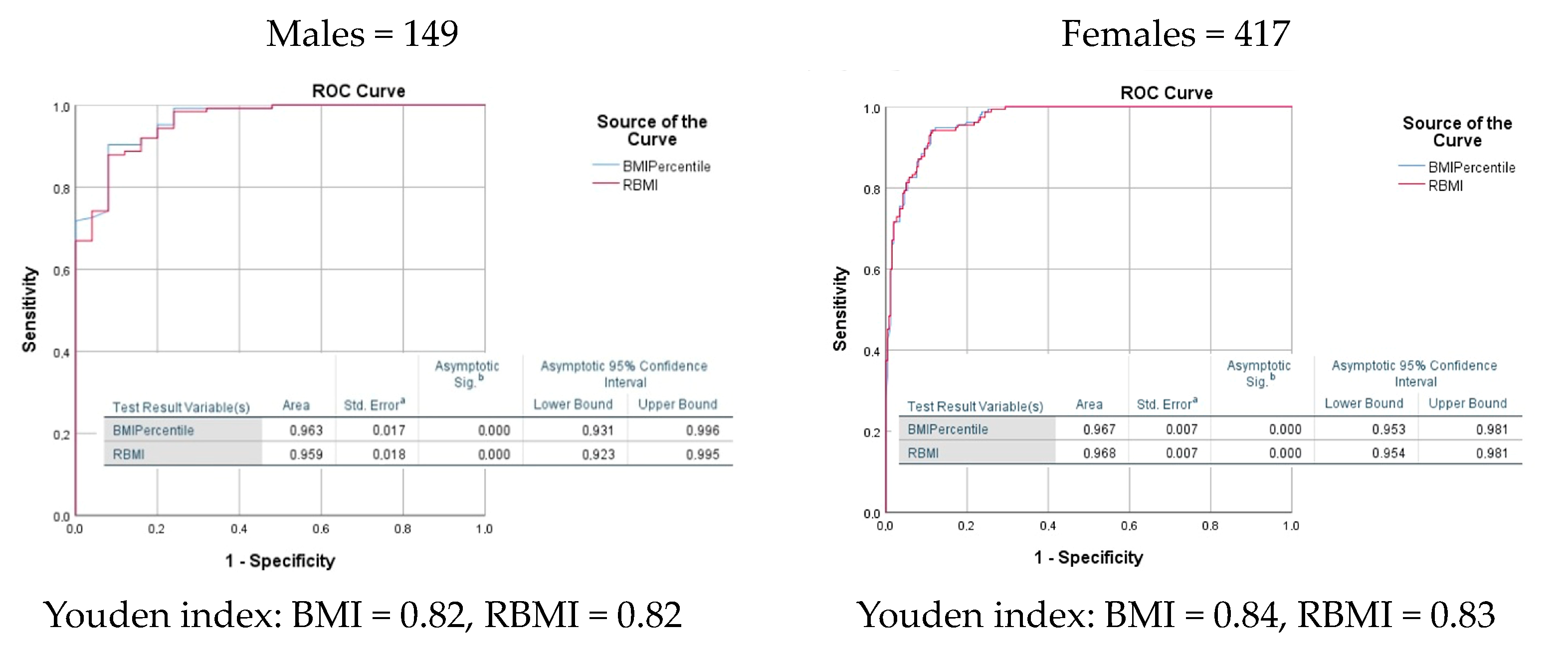
3.3. Comparing Performance of BMI to RBMI at Both Different Levels of BF% and Specific Cut Points to Detect and Categorize Increased BF% by Sex and Race
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Warren, M.; West, M.; Beck, S. The State of Obesity: Better Policies for a Healthier America; Trust for America’s Health: Washington, DC, USA, 2023; pp. 1–103. [Google Scholar]
- Simmonds, M.; Llewellyn, A.; Owen, C.G.; Woolacott, N. Predicting adult obesity from childhood obesity: A systematic review and meta-analysis. Obes. Rev. 2015, 17, 95. [Google Scholar] [CrossRef]
- Ward, Z.J.; Long, M.W.; Resch, S.C.; Giles, C.M.; Cradock, A.L.; Gortmaker, S.L. Simulation of growth trajectories of childhood obesity into adulthood. N. Engl. J. Med. 2017, 377, 2145–2153. [Google Scholar] [CrossRef]
- Demerath, E.W.; Schubert, C.M.; Maynard, L.M.; Sun, S.S.; Chumlea, W.C.; Pickoff, A.; Czerwinski, S.A.; Towne, B.; Siervogel, R.M. Do changes in body mass index percentile reflect changes in body composition in children? Data from the fels longitudinal study. Pediatrics 2006, 117, e487. [Google Scholar] [CrossRef] [PubMed]
- Freedman, D.S.; Wang, J.; Maynard, L.M.; Thornton, J.C.; Mei, Z.; Pierson, R.N., Jr.; Dietz, W.H.; Horlick, M. Relation of BMI to fat and fat-free mass among children and adolescents. Int. J. Obes. 2004, 29, 1. [Google Scholar] [CrossRef]
- Vehrs, P.R.; Fellingham, G.W.; McAferty, A.; Kelsey, L. Trends in BMI percentile and body fat percentage in children 12 to 17 years of age. Children 2022, 9, 744. [Google Scholar] [CrossRef]
- Stierman, B.; Ogden, C.L.; Yanovski, J.A.; Martin, C.B.; Sarafrazi, N.; Hales, C.M. Changes in adiposity among children and adolescents in the United States, 1999–2006 to 2011–2018. Am. J. Clin. Nutr. 2021, 14, 1495–1504. [Google Scholar] [CrossRef] [PubMed]
- Ryder, J.R.; Kaizer, A.M.; Rudser, K.D.; Daniels, S.R.; Kelly, A.S. Utility of body mass index in identifying excess adiposity in youth across the obesity spectrum. J. Pediatr. 2016, 177, 255. [Google Scholar] [CrossRef]
- Williams, D.P.; Going, S.B.; Lohman, T.G.; Harsha, D.W.; Srinivasan, S.R.; Webber, L.S.; Berenson, G.S. Body fatness and risk for elevated blood pressure, total cholesterol, and serum lipoprotein ratios in children and adolescents. Am. J. Public Health. 1992, 82, 358–363. [Google Scholar] [CrossRef]
- Javed, A.; Jumean, M.; Murad, M.H.; Okorodudu, D.; Kumar, S.; Somers, V.K.; Sochor, O.; Lopez-Jimenez, F. Diagnostic performance of body mass index to identify obesity as defined by body adiposity in children and adolescents: A systematic review and meta-analysis. Pediatr. Obes. 2015, 10, 234–244. [Google Scholar] [CrossRef]
- Cole, T.J.; Faith, M.S.; Pietrobelli, A.; Heo, M. What is the best measure of adiposity change in growing children: BMI, BMI%, BMI z-score or BMI centile? Eur. J. Clin. Nutr. 2005, 59, 419–425, Erratum in Eur. J. Clin. Nutr. 2005, 59, 807. [Google Scholar] [CrossRef]
- Velásquez-Mieyer, P.A.; Cowan, P.A.; Pérez-Faustinelli, S.; Nieto-Martínez, R.; Villegas-Barreto, C.; Tolley, E.A.; Lustig, R.H.; Alpert, B.S. Racial disparity in glucagon-like peptide 1 and inflammation markers among severely obese adolescents. Diabetes Care 2008, 31, 770–775. [Google Scholar] [CrossRef]
- Velasquez-Mieyer, P.A.; Cowan, P.A.; Neira, C.P.; Tylavsky, F. Assessing the risk of impaired glucose metabolism in overweight adolescents in a clinical setting. J. Nutr. Health Aging 2008, 12, 750S–757S. [Google Scholar] [CrossRef]
- Velasquez, P.A.; Cowan, P.; Christensen, M.; Lunar, L.; Maxwell, S.; Burghen, G. Can OGTT-derived indices uncover an overweight threshold for deterioration in adolescent glucose metabolism? Diabetologia 2003, 46 (Suppl. S2), A26. [Google Scholar]
- Centers for Disease Control and Prevention, National Center for Health Statistics. CDC Growth Charts: Extended BMI-for-Age Charts. Available online: https://www.cdc.gov/growthcharts/extended-bmi-charts.html (accessed on 24 December 2022).
- National Diabetes Data Group. Classification and diagnosis of diabetes mellitus and other categories of glucose intolerance. Diabetes 1979, 28, 1039–1057. [Google Scholar] [CrossRef]
- Cederholm, J. Findings in a health survey of middle-aged subjects in Uppsala 1981–1982. Risk factors for diabetes mellitus and cardiovascular disease. Upsala J. Med Sci. 1985, 90, 201–227. [Google Scholar] [CrossRef] [PubMed]
- West, K.M. Computing and expressing degree of fatness. JAMA 1980, 243, 1421–1422. [Google Scholar] [CrossRef]
- Velasquez-Mieyer, P.A.; Perez-Faustillino, S.; Cowan, P.A. Identifying children at risk for obesity, type 2 diabetes, and cardiovascular disease. Diabetes Spectr. 2005, 18, 213–220. [Google Scholar] [CrossRef]
- Freedman, D.S.; Sherry, B. The validity of BMI as an indicator of body fatness and risk among children. Pediatrics 2009, 124 (Suppl. S1), S23–S34. [Google Scholar] [CrossRef] [PubMed]
- Mechanick, J.I.; Farkouh, M.E.; Newman, J.D.; Garvey, W.T. Cardiometabolic-based chronic disease, adiposity and dysglycemia drivers: JACC state-of-the-art review. J. Am. Coll. Cardiol. 2020, 75, 525–538. [Google Scholar] [CrossRef] [PubMed]
- Bray, G.A. Beyond BMI. Nutrients 2023, 15, 2254. [Google Scholar] [CrossRef] [PubMed]
- Marshall, T.A.; Curtis, A.M.; Cavanaugh, J.E.; Warren, J.J.; Levy, S.M. Associations between body mass index and body composition measures in a birth cohort. Pediatr. Res. 2021, 91, 1606. [Google Scholar] [CrossRef]
- Freedman, D.S.; Wang, J.; Thornton, J.C.; Mei, Z.; Pierson, R.N.; Dietz, W.H.; Horlick, M. Racial/ethnic differences in body fatness among children and adolescents. Obesity 2008, 16, 1105–1111. [Google Scholar] [CrossRef]
- Gallagher, D.; Visser, M.; Sepulveda, D.; Pierson, R.N.; Harris, T.; Heymsfield, S.B. How useful is body mass index for comparison of body fatness across age, sex, and ethnic groups? Am. J. Epidemiol. 1996, 143, 228–239. [Google Scholar] [CrossRef]
- Nieto-Martinez, R.; Gonzalez-Rivas, J.P.; Florez, H.; Mechanick, J.I. Transcultural endocrinology: Adapting type-2 diabetes guidelines on a global scale. Endocrinol. Metab. Clin. N. Am. 2016, 45, 967–1009. [Google Scholar] [CrossRef]
- Romero-Corral, A.; Somers, V.K.; Sierra-Johnson, J.; Thomas, R.J.; Collazo-Clavell, M.L.; Korinek, J.; Allison, T.G.; Batsis, J.A.; Sert-Kuniyoshi, F.H.; Lopez-Jimenez, F. Accuracy of body mass index in diagnosing obesity in the adult general population. Int. J. Obes. 2008, 32, 959–966. [Google Scholar] [CrossRef]
- Flegal, K.M.; Cole, T.J. Construction of LMS Parameters for the Centers for Disease Control and Prevention 2000 Growth Charts; National Health Statistic Report; US Department of Health and Human Services: Washington, DC, USA, 2013; pp. 1–3.
- Velasquez-Mieyer, P.; Neira, C.P.; Nieto, R.; Cowan, P.A. Obesity and cardiometabolic syndrome in children. Ther. Adv. Cardiovasc. Dis. 2007, 1, 61–81. [Google Scholar] [CrossRef]
- Jebeile, H.; O’Malley, G.; Baur, L.A.; Kelly, A.S. Obesity in children and adolescents: Epidemiology, causes, assessment, and management. Lancet Diabetes Endocrinol. 2022, 10, 351–365. [Google Scholar] [CrossRef]
- Horesh, A.; Tsur, A.M.; Bardugo, A.; Twig, G. Adolescent and childhood obesity and excess morbidity and mortality in young adulthood-a systematic review. Curr. Obes. Rep. 2021, 10, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Gandhe, M.B.; Lenin, M.; Srinivasan, A.R. Evaluation of body mass index (BMI) percentile cut-off levels with reference to insulin resistance: A comparative study on South Indian obese and non-obese adolescents. J. Clin. Diagn. Res. 2013, 7, 1579–1582. [Google Scholar] [CrossRef] [PubMed]
- Simmonds, M.; Llewellyn, A.; Owen, C.G.; Woolacott, N. Simple tests for the diagnosis of childhood obesity: A systematic review and meta-analysis. Obes. Rev. 2016, 17, 1301–1315. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total | Males | Females | p | African Americans | Caucasians | p | |
|---|---|---|---|---|---|---|---|
| N (%) | 567 (100) | 149 (26.3) | 418 (73.7) | 210 (37.0) | 357 (63.0) | ||
| Age (y) | 13.2 (12.0–14.7) | 14.0 (12.2–15.6) | 12.9 (11.9–14.3) | 0.05 | 14.7 (13.0–16.1) | 12.5 (11.7–13.7) | <0.001 |
| Weight (kg) | 56.1 (43.1–90.4) | 82.5 (54.2–112.2) | 51.3 (41.1–76.0) | <0.001 | 94.5 (75.8–113.9) | 46.4 (39.6–56.4) | <0.001 |
| Height (cm) | 157.8 (151.3–164.8) | 162.8 (155.0–170.2) | 157.0 (150.3–163.0) | <0.001 | 162.5 (157.5–169.4) | 154.8 (149.2–161.9) | <0.001 |
| BMI | 22.4 (18.2–33.4) | 31.3 (22.7–39.0) | 20.4 (17.6–29.7) | <0.001 | 35.6 (29.3–41.3) | 19.4 (17.2–22.5) | <0.001 |
| BMI% | 85.0 (48.7–99.7) | 98.7 (86.5–99.5) | 74.3 (36.5–97.1) | <0.001 | 99.9 (96.7–99.5) | 60.5 (32.2–86.8) | <0.001 |
| RBMI | 120.0 (99.7–173.1) | 161.6 (119.5–197.4) | 111.4 (95.3–154.0) | <0.001 | 179.2 (150.6–209.9) | 103.5 (98.6–120.6) | <0.001 |
| BF% (DXA) | 32.2 (22.8–41.0) | 36.7 (29.3–42.1) | 30.0 (21.6–39.6) | <0.001 | 41.4 (34.9–46.5) | 26.2 (20.1–34.3) | <0.001 |
| Measure | All Subjects | Males | Females | African Americans | Caucasians | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| BMI% | RBMI | BMI% | RBMI | BMI% | RBMI | BMI% | RBMI | BMI% | RBMI | |
| Mean (95% CI) | 71.3 (68.8–73.9) | 137.4 (133.4–141.4) | 87.4 (83.7–91.0) | 159.8 (152.2–167.3) | 65.6 (62.5–68.6) | 129.4 (124.9–133.8) | 93.1 (91.8–96.0) | 179.8 (173.7–185.8) | 58.1 (54.9–61.2) | 112.4 (109.3–115.4) |
| Median | 85.0 | 118.7 | 98.7 | 161.4 | 74.3 | 11.1 | 99.0 | 179.2 | 60.5 | 103.5 |
| Standard Deviation | 31.24 | 48.3 | 22.5 | 46.7 | 31.9 | 46.4 | 15.7 | 44.3 | 30.5 | 29.3 |
| Min–Max | 0.2–99.9 | 75.3–347.9 | 0.2–99.9 | 75.3–252.3 | 0.7–99.9 | 76–347 | 0.2–99.9 | 75.3–272.6 | 0.7–99.7 | 76–253 |
| Asymmetry | −0.75 | 0.95 | −2.2 | 0.11 | −0.52 | 1.38 | −3.93 | 0.155 | −0.25 | 1.96 |
| Kolgomorov Test | 0.0001 * | 0.0001 * | 0.0001 * | 0.02 * | 0.0001 * | 0.0001 * | 0.0001 * | 0.20 | 0.0001 * | 0.0001 * |
| Cut point ≥ 25% total body fat | Total | Males | Females | |||||||||
| RBMI | Sen | Spe | Sum | RBMI | Sen | Spe | Sum | RBMI | Sen | Spe | Sum | |
| 110.11 | 84.47 | 95.16 | 179.63 | 114.76 | 89.52 | 84.00 | 173.52 | 105.67 | 87.50 | 91.93 | 179.43 | |
| 110.43 | 84.21 | 95.16 | 179.37 | 115.19 | 88.71 | 84.00 | 172.71 | 105.72 | 87.11 | 91.93 | 179.03 | |
| 110.87 | 83.95 | 95.16 | 179.11 | 116.35 | 88.71 | 88.00 | 176.71 | 105.76 | 87.11 | 92.55 | 179.66 | |
| 111.05 | 83.68 | 95.16 | 178.85 | 117.17 | 87.90 | 88.00 | 175.90 | 105.90 | 87.11 | 93.17 | 180.28 | |
| 111.10 | 83.42 | 95.16 | 178.58 | 117.54 | 87.90 | 92.00 | 179.90 | 106.05 | 87.11 | 93.79 | 180.90 | |
| 111.21 | 83.16 | 95.16 | 178.32 | 118.38 | 87.10 | 92.00 | 179.10 | 106.12 | 86.72 | 93.79 | 180.51 | |
| 111.37 | 82.89 | 95.16 | 178.06 | 119.25 | 86.29 | 92.00 | 178.29 | 106.58 | 86.33 | 93.79 | 180.12 | |
| 111.48 | 82.63 | 95.16 | 177.79 | 123.01 | 85.48 | 92.00 | 177.48 | 107.09 | 85.94 | 93.79 | 179.73 | |
| 111.62 | 82.37 | 95.16 | 177.53 | 126.98 | 84.68 | 92.00 | 176.68 | 107.26 | 85.55 | 93.79 | 179.34 | |
| 111.74 | 82.11 | 95.16 | 177.27 | 127.78 | 83.87 | 92.00 | 175.87 | 107.40 | 85.55 | 94.41 | 179.96 | |
| Cut point ≥ 30% total body fat | Total | Males | Females | |||||||||
| RBMI | Sen | Spe | Sum | RBMI | Sen | Spe | Sum | RBMI | Sen | Spe | Sum | |
| 109.51 | 94.97 | 85.08 | 180.05 | 117.54 | 93.52 | 75.61 | 169.13 | 109.21 | 94.29 | 88.89 | 183.17 | |
| 109.54 | 94.65 | 85.08 | 179.73 | 118.38 | 92.59 | 75.61 | 168.20 | 109.46 | 94.29 | 89.37 | 183.66 | |
| 109.59 | 94.65 | 85.48 | 180.14 | 119.25 | 92.59 | 78.05 | 170.64 | 109.54 | 93.81 | 89.37 | 183.18 | |
| 109.66 | 94.65 | 85.89 | 180.54 | 123.01 | 91.67 | 78.05 | 169.72 | 109.59 | 93.81 | 89.86 | 183.66 | |
| 109.80 | 94.65 | 86.29 | 180.94 | 126.98 | 91.67 | 80.49 | 172.15 | 109.75 | 93.81 | 90.34 | 184.15 | |
| 109.89 | 94.34 | 86.29 | 180.63 | 127.78 | 90.74 | 80.49 | 171.23 | 109.89 | 93.33 | 90.34 | 183.67 | |
| 109.93 | 94.03 | 86.29 | 180.32 | 129.33 | 89.81 | 80.49 | 170.30 | 109.93 | 92.86 | 90.34 | 183.20 | |
| 110.00 | 94.03 | 86.69 | 180.72 | 130.85 | 88.89 | 80.49 | 169.38 | 110.00 | 92.86 | 90.82 | 183.68 | |
| 110.07 | 93.71 | 86.69 | 180.40 | 131.49 | 87.96 | 80.49 | 168.45 | 110.07 | 92.38 | 90.82 | 183.20 | |
| 110.11 | 93.40 | 86.69 | 180.09 | 132.48 | 87.04 | 80.49 | 167.52 | 110.11 | 91.90 | 90.82 | 182.73 | |
| Cut point ≥ 85th percentile total body fat | Total | Males | Females | |||||||||
| RBMI | Sen | Spe | Sum | RBMI | Sen | Spe | Sum | RBMI | Sen | Spe | Sum | |
| 171.93 | 87.50 | 91.97 | 179.47 | 147.94 | 85.23 | 83.61 | 168.83 | 134.23 | 92.38 | 87.50 | 179.88 | |
| 172.76 | 87.50 | 92.24 | 179.74 | 148.57 | 84.09 | 83.61 | 167.70 | 134.55 | 92.38 | 87.82 | 180.20 | |
| 173.61 | 87.50 | 92.52 | 180.02 | 149.60 | 82.95 | 83.61 | 166.56 | 134.91 | 92.38 | 88.14 | 180.52 | |
| 175.32 | 87.50 | 92.80 | 180.30 | 150.09 | 82.95 | 85.25 | 168.20 | 135.04 | 92.38 | 88.46 | 180.84 | |
| 176.86 | 87.50 | 93.07 | 180.57 | 152.48 | 82.95 | 86.89 | 169.84 | 135.74 | 92.38 | 88.78 | 181.16 | |
| 177.21 | 85.71 | 93.07 | 178.79 | 156.98 | 81.82 | 86.89 | 168.70 | 136.48 | 91.43 | 88.78 | 180.21 | |
| 177.47 | 83.93 | 93.07 | 177.00 | 159.30 | 80.68 | 86.89 | 167.57 | 136.58 | 90.48 | 88.78 | 179.26 | |
| 177.91 | 83.93 | 93.35 | 177.28 | 159.90 | 79.55 | 86.89 | 166.43 | 136.61 | 89.52 | 88.78 | 178.31 | |
| 178.69 | 83.93 | 93.63 | 177.56 | 160.78 | 78.41 | 86.89 | 165.29 | 136.84 | 89.52 | 89.10 | 178.63 | |
| 179.21 | 82.14 | 93.63 | 175.77 | 161.38 | 77.27 | 86.89 | 164.16 | 137.15 | 89.52 | 89.42 | 178.95 | |
| Cut point ≥ 95th percentile total body fat | Total | Males | Females | |||||||||
| RBMI | Sen | Spe | Sum | RBMI | Sen | Spe | Sum | RBMI | Sen | Spe | Sum | |
| 150.34 | 95.12 | 83.52 | 178.64 | 170.52 | 91.07 | 82.80 | 173.87 | 150.02 | 92.54 | 86.57 | 179.11 | |
| 150.57 | 95.12 | 83.75 | 178.87 | 171.31 | 91.07 | 83.87 | 174.94 | 150.57 | 92.54 | 86.86 | 179.39 | |
| 151.73 | 95.12 | 83.97 | 179.09 | 171.92 | 91.07 | 84.95 | 176.02 | 151.73 | 92.54 | 87.14 | 179.68 | |
| 152.95 | 95.12 | 84.20 | 179.32 | 172.74 | 91.07 | 86.02 | 177.09 | 152.95 | 92.54 | 87.43 | 179.97 | |
| 153.07 | 95.12 | 84.42 | 179.55 | 173.90 | 91.07 | 87.10 | 178.17 | 153.07 | 92.54 | 87.71 | 180.25 | |
| 153.30 | 94.31 | 84.42 | 178.73 | 174.63 | 89.29 | 87.10 | 176.38 | 153.30 | 91.04 | 87.71 | 178.76 | |
| 154.16 | 94.31 | 84.65 | 178.96 | 174.76 | 89.29 | 88.17 | 177.46 | 154.43 | 91.04 | 88.00 | 179.04 | |
| 155.10 | 93.50 | 84.65 | 178.15 | 175.00 | 87.50 | 88.17 | 175.67 | 155.64 | 91.04 | 88.29 | 179.33 | |
| 155.64 | 93.50 | 84.88 | 178.37 | 175.19 | 85.71 | 88.17 | 173.89 | 156.61 | 91.04 | 88.57 | 179.62 | |
| 156.61 | 93.50 | 85.10 | 178.60 | 175.98 | 83.93 | 88.17 | 172.10 | 157.40 | 89.55 | 88.57 | 178.12 | |
| Categories | Males | Females | Both Sexes | |||||
|---|---|---|---|---|---|---|---|---|
| Traditional | Adiposity by BF% | BF Cut Points (%) | Reported RBMI Cut Points (%) | Proposed RBMI Cut Points (%) | BF Cut Points (%) | Reported RBMI Cut Points (%) | Proposed RBMI Cut Points (%) | Proposed RBMI Cut Points (%) |
| NW | Normal Adiposity | <20 | <100 | ≥75–<100 | <25 | <106.1 | ≥75–<110 | ≥75–<100 |
| OW | Mildly high Adiposity | ≥20–<25 | <117.6 | ≥100–<120 | ≥25–<35 | <117.7 | ≥110–<120 | ≥100–<120 |
| OB | Moderately high adiposity | ≥25–<35 | <161.7 | ≥120–<160 | ≥35–<45 | <160.0 | ≥120–<160 | ≥120–<160 |
| SVOB | Severely high adiposity | ≥35 | ≥161.7 | ≥160 | ≥45 | ≥160.0 | ≥160 | ≥160 |
| Adiposity Categories | Total (n = 567) | Males (n = 149) | Females (n = 418) | African Americans (n = 210) | Caucasians (n = 357) | |
|---|---|---|---|---|---|---|
| BMI% | NW (<85th %ile) | 65.9 (62.0–69.6) | 40.2 (32.0–48.8) | 72.8 (68.6–76.6) | 9.5 (6.2–14.2) | 73.7 (68.9–78.0) |
| OW (≥85th and <95th %ile) | 12.0 (9.6–14.8) | 11.8 (7.3–18.6) | 12.0 (9.4–15.3) | 8.1 (5.1–12.6) | 12.4 (9.1–15.8) | |
| OB (≥95th BMI–<99th %ile) | 11.5 (9.2–14.3) | 24.4 (17.8–32.6) | 8.0 (5.9–10.8) | 31.0 (25.1–37.5) | 9.2 (6.7–12.7) | |
| SVOB (≥99th %ile) | 10.6 (8.4–13.4) | 23.6 (17.1–31.7) | 7.2 (5.2–9.9) | 51.4 (44.7–58.1) | 5.0 (3.2–7.8) | |
| RBMI | NW (<100%) | 36.4 (32.7–40.4) | 21.3 (15.0–29.2) | 40.5 (36.2–45.0) | 3.8 (1.9–7.3) | 37.8 (32.9–42.9) |
| OW (≥100 <120%) | 31.8 (28.2–35.6) | 26.0 (19.1–34.2) | 33.3 (29.2–37.7) | 6.2 (3.6–10.3) | 35.9 (31.0–40.9 | |
| OB (≥120 <160%) | 17.0 (14.2–20.2) | 22.8 (16.4–30.8) | 15.4 (12.4–18.9) | 21.4 (16.4–27.5) | 17.6 (14.0–21.9) | |
| SVOB (≥160%) | 14.8 (12.2–17.8) | 29.9 (22.6–38.4) | 10.8 (8.3–13.8) | 68.6 (61.5–74.0) | 8.7 (6.2–12.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velasquez-Mieyer, P.A.; Nieto-Martinez, R.; Neira, C.P.; De Oliveira-Gomes, D.; Velasquez Rodriguez, A.E.; Ugel, E.; Cowan, P.A. Relative Body Mass Index Improves the BMI Percentile Performance for Detection and Monitoring of Excess Adiposity in Adolescents. Nutrients 2024, 16, 703. https://doi.org/10.3390/nu16050703
Velasquez-Mieyer PA, Nieto-Martinez R, Neira CP, De Oliveira-Gomes D, Velasquez Rodriguez AE, Ugel E, Cowan PA. Relative Body Mass Index Improves the BMI Percentile Performance for Detection and Monitoring of Excess Adiposity in Adolescents. Nutrients. 2024; 16(5):703. https://doi.org/10.3390/nu16050703
Chicago/Turabian StyleVelasquez-Mieyer, Pedro A., Ramfis Nieto-Martinez, Claudia P. Neira, Diana De Oliveira-Gomes, Andres E. Velasquez Rodriguez, Eunice Ugel, and Patricia A. Cowan. 2024. "Relative Body Mass Index Improves the BMI Percentile Performance for Detection and Monitoring of Excess Adiposity in Adolescents" Nutrients 16, no. 5: 703. https://doi.org/10.3390/nu16050703