
Different Dimensions of the Home Food Environment May Be Associated with the Body Mass Index of Older Adults: A Cross-Sectional Survey Conducted in Beijing, China

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Sample
2.3.1. Sampling Method
2.3.2. Sample Size Calculation
2.4. Ethical Review
2.5. Measurements
2.5.1. Participants’ Basic Information
2.5.2. Home Food Availability
2.5.3. Food Intake Information
2.5.4. Home Socioeconomic Status (SES)
2.5.5. Physical Measurement
2.6. Variables
2.6.1. Body Mass Index
2.6.2. Home Food Environment Variables
2.6.3. Confounders
2.7. Statistical Methods
3. Results
3.1. Participant Characteristics
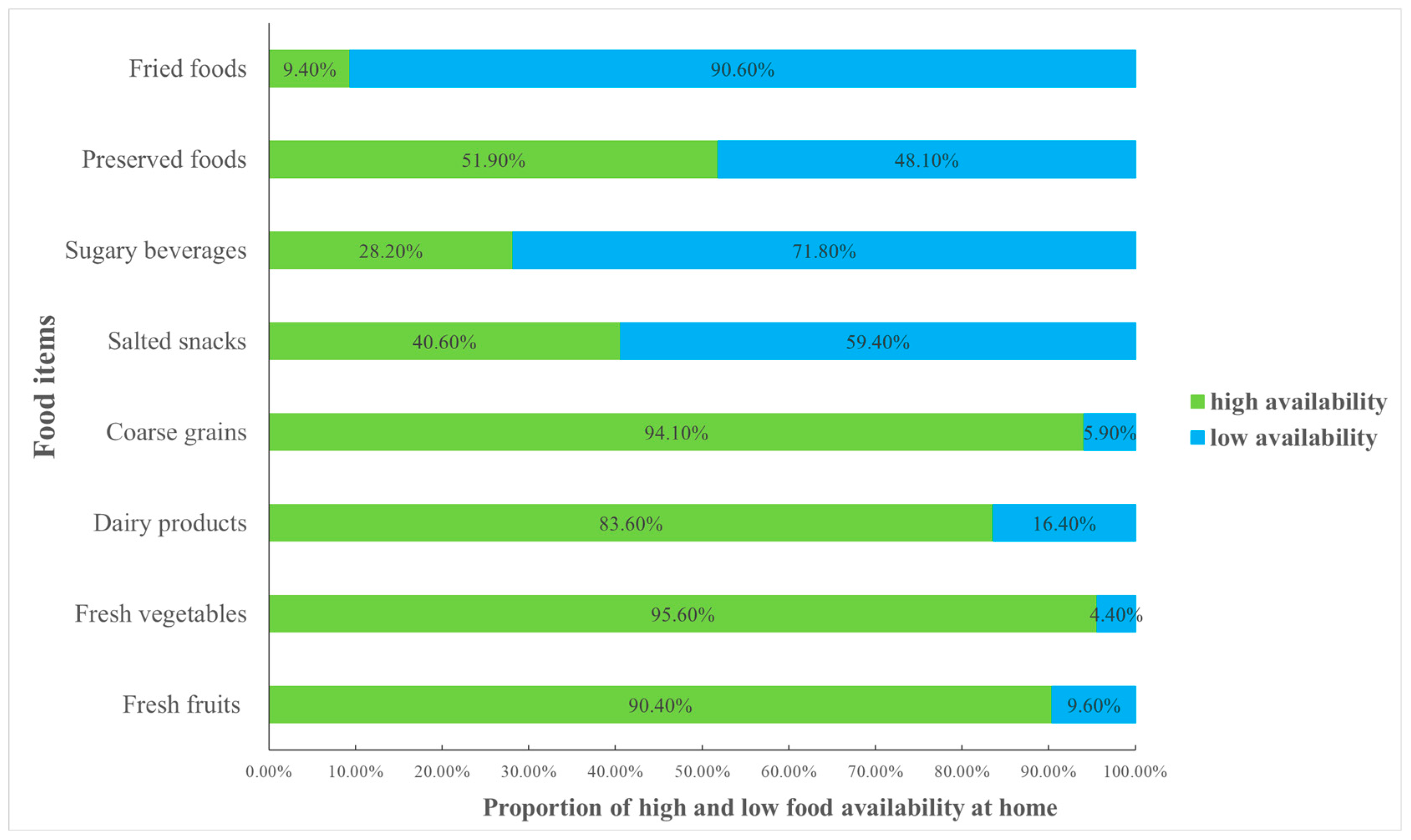
3.2. Home Food Availability
3.3. Living Conditions
3.4. Univariate Analysis of BMI
3.5. Association between Home Food Environment and BMI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Bureau of Statistics. National Data. Available online: https://data.stats.gov.cn/easyquery.htm?cn=C01 (accessed on 26 September 2023).
- Chen, X.; Iles, J.; Yao, Y.; Yip, W.; Meng, Q.; Berkman, L.; Chen, H.; Chen, X.; Feng, J.; Feng, Z.; et al. The path to healthy ageing in China: A Peking University-Lancet Commission. Lancet 2022, 400, 1967–2006. [Google Scholar] [CrossRef] [PubMed]
- Asia Pacific Cohort Studies Collaboration. The burden of overweight and obesity in the Asia-Pacific region. Obes. Rev. 2007, 8, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Du, S.; Lu, B.; Zhai, F.; Popkin, B.M. A new stage of the nutrition transition in China. Public Health Nutr. 2002, 5, 169–174. [Google Scholar] [CrossRef] [PubMed]
- National Health Commission Disease Prevention and Control Bureau. Report on Nutrition and Chronic Disease Status of Chinese Residents; People’s Medical Publishing House: Beijing, China, 2020. [Google Scholar]
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef] [PubMed]
- Bleich, S.; Cutler, D.; Murray, C.; Adams, A. Why is the developed world obese? Annu. Rev. Public Health 2008, 29, 273–295. [Google Scholar] [CrossRef]
- Story, M.; Kaphingst, K.M.; Robinson-O’Brien, R.; Glanz, K. Creating healthy food and eating environments: Policy and environmental approaches. Annu. Rev. Public Health 2008, 29, 253–272. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.J.; Crawford, D.A.; Salmon, J.; Carver, A.; Garnett, S.P.; Baur, L.A. Associations between the home food environment and obesity-promoting eating behaviors in adolescence. Obesity 2007, 15, 719–730. [Google Scholar] [CrossRef]
- Rosenkranz, R.R.; Dzewaltowski, D.A. Model of the home food environment pertaining to childhood obesity. Nutr. Rev. 2008, 66, 123–140. [Google Scholar] [CrossRef]
- Swinburn, B.; Egger, G.; Raza, F. Dissecting obesogenic environments: The development and application of a framework for identifying and prioritizing environmental interventions for obesity. Prev. Med. 1999, 29, 563–570. [Google Scholar] [CrossRef]
- Kegler, M.C.; Hermstad, A.; Haardorfer, R. Home food environment and associations with weight and diet among U.S. adults: A cross-sectional study. BMC Public Health 2021, 21, 1032. [Google Scholar] [CrossRef]
- Emery, C.F.; Olson, K.L.; Lee, V.S.; Habash, D.L.; Nasar, J.L.; Bodine, A. Home environment and psychosocial predictors of obesity status among community-residing men and women. Int. J. Obes. 2015, 39, 1401–1407. [Google Scholar] [CrossRef] [PubMed]
- Gorin, A.A.; Phelan, S.; Raynor, H.; Wing, R.R. Home food and exercise environments of normal-weight and overweight adults. Am. J. Health Behav. 2011, 35, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Kegler, M.C.; Alcantara, I.; Haardorfer, R.; Gazmararian, J.A.; Ballard, D.; Sabbs, D. The influence of home food environments on eating behaviors of overweight and obese women. J. Nutr. Educ. Behav. 2014, 46, 188–196. [Google Scholar] [CrossRef]
- Newton, S.; Braithwaite, D.; Akinyemiju, T.F. Socio-economic status over the life course and obesity: Systematic review and meta-analysis. PLoS ONE 2017, 12, e0177151. [Google Scholar] [CrossRef] [PubMed]
- Dinsa, G.D.; Goryakin, Y.; Fumagalli, E.; Suhrcke, M. Obesity and socioeconomic status in developing countries: A systematic review. Obes. Rev. 2012, 13, 1067–1079. [Google Scholar] [CrossRef]
- He, W.; James, S.A.; Merli, M.G.; Zheng, H. An increasing socioeconomic gap in childhood overweight and obesity in China. Am. J. Public Health 2014, 104, e14–e22. [Google Scholar] [CrossRef]
- Su, X.; Liu, T.; Li, N.N.; Sun, J.; Cui, J.M.; Zhu, W.L. Development and Assessment of Home Food Environment Measurement Questionnaire for School-aged Children. Food Nutr. China 2020, 26, 74–79. [Google Scholar] [CrossRef]
- Song, M.N.; Cheng, X.; Kong, J.X.; Wang, H.M. Prevalence and influencing factors of overweight and obesity among middle-aged and elderly people in China. Chin. J. Dis. Control Prev. 2018, 22, 804–808. [Google Scholar] [CrossRef]
- Zhang, M.; Jiang, Y.; Li, Y.; Wang, L.; Zhao, W. Prevalence of overweight and obesity among Chinese elderly aged 60 and above in 2010. Zhonghua Liu Xing Bing Xue Za Zhi 2014, 35, 365–369. [Google Scholar] [CrossRef]
- Beijing Municipal Bureau of Statistics. Beijing Statistical Zoning Code and Urban Rural Classification Code (2018 Edition). Available online: https://tjj.beijing.gov.cn/zwgkai/tjbz_31390/xzqhhcxfl_31391/cxfl_31674/202002/t20200214_1631903.html (accessed on 9 January 2024).
- Chai, W.; Fan, J.X.; Wen, M. Association of Individual and Neighborhood Factors with Home Food Availability: Evidence from the National Health and Nutrition Examination Survey. J. Acad. Nutr. Diet 2018, 118, 815–823. [Google Scholar] [CrossRef]
- Jin, Y. Study on Associations of Dietary Diversity with Nutrients Adequacy and Nutrition Related Chronic Disease in Chinese Adults; China Centre for Disease Control and Prevention: Beijing, China, 2009. [Google Scholar]
- Hu, Q.Q.; Han, X.X.; Ma, A.G.; Li, X.L. Investigation and analysis of dietary diversity score and health status of middle-aged and elderly people in rural areas. Food Nutr. China 2009, 12, 58–61. [Google Scholar]
- Jin, Y.; Li, Y.P.; Hu, X.Q.; Cui, Z.H.; He, Y.N.; Ma, G.S. Association between dietary diversity and nutrients adequacy in Chinese adults. Acta Nutr. Sin. 2009, 31, 21–25. [Google Scholar] [CrossRef]
- Zhan, S.L. The Influence of Family Socioeconomic Status on Student Academic Performance from Individual and School Perspectives: Insights from the Programme for International Student Assessment (PISA). J. Shanghai Educ. Res. 2009, 10–13. [Google Scholar]
- Chen, Y.H.; Cheng, G.; Guan, Y.S.; Zhang, D.J. The Mediating Effects of Subjective Social Status on the Relations between Self-Esteem and Socioeconomic Status for College Students. Psychol. Dev. Educ. 2014, 30, 594–600. [Google Scholar] [CrossRef]
- Guo, Y.R. Research on Environmental Influencing Factors of Overweight andObesity of Children and Adolescents in China; East China Normal University: Shanghai, China, 2020. [Google Scholar]
- Li, C.L. Stratification of Reputation in Contemporary Chinese Society: Measurement of Occupational Reputation and Socioeconomic Status Index. Sociol. Stud. 2005, 74–102. [Google Scholar] [CrossRef]
- General Administration of Sport of China. National Physical Fitness Standard Handbook; Senior Part; People’s Sports Publishing House of China: Beijing, China, 2003. [Google Scholar]
- Chinese Nutrition Society. Dietary Guidelines for Chinese Residents; People’s Medical Publishing House: Beijing, China, 2022. [Google Scholar]
- Zhang, M.; Guo, W.; Zhang, N.; He, H.R.; Zhang, Y.; Zhou, M.Z.; Zhang, J.F.; Li, M.X.; Ma, G.S. Association between Neighborhood Food Environment and Body Mass Index among Older Adults in Beijing, China: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 7658. [Google Scholar] [CrossRef] [PubMed]
- Tong, G.X.; Gao, X.; Xu, R.Y.; Qin, Y.; Huang, L.; Wang, X.M.; Song, W.J. Relationship between dietary pattern and risk of suffering from hypertension in physical examinees aged 35 years and above in Haidian District of Beijing. Pract. Prev. Med. 2022, 29, 906–911. [Google Scholar]
- Zhang, R.; Li, H.; Li, N.; Shi, J.F.; Li, J.; Chen, H.D.; Ren, J.S.; Chen, W.Q. Nested Case-control Study of Risk Factors for Upper Gastrointestinal Cancer Based on Population Screening Cohort in Urban Areas of China. China Cancer 2021, 30, 321–327. [Google Scholar]
- Wang, M.X.; Zhang, G.D.; Jiang, H.J.; Liu, X.M.; Peng, Y.H. Meta-analysis of the relationship between intake of pickled food in Chinese population and primary liver cancer. Clin. Res. Pract. 2020, 5, 1–4. [Google Scholar] [CrossRef]
- Li, H. Study on the Health Status and Related Factors of Civil Servant in Changchun District Government; Ji Lin University: Changchun, China, 2012. [Google Scholar]
- Tani, Y.; Kondo, N.; Takagi, D.; Saito, M.; Hikichi, H.; Ojima, T.; Kondo, K. Combined effects of eating alone and living alone on unhealthy dietary behaviors, obesity and underweight in older Japanese adults: Results of the JAGES. Appetite 2015, 95, 1–8. [Google Scholar] [CrossRef]
- Yamamoto, R.; Shinzawa, M.; Yoshimura, R.; Taneike, M.; Nakanishi, K.; Nishida, M.; Yamauchi-Takihara, K.; Kudo, T.; Moriyama, T. Living alone and prediction of weight gain and overweight/obesity in university students: A retrospective cohort study. J. Am. Coll. Health 2023, 71, 1417–1426. [Google Scholar] [CrossRef] [PubMed]
- Hammons, A.J.; Fiese, B.H. Is frequency of shared family meals related to the nutritional health of children and adolescents? Pediatrics 2011, 127, e1565–e1574. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.S. Research on Beijing Community Old Age Table Service Demand; Capital University of Economics and Business: Beijing, China, 2017. [Google Scholar]
- Hou, J. Research on Supply and Demand Deviation and Optimization Strategy of Catering Service for the Elderly in Xi’an Urban Community from the Perspective of Holistic Governance—Take District X as An Example; Northwest University: Xi’an, China, 2022. [Google Scholar]
- Yu, S.W. The Research on Service Improvement Planning of Community Canteens for the Elderly in Changsha from the Perspective of Urban Catalyst; Hunan University: Changsha, China, 2022. [Google Scholar]
- Wing, R.R.; Lang, W.; Wadden, T.A.; Safford, M.; Knowler, W.C.; Bertoni, A.G.; Hill, J.O.; Brancati, F.L.; Peters, A.; Wagenknecht, L.; et al. Benefits of modest weight loss in improving cardiovascular risk factors in overweight and obese individuals with type 2 diabetes. Diabetes Care 2011, 34, 1481–1486. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.; Burke, L.E.; Bray, G.A.; Blair, S.; Allison, D.B.; Pi-Sunyer, X.; Hong, Y.; Eckel, R.H.; American Heart Association Council on Nutrition; Physical Activity. Clinical implications of obesity with specific focus on cardiovascular disease: A statement for professionals from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism: Endorsed by the American College of Cardiology Foundation. Circulation 2004, 110, 2952–2967. [Google Scholar] [CrossRef]
- Cobb, L.K.; Appel, L.J.; Franco, M.; Jones-Smith, J.C.; Nur, A.; Anderson, C.A. The relationship of the local food environment with obesity: A systematic review of methods, study quality, and results. Obesity 2015, 23, 1331–1344. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Food Item | Concept and Examples |
|---|---|
| Fresh fruits | Natural, fresh, unprocessed fruits, such as apples, bananas, strawberries, watermelons, oranges, etc. |
| Fresh vegetables | Natural, fresh, unprocessed vegetables, such as leafy vegetables, fresh beans, rhizomes, melons, eggplant fruits, bacteria, algae, etc. |
| Dairy products | A variety of dairy products, such as fresh milk, cheese, yogurt, butter, cream, etc. |
| Coarse grains | Whole grains or cereals that have not been refined, including brown rice, quinoa, barley, oats, millet, buckwheat, etc. |
| Salted snacks | A category of foods that are typically savory in taste and contain added salt or salt-based flavorings, including potato chips, pretzels, popcorn, crackers, meat snacks like beef jerky, etc. |
| Sugary beverages | Drinks sweetened with various forms of sugar or sweeteners, including sodas, fruit juices, energy drinks, sweetened teas, flavored coffees, etc. |
| Preserved foods | Foods typically made by preservation with sugar or salt, including pickled vegetables, salted fish, salted eggs, salted meat, etc. |
| Fried foods | Various foods that are cooked by being submerged in hot oil or fat, such as French fries, fried chicken, tempura, onion rings, etc. |
| Item | Classification | n | % |
|---|---|---|---|
| BMI (kg/m2) | Underweight: below 20.0 | 45 | 2.6 |
| Normal: 20–26.9 | 950 | 53.8 | |
| Overweight and obese: 27.0 and above | 769 | 43.6 | |
| Gender | Male | 730 | 41.4 |
| Female | 1034 | 58.6 | |
| Age | 65–69 | 983 | 55.7 |
| 70–74 | 483 | 27.4 | |
| 75–79 | 298 | 16.9 | |
| Marital status | Unmarried | 3 | 0.2 |
| Married | 1482 | 84.0 | |
| Widowed | 260 | 14.7 | |
| Separated or divorced | 19 | 1.1 | |
| Educational level | Higher education | 190 | 10.8 |
| Secondary education 1 | 923 | 52.3 | |
| ≤Primary education | 651 | 36.9 | |
| Income level (RMB) 2 | ≤2000 | 409 | 23.2 |
| 2000–3500 | 652 | 37.0 | |
| 3500–5000 | 376 | 21.3 | |
| 5000–10,000 | 223 | 12.6 | |
| ≥10,000 | 24 | 1.4 | |
| Missing | 80 | 4.5 | |
| Neighborhood socioeconomic level | Urban | 899 | 51.0 |
| Suburban | 865 | 49.0 | |
| Frequency of exercise | Never | 198 | 11.2 |
| 1–2 times per week | 55 | 3.1 | |
| 3–4 times per week | 83 | 4.7 | |
| 5–6 times per week | 35 | 2.0 | |
| Every day | 1387 | 78.6 | |
| Missing | 6 | 0.3 | |
| Smoking | No 3 | 1464 | 83.0 |
| Yes | 300 | 17.0 | |
| Drinking | Once a week or more | 436 | 24.7 |
| Less than once a week | 1325 | 75.1 | |
| missing | 3 | 0.2 |
| Variables | Group | n | BMI | t/F | p |
|---|---|---|---|---|---|
| SES | High | 588 | 25.9 ± 3.4 | 5.403 | 0.005 |
| Medium | 588 | 26.5 ± 3.5 | |||
| Low | 588 | 26.4 ± 3.6 | |||
| Living condition | Living alone | 128 | 27.2 ± 3.8 | −3.237 | 0.001 |
| Not living alone | 1636 | 26.2 ± 3.5 | |||
| Availability of fresh fruits | High | 1594 | 26.3 ± 3.5 | −1.738 | 0.082 |
| Low | 170 | 25.8 ± 3.6 | |||
| Availability of fresh vegetables | High | 1686 | 26.2 ± 3.5 | 1.392 | 0.164 |
| Low | 78 | 26.8 ± 3.7 | |||
| Availability of dairy products | High | 1475 | 26.2 ± 3.5 | 1.019 | 0.308 |
| Low | 289 | 26.5 ± 3.4 | |||
| Availability of coarse grains | High | 1660 | 26.3 ± 3.5 | −0.960 | 0.337 |
| Low | 104 | 26.0 ± 3.3 | |||
| Availability of salted snacks | High | 717 | 26.2 ± 3.5 | 1.080 | 0.280 |
| Low | 1047 | 26.4 ± 3.5 | |||
| Availability of sugary beverages | High | 498 | 26.2 ± 3.5 | 0.446 | 0.656 |
| Low | 1266 | 26.3 ± 3.5 | |||
| Availability of preserved foods | High | 915 | 26.4 ± 3.4 | −1.772 | 0.076 |
| Low | 849 | 26.1 ± 3.6 | |||
| Availability of fried foods | High | 165 | 26.5 ± 3.7 | −0.783 | 0.433 |
| Low | 1599 | 26.2 ± 3.5 |
| Variable | Model 1 1 | Model 2 2 | ||||
|---|---|---|---|---|---|---|
| β | SE | p | β | SE | p | |
| SES | −0.280 | 0.104 | 0.007 | −0.356 | 0.108 | 0.001 |
| Living condition | 1.053 | 0.321 | 0.001 | 1.155 | 0.319 | <0.001 |
| Fresh fruits | 0.865 | 0.297 | 0.004 | - | ||
| Fresh vegetables | −0.902 | 0.417 | 0.031 | - | ||
| Dairy products | - | - | ||||
| Coarse grains | - | - | ||||
| Salted snacks | - | - | ||||
| Sugary beverages | - | - | ||||
| Preserved foods | - | 0.442 | 0.166 | 0.008 | ||
| Fried foods | - | - | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, M.; Chi, R.; Li, Z.; Fang, Y.; Zhang, N.; Wan, Q.; Ma, G. Different Dimensions of the Home Food Environment May Be Associated with the Body Mass Index of Older Adults: A Cross-Sectional Survey Conducted in Beijing, China. Nutrients 2024, 16, 289. https://doi.org/10.3390/nu16020289
Zhang M, Chi R, Li Z, Fang Y, Zhang N, Wan Q, Ma G. Different Dimensions of the Home Food Environment May Be Associated with the Body Mass Index of Older Adults: A Cross-Sectional Survey Conducted in Beijing, China. Nutrients. 2024; 16(2):289. https://doi.org/10.3390/nu16020289
Chicago/Turabian StyleZhang, Man, Ruixin Chi, Zhenhui Li, Yujie Fang, Na Zhang, Qiaoqin Wan, and Guansheng Ma. 2024. "Different Dimensions of the Home Food Environment May Be Associated with the Body Mass Index of Older Adults: A Cross-Sectional Survey Conducted in Beijing, China" Nutrients 16, no. 2: 289. https://doi.org/10.3390/nu16020289