
The Impact of Weight Bias and Stigma on the 24 h Dietary Recall Process in Adults with Overweight and Obesity: A Pilot Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
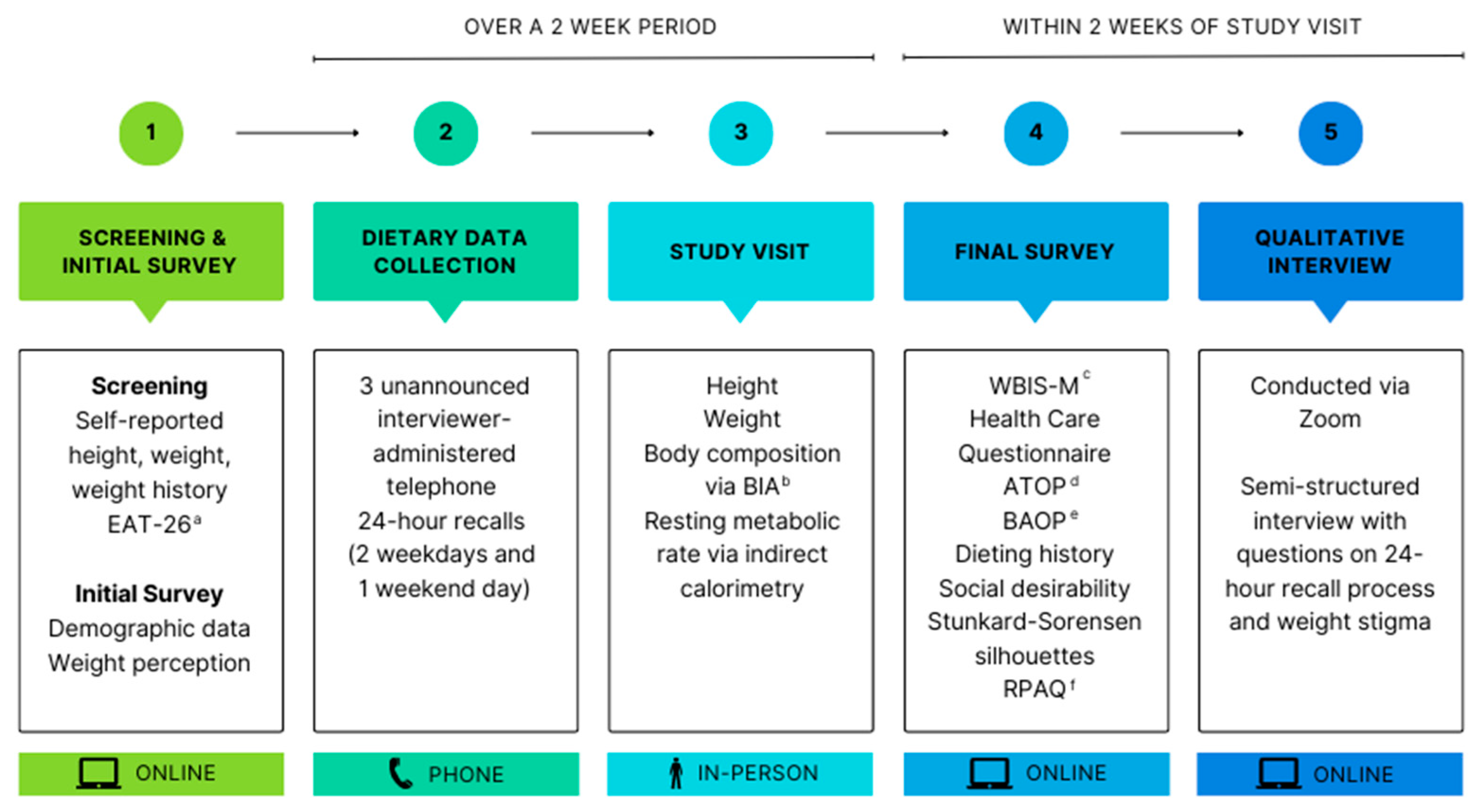
2.1. Research Design
2.2. Participants
2.3. Screening and Eligibility Criteria
2.4. Dietary Intake Assessment
2.5. Study Visit
2.6. Survey Measures
2.7. Qualitative Interview
2.8. Data Analysis
3. Results
“So, it made me want to make behavioral changes. But I think it was still difficult to do, just because it was such a busy time, work-wise and in my life. So um, and it’s yeah, I just I think it made behavioral changes for like, the next day, but not long term, cause it was like, I noticed it, made a quick change, but then I remembered how crazy life was, and like, why I didn’t have time to cook the day before, and then I was back to ordering out.”
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rubino, F.; Puhl, R.M.; Cummings, D.E.; Eckel, R.H.; Ryan, D.H.; Mechanick, J.I.; Nadglowski, J.; Ramos Salas, X.; Schauer, P.R.; Twenefour, D.; et al. Joint International Consensus Statement for Ending Stigma of Obesity. Nat. Med. 2020, 26, 485–497. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-K.; Berry, D.C. Impact of Weight Stigma on Physiological and Psychological Health Outcomes for Overweight and Obese Adults: A Systematic Review. J. Adv. Nurs. 2018, 74, 1030–1042. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.; Suh, Y. Health Consequences of Weight Stigma: Implications for Obesity Prevention and Treatment. Curr. Obes. Rep. 2015, 4, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Pearl, R.L. Weight Bias and Stigma: Public Health Implications and Structural Solutions. Soc. Issues Policy Rev. 2018, 12, 146–182. [Google Scholar] [CrossRef]
- Schvey, N.A.; Marwitz, S.E.; Mi, S.J.; Galescu, O.A.; Broadney, M.M.; Young-Hyman, D.; Brady, S.M.; Reynolds, J.C.; Tanofsky-Kraff, M.; Yanovski, S.Z.; et al. Weight-Based Teasing Is Associated with Gain in BMI and Fat Mass among Children and Adolescents at-Risk for Obesity: A Longitudinal Study. Pediatr. Obes. 2019, 14, e12538. [Google Scholar] [CrossRef] [PubMed]
- Phelan, S.; Burgess, D.; Yeazel, M.; Hellerstedt, W.; Griffin, J.; van Ryn, M. Impact of Weight Bias and Stigma on Quality of Care and Outcomes for Patients with Obesity. Obes. Rev. 2015, 16, 319–326. [Google Scholar] [CrossRef]
- Ryan, L.; Coyne, R.; Heary, C.; Birney, S.; Crotty, M.; Dunne, R.; Conlan, O.; Walsh, J.C. Weight Stigma Experienced by Patients with Obesity in Healthcare Settings: A Qualitative Evidence Synthesis. Obes. Rev. 2023, 24, e13606. [Google Scholar] [CrossRef]
- Durso, L.E.; Latner, J.D. Understanding Self-Directed Stigma: Development of the Weight Bias Internalization Scale. Obesity 2008, 16 (Suppl. S2), S80–S86. [Google Scholar] [CrossRef]
- Pearl, R.L.; Puhl, R.M. Weight Bias Internalization and Health: A Systematic Review. Obes. Rev. 2018, 19, 1141–1163. [Google Scholar] [CrossRef]
- Hunger, J.M.; Dodd, D.R.; Smith, A.R. Weight Discrimination, Anticipated Weight Stigma, and Disordered Eating. Eat. Behav. 2020, 37, 101383. [Google Scholar] [CrossRef]
- Hunger, J.M.; Major, B.; Blodorn, A.; Miller, C.T. Weighed Down by Stigma: How Weight-Based Social Identity Threat Contributes to Weight Gain and Poor Health. Soc. Personal. Psychol. Compass 2015, 9, 255–268. [Google Scholar] [CrossRef] [PubMed]
- Burrows, T.L.; Ho, Y.Y.; Rollo, M.E.; Collins, C.E. Validity of Dietary Assessment Methods When Compared to the Method of Doubly Labeled Water: A Systematic Review in Adults. Front. Endocrinol. 2019, 10, 850. [Google Scholar] [CrossRef] [PubMed]
- Ravelli, M.N.; Schoeller, D.A. Traditional Self-Reported Dietary Instruments Are Prone to Inaccuracies and New Approaches Are Needed. Front. Nutr. 2020, 7, 90. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.M.; Haslam, R.L.; Burrows, T.L.; Duncanson, K.R.; Ashton, L.M.; Rollo, M.E.; Shrewsbury, V.A.; Schumacher, T.L.; Collins, C.E. Issues in Measuring and Interpreting Diet and Its Contribution to Obesity. Curr. Obes. Rep. 2019, 8, 53–65. [Google Scholar] [CrossRef] [PubMed]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method Reduces Bias in the Collection of Energy Intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Wehling, H.; Lusher, J. People with a Body Mass Index ≥30 Under-Report Their Dietary Intake: A Systematic Review. J. Health Psychol. 2019, 24, 2042–2059. [Google Scholar] [CrossRef]
- Hales, C.M.; Fryar, C.D.; Carroll, M.D.; Freedman, D.S.; Ogden, C.L. Trends in Obesity and Severe Obesity Prevalence in US Youth and Adults by Sex and Age, 2007–2008 to 2015–2016. JAMA 2018, 319, 1723–1725. [Google Scholar] [CrossRef]
- Lissner, L. Measuring Food Intake in Studies of Obesity. Public Health Nutr. 2002, 5, 889–892. [Google Scholar] [CrossRef]
- Taren, D.; Tobar, M.; Hill, A.; Howell, W.; Shisslak, C.; Bell, I.; Ritenbaugh, C. The Association of Energy Intake Bias with Psychological Scores of Women. Eur. J. Clin. Nutr. 1999, 53, 570–578. [Google Scholar] [CrossRef]
- Horner, N.K.; Patterson, R.E.; Neuhouser, M.L.; Lampe, J.W.; Beresford, S.A.; Prentice, R.L. Participant Characteristics Associated with Errors in Self-Reported Energy Intake from the Women’s Health Initiative Food-Frequency Questionnaire. Am. J. Clin. Nutr. 2002, 76, 766–773. [Google Scholar] [CrossRef]
- Novotny, J.A.; Rumpler, W.V.; Riddick, H.; Hebert, J.R.; Rhodes, D.; Judd, J.T.; Baer, D.J.; McDowell, M.; Briefel, R. Personality Characteristics as Predictors of Underreporting of Energy Intake on 24-Hour Dietary Recall Interviews. J. Am. Diet. Assoc. 2003, 103, 1146–1151. [Google Scholar] [CrossRef]
- Tooze, J.A.; Subar, A.F.; Thompson, F.E.; Troiano, R.; Schatzkin, A.; Kipnis, V. Psychosocial Predictors of Energy Underreporting in a Large Doubly Labeled Water Study. Am. J. Clin. Nutr. 2004, 79, 795–804. [Google Scholar] [CrossRef]
- Briefel, R.R.; Sempos, C.T.; Mcdowell, M.A.; Chien, S.; Alaimo, K. Dietary Methods Research in the Third National Health and Nutrition Examination Survey: Underreporting of Energy Intake. Am. J. Clin. Nutr. 1997, 65, 1203S–1209S. [Google Scholar] [CrossRef]
- Lafay, L.; Basdevant, A.; Charles, M.-A.; Vray, M.; Balkau, B.; Borys, J.-M.; EschweÁge, E.; Romon, M. Determinants and Nature of Dietary Underreporting in a Free-Living Population: The Fleurbaix Laventie Ville Sante (FLVS) Study. Int. J. Obes. 1997, 21, 567–573. [Google Scholar] [CrossRef]
- Crawley, H.; Summerbell, C. Feeding Frequency and BMI among Teenagers Aged 16–17 Years. Int. J. Obes. 1997, 21, 159–161. [Google Scholar] [CrossRef]
- Johansson, L.; Solvoll, K.; Bjørneboe, G.E.; Drevon, C.A. Under-and Overreporting of Energy Intake Related to Weight Status and Lifestyle in a Nationwide Sample. Am. J. Clin. Nutr. 1998, 68, 266–274. [Google Scholar] [CrossRef]
- Lof, M.; Forsum, E. Validation of Energy Intake by Dietary Recall against Different Methods to Assess Energy Expenditure. J. Hum. Nutr. Diet. 2004, 17, 471–480. [Google Scholar] [CrossRef]
- Rennie, K.L.; Siervo, M.; Jebb, S.A. Can Self-Reported Dieting and Dietary Restraint Identify Underreporters of Energy Intake in Dietary Surveys? J. Am. Diet. Assoc. 2006, 106, 1667–1672. [Google Scholar] [CrossRef]
- Tyrovolas, S.; Koyanagi, A.; Stickley, A.; Haro, J.M. Weight Perception, Satisfaction, Control, and Low Energy Dietary Reporting in the US Adult Population: Results from the National Health and Nutrition Examination Survey 2007–2012. J. Acad. Nutr. Diet. 2016, 116, 579–589. [Google Scholar] [CrossRef]
- Burke, L.E.; Wang, J.; Sevick, M.A. Self-Monitoring in Weight Loss: A Systematic Review of the Literature. J. Am. Diet. Assoc. 2011, 111, 92–102. [Google Scholar] [CrossRef]
- Whitton, C.; Healy, J.D.; Dhaliwal, S.S.; Shoneye, C.; Harray, A.J.; Mullan, B.A.; McVeigh, J.A.; Boushey, C.J.; Kerr, D.A. Demographic and Psychosocial Correlates of Measurement Error and Reactivity Bias in a Four-Day Image-Based Mobile Food Record among Adults with Overweight and Obesity. Br. J. Nutr. 2022, 129, 725–736. [Google Scholar] [CrossRef] [PubMed]
- Friedman, K.E.; Ashmore, J.A.; Applegate, K.L. Recent Experiences of Weight-Based Stigmatization in a Weight Loss Surgery Population: Psychological and Behavioral Correlates. Obesity 2008, 16 (Suppl. S2), S69–S74. [Google Scholar] [CrossRef]
- Farrow, C.V.; Tarrant, M. Weight-Based Discrimination, Body Dissatisfaction and Emotional Eating: The Role of Perceived Social Consensus. Psychol. Health 2009, 24, 1021–1034. [Google Scholar] [CrossRef] [PubMed]
- Pearl, R.L.; Puhl, R.M.; Himmelstein, M.S.; Pinto, A.M.; Foster, G.D. Weight Stigma and Weight-Related Health: Associations of Self-Report Measures Among Adults in Weight Management. Ann. Behav. Med. 2020, 54, 904–914. [Google Scholar] [CrossRef]
- Puhl, R.M.; Heuer, C.A. The Stigma of Obesity: A Review and Update. Obesity 2009, 17, 941–964. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.M.; Himmelstein, M.S.; Quinn, D.M. Internalizing Weight Stigma: Prevalence and Sociodemographic Considerations in US Adults. Obesity 2018, 26, 167–175. [Google Scholar] [CrossRef] [PubMed]
- QuestionPro Inc. QuestionPro. Available online: www.questionpro.com (accessed on 1 March 2022).
- Garner, D.M.; Olmsted, M.P.; Bohr, Y.; Garfinkel, P.E. The Eating Attitudes Test: Psychometric Features and Clinical Correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, T.P.; Hull, S.G.; McNutt, S.; Mittl, B.; Islam, N.; Guenther, P.M.; Thompson, F.E.; Potischman, N.A.; Subar, A.F. Challenges in Converting an Interviewer-Administered Food Probe Database to Self-Administration in the National Cancer Institute Automated Self-Administered 24-Hour Recall (ASA24). J. Food Compos. Anal. 2009, 22, S48–S51. [Google Scholar] [CrossRef]
- Nutrition Coordinating Center. Nutrition Data System for Research 2021; Nutrition Coordinating Center: Minneapolis, MN, USA, 2021. [Google Scholar]
- Haugen, H.A.; Chan, L.-N.; Li, F. Indirect Calorimetry: A Practical Guide for Clinicians. Nutr. Clin. Pract. 2007, 22, 377–388. [Google Scholar] [CrossRef]
- Fullmer, S.; Benson-Davies, S.; Earthman, C.P.; Frankenfield, D.C.; Gradwell, E.; Lee, P.S.P.; Piemonte, T.; Trabulsi, J. Evidence Analysis Library Review of Best Practices for Performing Indirect Calorimetry in Healthy and Non–Critically Ill Individuals. J. Acad. Nutr. Diet. 2015, 115, 1417–1446.e2. [Google Scholar] [CrossRef]
- Irving, C.J.; Eggett, D.L.; Fullmer, S. Comparing Steady State to Time Interval and Non-Steady State Measurements of Resting Metabolic Rate. Nutr. Clin. Pr. 2017, 32, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Pearl, R.L.; Puhl, R.M. Measuring Internalized Weight Attitudes across Body Weight Categories: Validation of the Modified Weight Bias Internalization Scale. Body Image 2014, 11, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Wadden, T.A.; Anderson, D.A.; Foster, G.D.; Bennett, A.; Steinberg, C.; Sarwer, D.B. Obese Women’s Perceptions of Their Physicians’ Weight Management Attitudes and Practices. Arch. Fam. Med. 2000, 9, 854–860. [Google Scholar] [CrossRef] [PubMed]
- Allison, D.B.; Basile, V.C.; Yuker, H.E. The Measurement of Attitudes toward and Beliefs about Obese Persons. Int. J. Eat. Disord. 1991, 10, 599–607. [Google Scholar] [CrossRef]
- Lacroix, E.; Alberga, A.; Russell-Mathew, S.; McLaren, L.; von Ranson, K. Weight Bias: A Systematic Review of Characteristics and Psychometric Properties of Self-Report Questionnaires. Obes. Facts 2017, 10, 223–237. [Google Scholar] [CrossRef]
- Puhl, R.M. What Words Should We Use to Talk about Weight? A Systematic Review of Quantitative and Qualitative Studies Examining Preferences for Weight-Related Terminology. Obes. Rev. 2020, 21, e13008. [Google Scholar] [CrossRef] [PubMed]
- Kyle, T.K.; Puhl, R.M. Putting People First in Obesity: Obesity Biology and Integrated Physiology. Obesity 2014, 22, 1211. [Google Scholar] [CrossRef]
- Witt, A.A.; Katterman, S.N.; Lowe, M.R. Assessing the Three Types of Dieting in the Three-Factor Model of Dieting. The Dieting and Weight History Questionnaire. Appetite 2013, 63, 24–30. [Google Scholar] [CrossRef]
- Crowne, D.P.; Marlowe, D. A New Scale of Social Desirability Independent of Psychopathology. J. Consult. Psychol. 1960, 24, 349–354. [Google Scholar] [CrossRef]
- Stunkard, A.J.; Sørensen, T.; Schulsinger, F. Use of the Danish Adoption Register for the Study of Obesity and Thinness. Res. Publ. Assoc. Res. Nerv. Ment. Dis. 1983, 60, 115–120. [Google Scholar]
- Thompson, J.K.; Altabe, M.N. Psychometric Qualities of the Figure Rating Scale. Int. J. Eat. Disord. 1991, 10, 615–619. [Google Scholar] [CrossRef]
- Besson, H.; Brage, S.; Jakes, R.W.; Ekelund, U.; Wareham, N.J. Estimating Physical Activity Energy Expenditure, Sedentary Time, and Physical Activity Intensity by Self-Report in Adults. Am. J. Clin. Nutr. 2010, 91, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Mindell, J. Measuring Physical Activity in Adults Using the Recent Physical Activity Questionnaire (RPAQ). National Diet and Nutrition Survey. 2012. Available online: https://www.gov.wales/sites/default/files/statistics-and-research/2019-05/151209-national-diet-nutrition-survey-rolling-programme-years-2-5-app-v-en.pdf (accessed on 29 June 2022).
- Vuckovic, N.; Ritenbaugh, C.; Taren, D.L.; Tobar, M. A Qualitative Study of Participants’ Experiences with Dietary Assessment. J. Am. Diet. Assoc. 2000, 100, 1023–1028. [Google Scholar] [CrossRef] [PubMed]
- Zoom Video Communications, Inc. Zoom 2022. Available online: https://explore.zoom.us/en/about/ (accessed on 1 March 2022).
- Hopkins, M.; Michalowska, J.; Whybrow, S.; Horgan, G.W.; Stubbs, R.J. Identification of Psychological Correlates of Dietary Mis-Reporting under Laboratory and Free-Living Environments. Br. J. Nutr. 2020, 126, 264–275. [Google Scholar] [CrossRef] [PubMed]
- Lissner, L.; Troiano, R.P.; Midthune, D.; Heitmann, B.L.; Kipnis, V.; Subar, A.F.; Potischman, N. OPEN about Obesity: Recovery Biomarkers, Dietary Reporting Errors and BMI. Int. J. Obes. 2007, 31, 956–961. [Google Scholar] [CrossRef] [PubMed]
- Waterworth, S.P.; Kerr, C.J.; McManus, C.J.; Costello, R.; Sandercock, G.R.H. Obese Individuals Do Not Underreport Dietary Intake to a Greater Extent than Nonobese Individuals When Data Are Allometrically-Scaled. Am. J. Hum. Biol. 2022, 34, e23743. [Google Scholar] [CrossRef] [PubMed]
- Blodorn, A.; Major, B.; Hunger, J.; Miller, C. Unpacking the Psychological Weight of Weight Stigma: A Rejection-Expectation Pathway. J. Exp. Soc. Psychol. 2016, 63, 69–76. [Google Scholar] [CrossRef]
- Kagawa, M.; Hills, A.P. Preoccupation with Body Weight and Under-Reporting of Energy Intake in Female Japanese Nutrition Students. Nutrients 2020, 12, 830. [Google Scholar] [CrossRef]
- Kanellakis, S.; Sidiropoulou, S.; Apostolidou, E.; Skoufas, E.; Bountouvi, E.; Prelorentzou, T.; Manios, Y. Association of Dietary Intake Underreporting with Body Image Perception. Clin. Nutr. Open Sci. 2021, 40, 30–37. [Google Scholar] [CrossRef]
- Weinberger, N.-A.; Kersting, A.; Riedel-Heller, S.G.; Luck-Sikorski, C. Body Dissatisfaction in Individuals with Obesity Compared to Normal-Weight Individuals: A Systematic Review and Meta-Analysis. Obes. Facts 2017, 9, 424–441. [Google Scholar] [CrossRef]
- Lessard, L.M.; Puhl, R.M.; Himmelstein, M.S.; Pearl, R.L.; Foster, G.D. Eating and Exercise-Related Correlates of Weight Stigma: A Multinational Investigation. Obesity 2021, 29, 966–970. [Google Scholar] [CrossRef] [PubMed]
- Pearl, R.L.; Puhl, R.M.; Brownell, K.D. Positive Media Portrayals of Obese Persons: Impact on Attitudes and Image Preferences. Health Psychol. 2012, 31, 821–829. [Google Scholar] [CrossRef] [PubMed]
- Howes, E.M.; Harden, S.M.; Cox, H.K.; Hedrick, V.E. Communicating About Weight in Dietetics Practice: Recommendations for Reduction of Weight Bias and Stigma. J. Acad. Nutr. Diet. 2021, 121, 1674. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.M.; Andreyeva, T.; Brownell, K.D. Perceptions of Weight Discrimination: Prevalence and Comparison to Race and Gender Discrimination in America. Int. J. Obes. 2008, 32, 992–1000. [Google Scholar] [CrossRef]
- Neuhouser, M.L.; Di, C.; Tinker, L.F.; Thomson, C.; Sternfeld, B.; Mossavar-Rahmani, Y.; Stefanick, M.L.; Sims, S.; Curb, J.D.; Lamonte, M.; et al. Physical Activity Assessment: Biomarkers and Self-Report of Activity-Related Energy Expenditure in the WHI. Am. J. Epidemiol. 2013, 177, 576–585. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall (n = 39) | % | Overweight (n = 20) | % | Obesity (n = 19) | % |
|---|---|---|---|---|---|---|
| Sex | ||||||
| Male | 6 | 15.4 | 3 | 15.0 | 3 | 15.8 |
| Female | 33 | 84.6 | 17 | 85.0 | 16 | 84.2 |
| Gender identity | ||||||
| Man | 7 | 17.9 | 3 | 15.0 | 4 | 21.1 |
| Woman | 32 | 82.1 | 17 | 85.0 | 15 | 78.9 |
| Age (y) mean (SD) | 43.3 (15.0) | 38.8 (15.1) | 48.1 (13.8) | |||
| Educational attainment | ||||||
| High school | 8 | 20.5 | 2 | 10.0 | 6 | 31.6 |
| Associate’s degree | 4 | 10.3 | 3 | 15.0 | 1 | 5.3 |
| Bachelor’s degree | 11 | 28.2 | 7 | 35.0 | 4 | 21.1 |
| Master’s degree | 11 | 28.2 | 4 | 20.0 | 7 | 36.8 |
| Doctoral degree | 5 | 12.8 | 4 | 20.0 | 1 | 5.3 |
| Ethnicity | ||||||
| Hispanic/Latino | 2 | 5.1 | 2 | 10.0 | 0 | 0 |
| Not Hispanic/Latino | 37 | 94.9 | 18 | 90.0 | 19 | 100 |
| Race | ||||||
| Asian | 3 | 7.7 | 2 | 10.0 | 1 | 5.3 |
| Black | 1 | 2.6 | 1 | 5.0 | 0 | 0 |
| White | 33 | 84.6 | 15 | 75.0 | 18 | 94.7 |
| More than one race | 2 | 5.1 | 2 | 10.0 | 0 | 0 |
| Body Mass Index (kg/m2) mean (SD) | 31.0 (6.47) | 26.7 (1.61) | 35.5 (6.66) | |||
| Percentage body fat (BIA a) mean (SD) | 37.6 (8.43) | 32.2 (5.93) | 43.3 (6.81) | |||
| Weight Perception | ||||||
| Normal weight | 7 | 17.9 | 7 | 35.0 | 0 | 0 |
| Slightly overweight | 10 | 25.6 | 9 | 45.0 | 1 | 5.3 |
| Overweight | 16 | 41.0 | 4 | 20.0 | 12 | 63.2 |
| Extremely overweight | 6 | 15.4 | 0 | 0 | 6 | 31.6 |
| Overall (n = 39) | Overweight (n = 20) | Obesity (n = 19) | p-Value a | |
|---|---|---|---|---|
| Weight Bias Internalization b | ||||
| Mean (SD) | 3.54 (1.37) | 2.95 (1.48) | 4.20 (0.867) | 0.003 * |
| Missing c (n) | 1 | 0 | 1 | |
| Social Desirability d | ||||
| Mean (SD) | 16.0 (5.23) | 16.1 (6.46) | 15.8 (3.94) | 0.874 |
| Missing (n) | 6 | 4 | 2 | |
| ATOP e | ||||
| Mean (SD) | 67.0 (18.9) | 72.5 (16.7) | 61.8 (20.0) | 0.103 |
| Missing (n) | 6 | 4 | 2 | |
| BAOP f | ||||
| Mean (SD) | 20.9 (7.88) | 22.8 (8.16) | 18.9 (7.27) | 0.134 |
| Missing (n) | 2 | 1 | 1 | |
| Body Dissatisfaction g (Feel—Ideal) | ||||
| Mean (SD) | 2.42 (1.55) | 1.80 (1.47) | 3.11 (1.37) | 0.007 * |
| Missing (n) | 1 | 0 | 1 | |
| Body Dissatisfaction h (Think—Ideal) | ||||
| Mean (SD) | 2.11 (1.16) | 1.55 (1.10) | 2.72 (0.895) | <0.001 * |
| Missing (n) | 1 | 0 | 1 |
| n (%) | n (%) | ||
|---|---|---|---|
| When I lost weight and regained it, health care professionals criticized me for not trying harder. | I feel that I cannot speak freely with health care professionals about my weight. | ||
| Never | 26 (66.7%) | Never | 20 (51.3%) |
| Rarely | 5 (12.8%) | Rarely | 9 (23.1%) |
| Sometimes | 3 (7.7%) | Sometimes | 5 (12.8%) |
| Usually | 2 (5.1%) | Usually | 4 (10.3%) |
| Always | 1 (2.6%) | Always | 0 (0%) |
| Missing | 2 (5.1%) | Missing | 1 (2.6%) |
| Health care professionals have said critical or insulting things to me about my weight. | I feel that health care professionals don’t believe me when I tell them that I don’t eat that much. | ||
| Never | 20 (51.3%) | Never | 22 (56.4%) |
| Rarely | 9 (23.1%) | Rarely | 7 (17.9%) |
| Sometimes | 8 (20.5%) | Sometimes | 5 (12.8%) |
| Usually | 1 (2.6%) | Usually | 3 (7.7%) |
| Always | 0 (0%) | Always | 0 (0%) |
| Missing | 1 (2.6%) | Missing | 2 (5.1%) |
| I have been very upset by comments that health care professionals have made about my weight | I feel that health care professionals don’t treat overweight people as nicely as they do average-weight people. | ||
| Never | 20 (51.3%) | Never | 7 (17.9%) |
| Rarely | 11 (28.2%) | Rarely | 7 (17.9%) |
| Sometimes | 6 (15.4%) | Sometimes | 15 (38.5%) |
| Usually | 1 (2.6%) | Usually | 9 (23.1%) |
| Always | 0 (0%) | Always | 0 (0%) |
| Missing | 1 (2.6%) | Missing | 1 (2.6%) |
| I feel that I have been treated disrespectfully by people in the health care profession because of my weight. | Health care professionals have told me that I need to lose weight without my asking them. | ||
| Never | 26 (66.7%) | Never | 15 (38.5%) |
| Rarely | 6 (15.4%) | Rarely | 7 (17.9%) |
| Sometimes | 4 (10.3%) | Sometimes | 8 (20.5%) |
| Usually | 2 (5.1%) | Usually | 8 (20.5%) |
| Always | 0 (0%) | Always | 0 (0%) |
| Missing | 1 (2.6%) | Missing | 1 (2.6%) |
| Health care professionals have tried to scare me into losing weight by warning me about health risks associated with being overweight. | I feel that most health care professionals don’t understand how difficult it is to be overweight. | ||
| Never | 20 (51.3%) | Never | 7 (17.9%) |
| Rarely | 9 (23.1%) | Rarely | 8 (20.5%) |
| Sometimes | 5 (12.8%) | Sometimes | 8 (20.5%) |
| Usually | 4 (10.3%) | Usually | 13 (33.3%) |
| Always | 0 (0%) | Always | 1 (2.6%) |
| Missing | 1 (2.6%) | Missing | 2 (5.1%) |
| Model | Prediction Variables | R2 | β | Significance (p-Value) |
|---|---|---|---|---|
| 1a | WBIS-M b | 0.02 | −0.22 | 0.18 |
| 1b | WBIS-M | 0.09 | −0.46 | 0.32 |
| 2a | Weight stigma (yes vs. no) c | −0.02 | −0.09 | 0.59 |
| 2b | Weight stigma (yes vs. no) | −0.03 | −0.09 | 0.53 |
| 3a | ATOP d | −0.03 | 0.04 | 0.83 |
| 3b | ATOP | −0.16 | 0.15 | 0.75 |
| 4a | BAOP e | 0.01 | 0.18 | 0.28 |
| 4b | BAOP | −0.10 | 0.23 | 0.68 |
| Code | Description | % of Participants Reporting | Representative Quote |
|---|---|---|---|
| No changes to intake | No reported changes to intake during study period | 74 | “I don’t actually think it changed- like change my behavior. I know I wasn’t eating differently, because of it, I just ate what I wanted to eat, and then I tried to best of my ability actually tell you what it was.”—41-year-old man |
| Social desirability | Guilt about acceptability of food choices; desire to make a favorable impression on interviewer | 69 | “I think- it- the idea of talking to a stranger about what you’ve eaten and not knowing what their reaction is to it, right, having it be, whether it’s over video or over phone, like, what are they thinking of me?”—55-year-old man |
| Awareness | Increased awareness of intake | 67 | “So I think I started to be a little bit more conscious of what I was eating, or just like more aware. I didn’t feel negative about it. I think I just- noticed how much I was not cooking [laughs] um, as I was doing the recalls.” —29-year-old woman |
| Empirical nature of research | Desire for accuracy, justifying accurate reporting due to nature of research | 54 | “But, the science part of it’s like, well, if I didn’t tell you what I was eating, then you wouldn’t know what I was eating, and that would affect the study. Do you know what I mean?” —47-year-old woman |
| Neutral/positive recalls | No negative impact of recalls | 41 | “Um, I did, like during the actual phone call, it was pretty neutral every single time.” —19-year-old woman |
| No judgment | Expectations or perceptions of judgment about food intake during recall | 41 | “I like, didn’t worry about you necessarily judging me because I was like this, like I didn’t feel like you were going to.”—21-year-old woman |
| Dieting | Mention of intentional dieting, tracking, or weight loss program | 26 | “I would say, from a memory perspective, I didn’t find it hard, but I’ve done so many diets where you track foods, so I think I’m pretty cognizant of what I’m putting in.” —46-year-old woman |
| Changes to intake during study | Restricting intake during study period | 15 | “Um. I- well, you know, I definitely decided I wasn’t going to binge eat chips [laughs] if I knew I was going to be talking to you, and then because I didn’t know when I was going to be talking to you, you know, I stayed away from things like that the entire week.”—60-year-old woman |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Howes, E.M.; Parker, M.K.; Misyak, S.A.; DiFeliceantonio, A.G.; Davy, B.M.; Brown, L.E.C.; Hedrick, V.E. The Impact of Weight Bias and Stigma on the 24 h Dietary Recall Process in Adults with Overweight and Obesity: A Pilot Study. Nutrients 2024, 16, 191. https://doi.org/10.3390/nu16020191
Howes EM, Parker MK, Misyak SA, DiFeliceantonio AG, Davy BM, Brown LEC, Hedrick VE. The Impact of Weight Bias and Stigma on the 24 h Dietary Recall Process in Adults with Overweight and Obesity: A Pilot Study. Nutrients. 2024; 16(2):191. https://doi.org/10.3390/nu16020191
Chicago/Turabian StyleHowes, Erica M., Molly K. Parker, Sarah A. Misyak, Alexandra G. DiFeliceantonio, Brenda M. Davy, Letisha Engracia Cardoso Brown, and Valisa E. Hedrick. 2024. "The Impact of Weight Bias and Stigma on the 24 h Dietary Recall Process in Adults with Overweight and Obesity: A Pilot Study" Nutrients 16, no. 2: 191. https://doi.org/10.3390/nu16020191