

Intense Testing and Use of Vitamin D Supplements Leads to Slow Improvement in Vitamin D Adequacy Rates: A Cross-Sectional Analysis of Real-World Data
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
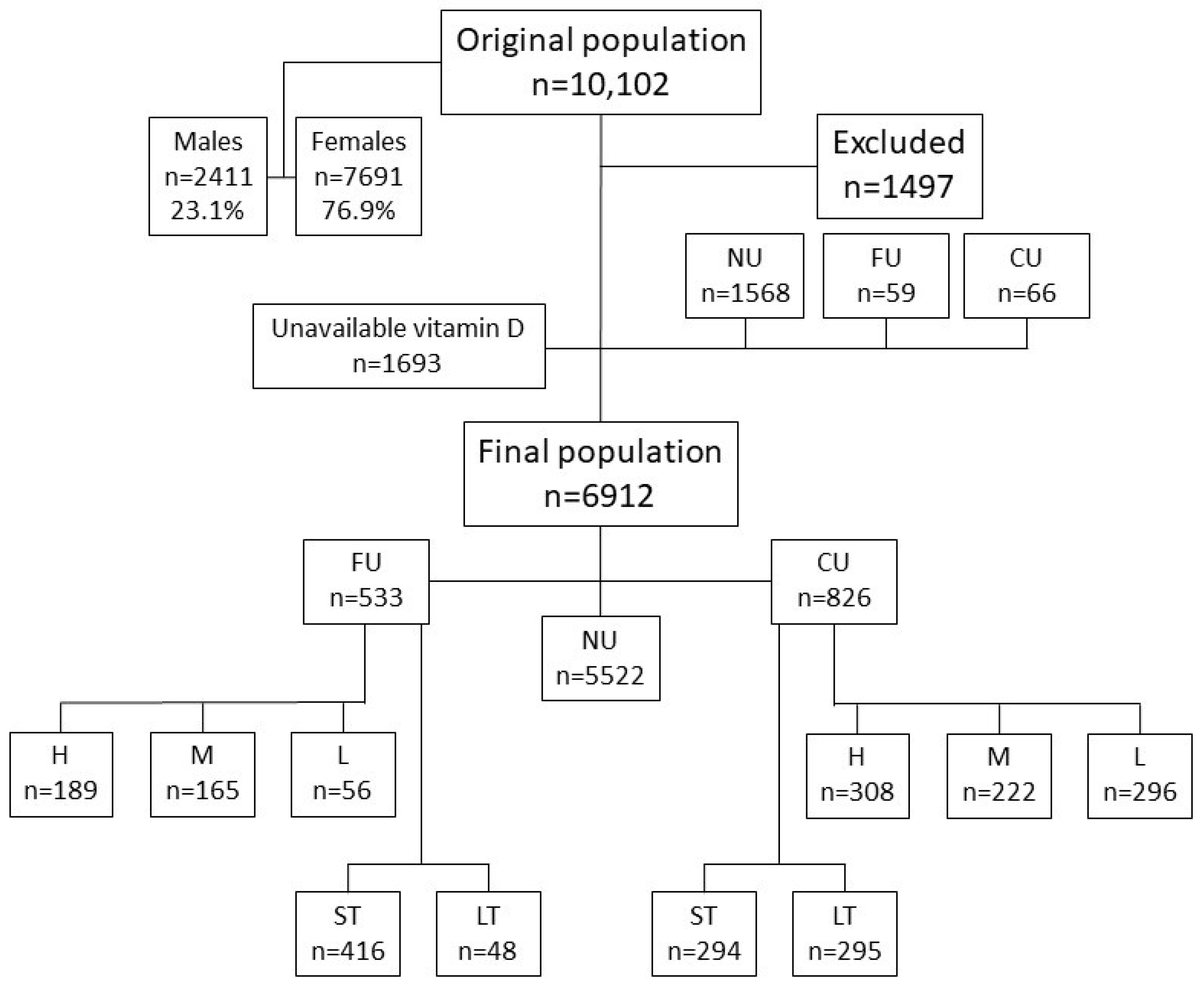
2.1. Inclusion Criteria
2.2. Exclusion Criteria
2.3. Subjects Grouping
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
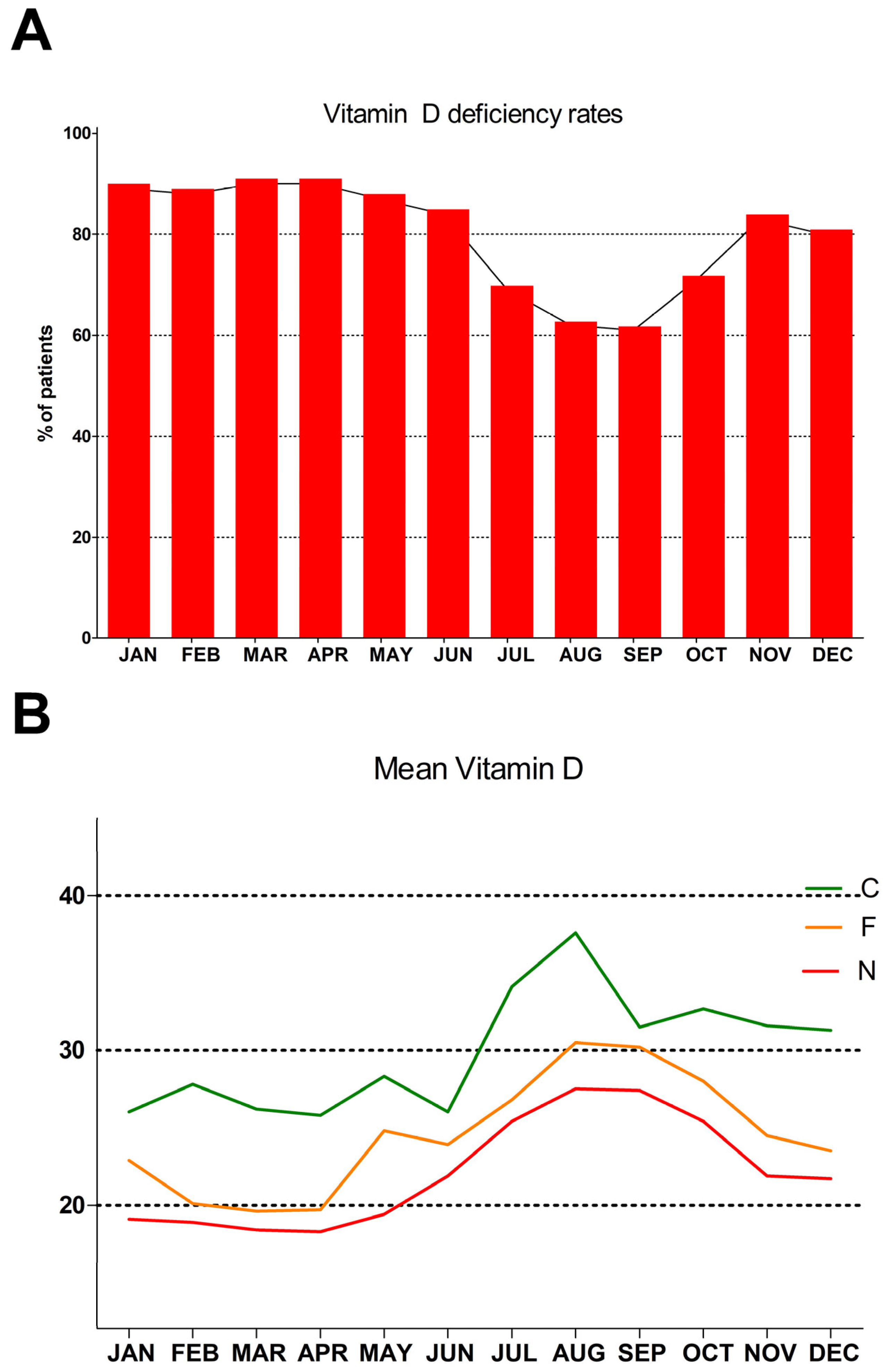
3.1. Monthly Distribution
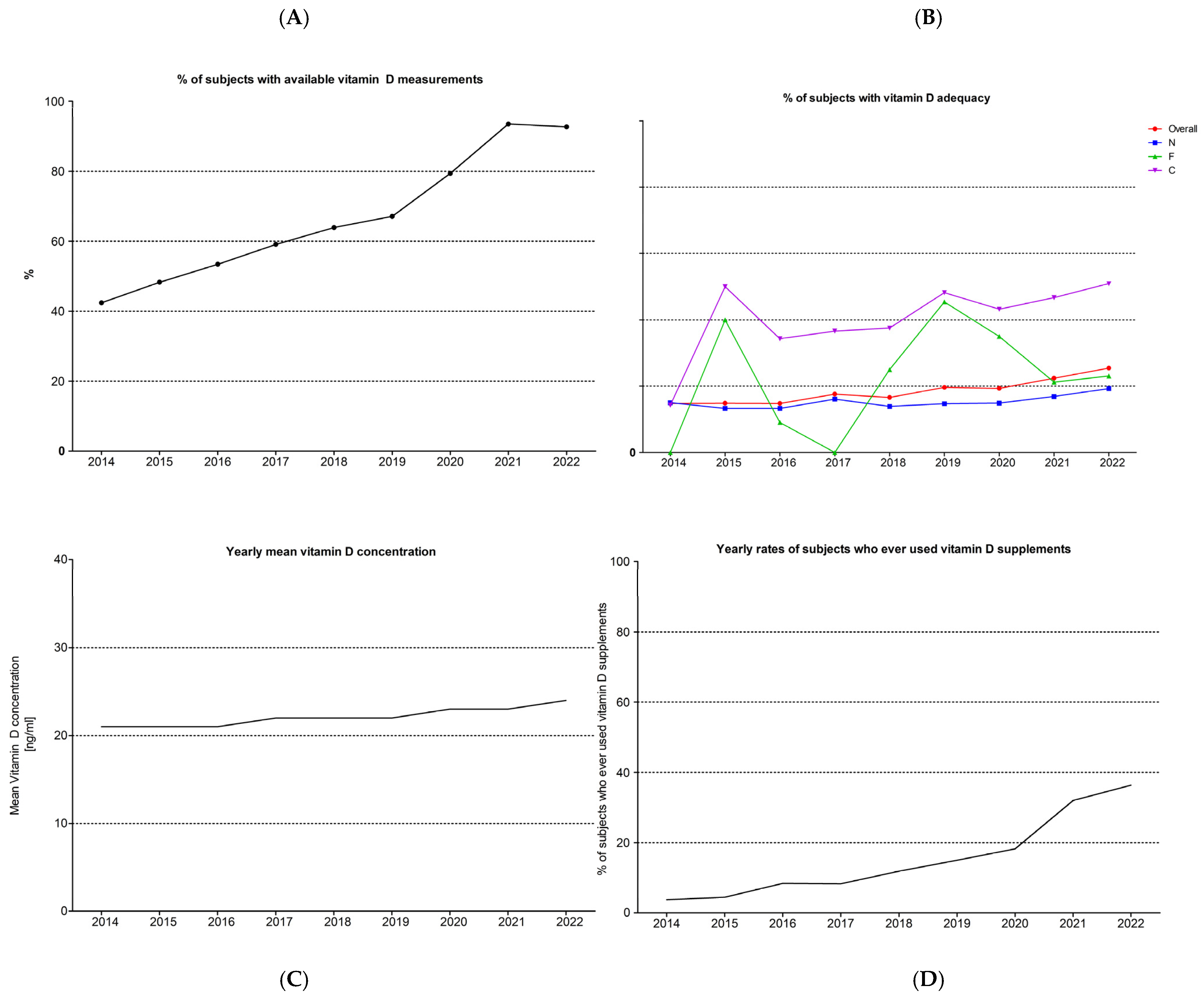
3.2. Vitamin D across the Years
3.3. Supplementation Dose and Duration Effects
3.4. Multivariate Regression Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holick, M.F. The One-Hundred-Year Anniversary of the Discovery of the Sunshine Vitamin D3: Historical, Personal Experience and Evidence-Based Perspectives. Nutrients 2023, 15, 593. [Google Scholar] [CrossRef] [PubMed]
- Papadimitriou, D.T. The Big Vitamin D Mistake. J. Prev. Med. Public Health = Yebang Uihakhoe Chi 2017, 50, 278–281. [Google Scholar] [CrossRef]
- Veugelers, P.J.; Ekwaru, J.P. A statistical error in the estimation of the recommended dietary allowance for vitamin D. Nutrients 2014, 6, 4472–4475. [Google Scholar] [CrossRef]
- Giustina, A.; Adler, R.A.; Binkley, N.; Bollerslev, J.; Bouillon, R.; Dawson-Hughes, B.; Ebeling, P.R.; Feldman, D.; Formenti, A.M.; Lazaretti-Castro, M.; et al. Consensus statement from 2(nd) International Conference on Controversies in Vitamin D. Rev. Endocr. Metab. Disord. 2020, 21, 89–116. [Google Scholar] [CrossRef]
- Roth, D.E.; Abrams, S.A.; Aloia, J.; Bergeron, G.; Bourassa, M.W.; Brown, K.H.; Calvo, M.S.; Cashman, K.D.; Combs, G.; De-Regil, L.M.; et al. Global prevalence and disease burden of vitamin D deficiency: A roadmap for action in low- and middle-income countries. Ann. N. Y. Acad. Sci. 2018, 1430, 44–79. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. Med. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Cesareo, R.; Attanasio, R.; Caputo, M.; Castello, R.; Chiodini, I.; Falchetti, A.; Guglielmi, R.; Papini, E.; Santonati, A.; Scillitani, A.; et al. Italian Association of Clinical Endocrinologists (AME) and Italian Chapter of the American Association of Clinical Endocrinologists (AACE) Position Statement: Clinical Management of Vitamin D Deficiency in Adults. Nutrients 2018, 10, 546. [Google Scholar] [CrossRef]
- Pludowski, P.; Holick, M.F.; Grant, W.B.; Konstantynowicz, J.; Mascarenhas, M.R.; Haq, A.; Povoroznyuk, V.; Balatska, N.; Barbosa, A.P.; Karonova, T.; et al. Vitamin D supplementation guidelines. J. Steroid Biochem. Mol. Biol. 2017, 175, 125–135. [Google Scholar] [CrossRef]
- Pludowski, P.; Takacs, I.; Boyanov, M.; Belaya, Z.; Diaconu, C.C.; Mokhort, T.; Zherdova, N.; Rasa, I.; Payer, J.; Pilz, S. Clinical Practice in the Prevention, Diagnosis and Treatment of Vitamin D Deficiency: A Central and Eastern European Expert Consensus Statement. Nutrients 2022, 14, 1483. [Google Scholar] [CrossRef]
- Watts, N.B.; Camacho, P.M.; Lewiecki, E.M.; Petak, S.M. American Association of Clinical Endocrinologists/American College of Endocrinology Clinical Practice Guidelines for the Diagnosis and Treatment of Postmenopausal Osteoporosis-2020 Update. Endocr. Pract. 2021, 27, 379–380. [Google Scholar] [CrossRef]
- Stepman, H.C.; Vanderroost, A.; Van Uytfanghe, K.; Thienpont, L.M. Candidate reference measurement procedures for serum 25-hydroxyvitamin D3 and 25-hydroxyvitamin D2 by using isotope-dilution liquid chromatography-tandem mass spectrometry. Clin. Chem. 2011, 57, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Bikle, D.D. Vitamin D Assays. Front. Horm. Res. 2018, 50, 14–30. [Google Scholar] [CrossRef] [PubMed]
- Giustina, A.; Bouillon, R.; Dawson-Hughes, B.; Ebeling, P.R.; Lazaretti-Castro, M.; Lips, P.; Marcocci, C.; Bilezikian, J.P. Vitamin D in the older population: A consensus statement. Endocrine 2022, 79, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Sempos, C.T.; Heijboer, A.C.; Bikle, D.D.; Bollerslev, J.; Bouillon, R.; Brannon, P.M.; DeLuca, H.F.; Jones, G.; Munns, C.F.; Bilezikian, J.P.; et al. Vitamin D assays and the definition of hypovitaminosis D: Results from the First International Conference on Controversies in Vitamin D. Br. J. Clin. Pharmacol. 2018, 84, 2194–2207. [Google Scholar] [CrossRef] [PubMed]
- Greenspan, S.L.; Schneider, D.L.; McClung, M.R.; Miller, P.D.; Schnitzer, T.J.; Bonin, R.; Smith, M.E.; Delucca, P.; Gormley, G.J.; Melton, M.E. Alendronate improves bone mineral density in elderly women with osteoporosis residing in long-term care facilities. A randomized, double-blind, placebo-controlled trial. Ann. Intern. Med. 2002, 136, 742–746. [Google Scholar] [CrossRef] [PubMed]
- Cosman, F.; Crittenden, D.B.; Adachi, J.D.; Binkley, N.; Czerwinski, E.; Ferrari, S.; Hofbauer, L.C.; Lau, E.; Lewiecki, E.M.; Miyauchi, A.; et al. Romosozumab Treatment in Postmenopausal Women with Osteoporosis. N. Engl. J. Med. 2016, 375, 1532–1543. [Google Scholar] [CrossRef] [PubMed]
- Papadimitriou, D.; Dermitzaki, E.; Kleanthous, K.; Papadimitriou, A.; Mastorakos, G. MON-541 Successful Treatment of Normocalcemic Hyperparathyroidism in Children. J. Endocr. Soc. 2019, 3, MON-541. [Google Scholar] [CrossRef]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Gordon, D.; Copeland, T.; D’Agostino, D.; et al. Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease. N. Engl. J. Med. 2019, 380, 33–44. [Google Scholar] [CrossRef]
- Matzarakis, A.P.; Katsoulis, V.D. Sunshine duration hours over the Greek region. Theor. Appl. Clim. 2005, 83, 107–120. [Google Scholar] [CrossRef]
- Katrinaki, M.; Kampa, M.; Margioris, A.; Castanas, E.; Malliaraki, N. Vitamin D levels in a large Mediterranean cohort: Reconsidering normal cut-off values. Hormones 2016, 15, 205–223. [Google Scholar] [CrossRef]
- Papapetrou, P.D.; Triantaphyllopoulou, M.; Karga, H.; Zagarelos, P.; Aloumanis, K.; Kostakioti, E.; Vaiopoulos, G. Vitamin D deficiency in the elderly in Athens, Greece. J. Bone Miner. Metab. 2007, 25, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [PubMed]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Berisha, A.T.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef] [PubMed]
- Elliott, T.M.; Gordon, L.G.; Webb, A.; Kift, R.; Foeglein, A.; Neale, R.E. Making the sunshine vitamin—How much sun exposure is needed to maintain 25-hydroxy vitamin D concentration? Photochem. Photobiol. 2023. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, F.; Raftery, T.; van Weele, M.; van Geffen, J.; McNamara, D.; O’Morain, C.; Mahmud, N.; Kelly, D.; Healy, M.; O’Sullivan, M.; et al. Sunshine is an Important Determinant of Vitamin D Status Even Among High-dose Supplement Users: Secondary Analysis of a Randomized Controlled Trial in Crohn’s Disease Patients. Photochem. Photobiol. 2019, 95, 1060–1067. [Google Scholar] [CrossRef] [PubMed]
- Khanna, T.; Shraim, R.; Zarkovic, M.; van Weele, M.; van Geffen, J.; Zgaga, L. Comprehensive Analysis of Seasonal and Geographical Variation in UVB Radiation Relevant for Vitamin D Production in Europe. Nutrients 2022, 14, 5189. [Google Scholar] [CrossRef] [PubMed]
- Vičič, V.; Kukec, A.; Kugler, S.; Geršak, K.; Osredkar, J.; Mikuš, R.P. Assessment of Vitamin D Status in Slovenian Premenopausal and Postmenopausal Women, Using Total, Free, and Bioavailable 25-Hydroxyvitamin D (25(OH)D). Nutrients 2022, 14, 5349. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Stallmann-Jorgensen, I.S.; Pollock, N.K.; Harris, R.A.; Keeton, D.; Huang, Y.; Li, K.; Bassali, R.; Guo, D.-H.; Thomas, J.; et al. A 16-week randomized clinical trial of 2000 international units daily vitamin D3 supplementation in black youth: 25-hydroxyvitamin D, adiposity, and arterial stiffness. J. Clin. Endocrinol. Metab. 2010, 95, 4584–4591. [Google Scholar] [CrossRef]
- Hassanein, M.M.; Huri, H.Z.; Baig, K.; Abduelkarem, A.R. Determinants and Effects of Vitamin D Supplementation in Postmenopausal Women: A Systematic Review. Nutrients 2023, 15, 685. [Google Scholar] [CrossRef]
- Zhao, S.; Gardner, K.; Taylor, W.; Marks, E.; Goodson, N. Vitamin D assessment in primary care: Changing patterns of testing. Lond. J. Prim. Care 2015, 7, 15–22. [Google Scholar] [CrossRef]
- Madden, J.M.; Duffy, M.J.; Zgaga, L.; Bennett, K. Trends in vitamin D supplement use in a general female and breast cancer population in Ireland: A repeated cross-sectional study. PLoS ONE 2018, 13, e0209033. [Google Scholar] [CrossRef] [PubMed]
- Horváth, L.; Mirani, S.; Girgis, M.M.F.; Rácz, S.; Bácskay, I.; Bhattoa, H.P.; Tóth, B.E. Six years’ experience and trends of serum 25-hydroxy vitamin D concentration and the effect of vitamin D3 consumption on these trends. Front. Pharmacol. 2023, 14, 1232285. [Google Scholar] [CrossRef] [PubMed]
- Dissanayake, H.A.; de Silva, N.L.; Sumanatilleke, M.; de Silva, S.D.N.; Gamage, K.K.K.; Dematapitiya, C.; Kuruppu, D.C.; Ranasinghe, P.; Pathmanathan, S.; Katulanda, P. Prognostic and Therapeutic Role of Vitamin D in COVID-19: Systematic Review and Meta-analysis. J. Clin. Endocrinol. Metab. 2021, 107, 1484–1502. [Google Scholar] [CrossRef] [PubMed]
- Pal, R.; Banerjee, M.; Bhadada, S.K.; Shetty, A.J.; Singh, B.; Vyas, A. Vitamin D supplementation and clinical outcomes in COVID-19: A systematic review and meta-analysis. J. Endocrinol. Investig. 2021, 45, 53–68. [Google Scholar] [CrossRef]
- Rawat, D.; Roy, A.; Maitra, S.; Shankar, V.; Khanna, P.; Baidya, D.K. Vitamin D supplementation and COVID-19 treatment: A systematic review and meta-analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102189. [Google Scholar] [CrossRef] [PubMed]
- Papadimitriou, D.T.; Dermitzaki, E.; Christopoulos, P.; Papagianni, M.; Kleanthous, K.; Marakaki, C.; Papadimitriou, A.; Mastorakos, G. Secondary Prevention of Diabetes Type 1 with Oral Calcitriol and Analogs, the PRECAL Study. Children 2023, 10, 862. [Google Scholar] [CrossRef] [PubMed]
- Papadimitriou, D.T.; Vassaras, A.K.; Holick, M.F. Association between population vitamin D status and SARS-CoV-2 related serious-critical illness and deaths: An ecological integrative approach. World J. Virol. 2021, 10, 111–129. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D status: Measurement, interpretation, and clinical application. Ann. Epidemiol. 2009, 19, 73–78. [Google Scholar] [CrossRef]
- Papadimitriou, D.T.; Dermitzaki, E.; Kleanthous, K.; Papadimitriou, A.; Mastorakos, G. Vitamin D revisited: Individualized Vitamin D normal values according to PTH levels; incidence and treatment of Normocalcemic Hyperparathyroidism in children. In European Society of Endocrinology; Bioscientifica Ltd.: North Bristol, UK, 2020; p. EP73. [Google Scholar] [CrossRef]
- Chong, B.; Jayabaskaran, J.; Kong, G.; Chan, Y.H.; Chin, Y.H.; Goh, R.; Kannan, S.; Ng, C.H.; Loong, S.; Kueh, M.T.W.; et al. Trends and predictions of malnutrition and obesity in 204 countries and territories: An analysis of the Global Burden of Disease Study 2019. EClinicalMedicine 2023, 57, 101850. [Google Scholar] [CrossRef]
- Jiang, X.; O’Reilly, P.F.; Aschard, H.; Hsu, Y.-H.; Richards, J.B.; Dupuis, J.; Ingelsson, E.; Karasik, D.; Pilz, S.; Berry, D.; et al. Genome-wide association study in 79,366 European-ancestry individuals informs the genetic architecture of 25-hydroxyvitamin D levels. Nat. Commun. 2018, 9, 260. [Google Scholar] [CrossRef]
- Cheng, J.B.; Levine, M.A.; Bell, N.H.; Mangelsdorf, D.J.; Russell, D.W. Genetic evidence that the human CYP2R1 enzyme is a key vitamin D 25-hydroxylase. Proc. Natl. Acad. Sci. USA 2004, 101, 7711–7715. [Google Scholar] [CrossRef] [PubMed]
- Speeckaert, M.; Huang, G.; Delanghe, J.R.; Taes, Y.E.C. Biological and clinical aspects of the vitamin D binding protein (Gc-globulin) and its polymorphism. Clin. Chim. Acta 2006, 372, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Zhang, F.; Richards, J.B.; Kestenbaum, B.; van Meurs, J.B.; Berry, D.; Kiel, D.P.; Streeten, E.A.; Ohlsson, C.; Koller, D.L.; et al. Common genetic determinants of vitamin D insufficiency: A genome-wide association study. Lancet 2010, 376, 180–188. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Units | Overall | D < 30 | D > 30 | N | F | C | p Value | |
|---|---|---|---|---|---|---|---|---|
| n (%) | - | 6912 (100) | 5319 (76.9) | 1593 (23.1) | 5522 (80.3) | 533 (7.7) | 826 (12.0) | NA |
| Age | Years | 44.0 (16.8) | 44.2 (16.7) c | 47.5 (17.3) | 45.7 a,b (16.4) | 43.4 (15.9) | 53.1 (16.0) | <0.0001 |
| Heart rate | bpm | 79.0 (12.1) | 80.2 c (12.3) | 77.8 (12.2) | 79.0 (12.1) | 78.3 (11.7) | 78.3 (12.0) | 0.85 |
| Systolic BP | mmHg | 125.0 (35.5) | 125.5 (16.1) | 124.8 (14.7) | 124.8 b (27.7) | 125.2 (14.0) | 126.3 (16.9) | 0.24 |
| Diastolic BP | mmHg | 78.5 (10.5) | 78.5 c (10.1) | 77.5 (10.0) | 78.4 (10.6) | 78.1 (9.4) | 79.5 (9.2) | 0.12 |
| Height | meters | 1.67 (0.08) | 1.70 (0.05) | 1.67 (0.10) | 1.66 b (0.09) | 1.64 (0.08) | 1.63 (0.08) | <0.0001 |
| Weight | kg | 77.1 (25.6) | 78.5 c (20.9) | 73.4 (75.6) | 77.7 b (26.5) | 73.7 (17.3) | 71.8 (16.4) | 0.0002 |
| Body mass index | kg/m2 | 27.9 (6.5) | 28.2 c (6.7) | 26.7 (5.8%) | 28.2 (9.6) | 27.4 (6.0) | 27.0 (6.2) | 0.09 |
| Female gender n (%) | - | 5195 (75.2) | 4146 c (78.0) | 1049 (65.9) | 4009 (82.1) a,b | 478 (89.7) | 708 (85.7) | <0.0001 |
| Male gender n (%) | - | 1717 (24.8) | 1173 c (22.0) | 544 (34.1) | 1544 (27.9) a,b | 55 (10.3) | 118 (14.3) |
| CH | CM | CL | FH | FM | FL | |
|---|---|---|---|---|---|---|
| Females | 260 | 186 | 262 | 221 | 193 | 64 |
| Males | 48 | 36 | 34 | 25 | 21 | 9 |
| %Males | 15.6 | 16.2 | 11.5 | 10.2 | 9.8 | 12.3 |
| Total | 308 | 222 | 296 | 246 | 214 | 73 |
| Vitamin D | Overall | N | F | C | p Values |
|---|---|---|---|---|---|
|
Mean ± SD >30/total %>30 ng/mL >20/total %>20 ng/mL |
23.0 ± 9.6 1358/6912 19.6 4121/6912 59.6 | 21.9 ± 9.0 a,b 864/5553 15.6 3089/5553 55.6 | 24.7 ± 8.5 b 123/533 23.2 385/533 72.2 | 29.6 ± 11.6 370/826 44.8 647/826 78.4 | <0.0001 |
| JAN |
20.2 ± 8.3 61/564 10.8 265/564 47.0 |
19.1 ± 7.4 a,b 34/456 7.4 194/456 42.5 | 22.9 ± 7.1 9/47 19.4 31/47 66.0 | 26.0 ± 11.8 17/60 28.3 40/60 66.6 | <0.0001 |
| FEB |
20.1 ± 9.7 69/600 11.5 272/600 45.3 | 18.9 ± 9.5 b 38/487 7.7 194/487 39.8 |
20.1 ± 5.7 b 3/35 7.4 17/35 48.6 | 27.8 ± 9.4 29/78 36.7 61/78 78.2 | <0.0001 |
| MAR |
19.4 ± 8.5 64/672 9.5 294/672 43.8 |
18.4 ± 7.6 b 35/541 6.5 215/541 39.7 | 19.6 ± 7.5 b 4/55 7.1 24/55 43.6 | 26.2 ± 11.7 25/77 32.2 55/77 71.4 | <0.0001 |
| APR |
19.2 ± 8.8 51/508 10.0 216/508 42.5 | 18.3 ± 7.6 b 29/416 6.9 157/416 37.7 | 19.7 ± 7.5 b 3/39 6.7 19/39 48.7 |
25.8 ± 8.9 19/53 36.6 40/53 75.5 | <0.0001 |
| MAY |
21.0 ± 8.1 77/608 12.6 297/608 48.8 |
19.4 ± 7.3 a,b 38/487 7.7 206/487 42.3 |
24.8 ± 7.2 8/36 21.4 28/36 77.8 |
28.3 ± 12.4 31/84 36.9 63/84 75.0 | <0.0001 |
| JUN |
22.5 ± 8.2 101/632 16.0 361/632 57.1 |
21.9 ± 7.7 b 66/522 12.7 300/522 57.5 |
23.9 ± 8.7 8/29 27.3 20/29 69.0 |
26.0 ± 10.1 29/82 34.9 41/62 66.1 | 0.0051 |
| JUL |
26.7 ± 9.5 183/595 30.8 452/595 76.0 |
25.4 ± 8.9 b 121/463 26.1 332/463 71.7 |
26.8 ± 8.4 b 16/57 27.3 47/57 82.4 |
34.1 ± 10.6 47/75 62.1 73/75 97.3 | <0.0001 |
| AUG |
28.7 ± 10.8 125/330 37.8 280/330 84.8 |
27.5 ± 9.6 b 90/259 34.7 213/259 82.2 |
30.5 ± 8.5 17/43 39.4 40/43 93.0 |
37.6 ± 18.0 18/29 63.6 27/29 93.1 | 0.0203 |
| SEP |
28.1 ± 10.0 248/639 38.8 519/639 81.2 |
27.4 ± 9.9 b 182/509 35.7 400/509 78.6 |
30.2 ± 8.7 29/55 52.4 50/55 90.9 |
31.5 ± 10.5 38/75 50.0 69/75 92.0 | 0.0026 |
| OCT |
26.5 ± 9.1 157/542 29.0 415/542 76.6 |
25.4 ± 8.7 b 104/434 24.0 324/434 74.7 |
28.0 ± 5.8 12/36 32.1 32/36 88.9 |
32.7 ± 10.5 42/71 58.2 59/71 83.1 | <0.0001 |
| NOV |
23.2 ± 9.1 114/676 16.9 422/676 62.4 |
21.9 ± 7.8 b 65/548 11.8 323/548 58.9 |
24.5 ± 9.1 b 10/52 20.0 38/52 73.1 |
31.6 ± 12.8 39/75 51.7 61/75 81.3 | <0.0001 |
| DEC |
23.0 ± 9.2 108/546 19.8 328/546 60.1 |
21.7 ± 8.7 b 64/430 14.8 231/430 53.7 |
23.5 ± 5.9 b 6/49 13.2 39/49 79.6 |
31.3 ± 10.3 38/66 56.9 58/66 87.9 | <0.0001 |
| p values | <0.0001 | <0.0001 | <0.0001 | <0.0001 | . |
| 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | |
|---|---|---|---|---|---|---|---|---|---|
| Tests | 316 | 673 | 606 | 694 | 656 | 582 | 672 | 1474 | 1240 |
| Patients | 745 | 1395 | 1134 | 1174 | 1027 | 868 | 846 | 1576 | 1337 |
| %Tests | 42.4 | 48.3 | 53.4 | 59.1 | 63.9 | 67.1 | 79.4 | 93.5 | 92.7 |
| 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | |
|---|---|---|---|---|---|---|---|---|---|
| Current users | 9 | 23 | 45 | 53 | 73 | 73 | 96 | 239 | 214 |
| Former users | 3 | 6 | 5 | 4 | 5 | 14 | 26 | 233 | 237 |
| Never users | 304 | 643 | 555 | 637 | 578 | 495 | 550 | 1002 | 789 |
| Total | 316 | 673 | 606 | 694 | 656 | 582 | 672 | 1474 | 1240 |
| %N | 96.3 | 95.6 | 91.6 | 91.8 | 88.1 | 85.0 | 81.8 | 68.0 | 63.6 |
| >30 | 47/316 | 100/673 | 90/606 | 122/694 | 109/656 | 114/582 | 130/672 | 330/1474 | 316/1240 |
| %>30 | 14.8 | 14.9 | 14.8 | 17.6 | 16.6 | 19.6 | 19.3 | 22.4 | 25.5 |
| Mean ± SD | 22.0 ± 9.8 | 21.5 ± 8.7 | 21.5 ± 9.2 | 22.1 ± 9.1 | 22.0 ± 9.1 | 22.8 ± 10.5 | 23.2 ± 9.5 | 23.8 ± 9.4 b,c,d,e | 24.9 ± 10.3 a,b,c,d,e,f,g |
| N mean ± SD | 21.9 ± 9.8 | 21.2 ± 8.1 | 21.1 ± 8.9 | 21.6 ± 8.9 | 21.4 ± 8.3 | 21.7 ± 10.0 | 21.9 ± 8.6 | 22.4 ± 8.8 | 23.2 ± 9.5 b,c |
| <30 | >30 | Total | %>30 | |
|---|---|---|---|---|
| CHLT | 31 | 66 | 97 | 68.0 |
| CHST | 93 | 97 | 190 | 51.1 |
| CMLT | 57 | 71 | 128 | 55.5 |
| CMST | 60 | 46 | 106 | 43.4 |
| CLLT | 109 | 80 | 189 | 42.3 |
| CLST | 84 | 33 | 117 | 28.2 |
| FHLT | 13 | 7 | 20 | 35.0 |
| FHST | 187 | 64 | 251 | 25.5 |
| FMLT | 12 | 4 | 16 | 25.0 |
| FMST | 131 | 39 | 170 | 22.9 |
| FLLT | 15 | 3 | 18 | 16.7 |
| FLST | 47 | 10 | 57 | 17.5 |
| Total | 839 | 520 | 1359 | 37.2 |
| Coefficient B | Standard Error | z-Value | p Value | Odds Ratio | 95% Conf. Interval | |
|---|---|---|---|---|---|---|
| Male gender | 0.33 | 0.08 | 4.27 | <0.001 | 1.4 | 1.2–1.63 |
| Age | 0.01 | 0.00 | 4.44 | <0.001 | 1.01 | 1.01–1.01 |
| Low-dose supplement | −0.61 | 0.18 | 3.33 | <0.001 | 0.55 | 0.38–0.78 |
| High-dose supplement | 0.18 | 0.15 | 1.19 | 0.23 | 1.2 | 0.89–1.63 |
| Former use | 0.78 | 0.8 | 0.98 | 0.33 | 2.19 | 0.46–10.42 |
| Current use | 1.66 | 0.8 | 2.08 | 0.04 | 5.27 | 1.1–25.3 |
| Long-term treatment | 0.25 | 0.8 | 0.32 | 0.75 | 1.29 | 0.27–6.23 |
| Short-term treatment | −0.54 | 0.79 | 0.68 | 0.5 | 0.58 | 0.12–2.75 |
| BMI | −0.05 | 0.01 | 8.30 | <0.001 | 0.95 | 0.94–0.96 |
| Constant | −0.63 | 0.17 | 3.72 | <0.001 | 0.53 | . |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paparodis, R.D.; Bantouna, D.; Karvounis, E.; Zoupas, I.; Livadas, S.; Angelopoulos, N.; Imam, S.; Papadimitriou, D.T.; Jaume, J.C. Intense Testing and Use of Vitamin D Supplements Leads to Slow Improvement in Vitamin D Adequacy Rates: A Cross-Sectional Analysis of Real-World Data. Nutrients 2024, 16, 111. https://doi.org/10.3390/nu16010111
Paparodis RD, Bantouna D, Karvounis E, Zoupas I, Livadas S, Angelopoulos N, Imam S, Papadimitriou DT, Jaume JC. Intense Testing and Use of Vitamin D Supplements Leads to Slow Improvement in Vitamin D Adequacy Rates: A Cross-Sectional Analysis of Real-World Data. Nutrients. 2024; 16(1):111. https://doi.org/10.3390/nu16010111
Chicago/Turabian StylePaparodis, Rodis D., Dimitra Bantouna, Evangelos Karvounis, Ioannis Zoupas, Sarantis Livadas, Nicholas Angelopoulos, Shahnawaz Imam, Dimitrios T. Papadimitriou, and Juan C. Jaume. 2024. "Intense Testing and Use of Vitamin D Supplements Leads to Slow Improvement in Vitamin D Adequacy Rates: A Cross-Sectional Analysis of Real-World Data" Nutrients 16, no. 1: 111. https://doi.org/10.3390/nu16010111