


Association between Dietary Patterns and Metabolic Syndrome and Modification Effect of Altitude: A Cohort Study of Tibetan Adults in China

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
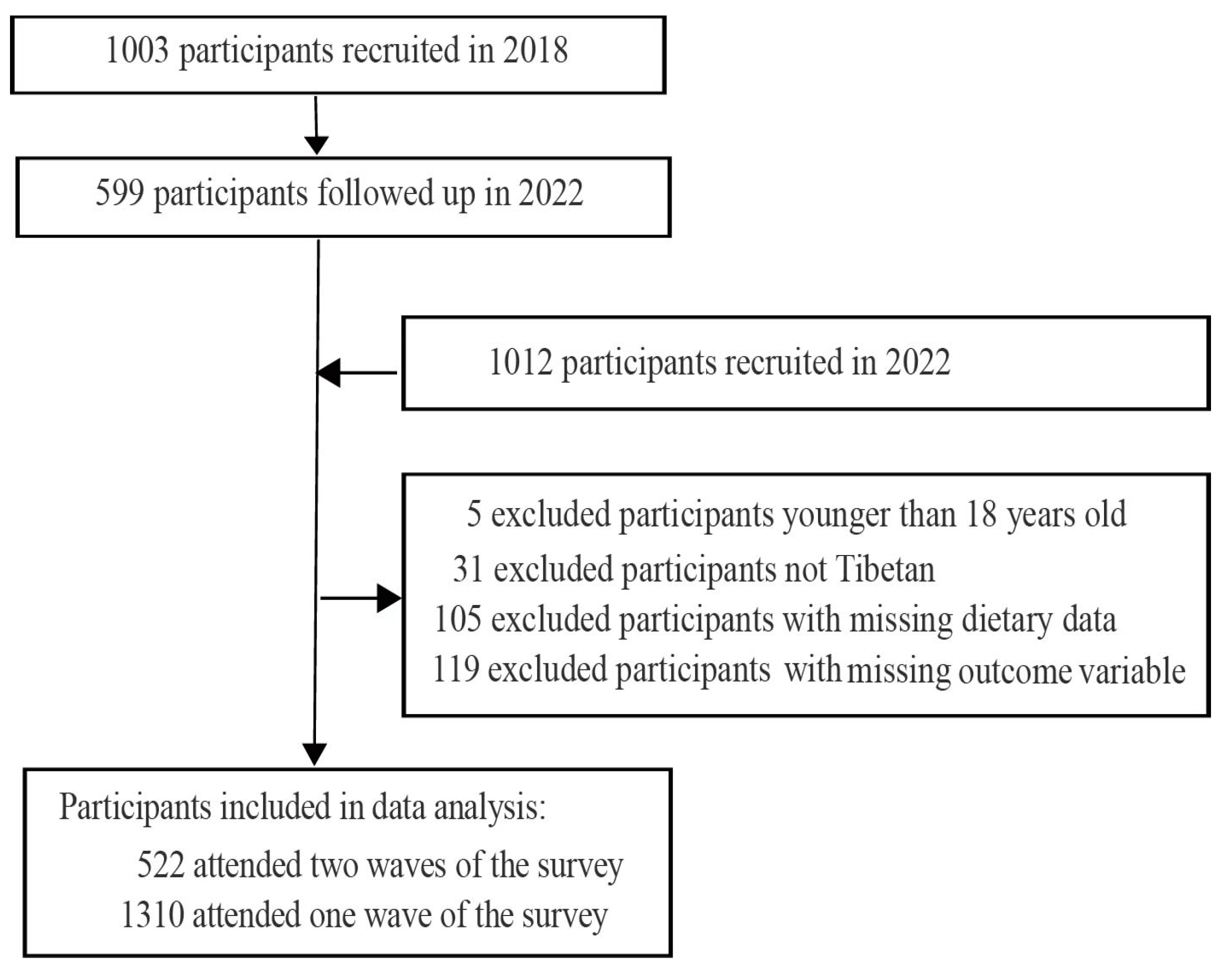
2.1. The Participants and Study Design
2.2. Outcome Variable: The Criteria for MetS and Its Components
2.3. Exposure Variable: Dietary Assessment and Dietary Patterns
2.4. Covariates
2.5. Statistical Analyses
3. Results
3.1. Metabolic Syndrome and Dietary Patterns
3.2. Characteristics of the Participants among Different Dietary Patterns
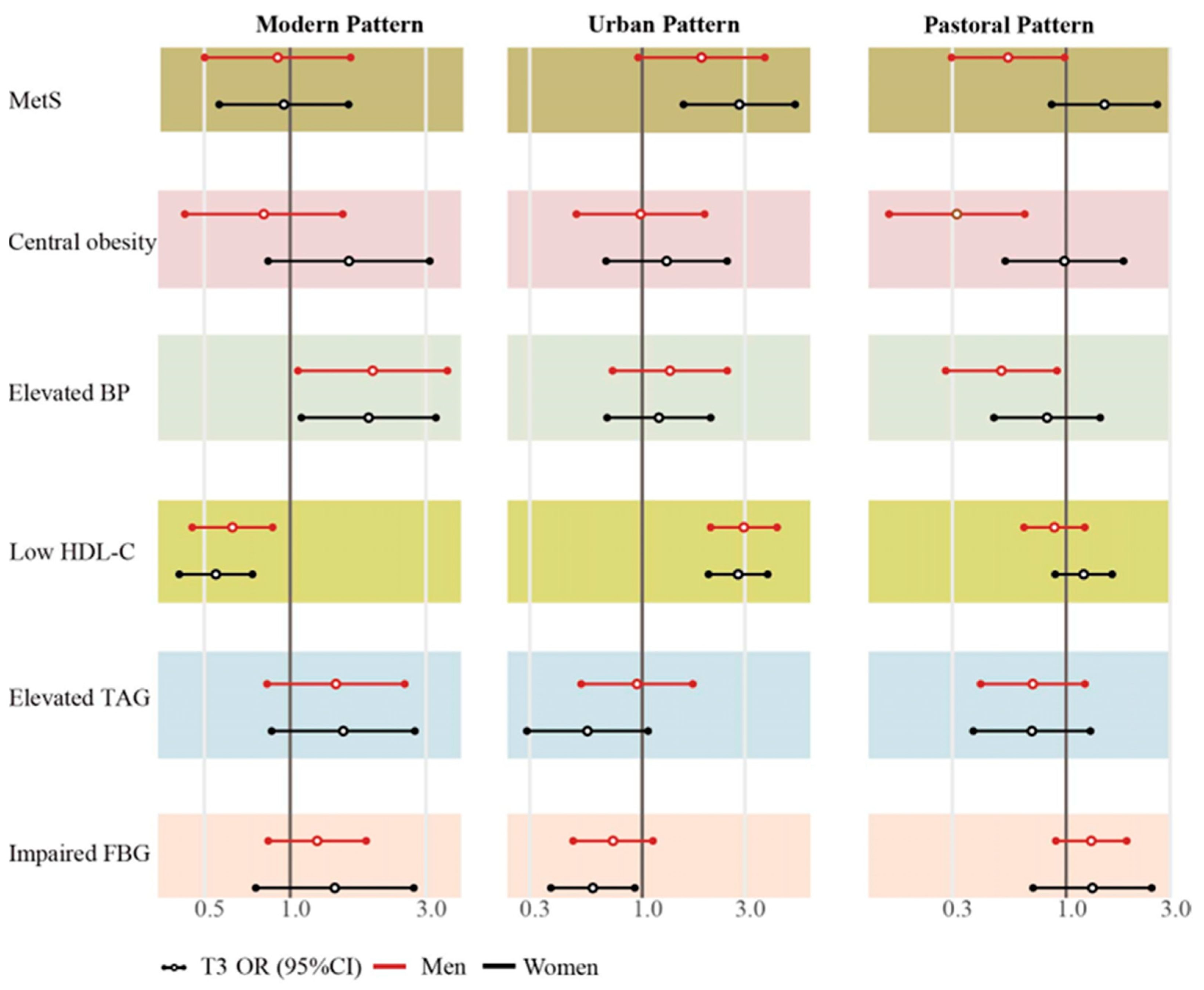
3.3. Prospective Associations among Dietary Patterns Tertile Scores with MetS and Its Components
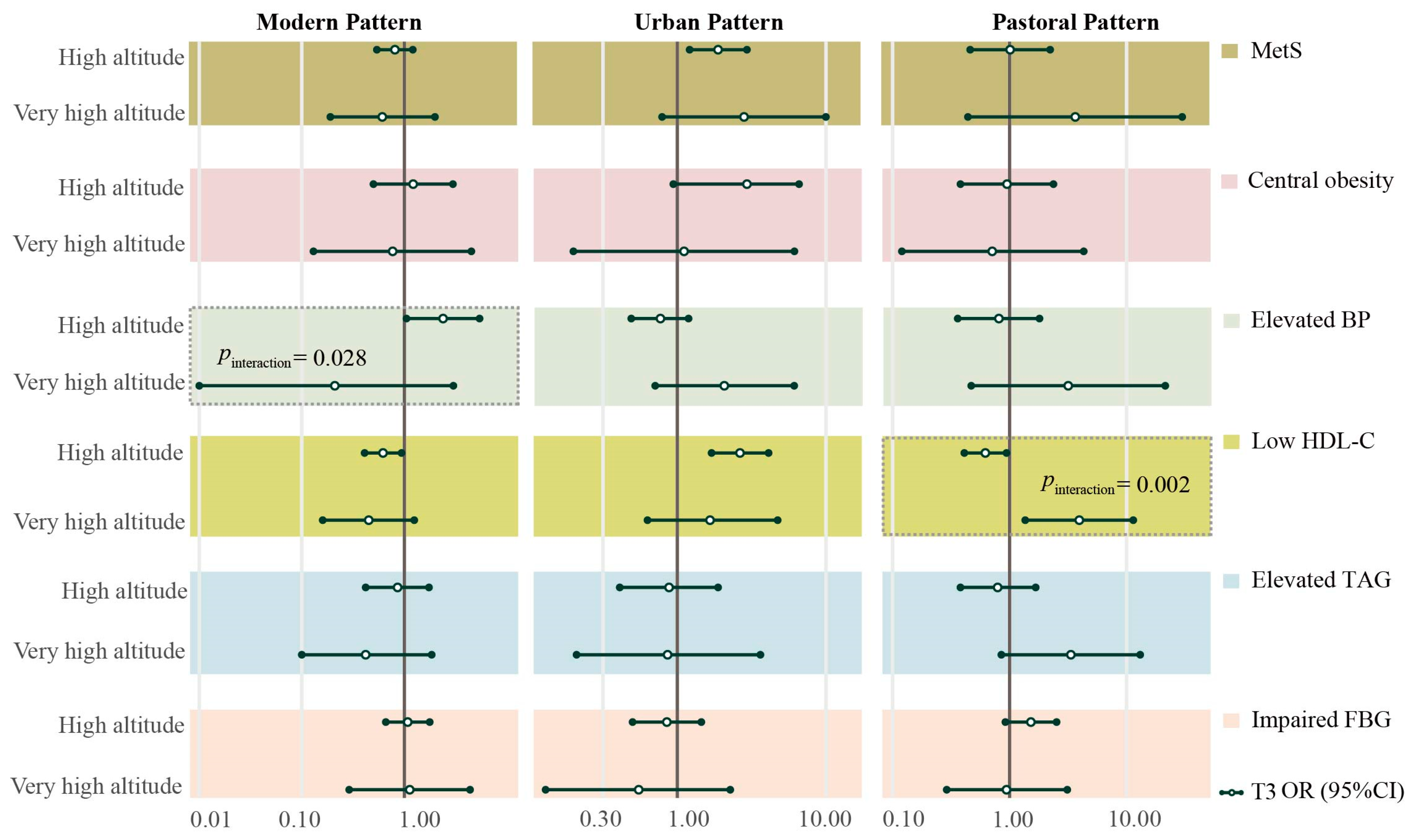
3.4. The Effect of Dietary Patterns Was Modified by Altitude
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef]
- Scholze, J.; Alegria, E.; Ferri, C.; Langham, S.; Stevens, W.; Jeffries, D.; Uhl-Hochgraeber, K. Epidemiological and Economic Burden of Metabolic Syndrome and Its Consequences in Patients with Hypertension in Germany, Spain and Italy; a Prevalence-Based Model. BMC Public Health 2010, 10, 529. [Google Scholar] [CrossRef] [PubMed]
- Bishehsari, F.; Voigt, R.M.; Keshavarzian, A. Circadian Rhythms and the Gut Microbiota: From the Metabolic Syndrome to Cancer. Nat. Rev. Endocrinol. 2020, 16, 731–739. [Google Scholar] [CrossRef] [PubMed]
- Yao, F.; Bo, Y.; Zhao, L.; Li, Y.; Ju, L.; Fang, H.; Piao, W.; Yu, D.; Lao, X. Prevalence and Influencing Factors of Metabolic Syndrome among Adults in China from 2015 to 2017. Nutrients 2021, 13, 4475. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhao, L.; Gao, L.; Pan, A.; Xue, H. Health Policy and Public Health Implications of Obesity in China. Lancet Diabetes Endocrinol. 2021, 9, 446–461. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Peng, W.; Zhao, Z.; Zhang, M.; Shi, Z.; Song, Z.; Zhang, X.; Li, C.; Huang, Z.; Sun, X.; et al. Prevalence and Treatment of Diabetes in China, 2013–2018. JAMA 2021, 326, 2498–2506. [Google Scholar] [CrossRef]
- Li, R.; Li, W.; Lun, Z.; Zhang, H.; Sun, Z.; Kanu, J.S.; Qiu, S.; Cheng, Y.; Liu, Y. Prevalence of Metabolic Syndrome in Mainland China: A Meta-Analysis of Published Studies. BMC Public Health 2016, 16, 296. [Google Scholar] [CrossRef]
- Qin, X.; Qiu, L.; Tang, G.; Tsoi, M.-F.; Xu, T.; Zhang, L.; Qi, Z.; Zhu, G.; Cheung, B.M.Y. Prevalence of Metabolic Syndrome among Ethnic Groups in China. BMC Public Health 2020, 20, 297. [Google Scholar] [CrossRef]
- Peng, W.; Liu, Y.; Malowany, M.; Chen, H.; Su, X.; Liu, Y. Metabolic Syndrome and Its Relation to Dietary Patterns among a Selected Urbanised and Semi-Urbanised Tibetan Population in Transition from Nomadic to Settled Living Environment. Public Health Nutr. 2021, 24, 984–992. [Google Scholar] [CrossRef]
- Drake, I.; Sonestedt, E.; Ericson, U.; Wallström, P.; Orho-Melander, M. A Western Dietary Pattern Is Prospectively Associated with Cardio-Metabolic Traits and Incidence of the Metabolic Syndrome. Br. J. Nutr. 2018, 119, 1168–1176. [Google Scholar] [CrossRef]
- Hoyas, I.; Leon-Sanz, M. Nutritional Challenges in Metabolic Syndrome. J. Clin. Med. 2019, 8, 1301. [Google Scholar] [CrossRef] [PubMed]
- Castro-Barquero, S.; Ruiz-León, A.M.; Sierra-Pérez, M.; Estruch, R.; Casas, R. Dietary Strategies for Metabolic Syndrome: A Comprehensive Review. Nutrients 2020, 12, 2983. [Google Scholar] [CrossRef] [PubMed]
- Rani, V.; Deep, G.; Singh, R.K.; Palle, K.; Yadav, U.C.S. Oxidative Stress and Metabolic Disorders: Pathogenesis and Therapeutic Strategies. Life Sci. 2016, 148, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Li, X.; Adams, H.; Kubena, K.; Guo, S. Etiology of Metabolic Syndrome and Dietary Intervention. Int. J. Mol. Sci. 2018, 20, 128. [Google Scholar] [CrossRef]
- Pena, E.; El Alam, S.; Siques, P.; Brito, J. Oxidative Stress and Diseases Associated with High-Altitude Exposure. Antioxidants 2022, 11, 267. [Google Scholar] [CrossRef]
- Lopez-Pascual, A.; Bes-Rastrollo, M.; Sayón-Orea, C.; Perez-Cornago, A.; Díaz-Gutiérrez, J.; Pons, J.J.; Martínez-González, M.A.; González-Muniesa, P.; Martínez, J.A. Living at a Geographically Higher Elevation Is Associated with Lower Risk of Metabolic Syndrome: Prospective Analysis of the SUN Cohort. Front. Physiol. 2016, 7, 658. [Google Scholar] [CrossRef]
- Lopez-Pascual, A.; Arévalo, J.; Martínez, J.A.; González-Muniesa, P. Inverse Association Between Metabolic Syndrome and Altitude: A Cross-Sectional Study in an Adult Population of Ecuador. Front. Endocrinol. 2018, 9, 658. [Google Scholar] [CrossRef]
- Xiao, Z.; Sun, X.; Zhaxi, D.; Zhang, F.; Ji, Y.; Cheng, T.; Li, X.; Xu, X. Distinct Nutrient Intake Style in Inhabitants of Ultra-High-Altitude Areas in North of Tibet, China: A Cross-Sectional Study Based on Newly Developed Tibetan Food Frequency Questionnaires. Front. Nutr. 2021, 8, 743896. [Google Scholar] [CrossRef]
- Li, K.; Zhang, Q.; Cai, H.; He, R.; Nima, Q.; Li, Y.; Suolang, D.; Cidan, Z.; Wangqing, P.; Zhao, X.; et al. Association of Tibetan Habitual Food and Metabolic Syndrome Among Tibetan People in China: A Cross-Sectional Study. Front. Nutr. 2022, 9, 888317. [Google Scholar] [CrossRef]
- Li, T.; Tang, X.; Liu, Y.; Li, Y.; He, B. Dietary Patterns and Metabolic Syndrome among Urbanized Tibetans: A Cross-Sectional Study. Environ. Res. 2021, 200, 111354. [Google Scholar] [CrossRef]
- Peng, W.; Wang, Y.X.; Wang, H.J.; Li, K.; Sun, X.M.; Wang, Y.F. The prevalence and associated factors of metabolic syndrome among Tibetan pastoralists in transition from nomadic to settled urban environment. Zhonghua Liu Xing Bing Xue Za Zhi 2022, 43, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.; Liu, Y.; Liu, Y.; Zhao, H.; Chen, H. Major Dietary Patterns and Their Relationship to Obesity among Urbanized Adult Tibetan Pastoralists. Asia Pac. J. Clin. Nutr. 2019, 28, 507–519. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the Metabolic Syndrome. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, A.M.; Greenland, S. Causal Directed Acyclic Graphs. JAMA 2022, 327, 1083–1084. [Google Scholar] [CrossRef]
- Chinese Center for Disease Control and Prevention; Chinese Center for DiseaNational Center for Chronic and Noncommunicable Disease Control and Prevention. China Chronic Disease and Risk Factor Surveillance Report 2018, 3rd ed.; People’s Medical Publishing House: Beijing, China, 2021; ISBN 978-7-117-32099-3. [Google Scholar]
- Wickham, H. Ggplot2. WIREs Comput. Stat. 2011, 3, 180–185. [Google Scholar] [CrossRef]
- Rothman, K.J. No Adjustments Are Needed for Multiple Comparisons. Epidemiology 1990, 1, 43–46. [Google Scholar] [CrossRef]
- Huang, X.; Hu, Y.; Du, L.; Lin, X.; Wu, W.; Fan, L.; Li, L.; Zhong, X.; Gong, Q.; Gao, L.; et al. Metabolic Syndrome in Native Populations Living at High Altitude: A Cross-Sectional Survey in Derong, China. BMJ Open 2020, 10, e032840. [Google Scholar] [CrossRef]
- Yao, S.; Zhou, Y.; Xu, L.; Zhang, Q.; Bao, S.; Feng, H.; Ge, W. Association between Hyperuricemia and Metabolic Syndrome: A Cross-Sectional Study in Tibetan Adults on the Tibetan Plateau. Front. Endocrinol. 2022, 13, 964872. [Google Scholar] [CrossRef]
- Miao, J.; Wu, X. Urbanization, Socioeconomic Status and Health Disparity in China. Health Place 2016, 42, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Peng, W. Nutritional Implications of Tibetan Plateau Resettling and Urbanization Programmes. UNSCN Nutrition 2019, 44, 83–90. [Google Scholar]
- Nardocci, M.; Polsky, J.Y.; Moubarac, J.-C. Consumption of Ultra-Processed Foods Is Associated with Obesity, Diabetes and Hypertension in Canadian Adults. Can J. Public Health 2021, 112, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Zama, N.; Ramdass, K.; Mokgohloa, K. Salty and Savoury Snacks Compliance with 2016 and 2019 Sodium Content Targets—Durban Market, South Africa. Int. J. Environ. Res. Public Health 2022, 19, 14118. [Google Scholar] [CrossRef] [PubMed]
- Tighe, P.; Duthie, G.; Vaughan, N.; Brittenden, J.; Simpson, W.G.; Duthie, S.; Mutch, W.; Wahle, K.; Horgan, G.; Thies, F. Effect of Increased Consumption of Whole-Grain Foods on Blood Pressure and Other Cardiovascular Risk Markers in Healthy Middle-Aged Persons: A Randomized Controlled Trial. Am. J. Clin. Nutr. 2010, 92, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Yuan, Y.; Zheng, M.; Pan, A.; Wang, M.; Zhao, M.; Li, Y.; Yao, S.; Chen, S.; Wu, S.; et al. Association of Age of Onset of Hypertension with Cardiovascular Diseases and Mortality. J. Am. Coll. Cardiol. 2020, 75, 2921–2930. [Google Scholar] [CrossRef]
- Pretorius, B.; Schönfeldt, H.C. Cholesterol, Fatty Acids Profile and the Indices of Atherogenicity and Thrombogenicity of Raw Lamb and Mutton Offal. Food Chem. 2021, 345, 128868. [Google Scholar] [CrossRef]
- Gou, R.; Gou, Y.; Qin, J.; Luo, T.; Gou, Q.; He, K.; Xiao, S.; Li, R.; Li, T.; Xiao, J.; et al. Association of Dietary Intake of Saturated Fatty Acids with Hypertension: 1999–2018 National Health and Nutrition Examination Survey. Front. Nutr. 2022, 9, 1006247. [Google Scholar] [CrossRef]
- Nakamura, H.; Tsujiguchi, H.; Kambayashi, Y.; Hara, A.; Miyagi, S.; Yamada, Y.; Nguyen, T.T.T.; Shimizu, Y.; Hori, D.; Nakamura, H. Relationship between Saturated Fatty Acid Intake and Hypertension and Oxidative Stress. Nutrition 2019, 61, 8–15. [Google Scholar] [CrossRef]
- Mente, A.; Dehghan, M.; Rangarajan, S.; McQueen, M.; Dagenais, G.; Wielgosz, A.; Lear, S.; Li, W.; Chen, H.; Yi, S.; et al. Association of Dietary Nutrients with Blood Lipids and Blood Pressure in 18 Countries: A Cross-Sectional Analysis from the PURE Study. Lancet Diabetes Endocrinol. 2017, 5, 774–787. [Google Scholar] [CrossRef]
- Bergouignan, A.; Momken, I.; Schoeller, D.A.; Simon, C.; Blanc, S. Metabolic Fate of Saturated and Monounsaturated Dietary Fats: The Mediterranean Diet Revisited from Epidemiological Evidence to Cellular Mechanisms. Prog. Lipid Res. 2009, 48, 128–147. [Google Scholar] [CrossRef]
- Kim, Y.; Je, Y. Meat Consumption and Risk of Metabolic Syndrome: Results from the Korean Population and a Meta-Analysis of Observational Studies. Nutrients 2018, 10, 390. [Google Scholar] [CrossRef]
- Huang, L.N.; Wang, H.J.; Wang, Z.H.; Zhang, J.G.; Jia, X.F.; Zhang, B.; Ding, G.Q. Association of Red Meat Usual Intake with Serum Ferritin and the Risk of Metabolic Syndrome in Chinese Adults: A Longitudinal Study from the China Health and Nutrition Survey. Biomed. Environ. Sci. 2020, 33, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Ding, J.; Liang, J.; Zhang, Y. Associations of Whole Grain and Refined Grain Consumption with Metabolic Syndrome. A Meta-Analysis of Observational Studies. Front. Nutr. 2021, 8, 695620. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Zhuang, P.; Zhan, C.; Shen, X.; Jiao, J.; Zhang, Y. Egg and Dietary Cholesterol Consumption and the Prevalence of Metabolic Syndrome: Findings from a Population-Based Nationwide Cohort. J. Acad. Nutr. Diet. 2022, 122, 758–770. [Google Scholar] [CrossRef]
- Siri-Tarino, P.W.; Sun, Q.; Hu, F.B.; Krauss, R.M. Saturated Fatty Acids and Risk of Coronary Heart Disease: Modulation by Replacement Nutrients. Curr. Atheroscler. Rep. 2010, 12, 384–390. [Google Scholar] [CrossRef]
- Obeid, R.; Awwad, H.M.; Rabagny, Y.; Graeber, S.; Herrmann, W.; Geisel, J. Plasma Trimethylamine N-Oxide Concentration Is Associated with Choline, Phospholipids, and Methyl Metabolism. Am. J. Clin. Nutr. 2016, 103, 703–711. [Google Scholar] [CrossRef]
- Moreira, M.A.; Vafaei, A.; da Câmara, S.M.A.; Nascimento, R.A.D.; de Morais, M.D.S.M.; Almeida, M.D.G.; Maciel, Á.C.C. Metabolic Syndrome (MetS) and Associated Factors in Middle-Aged Women: A Cross-Sectional Study in Northeast Brazil. Women Health 2020, 60, 601–617. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.; Li, K.; Yan, A.F.; Shi, Z.; Zhang, J.; Cheskin, L.J.; Hussain, A.; Wang, Y. Prevalence, Management, and Associated Factors of Obesity, Hypertension, and Diabetes in Tibetan Population Compared with China Overall. Int. J. Env. Res. Public Health 2022, 19, 8787. [Google Scholar] [CrossRef]
- Zhang, G.; Junmei, W.; Jinxin, C. Analysis of β-Glucan Content in Barley Cultivars from Different Locations of China. Food Chem. 2002, 79, 251–254. [Google Scholar] [CrossRef]
- Aoe, S.; Ichinose, Y.; Kohyama, N.; Komae, K.; Takahashi, A.; Abe, D.; Yoshioka, T.; Yanagisawa, T. Effects of High β-Glucan Barley on Visceral Fat Obesity in Japanese Individuals: A Randomized, Double-Blind Study. Nutrition 2017, 42, 1–6. [Google Scholar] [CrossRef]
- Aljuraiban, G.S.; Stamler, J.; Chan, Q.; Horn, L.V.; Daviglus, M.L.; Elliott, P.; Oude Griep, L.M. Relations between Dairy Product Intake and Blood Pressure: The INTERnational Study on MAcro/Micronutrients and Blood Pressure. J. Hypertens. 2018, 36, 2049–2058. [Google Scholar] [CrossRef]
- Pradhan, A.D. Sex Differences in the Metabolic Syndrome: Implications for Cardiovascular Health in Women. Clin. Chem. 2014, 60, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Rohrmann, S.; Linseisen, J.; Allenspach, M.; von Eckardstein, A.; Müller, D. Plasma Concentrations of Trimethylamine-N-Oxide Are Directly Associated with Dairy Food Consumption and Low-Grade Inflammation in a German Adult Population. J. Nutr. 2016, 146, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Yoo, W.; Zieba, J.K.; Foegeding, N.J.; Torres, T.P.; Shelton, C.D.; Shealy, N.G.; Byndloss, A.J.; Cevallos, S.A.; Gertz, E.; Tiffany, C.R.; et al. High-Fat Diet-Induced Colonocyte Dysfunction Escalates Microbiota-Derived Trimethylamine N-Oxide. Science 2021, 373, 813–818. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Liu, G.; Yang, J.; Zhu, J.; Wang, Q.; Zhou, Y.; Gu, W.; La, L.; Li, X. Changes in the Gut Microbiota of Rats in High-Altitude Hypoxic Environments. Microbiol. Spectr. 2022, 10, e01626-22. [Google Scholar] [CrossRef] [PubMed]
- Thompson, F.E.; Subar, A.F.; Brown, C.C.; Smith, A.F.; Sharbaugh, C.O.; Jobe, J.B.; Mittl, B.; Gibson, J.T.; Ziegler, R.G. Cognitive Research Enhances Accuracy of Food Frequency Questionnaire Reports: Results of an Experimental Validation Study. J. Am. Diet. Assoc. 2002, 102, 212–225. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Food Groups | Modern Pattern | Urban Pattern | Pastoral Pattern |
|---|---|---|---|
| Factor 1 | Factor 2 | Factor 3 | |
| Pulses | 0.60 | 0.06 | −0.01 |
| Poultry | 0.60 | 0.05 | 0.00 |
| Whole grains | 0.54 | 0.08 | −0.09 |
| Offal | 0.53 | −0.07 | 0.06 |
| Processed meat | 0.51 | 0.10 | −0.06 |
| Fresh fruits | 0.50 | 0.13 | −0.03 |
| Processed vegetables | 0.50 | −0.01 | −0.04 |
| Nut and seeds | 0.43 | 0.20 | 0.08 |
| Pork | 0.39 | 0.14 | −0.15 |
| Sugar-sweetened beverages | 0.39 | 0.27 | −0.04 |
| Salty snacks | 0.32 | 0.24 | 0.05 |
| Dark vegetables | 0.13 | 0.64 | −0.15 |
| Light vegetables | 0.13 | 0.61 | −0.10 |
| Refined grains | −0.12 | 0.55 | −0.00 |
| Tubes and roots | 0.21 | 0.54 | −0.09 |
| Onion and spring onion | 0.14 | 0.49 | −0.15 |
| Beef and mutton | −0.27 | 0.45 | 0.24 |
| Eggs | 0.20 | 0.30 | −0.03 |
| Tibetan cheese | −0.04 | −0.08 | 0.74 |
| Tsamba | −0.01 | −0.21 | 0.71 |
| Butter tea and milk tea | −0.06 | 0.27 | 0.48 |
| Desserts | 0.21 | 0.22 | 0.41 |
| Whole-fat dairy | 0.02 | 0.28 | 0.32 |
| Fried foods | 0.29 | 0.02 | 0.16 |
| Seafood | 0.21 | 0.07 | −0.04 |
| Non-caloric drink | −0.08 | 0.24 | −0.28 |
| Variances explained (%) | 11.68 | 9.47 | 7.02 |
| Cumulative variance explained (%) | 11.68 | 21.15 | 28.17 |
| Modern Pattern | Urban Pattern | Pastoral Pattern | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T3 | p | T1 | T2 | T3 | p | T1 | T2 | T3 | p | |
| Survey year (%) | <0.001 | <0.001 | 0.082 | |||||||||
| 2018 | 393 (61.70) | 320 (50.96) | 232 (40.92) | 189 (33.16) | 261 (43.94) | 495 (74.10) | 292 (47.95) | 333 (53.97) | 320 (52.81) | |||
| 2022 | 244 (38.30) | 308 (49.04) | 335 (59.08) | 381 (66.84) | 333 (56.06) | 173 (25.90) | 317 (52.05) | 284 (46.03) | 286 (47.19) | |||
| Age(years) | 46.43 ± 13.51 | 43.25 ± 14.51 | 39.28 ± 14.22 | <0.001 | 46.02 ± 15.34 | 43.37 ± 13.74 | 40.45 ± 13.54 | <0.001 | 39.44 ± 14.90 | 44.92 ± 14.01 | 45.01 ± 13.45 | <0.001 |
| Sex (%) | 0.362 | 0.404 | 0.163 | |||||||||
| Men | 304 (47.72) | 275 (43.79) | 263 (46.38) | 253 (44.39) | 286 (48.15) | 303 (45.36) | 299 (49.10) | 273 (44.25) | 270 (44.55) | |||
| Women | 333 (52.28) | 353 (56.21) | 304 (53.62) | 317 (55.61) | 308 (51.85) | 365 (54.64) | 310 (50.90) | 344 (55.75) | 336 (55.45) | |||
| Marital (%) | <0.001 | 0.105 | <0.001 | |||||||||
| Unmarried/widowed/divorced/separated | 53 (8.33) | 87 (13.88) | 111 (19.61) | 90 (15.82) | 83 (14.02) | 78 (11.68) | 128 (21.12) | 65 (10.53) | 58 (9.57) | |||
| Married | 583 (91.67) | 540 (86.12) | 455 (80.39) | 479 (84.18) | 509 (85.98) | 590 (88.32) | 478 (78.88) | 552 (89.47) | 548 (90.43) | |||
| Education (%) | <0.001 | <0.001 | <0.001 | |||||||||
| No schooling | 513 (81.56) | 454 (72.52) | 353 (62.70) | 456 (80.28) | 436 (74.02) | 428 (64.75) | 355 (58.68) | 479 (78.14) | 486 (81.00) | |||
| <6 years of schooling | 60 (9.54) | 54 (8.63) | 47 (8.35) | 42 (7.39) | 47 (7.98) | 72 (10.89) | 52 (8.60) | 55 (8.97) | 54 (9.00) | |||
| ≥6 years of schooling | 56 (8.90) | 118 (18.85) | 163 (28.95) | 70 (12.32) | 106 (18.00) | 161 (24.36) | 198 (32.73) | 79 (12.89) | 60 (10.00) | |||
| Insurance (%) | <0.001 | <0.001 | 0.006 | |||||||||
| Urban insurance | 234 (37.20) | 213 (34.03) | 277 (49.20) | 127 (22.36) | 180 (30.56) | 417 (63.09) | 271 (44.79) | 237 (38.66) | 216 (36.00) | |||
| Rural/No insurance | 395 (62.80) | 413 (65.97) | 286 (50.80) | 441 (77.64) | 409 (69.44) | 244 (36.91) | 334 (55.21) | 376 (61.34) | 384 (64.00) | |||
| Household income (Yuan, %) | 0.001 | 0.001 | 0.105 | |||||||||
| <20,000 | 165 (26.79) | 160 (26.40) | 93 (17.13) | 139 (25.36) | 138 (24.04) | 141 (21.93) | 137 (23.46) | 130 (21.89) | 151 (25.72) | |||
| 20,000~100,000 | 378 (61.36) | 374 (61.72) | 371 (68.32) | 363 (66.24) | 365 (63.59) | 395 (61.43) | 358 (61.30) | 395 (66.50) | 370 (63.03) | |||
| 100,000~ | 73 (11.85) | 72 (11.88) | 79 (14.55) | 46 (8.39) | 71 (12.37) | 107 (16.64) | 89 (15.24) | 69 (11.62) | 66 (11.24) | |||
| Smoking (%) | 0.073 | <0.001 | <0.001 | |||||||||
| Never | 502 (79.94) | 503 (80.35) | 429 (76.20) | 474 (83.60) | 484 (82.17) | 476 (72.01) | 433 (71.69) | 507 (82.71) | 494 (82.33) | |||
| Former smoker (%) | 41 (6.53) | 40 (6.39) | 28 (4.97) | 34 (6.00) | 29 (4.92) | 46 (6.96) | 45 (7.45) | 26 (4.24) | 38 (6.33) | |||
| Current, <5 cigarettes/d | 19 (3.03) | 12 (1.92) | 22 (3.91) | 10 (1.76) | 14 (2.38) | 29 (4.39) | 29 (4.80) | 14 (2.28) | 10 (1.67) | |||
| Current, ≥5 cigarettes/d | 66 (10.51) | 71 (11.34) | 84 (14.92) | 49 (8.64) | 62 (10.53) | 110 (16.64) | 97 (16.06) | 66 (10.77) | 58 (9.67) | |||
| Alcohol drinking (%) | 0.654 | 0.003 | <0.001 | |||||||||
| Never | 535 (85.06) | 529 (84.50) | 459 (81.53) | 490 (86.27) | 507 (86.08) | 526 (79.58) | 465 (76.86) | 524 (85.48) | 534 (89.00) | |||
| Abstinence | 41 (6.52) | 40 (6.39) | 41 (7.28) | 39 (6.87) | 32 (5.43) | 51 (7.72) | 49 (8.10) | 41 (6.69) | 32 (5.33) | |||
| <40 g/week | 48 (7.63) | 49 (7.83) | 54 (9.59) | 37 (6.51) | 44 (7.47) | 70 (10.59) | 76 (12.56) | 44 (7.18) | 31 (5.17) | |||
| ≥40 g/week | 5 (0.79) | 8 (1.28) | 9 (1.60) | 2 (0.35) | 6 (1.02) | 14 (2.12) | 15 (2.48) | 4 (0.65) | 3 (0.50) | |||
| Physical activity (%) | 0.021 | 0.003 | 0.009 | |||||||||
| Light | 392 (62.42) | 378 (60.48) | 344 (61.21) | 321 (56.51) | 350 (59.63) | 443 (67.12) | 382 (63.25) | 376 (61.44) | 356 (59.43) | |||
| Moderate | 153 (24.36) | 148 (23.68) | 162 (28.83) | 164 (28.87) | 154 (26.24) | 145 (21.97) | 164 (27.15) | 156 (25.49) | 143 (23.87) | |||
| Heavy | 83 (13.22) | 99 (15.84) | 56 (9.96) | 83 (14.61) | 83 (14.14) | 72 (10.91) | 58 (9.60) | 80 (13.07) | 100 (16.69) | |||
| Altitude 2 (%) | 0.050 | 0.003 | <0.001 | |||||||||
| High altitude | 372 (77.50) | 443 (83.58) | 384 (80.67) | 407 (76.07) | 436 (82.58) | 356 (84.16) | 437 (87.75) | 395 (79.64) | 367 (74.59) | |||
| Very high altitude | 108 (22.50) | 87 (16.42) | 92 (19.33) | 128 (23.93) | 92 (17.42) | 67 (15.84) | 61 (12.25) | 101 (20.36) | 125 (25.41) | |||
| Modern Pattern | Urban Pattern | Pastoral Pattern | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T3 | ptrend | T1 | T2 | T3 | ptrend | T1 | T2 | T3 | ptrend | |
| Median | −0.66 | −0.24 | 0.52 | −0.92 | −0.14 | 0.98 | −0.85 | −0.04 | 0.76 | |||
| MetS | ||||||||||||
| Crude | 1.00 | 0.68 (0.46, 1.01) | 0.69 (0.46, 1.03) | 0.102 | 1.00 | 0.97 (0.65, 1.43) | 1.37 (0.92, 2.05) | 0.098 | 1.00 | 1.74 (1.18, 2.59) | 1.30 (0.87, 1.93) | 0.212 |
| Model 1 | 1.00 | 0.83 (0.57, 1.20) | 1.00 (0.69, 1.46) | 0.856 | 1.00 | 1.30 (0.88, 1.92) | 2.68 (1.76, 4.10) | <0.001 | 1.00 | 1.20 (0.82, 1.75) | 0.87 (0.59, 1.28) | 0.442 |
| Model 2 | 1.00 | 0.82 (0.56, 1.20) | 0.94 (0.64, 1.39) | 0.851 | 1.00 | 1.24 (0.83, 1.84) | 2.40 (1.53, 3.76) | <0.001 | 1.00 | 1.20 (0.81, 1.78) | 0.91 (0.61, 1.37) | 0.610 |
| Model 3 | 1.00 | 0.79 (0.51, 1.21) | 0.92 (0.59, 1.44) | 0.861 | 1.00 | 1.20 (0.79, 1.83) | 2.25 (1.36, 3.73) | 0.002 | 1.00 | 1.19 (0.77, 1.83) | 1.02 (0.66, 1.60) | 0.941 |
| Model 4 | 1.00 | 0.69 (0.37, 1.29) | 0.67 (0.35, 1.29) | 0.257 | 1.00 | 1.52 (0.82, 2.80) | 3.42 (1.65, 7.10) | 0.001 | 1.00 | 1.52 (0.82, 2.82) | 1.15 (0.60, 2.22) | 0.710 |
| Central obesity | ||||||||||||
| Crude | 1.00 | 0.68 (0.45, 1.04) | 0.75 (0.50, 1.14) | 0.274 | 1.00 | 0.74 (0.48, 1.12) | 0.54 (0.35, 0.82) | 0.005 | 1.00 | 1.57 (1.03, 2.39) | 1.10 (0.72, 1.68) | 0.662 |
| Model 1 | 1.00 | 0.77 (0.49, 1.21) | 1.12 (0.71, 1.76) | 0.451 | 1.00 | 1.02 (0.65, 1.59) | 1.13 (0.72, 1.77) | 0.584 | 1.00 | 0.89 (0.57, 1.40) | 0.57 (0.36, 0.90) | 0.016 |
| Model 2 | 1.00 | 0.81 (0.52, 1.27) | 1.18 (0.75, 1.87) | 0.359 | 1.00 | 1.03 (0.66, 1.61) | 1.13 (0.70, 1.83) | 0.602 | 1.00 | 0.86 (0.54, 1.35) | 0.57 (0.35, 0.92) | 0.019 |
| Model 3 | 1.00 | 0.73 (0.44, 1.19) | 1.16 (0.70, 1.93) | 0.393 | 1.00 | 0.99 (0.62, 1.57) | 1.40 (0.81, 2.38) | 0.216 | 1.00 | 1.13 (0.69, 1.85) | 0.70 (0.42, 1.16) | 0.150 |
| Model 4 | 1.00 | 0.64 (0.30, 1.36) | 1.26 (0.56, 2.81) | 0.457 | 1.00 | 0.93 (0.45, 1.92) | 1.95 (0.84, 4.51) | 0.111 | 1.00 | 1.19 (0.55, 2.61) | 0.83 (0.37, 1.88) | 0.629 |
| Elevated BP | ||||||||||||
| Crude | 1.00 | 0.84 (0.57, 1.22) | 1.34 (0.92, 1.96) | 0.069 | 1.00 | 0.77 (0.53, 1.11) | 0.79 (0.55, 1.14) | 0.247 | 1.00 | 1.25 (0.87, 1.81) | 1.03 (0.71, 1.50) | 0.870 |
| Model 1 | 1.00 | 1.06 (0.73, 1.55) | 2.20 (1.49, 3.25) | <0.001 | 1.00 | 1.01 (0.70, 1.45) | 1.63 (1.11, 2.38) | 0.008 | 1.00 | 0.81 (0.56, 1.17) | 0.62 (0.43, 0.91) | 0.015 |
| Model 2 | 1.00 | 0.97 (0.66, 1.43) | 1.94 (1.29, 2.90) | 0.001 | 1.00 | 0.91 (0.62, 1.33) | 1.28 (0.85, 1.94) | 0.195 | 1.00 | 0.82 (0.56, 1.22) | 0.64 (0.43, 0.96) | 0.030 |
| Model 3 | 1.00 | 0.95 (0.60, 1.50) | 2.07 (1.27, 3.39) | 0.002 | 1.00 | 0.81 (0.52, 1.25) | 1.08 (0.66, 1.76) | 0.757 | 1.00 | 0.94 (0.59, 1.49) | 0.73 (0.45, 1.18) | 0.197 |
| Model 4 | 1.00 | 0.99 (0.51, 1.92) | 1.66 (0.82, 3.35) | 0.137 | 1.00 | 0.75 (0.40, 1.42) | 0.77 (0.37, 1.58) | 0.483 | 1.00 | 1.06 (0.54, 2.07) | 0.96 (0.48, 1.90) | 0.887 |
| Low HDL-C | ||||||||||||
| Crude | 1.00 | 0.78 (0.64, 0.95) | 0.61 (0.50, 0.75) | <0.001 | 1.00 | 1.28 (1.05, 1.56) | 3.07 (2.50, 3.77) | <0.001 | 1.00 | 1.12 (0.92, 1.37) | 1.04 (0.85, 1.27) | 0.683 |
| Model 1 | 1.00 | 0.77 (0.63, 0.94) | 0.61 (0.49, 0.75) | <0.001 | 1.00 | 1.35 (1.10, 1.66) | 3.41 (2.76, 4.23) | <0.001 | 1.00 | 1.08 (0.89, 1.33) | 1.01 (0.83, 1.23) | 0.947 |
| Model 2 | 1.00 | 0.79 (0.64, 0.98) | 0.58 (0.47, 0.72) | <0.001 | 1.00 | 1.30 (1.05, 1.61) | 2.88 (2.27, 3.64) | <0.001 | 1.00 | 1.15 (0.92, 1.42) | 1.06 (0.86, 1.32) | 0.602 |
| Model 3 | 1.00 | 0.88 (0.70, 1.10) | 0.71 (0.56, 0.90) | 0.005 | 1.00 | 1.31 (1.04, 1.63) | 2.36 (1.83, 3.04) | <0.001 | 1.00 | 1.00 (0.79, 1.26) | 0.97 (0.76, 1.23) | 0.806 |
| Model 4 | 1.00 | 0.82 (0.58, 1.17) | 0.60 (0.41, 0.87) | 0.007 | 1.00 | 1.42 (1.00, 2.01) | 2.47 (1.66, 3.69) | <0.001 | 1.00 | 1.10 (0.76, 1.58) | 0.85 (0.58, 1.23) | 0.358 |
| Elevated TAG | ||||||||||||
| Crude | 1.00 | 0.84 (0.58, 1.22) | 1.14 (0.79, 1.65) | 0.349 | 1.00 | 0.83 (0.57, 1.20) | 0.58 (0.39, 0.86) | 0.007 | 1.00 | 0.93 (0.65, 1.35) | 0.90 (0.62, 1.30) | 0.565 |
| Model 1 | 1.00 | 0.93 (0.63, 1.38) | 1.50 (1.02, 2.22) | 0.021 | 1.00 | 0.92 (0.63, 1.35) | 0.79 (0.53, 1.19) | 0.260 | 1.00 | 0.76 (0.51, 1.12) | 0.72 (0.48, 1.08) | 0.113 |
| Model 2 | 1.00 | 0.94 (0.63, 1.40) | 1.50 (1.00, 2.26) | 0.033 | 1.00 | 0.87 (0.58, 1.28) | 0.73 (0.46, 1.14) | 0.163 | 1.00 | 0.73 (0.48, 1.09) | 0.69 (0.46, 1.05) | 0.088 |
| Model 3 | 1.00 | 0.93 (0.71, 1.22) | 1.19 (0.89, 1.58) | 0.179 | 1.00 | 0.88 (0.68, 1.15) | 0.97 (0.72, 1.30) | 0.821 | 1.00 | 0.83 (0.62, 1.10) | 0.81 (0.61, 1.07) | 0.141 |
| Model 4 | 1.00 | 0.64 (0.31, 1.34) | 0.76 (0.36, 1.60) | 0.533 | 1.00 | 0.72 (0.36, 1.45) | 0.85 (0.38, 1.88) | 0.689 | 1.00 | 0.69 (0.32, 1.48) | 0.95 (0.44, 2.03) | 0.915 |
| Impaired FBG | ||||||||||||
| Crude | 1.00 | 0.88 (0.60, 1.29) | 1.05 (0.71, 1.54) | 0.697 | 1.00 | 0.76 (0.51, 1.13) | 0.32 (0.19, 0.52) | <0.001 | 1.00 | 1.19 (0.82, 1.76) | 1.66 (1.14, 2.43) | 0.008 |
| Model 1 | 1.00 | 0.97 (0.65, 1.46) | 1.43 (0.94, 2.16) | 0.074 | 1.00 | 0.89 (0.59, 1.33) | 0.44 (0.27, 0.73) | 0.001 | 1.00 | 0.95 (0.63, 1.43) | 1.32 (0.88, 1.97) | 0.162 |
| Model 2 | 1.00 | 0.95 (0.63, 1.43) | 1.48 (0.96, 2.29) | 0.054 | 1.00 | 0.95 (0.63, 1.43) | 0.49 (0.29, 0.81) | 0.005 | 1.00 | 1.00 (0.65, 1.52) | 1.38 (0.91, 2.09) | 0.113 |
| Model 3 | 1.00 | 0.94 (0.71, 1.24) | 1.16 (0.87, 1.56) | 0.245 | 1.00 | 0.95 (0.70, 1.23) | 0.74 (0.54, 1.02) | 0.065 | 1.00 | 1.05 (0.78, 1.41) | 1.42 (1.06, 1.90) | 0.015 |
| Model 4 | 1.00 | 1.24 (0.62, 2.47) | 1.18 (0.57, 2.45) | 0.689 | 1.00 | 1.06 (0.55, 2.04) | 0.79 (0.36, 1.73) | 0.564 | 1.00 | 1.30 (0.63, 2.67) | 1.68 (0.80, 3.54) | 0.166 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.; Wang, Y.; Shi, Z.; Zhao, L.; Jian, W.; Li, K.; Xu, R.; Wu, Y.; Xu, F.; Wang, Y.; et al. Association between Dietary Patterns and Metabolic Syndrome and Modification Effect of Altitude: A Cohort Study of Tibetan Adults in China. Nutrients 2023, 15, 2226. https://doi.org/10.3390/nu15092226
Wang H, Wang Y, Shi Z, Zhao L, Jian W, Li K, Xu R, Wu Y, Xu F, Wang Y, et al. Association between Dietary Patterns and Metabolic Syndrome and Modification Effect of Altitude: A Cohort Study of Tibetan Adults in China. Nutrients. 2023; 15(9):2226. https://doi.org/10.3390/nu15092226
Chicago/Turabian StyleWang, Haijing, Yanxiang Wang, Zumin Shi, Lei Zhao, Wenxiu Jian, Ke Li, Ruihua Xu, Yan Wu, Fei Xu, Youfa Wang, and et al. 2023. "Association between Dietary Patterns and Metabolic Syndrome and Modification Effect of Altitude: A Cohort Study of Tibetan Adults in China" Nutrients 15, no. 9: 2226. https://doi.org/10.3390/nu15092226