
Dietary Oncopharmacognosy as a Crosswalk between Precision Oncology and Precision Nutrition

 ,
, {kind=link}
Abstract
:1. Introduction
2. Definitions
3. The Top-Down Approach: Dietary Patterns
4. Bottom-Up: Natural Products from Food
5. From Food Patterns and Their Bioactive Food Components to Precision Oncology
6. A Mechanistic Foundation
6.1. Protein Kinases
6.2. Apoptosis
6.3. Angiogenesis
6.4. Immune Checkpoints
7. Developing the Cross Walk between Precision Oncology and Precision Nutrition
8. Next Steps
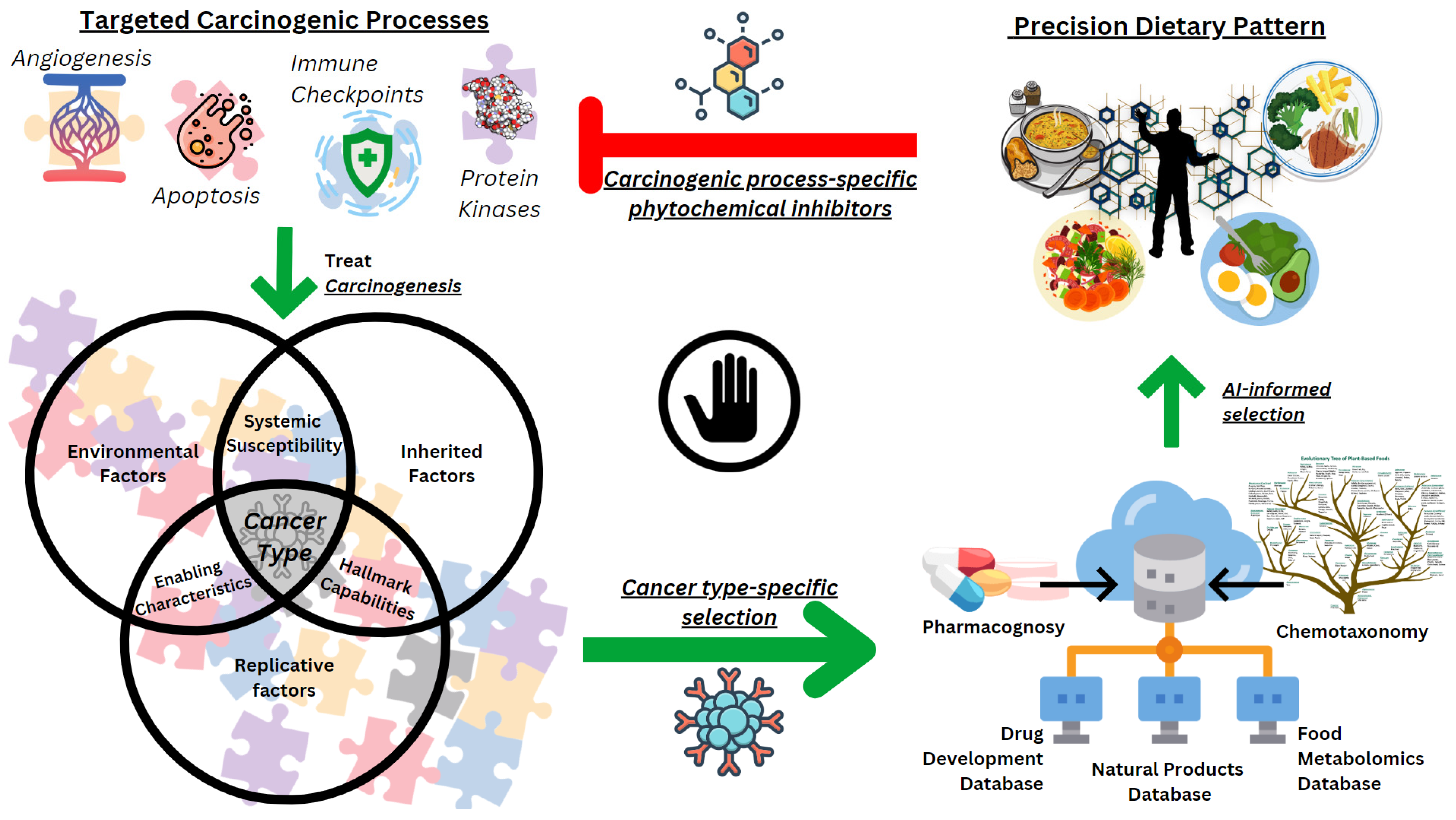
- Identify a specific molecular subtype of cancer. There are many molecular subtypes of cancer for which small-molecule drugs are in use. Serious consideration should be given to investigating cancer subtypes in which multiple cellular processes have been shown to be successfully targeted. This will increase the likelihood that precision food patterns will exert synergistic effects. It would also be beneficial for the selection of molecular cancer subtypes in which a watchful waiting period exists between initial diagnosis and initiation of treatment. Finally, consideration needs to be given to whether it is feasible to monitor the pharmacologic activity of food molecules systemically and on the target tumor cell population of the cancer subtype selected for investigation. Therefore, a particular cancer type in a particular patient provides a list of key identifying molecules, dysregulation of which continuously drives this carcinogenesis, and thus, they are to be targeted specifically in this patient.
- Identify effective small-molecule inhibitors of that cancer and the pharmacokinetic and pharmacodynamic properties associated with successful outcomes. The drug development literature needs to be carefully mined for structure-activity relationships and to ensure that critical data about the pharmacological determinants of successful outcomes are available for examination. Standards for this purpose have been published, and the need to consider potential off-target effects has been emphasized [90,91].
- Identify structural similarities in the identified small-molecule drugs and the natural products that are components of specific foods. The literature is replete with in silico analyses of structure relationships that have led to the identification and development of clinically effective small-molecule inhibitors. This has occurred in the science of pharmacognosy as well as in drug development [92]. These same approaches now need to be applied to the food metabolome: certain postprandial metabolites detected in circulation possess the same or functionally similar biochemical/pharmacological properties as the components of small-molecule drugs found in the previous step; therefore, exposure of tissues to them mimics administration of small-molecule inhibitors of interest, i.e., we are selecting for food metabolites of similar biochemical functionality as the small-molecule inhibitors selected for specific cancer type.
- Design specific food patterns predicted to exert effects on identified targets. Some food metabolites can be found post-consumption in more than one type of food. For instance, in the realm of plant-based food patterns, there is a botanical classification method based on the similarity of phytochemicals found in a plant (chemotaxonomy) which can be utilized to determine the plants of interest providing specific food metabolites with the necessary inhibitory properties. This will allow diversifying the food patterns tailored for a specific patient based on their molecular cancer type, ensuring enough exposure to inhibitory phytochemicals to achieve desired long-term anti-cancer effects. Such precision food patterns that are to be developed must also satisfy guidelines, such as Recommended Dietary Intakes and Dietary Guidelines for Americans, considering the multi-faceted impact of the diet in determining the health status, especially considering the ongoing pandemic of metabolic disorders.
- Assess effects in well-designed Phase I trials. Well-accepted trial designs have been established for the initial evaluation of small-molecule inhibitors that are now being successfully used in the clinic [93]. The trial protocols for precision dietary/food patterns should parallel those designs as food-derived metabolites with anti-cancer properties should be perceived as pharmacological agents based on the fact that they undergo similar kinetics and dynamics in an organism with a targeted effect of interest as any other pharmaceutical drugs (food pharmacology).
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Doll, R.; Peto, R. The Causes of Cancer: Quantitative Estimates of Avoidable Risks of Cancer in the United States Today. J. Natl. Cancer Inst. 1981, 66, 1192–1308. [Google Scholar] [CrossRef]
- Doll, R. Epidemiology of chronic non-infectious disease: Current status and future perspective. Rev. Bras. Epidemiol. 1998, 1, 94–103. [Google Scholar] [CrossRef]
- Milner, J.A. Molecular Targets for Bioactive Food Components. J. Nutr. 2004, 134, 2492S–2498S. [Google Scholar] [CrossRef] [PubMed]
- Vargas, A.J.; Thompson, P.A. Diet and Nutrient Factors in Colorectal Cancer Risk. Nutr. Clin. Pract. 2012, 27, 613–623. [Google Scholar] [CrossRef]
- Steck, S.E.; Murphy, E.A. Dietary patterns and cancer risk. Nat. Rev. Cancer 2020, 20, 125–138. [Google Scholar] [CrossRef] [PubMed]
- Studies linking diet with health must get a whole lot better. Nature 2022, 610, 231. [CrossRef] [PubMed]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K. Body Fatness and Cancer—Viewpoint of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef]
- Sporn, M.B. Carcinogenesis and cancer: Different perspectives on the same disease. Cancer Res. 1991, 51, 6215–6218. [Google Scholar]
- Sporn, M.B.; Suh, N. Chemoprevention: An essential approach to controlling cancer. Nat. Rev. Cancer 2002, 2, 537–543. [Google Scholar] [CrossRef]
- Tokheim, C.J.; Papadopoulos, N.; Kinzler, K.W.; Vogelstein, B.; Karchin, R. Evaluating the evaluation of cancer driver genes. Proc. Natl. Acad. Sci. USA 2016, 113, 14330–14335. [Google Scholar] [CrossRef]
- Smith, M.T.; Guyton, K.Z.; Gibbons, C.F.; Fritz, J.M.; Portier, C.J.; Rusyn, I.; DeMarini, D.M.; Caldwell, J.C.; Kavlock, R.J.; Lambert, P.F.; et al. Key Characteristics of Carcinogens as a Basis for Organizing Data on Mechanisms of Carcinogenesis. Environ. Health Perspect. 2016, 124, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Cho, K.-H. Critical transition and reversion of tumorigenesis. Exp. Mol. Med. 2023, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Tomasetti, C.; Li, L.; Vogelstein, B. Stem cell divisions, somatic mutations, cancer etiology, and cancer prevention. Science 2017, 355, 1330–1334. [Google Scholar] [CrossRef] [PubMed]
- Desaulniers, D.; Vasseur, P.; Jacobs, A.; Aguila, M.C.; Ertych, N.; Jacobs, M.N. Integration of Epigenetic Mechanisms into Non-Genotoxic Carcinogenicity Hazard Assessment: Focus on DNA Methylation and Histone Modifications. Int. J. Mol. Sci. 2021, 22, 969. [Google Scholar] [CrossRef]
- Hanahan, D. Hallmarks of Cancer: New Dimensions. Cancer Discov. 2022, 12, 31–46. [Google Scholar] [CrossRef]
- Choi, J.; Zhang, X.; Li, W.; Houston, M.; Peregrina, K.; Dubin, R.; Ye, K.; Augenlicht, L.H. Dietary Induced Dynamic Plasticity of Intestinal Stem Cells and the Mucosa in Elevating Risk for Tumor Development. bioRxiv 2022. [Google Scholar] [CrossRef]
- Akhoon, N. Precision Medicine: A New Paradigm in Therapeutics. Int. J. Prev. Med. 2021, 12, 12. [Google Scholar] [CrossRef]
- Buckeridge, D.L. Precision, Equity, and Public Health and Epidemiology Informatics—A Scoping Review. Yearb. Med. Inform. 2020, 29, 226–230. [Google Scholar] [CrossRef]
- Schmidt, K.T.; Chau, C.H.; Price, D.K.; Figg, W.D. Precision Oncology Medicine: The Clinical Relevance of Patient-Specific Biomarkers Used to Optimize Cancer Treatment. J. Clin. Pharm. 2016, 56, 1484–1499. [Google Scholar] [CrossRef]
- Carugo, A.; Draetta, G.F. Academic Discovery of Anticancer Drugs: Historic and Future Perspectives. Annu. Rev. Cancer Biol. 2019, 3, 385–408. [Google Scholar] [CrossRef]
- Livingstone, K.M.; Ramos-Lopez, O.; Pérusse, L.; Kato, H.; Ordovas, J.M.; Martínez, J.A. Precision nutrition: A review of current approaches and future endeavors. Trends Food Sci. Technol. 2022, 128, 253–264. [Google Scholar] [CrossRef]
- Thompson, H.J.; Neil, E.S.; McGinley, J.N.; Fitzgerald, V.K.; El Bayoumy, K.; Manni, A. Building a Foundation for Precision Onco-Nutrition: Docosahexaenoic Acid and Breast Cancer. Cancers 2021, 14, 157. [Google Scholar] [CrossRef]
- Council, N.R. Diet, Nutrition, and Cancer; The National Academies Press: Washington, DC, USA, 1982; p. 496. [Google Scholar]
- Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [CrossRef] [PubMed]
- Solans, M.; Chan, D.S.M.; Mitrou, P.; Norat, T.; Romaguera, D. A systematic review and meta-analysis of the 2007 WCRF/AICR score in relation to cancer-related health outcomes. Ann. Oncol. 2020, 31, 352–368. [Google Scholar] [CrossRef] [PubMed]
- Key, T.J.; Bradbury, K.E.; Perez-Cornago, A.; Sinha, R.; Tsilidis, K.K.; Tsugane, S. Diet, nutrition, and cancer risk: What do we know and what is the way forward? BMJ 2020, 368, m511. [Google Scholar] [CrossRef]
- Papadimitriou, N.; Markozannes, G.; Kanellopoulou, A.; Critselis, E.; Alhardan, S.; Karafousia, V.; Kasimis, J.C.; Katsaraki, C.; Papadopoulou, A.; Zografou, M.; et al. An umbrella review of the evidence associating diet and cancer risk at 11 anatomical sites. Nat. Commun. 2021, 12, 4579. [Google Scholar] [CrossRef]
- Tomasetti, C.; Vogelstein, B. Cancer etiology. Variation in cancer risk among tissues can be explained by the number of stem cell divisions. Science 2015, 347, 78–81. [Google Scholar] [CrossRef]
- Alsharairi, N.A. The Effects of Dietary Supplements on Asthma and Lung Cancer Risk in Smokers and Non-Smokers: A Review of the Literature. Nutrients 2019, 11, 725. [Google Scholar] [CrossRef]
- Neuhouser, M.L.; Prentice, R.L.; Tinker, L.F.; Lampe, J.W. Enhancing Capacity for Food and Nutrient Intake Assessment in Population Sciences Research. Annu Rev Public Health 2023, 44, 37–54. [Google Scholar] [CrossRef]
- Lopez-Pentecost, M.; Crane, T.E.; Garcia, D.O.; Kohler, L.N.; Wertheim, B.C.; Hebert, J.R.; Steck, S.E.; Shivappa, N.; Santiago-Torres, M.; Neuhouser, M.L.; et al. Role of dietary patterns and acculturation in cancer risk and mortality among postmenopausal Hispanic women: Results from the Women’s Health Initiative (WHI). Z Gesundh Wiss. 2022, 30, 811–822. [Google Scholar] [CrossRef]
- Liese, A.D.; Wambogo, E.; Lerman, J.L.; Boushey, C.J.; Neuhouser, M.L.; Wang, S.; Harmon, B.E.; Tinker, L.F. Variations in Dietary Patterns Defined by the Healthy Eating Index 2015 and Associations with Mortality: Findings from the Dietary Patterns Methods Project. J. Nutr. 2022, 152, 796–804. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, M.S. Nutrition and cancer: A review of the evidence for an anti-cancer diet. Nutr. J. 2004, 3, 19. [Google Scholar] [CrossRef]
- Zhong, L.; Li, Y.; Xiong, L.; Wang, W.; Wu, M.; Yuan, T.; Yang, W.; Tian, C.; Miao, Z.; Wang, T.; et al. Small molecules in targeted cancer therapy: Advances, challenges, and future perspectives. Signal Transduct. Target. Ther. 2021, 6, 201. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Qian, W.; Sun, X.; Jiang, S. Small-molecule inhibitors, immune checkpoint inhibitors, and more: FDA-approved novel therapeutic drugs for solid tumors from 1991 to 2021. J. Hematol. Oncol. 2022, 15, 143. [Google Scholar] [CrossRef] [PubMed]
- Ayala-Aguilera, C.C.; Valero, T.; Lorente-Macías, Á.; Baillache, D.J.; Croke, S.; Unciti-Broceta, A. Small Molecule Kinase Inhibitor Drugs (1995–2021): Medical Indication, Pharmacology, and Synthesis. J. Med. Chem. 2022, 65, 1047–1131. [Google Scholar] [CrossRef]
- Molinski, T.F. Microscale methodology for structure elucidation of natural products. Curr. Opin. Biotechnol. 2010, 21, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Lescinsky, H.; Afshin, A.; Ashbaugh, C.; Bisignano, C.; Brauer, M.; Ferrara, G.; Hay, S.I.; He, J.; Iannucci, V.; Marczak, L.B.; et al. Health effects associated with consumption of unprocessed red meat: A Burden of Proof study. Nat. Med. 2022, 28, 2075–2082. [Google Scholar] [CrossRef]
- Stanaway, J.D.; Afshin, A.; Ashbaugh, C.; Bisignano, C.; Brauer, M.; Ferrara, G.; Garcia, V.; Haile, D.; Hay, S.I.; He, J.; et al. Health effects associated with vegetable consumption: A Burden of Proof study. Nat. Med. 2022, 28, 2066–2074. [Google Scholar] [CrossRef]
- Wink, M. Evolution of secondary metabolites from an ecological and molecular phylogenetic perspective. Phytochemistry 2003, 64, 3–19. [Google Scholar] [CrossRef]
- Wink, M. Plant secondary metabolism: Diversity, function and its evolution. Nat. Prod. Commun. 2008, 3, 1205–1216. [Google Scholar] [CrossRef]
- Klurfeld, D.M.; Davis, C.D.; Karp, R.W.; Allen-Vercoe, E.; Chang, E.B.; Chassaing, B.; Fahey, G.C., Jr.; Hamaker, B.R.; Holscher, H.D.; Lampe, J.W.; et al. Considerations for best practices in studies of fiber or other dietary components and the intestinal microbiome. Am. J. Physiol. Endocrinol. Metab. 2018, 315, E1087–E1097. [Google Scholar] [CrossRef] [PubMed]
- Baier, A.; Szyszka, R. Compounds from Natural Sources as Protein Kinase Inhibitors. Biomolecules 2020, 10, 1546. [Google Scholar] [CrossRef] [PubMed]
- Roskoski, R. Properties of FDA-approved small molecule protein kinase inhibitors: A 2023 update. Pharmacol. Res. 2023, 187, 106552. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Z.; Vong, C.T.; Chen, F.; Tan, H.; Zhang, C.; Wang, N.; Cui, L.; Wang, Y.; Feng, Y. Immunomodulatory potential of natural products from herbal medicines as immune checkpoints inhibitors: Helping to fight against cancer via multiple targets. Med. Res. Rev. 2022, 42, 1246–1279. [Google Scholar] [CrossRef] [PubMed]
- Juliano, R.L. Addressing cancer signal transduction pathways with antisense and siRNA oligonucleotides. NAR Cancer 2020, 2, zcaa025. [Google Scholar] [CrossRef]
- Hager, K.; Cudhea, F.P.; Wong, J.B.; Berkowitz, S.A.; Downer, S.; Lauren, B.N.; Mozaffarian, D. Association of National Expansion of Insurance Coverage of Medically Tailored Meals with Estimated Hospitalizations and Health Care Expenditures in the US. JAMA Netw. Open 2022, 5, e2236898. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Tan, T.C.; Horiuchi, K.M.; Laws, D.; Ambrosy, A.P.; Lee, K.K.; Maring, B.L.; Joy, J.; Couch, C.; Hepfer, P.; et al. Effect of Medically Tailored Meals on Clinical Outcomes in Recently Hospitalized High-Risk Adults. Med. Care 2022, 60, 750–758. [Google Scholar] [CrossRef]
- Hoelder, S.; Clarke, P.A.; Workman, P. Discovery of small molecule cancer drugs: Successes, challenges and opportunities. Mol. Oncol. 2012, 6, 155–176. [Google Scholar] [CrossRef]
- Liu, G.H.; Chen, T.; Zhang, X.; Ma, X.L.; Shi, H.S. Small molecule inhibitors targeting the cancers. MedComm 2022, 3, e181. [Google Scholar] [CrossRef]
- Sun, G.; Rong, D.; Li, Z.; Sun, G.; Wu, F.; Li, X.; Cao, H.; Cheng, Y.; Tang, W.; Sun, Y. Role of Small Molecule Targeted Compounds in Cancer: Progress, Opportunities, and Challenges. Front. Cell Dev. Biol. 2021, 9, 694363. [Google Scholar] [CrossRef]
- Alganem, K.; Hamoud, A.-R.; Creeden, J.F.; Henkel, N.D.; Imami, A.S.; Joyce, A.W.; Ryan, V.W.G.; Rethman, J.B.; Shukla, R.; O’Donovan, S.M.; et al. The active kinome: The modern view of how active protein kinase networks fit in biological research. Curr. Opin. Pharmacol. 2022, 62, 117–129. [Google Scholar] [CrossRef] [PubMed]
- Fleuren, E.D.G.; Zhang, L.; Wu, J.; Daly, R.J. The kinome ‘at large’ in cancer. Nat. Rev. Cancer 2016, 16, 83–98. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Chaerkady, R.; Wu, J.; Hwang, H.J.; Papadopoulos, N.; Kopelovich, L.; Maitra, A.; Matthaei, H.; Eshleman, J.R.; Hruban, R.H.; et al. Mutant proteins as cancer-specific biomarkers. Proc. Natl. Acad. Sci. USA 2011, 108, 2444–2449. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. The hallmarks of cancer. Cell 2000, 100, 57–70. [Google Scholar] [CrossRef]
- Martínez-Jiménez, F.; Muiños, F.; Sentís, I.; Deu-Pons, J.; Reyes-Salazar, I.; Arnedo-Pac, C.; Mularoni, L.; Pich, O.; Bonet, J.; Kranas, H.; et al. A compendium of mutational cancer driver genes. Nat. Rev. Cancer 2020, 20, 555–572. [Google Scholar] [CrossRef]
- Bozic, I.; Antal, T.; Ohtsuki, H.; Carter, H.; Kim, D.; Chen, S.; Karchin, R.; Kinzler, K.W.; Vogelstein, B.; Nowak, M.A. Accumulation of driver and passenger mutations during tumor progression. Proc. Natl. Acad. Sci. USA 2010, 107, 18545–18550. [Google Scholar] [CrossRef]
- Vogelstein, B.; Kinzler, K.W. The Path to Cancer --Three Strikes and You’re Out. N. Engl. J. Med. 2015, 373, 1895–1898. [Google Scholar] [CrossRef]
- Tomasetti, C.; Marchionni, L.; Nowak, M.A.; Parmigiani, G.; Vogelstein, B. Only three driver gene mutations are required for the development of lung and colorectal cancers. Proc. Natl. Acad. Sci. USA 2015, 112, 118–123. [Google Scholar] [CrossRef]
- Wang, Y.; Douville, C.; Cohen, J.D.; Mattox, A.; Curtis, S.; Silliman, N.; Popoli, M.; Ptak, J.; Dobbyn, L.; Nehme, N.; et al. Detection of rare mutations, copy number alterations, and methylation in the same template DNA molecules. Proc. Natl. Acad. Sci. USA 2023, 120, e2220704120. [Google Scholar] [CrossRef]
- Imran, M.; Asdaq, S.M.B.; Khan, S.A.; Unnikrishnan Meenakshi, D.; Alamri, A.S.; Alsanie, W.F.; Alhomrani, M.; Mohzari, Y.; Alrashed, A.; AlMotairi, M.; et al. Innovations and Patent Trends in the Development of USFDA Approved Protein Kinase Inhibitors in the Last Two Decades. Pharmaceuticals 2021, 14, 710. [Google Scholar] [CrossRef] [PubMed]
- Roskoski, R. Properties of FDA-approved small molecule protein kinase inhibitors. Pharmacol. Res. 2019, 144, 19–50. [Google Scholar] [CrossRef] [PubMed]
- Kannaiyan, R.; Mahadevan, D. A comprehensive review of protein kinase inhibitors for cancer therapy. Expert Rev. Anticancer Ther. 2018, 18, 1249–1270. [Google Scholar] [CrossRef]
- Thompson, H.J.; Levitt, J.O.; McGinley, J.N.; Chandler, P.; Guenther, P.M.; Huybrechts, I.; Playdon, M.C. Measuring Dietary Botanical Diversity as a Proxy for Phytochemical Exposure. Nutrients 2021, 13, 1295. [Google Scholar] [CrossRef] [PubMed]
- Thompson, H.J.; Lutsiv, T. Natural Products in Precision Oncology: Plant-Based Small Molecule Inhibitors of Protein Kinases for Cancer Chemoprevention. Nutrients 2023, 15, 1192. [Google Scholar] [CrossRef] [PubMed]
- Lim, B.; Greer, Y.; Lipkowitz, S.; Takebe, N. Novel Apoptosis-Inducing Agents for the Treatment of Cancer, a New Arsenal in the Toolbox. Cancers 2019, 11, 1087. [Google Scholar] [CrossRef]
- Liu, C.; Zeng, Y.; Wen, Y.; Huang, X.; Liu, Y. Natural Products Modulate Cell Apoptosis: A Promising Way for the Treatment of Ulcerative Colitis. Front. Pharmacol. 2022, 13, 806148. [Google Scholar] [CrossRef]
- Shadman, M. Diagnosis and Treatment of Chronic Lymphocytic Leukemia: A Review. JAMA 2023, 329, 918–932. [Google Scholar] [CrossRef]
- Pfeffer, C.M.; Singh, A.T.K. Apoptosis: A Target for Anti-cancer Therapy. Int. J. Mol. Sci. 2018, 19, 448. [Google Scholar] [CrossRef]
- Fischer, K.; Al-Sawaf, O.; Hallek, M. Preventing and monitoring for tumor lysis syndrome and other toxicities of venetoclax during treatment of chronic lymphocytic leukemia. Hematol. Am. Soc. Hematol. Educ. Program 2020, 2020, 357–362. [Google Scholar] [CrossRef]
- Tahergorabi, Z.; Khazaei, M. A review on angiogenesis and its assays. Iran J. Basic Med. Sci. 2012, 15, 1110–1126. [Google Scholar] [PubMed]
- Hicklin, D.J.; Ellis, L.M. Role of the Vascular Endothelial Growth Factor Pathway in Tumor Growth and Angiogenesis. J. Clin. Oncol. 2005, 23, 1011–1027. [Google Scholar] [CrossRef] [PubMed]
- Eelen, G.; Treps, L.; Li, X.; Carmeliet, P. Basic and Therapeutic Aspects of Angiogenesis Updated. Circ. Res. 2020, 127, 310–329. [Google Scholar] [CrossRef] [PubMed]
- Cook, K.M.; Figg, W.D. Angiogenesis Inhibitors: Current Strategies and Future Prospects. CA Cancer J. Clin. 2010, 60, 222–243. [Google Scholar] [CrossRef] [PubMed]
- Rege, T.A.; Fears, C.Y.; Gladson, C.L. Endogenous inhibitors of angiogenesis in malignant gliomas: Nature’s antiangiogenic therapy. Neuro Oncol. 2005, 7, 106–121. [Google Scholar] [CrossRef]
- Ansari, M.J.; Bokov, D.; Markov, A.; Jalil, A.T.; Shalaby, M.N.; Suksatan, W.; Chupradit, S.; Al-Ghamdi, H.S.; Shomali, N.; Zamani, A.; et al. Cancer combination therapies by angiogenesis inhibitors; a comprehensive review. Cell Commun. Signal. 2022, 20, 49. [Google Scholar] [CrossRef]
- Martínez-Poveda, B.; Torres-Vargas, J.A.; Ocaña, M.d.C.; García-Caballero, M.; Medina, M.Á.; Quesada, A.R. The Mediterranean Diet, a Rich Source of Angiopreventive Compounds in Cancer. Nutrients 2019, 11, 2036. [Google Scholar] [CrossRef]
- Salehi, B.; Machin, L.; Monzote, L.; Sharifi-Rad, J.; Ezzat, S.M.; Salem, M.A.; Merghany, R.M.; El Mahdy, N.M.; Kılıç, C.S.; Sytar, O.; et al. Therapeutic Potential of Quercetin: New Insights and Perspectives for Human Health. ACS Omega 2020, 5, 11849–11872. [Google Scholar] [CrossRef]
- Li, W.W.; Li, V.W.; Hutnik, M.; Chiou, A.S. Tumor angiogenesis as a target for dietary cancer prevention. J. Oncol. 2012, 2012, 879623. [Google Scholar] [CrossRef]
- Baumeister, S.H.; Freeman, G.J.; Dranoff, G.; Sharpe, A.H. Coinhibitory Pathways in Immunotherapy for Cancer. Annu. Rev. Immunol. 2016, 34, 539–573. [Google Scholar] [CrossRef]
- Carbone, D.P.; Reck, M.; Paz-Ares, L.; Creelan, B.; Horn, L.; Steins, M.; Felip, E.; van den Heuvel, M.M.; Ciuleanu, T.E.; Badin, F.; et al. First-Line Nivolumab in Stage IV or Recurrent Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 376, 2415–2426. [Google Scholar] [CrossRef] [PubMed]
- Marin-Acevedo, J.A.; Kimbrough, E.O.; Lou, Y. Next generation of immune checkpoint inhibitors and beyond. J. Hematol. Oncol. 2021, 14, 45. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-J.; Thi, E.P.; Carpio, V.H.; Bi, Y.; Cole, A.G.; Dorsey, B.D.; Fan, K.; Harasym, T.; Iott, C.L.; Kadhim, S.; et al. Checkpoint inhibition through small molecule-induced internalization of programmed death-ligand 1. Nat. Commun. 2021, 12, 1222. [Google Scholar] [CrossRef] [PubMed]
- Sasikumar, P.G.; Sudarshan, N.S.; Adurthi, S.; Ramachandra, R.K.; Samiulla, D.S.; Lakshminarasimhan, A.; Ramanathan, A.; Chandrasekhar, T.; Dhudashiya, A.A.; Talapati, S.R.; et al. PD-1 derived CA-170 is an oral immune checkpoint inhibitor that exhibits preclinical anti-tumor efficacy. Commun. Biol. 2021, 4, 699. [Google Scholar] [CrossRef]
- Saldívar-González, F.I.; Aldas-Bulos, V.D.; Medina-Franco, J.L.; Plisson, F. Natural product drug discovery in the artificial intelligence era. Chem. Sci. 2022, 13, 1526–1546. [Google Scholar] [CrossRef]
- Mishra, S.K.; Jain, N.; Shankar, U.; Tawani, A.; Mishra, A.; Kumar, A. SMMDB: A web-accessible database for small molecule modulators and their targets involved in neurological diseases. Database 2018, 2018, bay082. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer. World Health Organization. Exposome Explorer. Available online: http://exposome-explorer.iarc.fr/ (accessed on 1 February 2023).
- Gonzalez, G.; Gong, S.; Laponogov, I.; Bronstein, M.; Veselkov, K. Predicting anti-cancer hyperfoods with graph convolutional networks. Hum Genom. 2021, 15, 33. [Google Scholar] [CrossRef]
- Cayman Chemical. Small Molecule Inhibitors Selection Guide. Available online: https://www.caymanchem.com/news/small-molecule-inhibitors-selection-guide (accessed on 15 February 2023).
- Uitdehaag, J.C.; Verkaar, F.; Alwan, H.; de Man, J.; Buijsman, R.C.; Zaman, G.J. A guide to picking the most selective kinase inhibitor tool compounds for pharmacological validation of drug targets. Br. J. Pharm. 2012, 166, 858–876. [Google Scholar] [CrossRef]
- Salimi, A.; Lim, J.H.; Jang, J.H.; Lee, J.Y. The use of machine learning modeling, virtual screening, molecular docking, and molecular dynamics simulations to identify potential VEGFR2 kinase inhibitors. Sci. Rep. 2022, 12, 18825. [Google Scholar] [CrossRef]
- Fountzilas, E.; Tsimberidou, A.M.; Vo, H.H.; Kurzrock, R. Clinical trial design in the era of precision medicine. Genome Med. 2022, 14, 101. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thompson, H.J.; Lutsiv, T.; McGinley, J.N.; Hussan, H.; Playdon, M.C. Dietary Oncopharmacognosy as a Crosswalk between Precision Oncology and Precision Nutrition. Nutrients 2023, 15, 2219. https://doi.org/10.3390/nu15092219
Thompson HJ, Lutsiv T, McGinley JN, Hussan H, Playdon MC. Dietary Oncopharmacognosy as a Crosswalk between Precision Oncology and Precision Nutrition. Nutrients. 2023; 15(9):2219. https://doi.org/10.3390/nu15092219
Chicago/Turabian StyleThompson, Henry J., Tymofiy Lutsiv, John N. McGinley, Hisham Hussan, and Mary C. Playdon. 2023. "Dietary Oncopharmacognosy as a Crosswalk between Precision Oncology and Precision Nutrition" Nutrients 15, no. 9: 2219. https://doi.org/10.3390/nu15092219