
A Positive Causal Relationship between Noodle Intake and Metabolic Syndrome: A Two-Sample Mendelian Randomization Study


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Demographic, Anthropometric, Biochemical, and Clinical Parameter Assessment
2.3. MetS Definition
2.4. Food and Nutrient Intake Measurement
2.5. Dietary Patterns, Dietary Inflammatory Index (DII), Glycemic Index (GI), and Glycemic Load (GL)
2.6. Genotyping and Quality Control
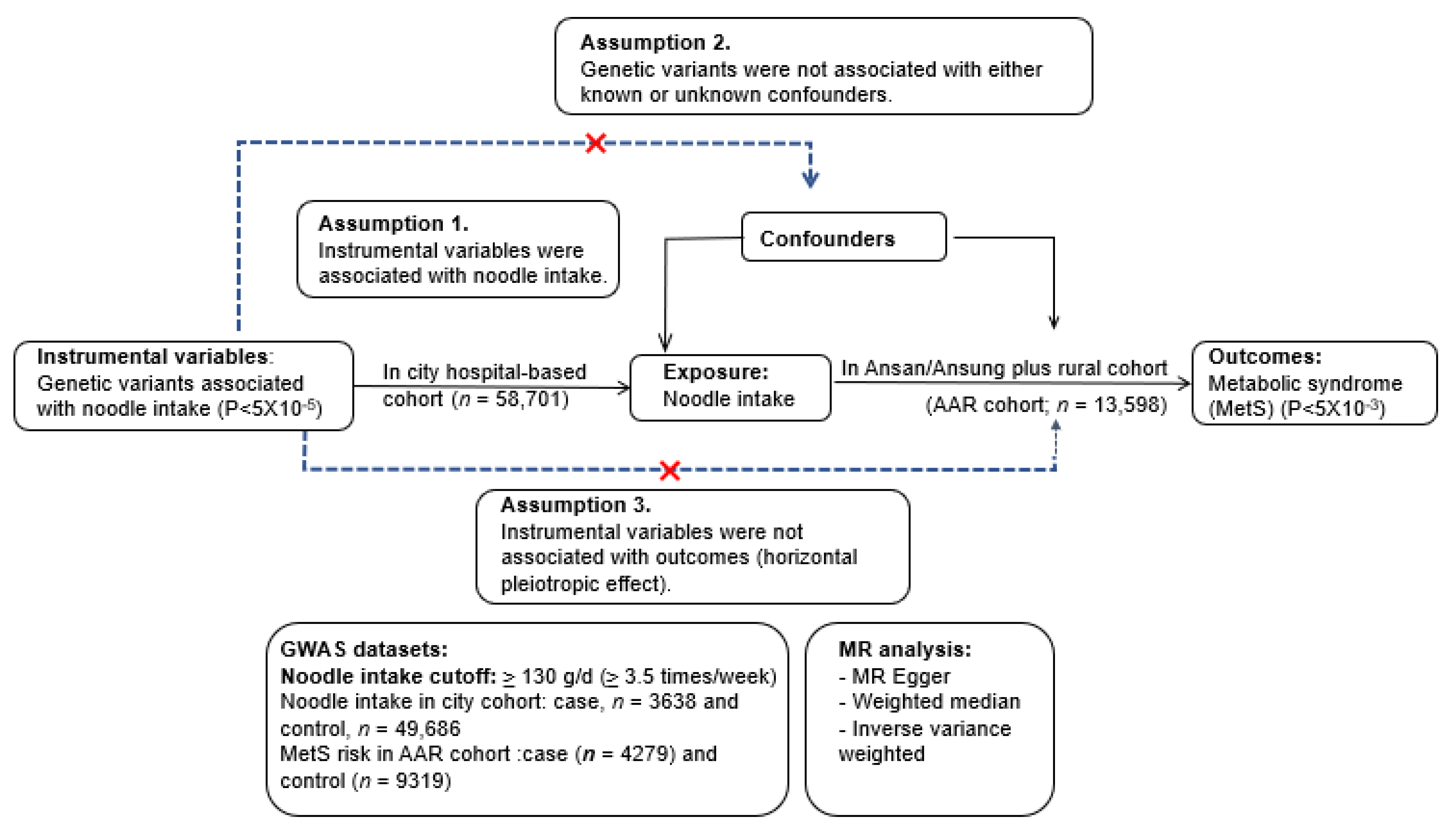
2.7. Identification of Instrumental Variables in a Two-Sample MR Analysis
2.8. A Two-Sample MR Analysis Design
2.9. Statistical Analysis
3. Results
3.1. Demographic Characteristics and Lifestyles of the Participants
3.2. Food and Nutrient Intake
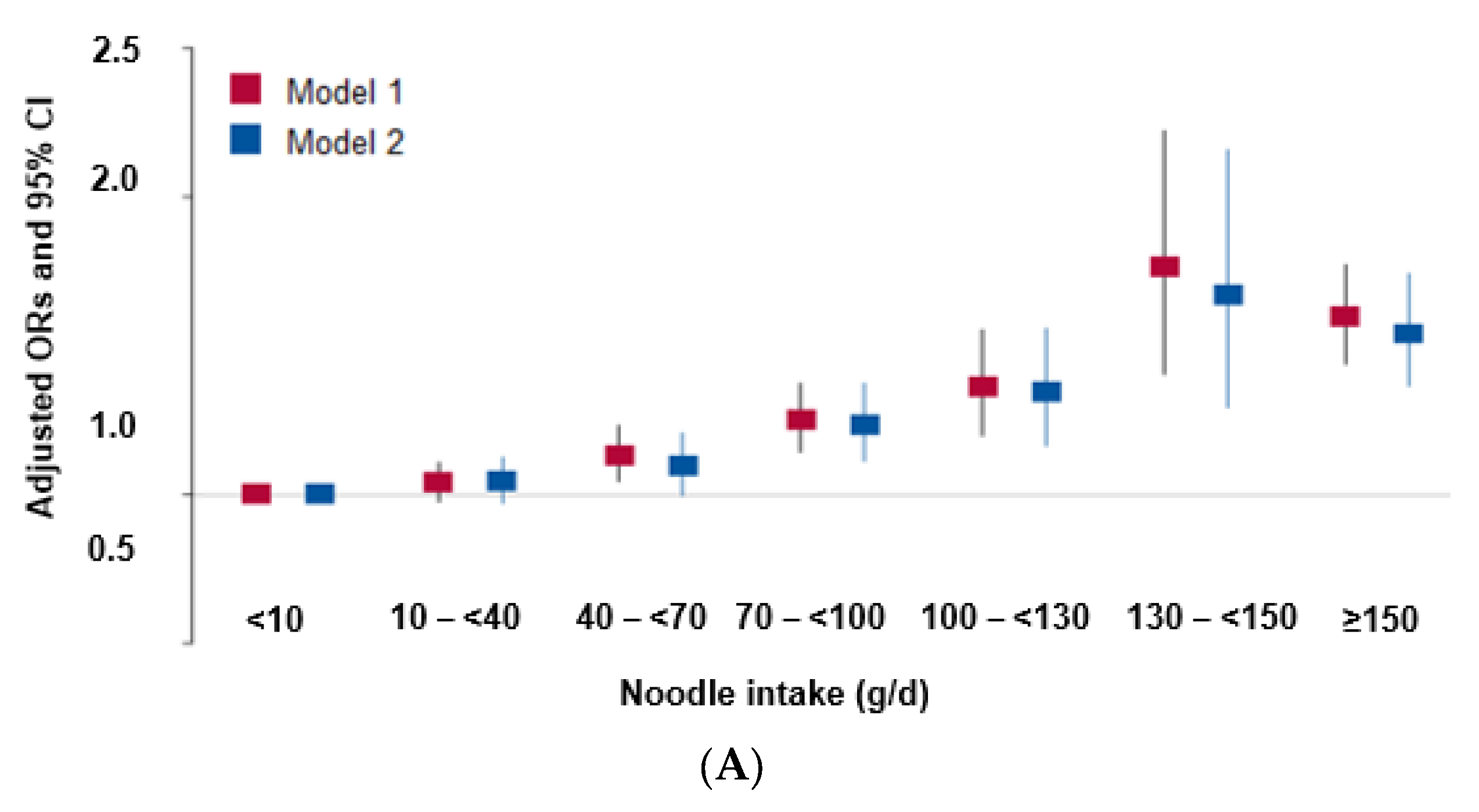
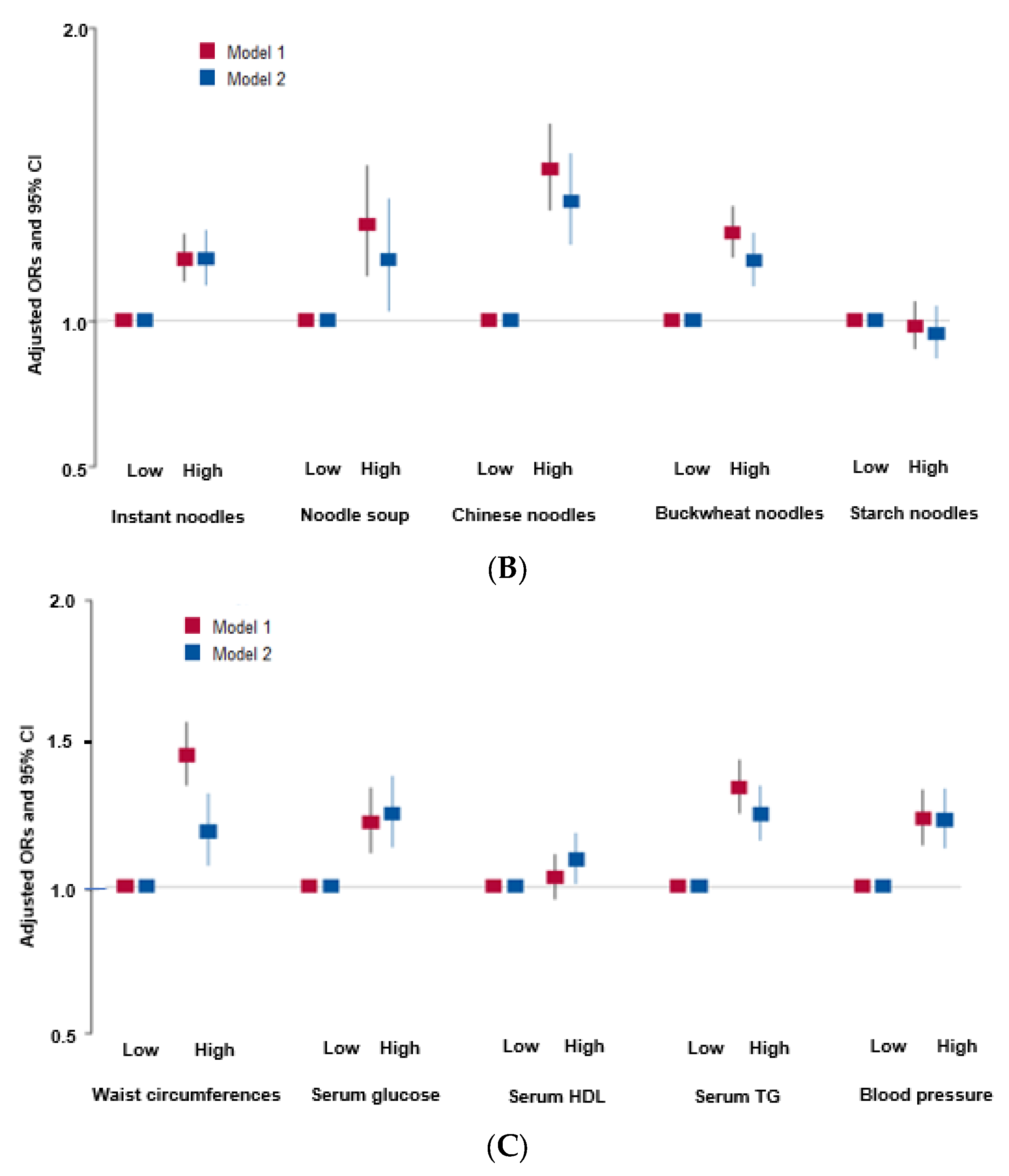
3.3. Observational Association of Noodle Intake, MetS, and Its Components
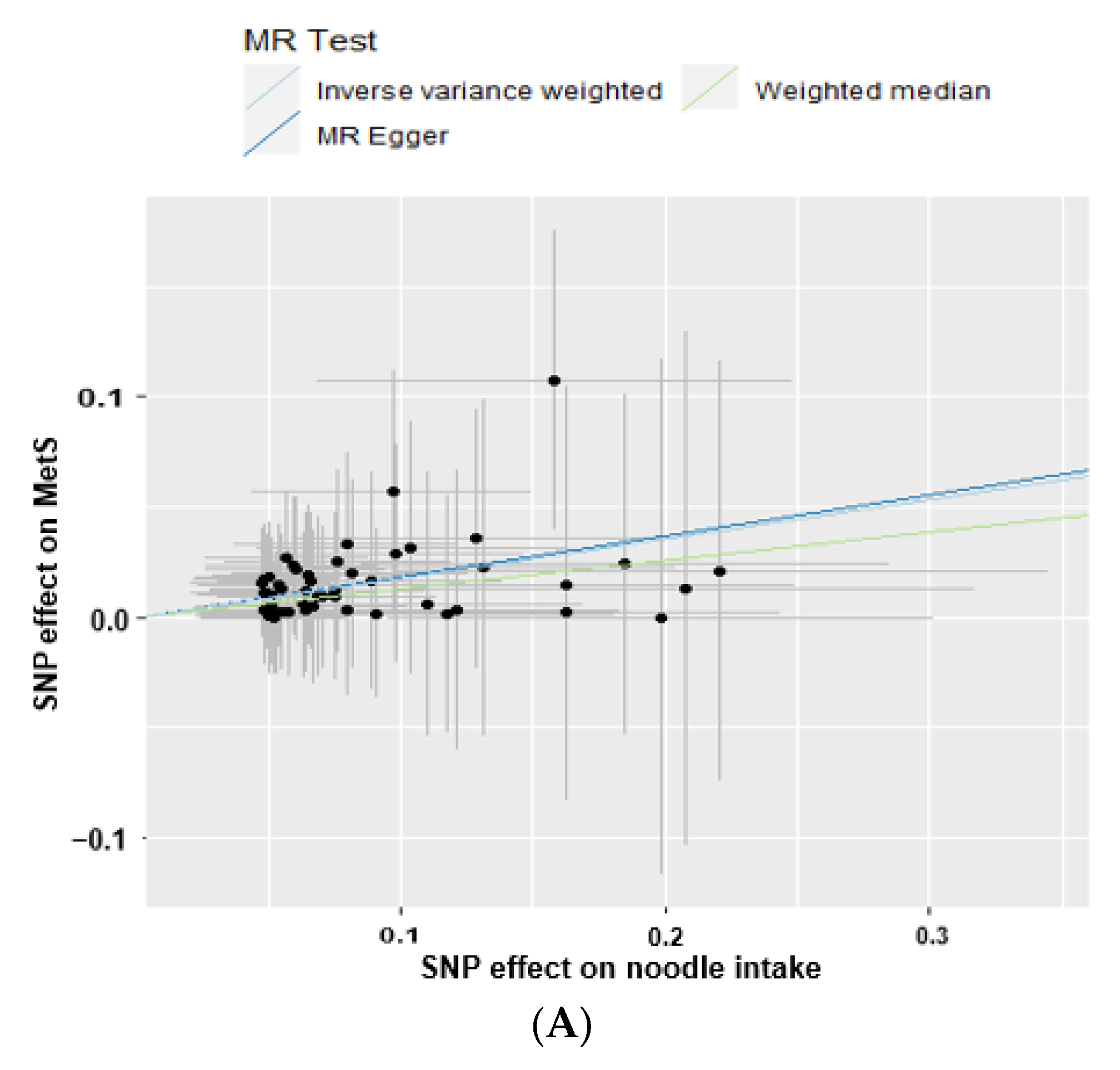
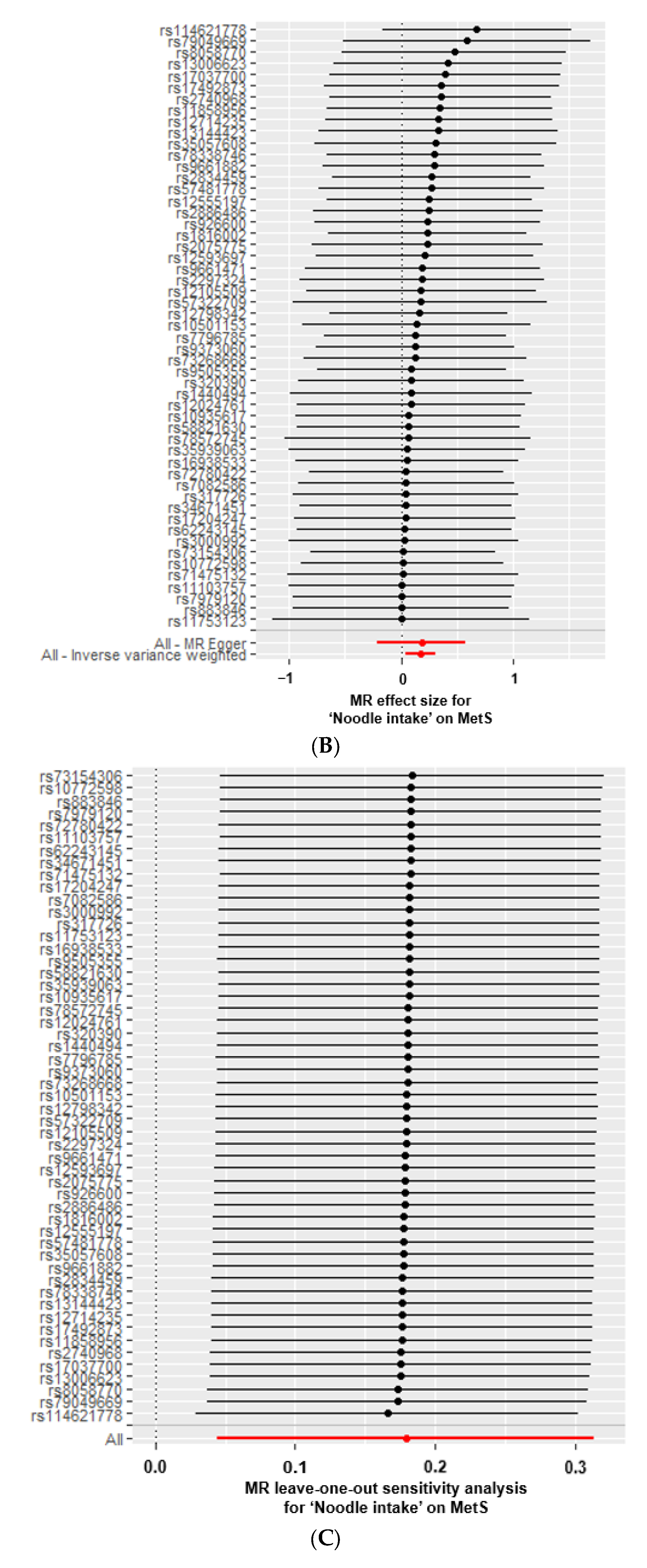
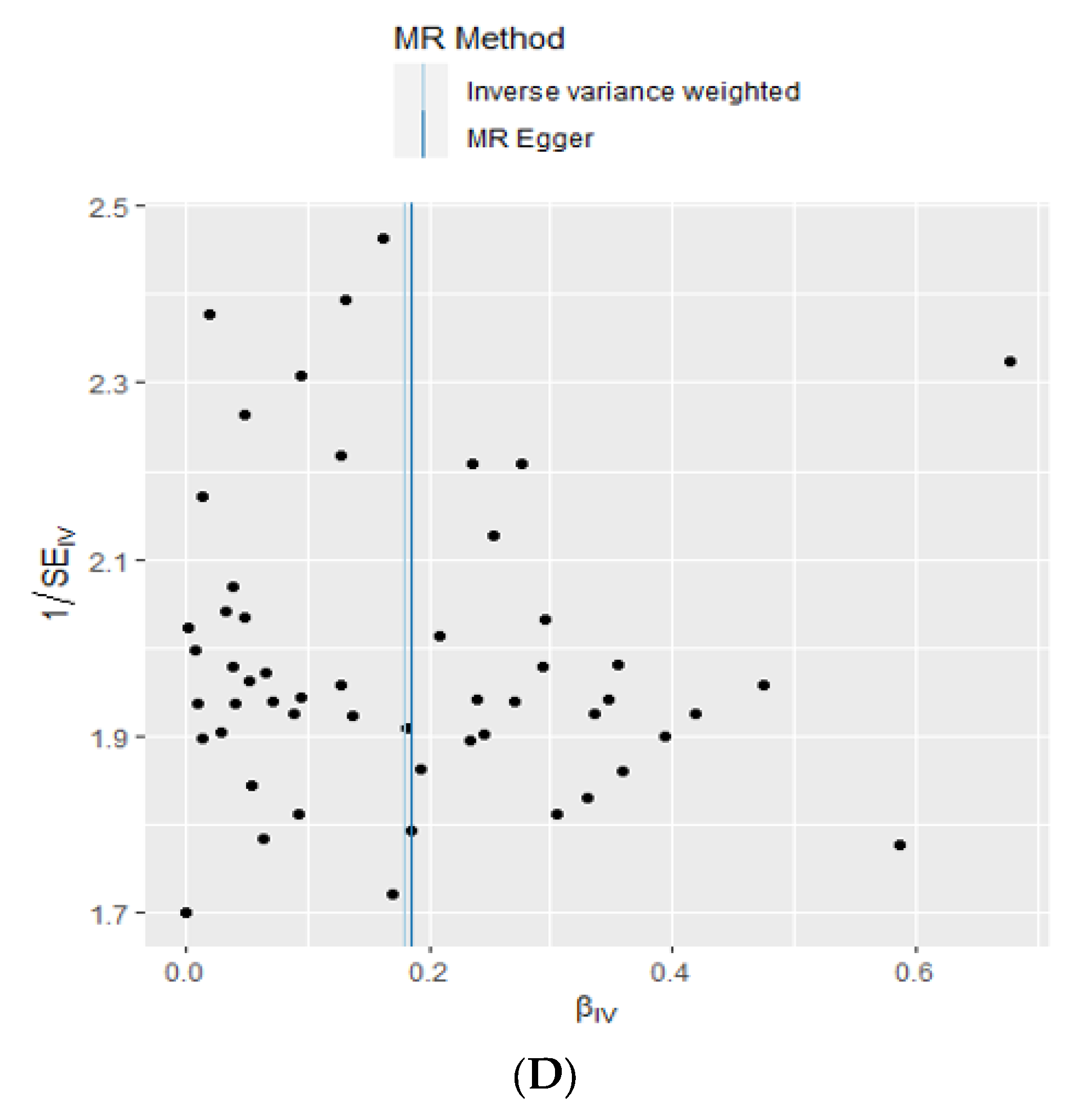
3.4. A Causal Relationship between Total Noodle Intake with MetS and Its Components by a Two-Sample MR Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Park, S.; Zhang, T. A Positive Association of Overactivated Immunity with Metabolic Syndrome Risk and Mitigation of Its Association by a Plant-Based Diet and Physical Activity in a Large Cohort Study. Nutrients 2021, 13, 2308. [Google Scholar] [CrossRef]
- Kim, M.; Lee, S.; Shin, K.; Son, D.; Kim, S.; Joe, H.; Yoo, B.; Hong, S.; Cho, C.; Shin, H.; et al. The Change of Metabolic Syndrome Prevalence and Its Risk Factors in Korean Adults for Decade: Korea National Health and Nutrition Examination Survey for 2008–2017. Korean J. Fam. Pr. 2020, 10, 44–52. [Google Scholar] [CrossRef]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.J.; Kim, M.J.; Hur, H.J.; Lee, B.K.; Kim, M.S.; Park, S. Association Between Korean-Style Balanced Diet and Risk of Abdominal Obesity in Korean Adults: An Analysis Using KNHANES-VI (2013–2016). Front. Nutr. 2021, 8, 772347. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Hur, H.J.; Jang, D.J.; Kim, M.S.; Park, S.; Yang, H.J. Inverse association of a traditional Korean diet composed of a multigrain rice-containing meal with fruits and nuts with metabolic syndrome risk: The KoGES. Front. Nutr. 2022, 9, 1051637. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.A.; Kim, J.; Cho, E.R.; Shin, A. Dietary patterns and the prevalence of metabolic syndrome in Korean women. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.J.; Cho, E.; Lee, H.-J.; Fung, T.T.; Rimm, E.; Rosner, B.; Manson, J.E.; Wheelan, K.; Hu, F.B. Instant Noodle Intake and Dietary Patterns Are Associated with Distinct Cardiometabolic Risk Factors in Korea. J. Nutr. 2014, 144, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Ha, K.; Kim, K.; Chun, O.K.; Joung, H.; Song, Y. Differential association of dietary carbohydrate intake with metabolic syndrome in the US and Korean adults: Data from the 2007–2012 NHANES and KNHANES. Eur. J. Clin. Nutr. 2018, 72, 848–860. [Google Scholar] [CrossRef]
- Huh, I.S.; Kim, H.; Jo, H.K.; Lim, C.S.; Kim, J.S.; Kim, S.J.; Kwon, O.; Oh, B.; Chang, N. Instant noodle consumption is associated with cardiometabolic risk factors among college students in Seoul. Nutr. Res. Pract. 2017, 11, 232–239. [Google Scholar] [CrossRef]
- Huang, M.; Li, J.; Ha, M.A.; Riccardi, G.; Liu, S. A systematic review on the relations between pasta consumption and cardio-metabolic risk factors. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 939–948. [Google Scholar] [CrossRef]
- Pounis, G.; Castelnuovo, A.D.; Costanzo, S.; Persichillo, M.; Bonaccio, M.; Bonanni, A.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L.; et al. Association of pasta consumption with body mass index and waist-to-hip ratio: Results from Moli-sani and INHES studies. Nutr. Diabetes 2016, 6, e218. [Google Scholar] [CrossRef] [PubMed]
- Park, S. Association between polygenetic risk scores related to sarcopenia risk and their interactions with regular exercise in a large cohort of Korean adults. Clin. Nutr. 2021, 40, 5355–5364. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Ahn, J.; Lee, B.-K. Self-rated subjective health status is strongly associated with sociodemographic factors, lifestyle, nutrient intakes, and biochemical indices, but not smoking status: KNHANES 2007–2012. J. Korean Med. Sci. 2015, 30, 1279–1287. [Google Scholar] [CrossRef]
- Park, S.; Liu, M.; Kang, S. Alcohol intake interacts with CDKAL1, HHEX, and OAS3 genetic variants, associated with the risk of type 2 diabetes by lowering insulin secretion in Korean adults. Alcohol. Clin. Exp. Res. 2018, 42, 2326–2336. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Han, B.-G.; Group, K. Cohort profile: The Korean genome and epidemiology study (KoGES) consortium. Int. J. Epidemiol. 2017, 46, e20. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef]
- Liu, J.; Grundy, S.M.; Wang, W.; Smith, S.C., Jr.; Vega, G.L.; Wu, Z.; Zeng, Z.; Wang, W.; Zhao, D. Ethnic-Specific Criteria for the Metabolic Syndrome: Evidence from China. Diabetes Care 2006, 29, 1414–1416. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.; Kwon, E.; Shim, J.; Park, M.; Joo, Y.; Kimm, K.; Park, C.; Kim, D. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef]
- Park, S.; Kang, S. A Western-style diet interacts with genetic variants of the LDL receptor to hyper-LDL cholesterolemia in Korean adults. Public Health Nutr. 2021, 24, 2964–2974. [Google Scholar] [CrossRef]
- Kim, D.-Y.; Kim, Y.; Lim, H. Glycaemic indices and glycaemic loads of common Korean carbohydrate-rich foods. Br. J. Nutr. 2019, 121, 416–425. [Google Scholar] [CrossRef]
- Foster-Powell, K.; Holt, S.H.; Brand-Miller, J.C. International table of glycemic index and glycemic load values: 2002. Am. J. Clin. Nutr. 2002, 76, 5–56. [Google Scholar] [CrossRef] [PubMed]
- Wolever, T.M.S.; Jenkins, D.J.A. The use of the glycemic index in predicting the blood glucose response to mixed meals. Am. J. Clin. Nutr. 1986, 43, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Hong, K.W.; Kim, S.H.; Zhang, X.; Park, S. Interactions among the variants of insulin-related genes and nutrients increase the risk of type 2 diabetes. Nutr. Res. 2018, 51, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Rabbee, N.; Speed, T.P. A genotype calling algorithm for affymetrix SNP arrays. Bioinformatics 2006, 22, 7–12. [Google Scholar] [CrossRef]
- Park, S.; Zhang, X.; Lee, N.R.; Jin, H.-S. TRPV1 gene polymorphisms are associated with type 2 diabetes by their interaction with fat consumption in the Korean genome epidemiology study. J. Nutr. Nutr. 2016, 9, 47–61. [Google Scholar] [CrossRef]
- Storey, J.D.; Tibshirani, R. Statistical significance for genome wide studies. Proc. Natl. Acad. Sci. USA 2003, 100, 9440–9445. [Google Scholar] [CrossRef]
- De Leeuw, C.; Savage, J.; Bucur, I.G.; Heskes, T.; Posthuma, D. Understanding the assumptions underlying Mendelian randomization. Eur. J. Hum. Genet. 2022, 30, 653–660. [Google Scholar] [CrossRef]
- Burgess, S.; Thompson, S.G. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur. J. Epidemiol. 2017, 32, 377–389. [Google Scholar] [CrossRef]
- Huang, M.; Lo, K.; Li, J.; Allison, M.; Wu, W.-C.; Liu, S. Pasta meal intake in relation to risks of type 2 diabetes and atherosclerotic cardiovascular disease in postmenopausal women: Findings from the Women’s Health Initiative. BMJ Nutr. Prev. Health 2021, 4, 195–205. [Google Scholar] [CrossRef]
- Wang, Y.; Dai, Y.; Tian, T.; Zhang, J.; Xie, W.; Pan, D.; Xu, D.; Lu, Y.; Wang, S.; Xia, H.; et al. The Effects of Dietary Pattern on Metabolic Syndrome in Jiangsu Province of China: Based on a Nutrition and Diet Investigation Project in Jiangsu Province. Nutrients 2021, 13, 4451. [Google Scholar] [CrossRef]
- Chen, Y.; Kang, M.; Kim, H.; Xu, W.; Lee, J.E. Associations of dietary patterns with obesity and weight change for adults aged 18–65 years: Evidence from the China Health and Nutrition Survey (CHNS). PLoS ONE 2023, 18, e0279625. [Google Scholar] [CrossRef] [PubMed]
- Bergia, R.E.; Giacco, R.; Hjorth, T.; Biskup, I.; Zhu, W.; Costabile, G.; Vitale, M.; Campbell, W.W.; Landberg, R.; Riccardi, G. Differential Glycemic Effects of Low- versus High-Glycemic Index Mediterranean-Style Eating Patterns in Adults at Risk for Type 2 Diabetes: The MEDGI-Carb Randomized Controlled Trial. Nutrients 2022, 14, 706. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Park, S.; Yang, H.J.; Shin, P.K.; Hur, H.J.; Park, S.J.; Lee, K.H.; Hong, M.; Kim, J.H.; Choi, S.W.; et al. Alleviation of Dyslipidemia via a Traditional Balanced Korean Diet Represented by a Low Glycemic and Low Cholesterol Diet in Obese Women in a Randomized Controlled Trial. Nutrients 2022, 14, 235. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Kang, S. High carbohydrate and noodle/meat-rich dietary patterns interact with the minor haplotype in the 22q13 loci to increase its association with non-alcoholic fatty liver disease risk in Koreans. Nutr. Res. 2020, 82, 88–98. [Google Scholar] [CrossRef]
- Burgess, S.; Small, D.S.; Thompson, S.G. A review of instrumental variable estimators for Mendelian randomization. Stat. Methods Med. Res. 2017, 26, 2333–2355. [Google Scholar] [CrossRef]
- Bowden, J.; Davey Smith, G.; Burgess, S. Mendelian randomization with invalid instruments: Effect estimation and bias detection through Egger regression. Int. J. Epidemiol. 2015, 44, 512–525. [Google Scholar] [CrossRef]
- Park, S. A Causal and Inverse Relationship between Plant-Based Diet Intake and in a Two-Sample Mendelian Randomization Study. Foods 2023, 12, 545. [Google Scholar] [CrossRef]
- Bowden, J. Misconceptions on the use of MR-Egger regression and the evaluation of the InSIDE assumption. Int. J. Epidemiol. 2017, 46, 2097–2099. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H. Overview of Mendelian Randomization Analysis. J. Rheum. Dis. 2020, 27, 241–246. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Men (n = 20,293) | Women (n = 38,408) | |||
|---|---|---|---|---|
| Low Intake of Noodles (n = 17,799) | High Intake of Noodle (n = 2494) | Low Intake of Noodles (n = 36,409) | High Intake of Noodle (n = 1999) | |
| Age (years) | 56.7 ± 0.06 a | 54.3 ± 0.16 b | 52.5 ± 0.04 c | 50.3 ± 0.179 d***+++ |
| Education (Yes, %) ≤Middle school High school ≥College | 1554 (14.2) 8314 (75.8) 1105 (10.1) | 199 (13.2) ‡ 1120 (74.4) 186 (12.4) | 6529 (22.6) 20,711 (71.7) 1665 (5.76) | 209 (14.1) ‡‡‡ 1160 (78.1) 117 (7.87) |
| Income (Yes, %) ≤$2000 $2000–4000 >$4000 | 1449 (8.57) 7179 (42.4) 8287 (49.0) | 157 (6.55) ‡‡ 1028 (42.9) 1213 (50.6) | 4038 (11.8) 15,144 (44.2) 15,049 (44.0) | 134 (7.07) ‡‡‡ 841 (44.4) 921 (48.6) |
| Past smoker Smoker (Yes, %) | 7795 (43.9) 4740 (26.7) | 1000 (40.1) 924 (37.1) ‡‡‡ | 418 (1.15) 663 (1.83) | 42 (2.11) 86 (4.31) ‡‡‡ |
| Alcohol intake (g/day) | 6.5 ± 0.11 b | 10.3 ± 0.28 a | 1.7 ± 0.08 c | 2.2 ± 0.31 c***+++## |
| Physical activity (Yes, %) | 10,547 (59.5) | 1405 (56.4) ‡‡ | 19,091 (52.6) | 933 (46.7) ‡‡‡ |
| Energy (EER percent) | 86.9 ± 0.24 d | 110.5 ± 0.61 b | 97.7 ± 0.16 c | 131.5 ± 0.66 a***+++### |
| Carbohydrates (En%) | 72.0 ± 0.06 a | 68.8 ± 0.14 b | 72.0 ± 0.04 a | 68.5 ± 0.15 b+++ |
| Protein (En%) | 13.0 ± 0.02 d | 13.7 ± 0.05 b | 13.5 ± 0.01 c | 14.1 ± 0.06 a***+++ |
| Fat (En%) | 13.7 ± 0.04 b | 16.5 ± 0.11 a | 13.6 ± 0.03 b | 16.5 ± 0.12 a+++ |
| Saturated fat (En%) | 4.27 ± 0.01 c | 5.37 ± 0.03 a | 4.35 ± 0.01 b | 5.22 ± 0.03 a+++### |
| Monounsaturated fat (En%) | 5.46 ± 0.01 c | 6.86 ± 0.02 a | 5.35 ± 0.01 d | 6.72 ± 0.03 b***++ |
| Polyunsaturated fat (En%) | 3.10 ± 0.02 b | 3.80 ± 0.04 a | 3.08 ± 0.01 b | 3.78 ± 0.05 a+++ |
| Cholesterol (mg/day) | 162.7 ± 0.79 d | 193.3 ± 1.99 b | 168.0 ± 0.53 c | 210.1 ± 2.16 a***+++## |
| Fiber (g/day) | 16.1 ± 0.07 a | 16.4 ± 0.16 a | 14.0 ± 0.04 b | 13.1 ± 0.18 c** |
| Calcium (mg/day) | 453 ± 1.50 a | 373 ± 3.73 c | 449 ± 0.99 a | 390 ± 5.1 b***+++### |
| Sodium (g/day) | 2.67 ± 0.01 b | 2.82 ± 0.02 a | 2.29 ± 0.01 c | 2.30 ± 0.03 c***+++## |
| Potassium (g/day) | 2.34 ± 0.01 a | 2.13 ± 0.01 c | 2.20 ± 0.003 b | 1.81 ± 0.02 d***+++### |
| Vitamin C (mg/day) | 105 ± 0.47 b | 87.3 ± 1.18 d | 109 ± 0.32 a | 77.3 ± 1.31 c***+++## |
| Vitamin D (ug/day) | 6.2 ± 0.04 b | 4.2 ± 0.09 c | 6.8 ± 0.02 a | 4.0 ± 0.10 c*+++### |
| DII (scores) | −20.6 ± 0.12 a | −18.6 ± 0.29 b | −19.1 ± 0.08 b | −15.0 ± 0.32 c***+++### |
| Flavonoids (mg/day) | 36.3 ± 0.25 b | 27.8 ± 0.62 c | 40.9 ± 0.16 a | 26.3 ± 0.68 c**+++### |
| Men (n = 20,293) | Women (n = 38,408) | |||
|---|---|---|---|---|
| Low Intake of Noodles (n = 17,799) | High Intake of Noodle (n = 2494) | Low Intake of Noodles (n = 36,409) | High Intake of Noodle (n = 1999) | |
| Total noodle | 47.6 ± 0.49 c | 213.1 ± 1.22 b | 30.6 ± 0.32 d | 221.2 ± 1.35 a***+++### |
| Instant noodles | 10.8 ± 0.13 c | 30.9 ± 0.32 a | 5.21 ± 0.09 d | 22.7 ± 0.35 b***+++## |
| Wheat noodle soup | 18.3 ± 0.28 c | 85.3 ± 0.70 b | 15.6 ± 0.18 d | 108.5 ± 0.77 a***+++### |
| Chinese noodle | 14.7 ± 0.29 c | 84.3 ± 0.73 a | 7.1 ± 0.20 d | 74.7 ± 0.81 b***+++ |
| Buckwheat noodle | 3.23 ± 0.08 c | 12.1 ± 0.20 b | 2.23 ± 0.05 d | 14.7 ± 0.22 a***+++### |
| Starch noodle | 0.56 ± 0.02 a | 0.57 ± 0.05 a | 0.43 ± 0.01 b | 0.54 ± 0.05 ab* |
| White rice | 147 ± 2.0 b | 179 ± 5.03 a | 82.6 ± 1.34 d | 113 ± 5.58 c***+++ |
| Whole grains | 523 ± 2.04 a | 431 ± 5.07 c | 457 ± 1.35 b | 329 ± 5.62 d***+++### |
| Bread | 12.5 ± 0.19 c | 13.9 ± 0.46 b | 12.7 ± 0.12 c | 21.2 ± 0.51 a***+++### |
| Cookie | 3.07 ± 0.06 a | 2.44 ± 0.16 c | 2.72 ± 0.04 b | 2.53 ± 0.18 bc+++ |
| Potato | 17.4 ± 0.21 b | 13.9 ± 0.52 c | 20.7 ± 0.14 a | 16.0 ± 0.57 b***+++ |
| Green vegetables | 70.8 ± 0.52 a | 54.4 ± 1.30 c | 75.0 ± 0.35 b | 54.0 ± 1.47 c+++# |
| White vegetables | 45.9 ± 0.33 a | 39.6 ± 0.83 b | 41.0 ± 0.22 b | 30.6 ± 0.92 c***+++## |
| Kimchi | 158 ± 0.91 a | 143 ± 2.26 b | 131 ± 0.60 c | 103 ± 2.51 d***+++### |
| Fruits | 199 ± 1.68 b | 147 ± 4.19 c | 237 ± 1.11 a | 144 ± 4.64 c***+++### |
| Beans | 30.3 ± 0.20 a | 27.0 ± 0.50 c | 29.2 ± 0.13 b | 24.3 ± 0.55 d***+++# |
| Seaweeds | 1.81 ± 0.02 b | 1.40 ± 0.04 c | 2.12 ± 0.01 a | 1.55 ± 0.05 c***+++## |
| Meats | 47.7 ± 0.28 a | 44.3 ± 0.69 b | 33.8 ± 0.18 c | 25.8 ± 0.76 d***+++### |
| Fish | 35.5 ± 0.24 a | 26.3 ± 0.60 c | 33.5 ± 0.16 b | 20.5 ± 0.67 d***+++### |
| Process meats | 48.7 ± 0.72 a | 41.7 ± 1.79 b | 44.8 ± 0.48 b | 38.0 ± 1.99 bc**+++ |
| Milk and milk products | 109.2 ± 1.04 b | 69.6 ± 2.60 c | 128.7 ± 0.69 a | 75.4 ± 2.88 c***+++## |
| Nuts | 1.6 ± 0.03 b | 1.1 ± 0.08 c | 1.9 ± 0.02 a | 1.3 ± 0.09 c***+++ |
| Coffee | 4.2 ± 0.03 a | 4.2 ± 0.06 a | 3.3 ± 0.02 c | 3.5 ± 0.07 b***# |
| Glycemic index | 49.4 ± 0.10 c | 59.8 ± 0.28 a | 45.6 ± 0.08 d | 58.2 ± 0.32 b***+++### |
| Glycemic load | 154 ± 0.35 b | 193 ± 0.97 a | 142 ± 0.25 d | 186 ± 1.1576 b***+++### |
| KBD (N, %) | 6909 (38.8) | 1278 (51.2) ‡‡‡ | 10,678 (29.3) | 750 (37.5) ‡‡‡ |
| PBD (N, %) | 3719 (20.9) | 563 (22.6) ‡ | 14,499 (39.8) | 999 (50.0) ‡‡‡ |
| WSD (N, %) | 8044 (45.2) | 2379 (95.4) ‡‡‡ | 11,389 (31.3) | 1822 (91.2) ‡‡‡ |
| RMD (N, %) | 5577 (31.3) | 947 (38.0) ‡‡‡ | 12,235 (33.9) | 749 (37.5) ‡‡ |
| Men (n = 20,293) | Women (n = 38,408) | |||||
|---|---|---|---|---|---|---|
| Low Intake of Noodles (n = 17,799) | High Intake of Noodles (n = 2494) | Adjusted OR | Low Intake of Noodles (n = 36,409) | High Intake of Noodle (n = 1999) | Adjusted OR | |
| MetS (Yes, %) 1 | 3052 (17.2) | 546 (21.9) ‡‡‡ | 1.341 (1.182–1.523) | 4438 (12.2) | 264 (13.2) | 1.345 (1.144–1.580) |
| BMI (mg/kg2) 2 | 24.4 ± 0.02 b | 24.7 ± 0.07 a | 1.147 (1.045–1.260) | 23.6 ± 0.02 c | 23.7 ± 0.08 c***+++ | 1.165 (1.047–1.296) |
| Waist C. (cm) 3 | 84.3 ± 0.04 b | 84.7 ± 0.11 a | 1.263 (1.141–1.398) | 78.8 ± 0.03 c | 79 ± 0.13 c***++# | 1.257 (1.111–1.423) |
| SMI (kg/m2) 4 | 7.2 ± 0.01 a | 7.3 ± 0.02 a | 1.047 (0.951–1.153) | 6.1 ± 0 b | 6.1 ± 0.02 b | 1.068 (0.946–1.206) |
| Fat mass (%) 5 | 22.6 ± 0.01 c | 22.6 ± 0.02 b | 1.232 (1.115–1.361) | 31.4 ± 0.01 a | 31.5 ± 0.03 a***++ | 1.169 (1.055–1.295) |
| Plasma glucose (mg/dL) 6 | 98 ± 0.17 b | 100.1 ± 0.47 a | 1.210 (1.074–1.363) | 93.5 ± 0.12 c | 94.5 ± 0.52 c***+++ | 1.248 (1.053–1.479) |
| Blood HbA1 c (%) 7 | 5.67 ± 0.01 b | 5.73 ± 0.02 a | 1.297 (1.068–1.575) | 5.73 ± 0.01 b | 5.73 ± 0.02 b# | 1.578 (1.226–2.031) |
| Insulin resistance (%) 8 | 1910 (11.1) | 299 (14.5) ‡‡‡ | 1.288 (1.118–1.484) | 1961 (6.04) | 105 (6.65) | 1.196 (0.970–1.475) |
| Serum total cholesterol (mg/dL) 9 | 190.6 ± 0.31 c | 193.2 ± 0.85 b | 1.202 (1.071–1.350) | 201.3 ± 0.22 a | 200.3 ± 0.95 a+++## | 1.028 (0.915–1.155) |
| Serum HDL (mg/dL) 10 | 49.4 ± 0.11 b | 49.7 ± 0.3 b | 1.063 (0.945–1.195) | 56.1 ± 0.08 a | 56.3 ± 0.33 a*** | 1.071 (0.963–1.191) |
| Serum LDL (mg/dL) 11 | 113 ± 0.28 b | 112.8 ± 0.78 b | 1.137 (0.990–1.306) | 122.1 ± 0.2 a | 119.9 ± 0.87 a*** | 1.142 (1.001–1.302) |
| Serum TG (mg/dL) 12 | 140.9 ± 0.72 b | 153.4 ± 2 a | 1.199 (1.087–1.321) | 116 ± 0.51 c | 120.8 ± 2.23 c***+++# | 1.284 (1.144–1.441) |
| SBP (mmHg) 13 | 124.6 ± 0.12 a | 125.1 ± 0.33 a | 1.097 (0.997–1.208) | 121.3 ± 0.09 b | 121.2 ± 0.37 b*** | 1.099 (0.981–1.230) |
| DBP (mmHg) 14 | 77.8 ± 0.08 a | 78.3 ± 0.22 a | 1.233 (1.079–1.409) | 74.7 ± 0.06 b | 74.6 ± 0.25 b*** | 0.971 (0.798–1.182) |
| Serum hs-CRP (mg/L) 15 | 0.142 ± 0.004 | 0.154 ± 0.01 | 1.013 (0.708–1.449) | 0.136 ± 0.003 | 0.148 ± 0.011 | 1.093 (0.696–1.716) |
| Serum urate (mg/dL) 16 | 5.54 ± 0.01 | 5.62 ± 0.02 | 1.126 (1.023–1.240) | 4.22 ± 0.01 | 4.25 ± 0.02 | 1.360 (1.065–1.736) |
| eGFR (ml/min) 17 | 84.7 ± 0.13 b | 84.6 ± 0.33 b | 1.273 (0.996–1.628) | 86.5 ± 0.09 a | 86.7 ± 0.36 a*** | 1.288 (0.962–1.724) |
| Serum AST (U/L) 18 | 24.7 ± 0.24 a | 26 ± 0.59 a | 1.169 (0.972–1.407) | 23.1 ± 0.16 b | 23.1 ± 0.64 b*** | 1.025 (0.790–1.329) |
| Serum ALT (U/L) 19 | 25.5 ± 0.23 b | 27.2 ± 0.56 a | 1.065 (0.945–1.201) | 20.7 ± 0.16 c | 20.4 ± 0.61 a***+++## | 0.905 (0.751–1.092) |
| 9 | MR | Heterogeneity | Pleiotropy | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Method | OR (95% CI) | p | Method | Q | p-Value | Intercept | SE | p-Value | |
| Metabolic syndrome | MR-Egger | 1.204(0.811~1.787) | 0.362 | MR-Egger | 5.214 | 1 | −0.0005 | 0.014 | 0.973 |
| WMD a | 1.137(0.957~1.352) | 0.145 | |||||||
| IVW | 1.196(1.045~1.368) | 0.0009 | IVW | 5.215 | 1 | ||||
| WMO b | 1.061(0.740~1.521) | 0.748 | |||||||
| Hypertension | MR-Egger | 1.089(0.858~1.383) | 0.486 | MR-Egger | 4.436 | 1 | 0.002 | 0.008 | 0.787 |
| WMD a | 1.097(0.984~1.222) | 0.095 | |||||||
| IVW | 1.124(1.036~1.218) | 0.005 | IVW | 4.510 | 1 | ||||
| WMO b | 1.095(0.872~1.375) | 0.437 | |||||||
| Dyslipidemia | MR-Egger | 1.236(0.833~1.835) | 0.298 | MR-Egger | 3.878 | 1 | −0.002 | 0.014 | 0.899 |
| WMD a | 1.151(0.966~1.373) | 0.116 | |||||||
| IVW | 1.206(1.055~1.379) | 0.006 | IVW | 3.894 | 1 | ||||
| WMO b | 1.105(0.743~1.644) | 0.624 | |||||||
| Exposures | Method | β (95% CI) | p | Method | Q | p-value | Intercept | SE | p-value |
| Serum triglyceride concentrations (mg/dL) | MR-Egger | 0.145(−0.181~0.471) | 0.387 | MR-Egger | 2.285 | 1 | −0.000089 | 0.011 | 0.994 |
| WMD a | 0.117(−0.022~0.257) | 0.100 | |||||||
| IVW | 0.144(0.033~0.255) | 0.011 | IVW | 2.285 | 1 | ||||
| WMO b | 0.103(−0.185~0.392) | 0.486 | |||||||
| Serum LDL concentrations (mg/dL) | MR-Egger | 0.119(−0.210~0.447) | 0.482 | MR-Egger | 3.301 | 1 | 0.0007 | 0.011 | 0.949 |
| WMD a | 0.107(−0.034~0.248) | 0.138 | |||||||
| IVW | 0.129(0.017~0.240) | 0.024 | IVW | 3.306 | 1 | ||||
| WMO b | 0.049(−0.249~0.346) | 0.750 | |||||||
| Serum HDL concentrations (mg/dL) | MR-Egger | 0.121(−0.105~0.346) | 0.300 | MR-Egger | 3.081 | 1 | −0.002 | 0.008 | 0.788 |
| WMD a | 0.080(−0.013~0.173) | 0.091 | |||||||
| IVW | 0.091(0.015~0.168) | 0.020 | IVW | 3.154 | 1 | ||||
| WMO b | 0.061(−0.147~0.269) | 0.569 | |||||||
| Serum glucose concentrations (mg/dL) | MR-Egger | 0.282(−0.084~0.648) | 0.138 | MR-Egger | 5.709 | 1 | −0.007 | 0.013 | 0.580 |
| WMD a | 0.141(−0.020~0.303) | 0.086 | |||||||
| IVW | 0.184(0.060~0.308) | 0.004 | IVW | 6.019 | 1 | ||||
| WMO b | 0.074(−0.237~0.386) | 0.642 | |||||||
| BMI | MR-Egger | 0.097(−0.119~0.313) | 0.384 | MR-Egger | 3.729 | 1 | 0.0007 | 0.007 | 0.922 |
| WMD a | 0.087(−0.005~0.180) | 0.064 | |||||||
| IVW | 0.107(0.034~0.180) | 0.004 | IVW | 3.739 | 1 | ||||
| WMO b | 0.068(−0.133~0.269) | 0.511 | |||||||
| Waist circumferences (cm) | MR-Egger | 0.208(−0.243~0.659) | 0.370 | MR-Egger | 2.479 | 1 | −0.001 | 0.016 | 0.945 |
| WMD a | 0.179(−0.012~0.370) | 0.066 | |||||||
| IVW | 0.193(0.039~0.347) | 0.014 | IVW | 2.484 | 1 | ||||
| WMO b | 0.136(−0.240~0.513) | 0.481 | |||||||
| Body fat | MR-Egger | 0.218(−0.222~0.658) | 0.337 | MR-Egger | 4.117 | 1 | −0.002 | 0.015 | 0.889 |
| WMD a | 0.151(−0.047~0.349) | 0.134 | |||||||
| IVW | 0.188(0.038~0.338) | 0.014 | IVW | 4.136 | 1 | ||||
| WMO b | 0.100(−0.303~0.502) | 0.630 | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Liu, M. A Positive Causal Relationship between Noodle Intake and Metabolic Syndrome: A Two-Sample Mendelian Randomization Study. Nutrients 2023, 15, 2091. https://doi.org/10.3390/nu15092091
Park S, Liu M. A Positive Causal Relationship between Noodle Intake and Metabolic Syndrome: A Two-Sample Mendelian Randomization Study. Nutrients. 2023; 15(9):2091. https://doi.org/10.3390/nu15092091
Chicago/Turabian StylePark, Sunmin, and Meiling Liu. 2023. "A Positive Causal Relationship between Noodle Intake and Metabolic Syndrome: A Two-Sample Mendelian Randomization Study" Nutrients 15, no. 9: 2091. https://doi.org/10.3390/nu15092091