
Age and Sex Differences in the Association between Serum Vitamin E Levels and Depressive Symptoms: Korea National Health and Nutrition Examination Survey

Abstract
:1. Introduction
2. Materials and Methods
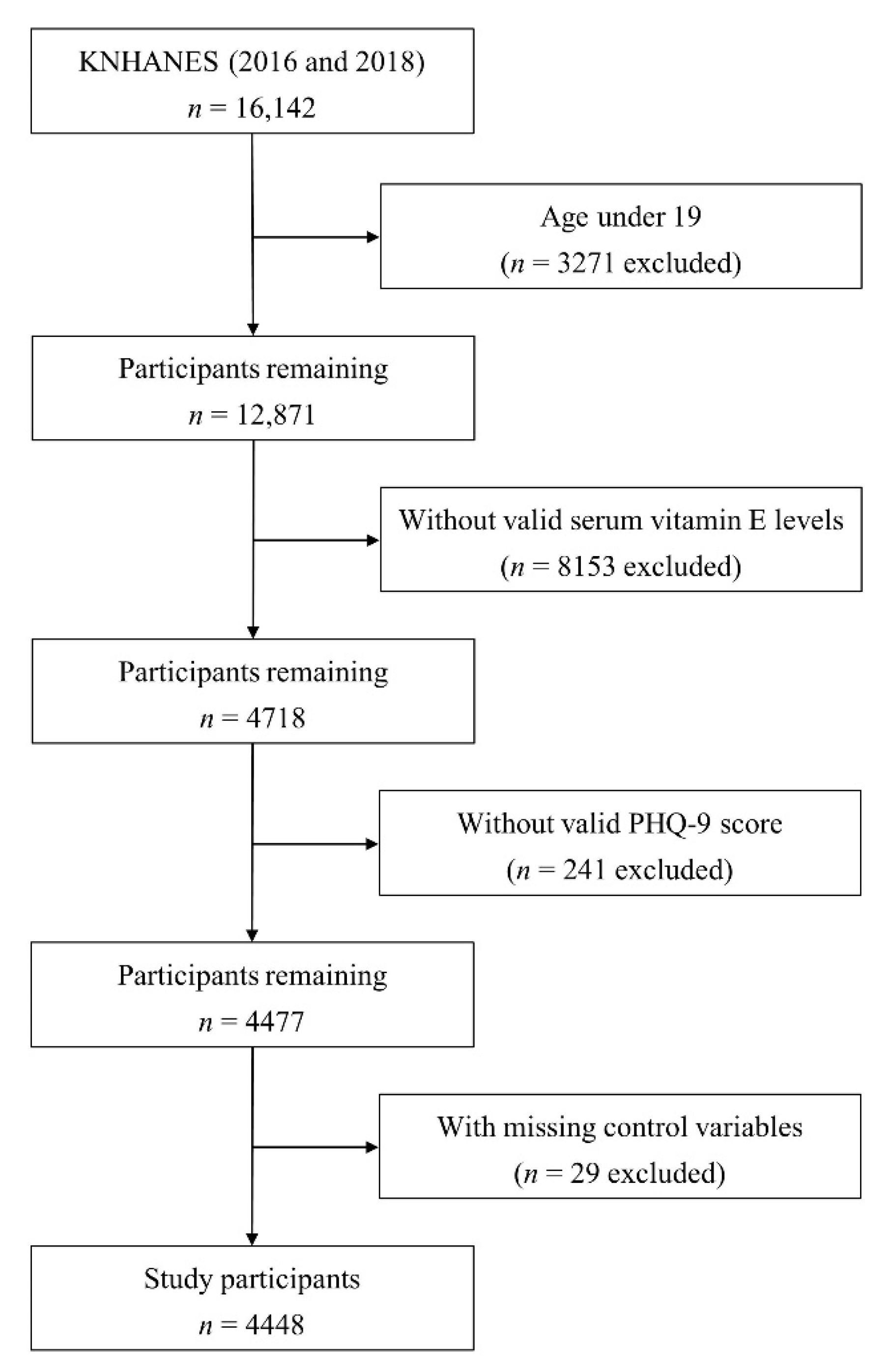
2.1. Participants
2.2. Measures
2.2.1. Patient Health Questionnaire-9
2.2.2. Serum Vitamin E Levels, Serum Lipid Levels, and Adjustment of Vitamin E Levels According to Total Lipid Levels
2.2.3. Covariates and Dietary Supplement Use Status
2.3. Statistical Analyses
3. Results
3.1. Participants’ Baseline Characteristics
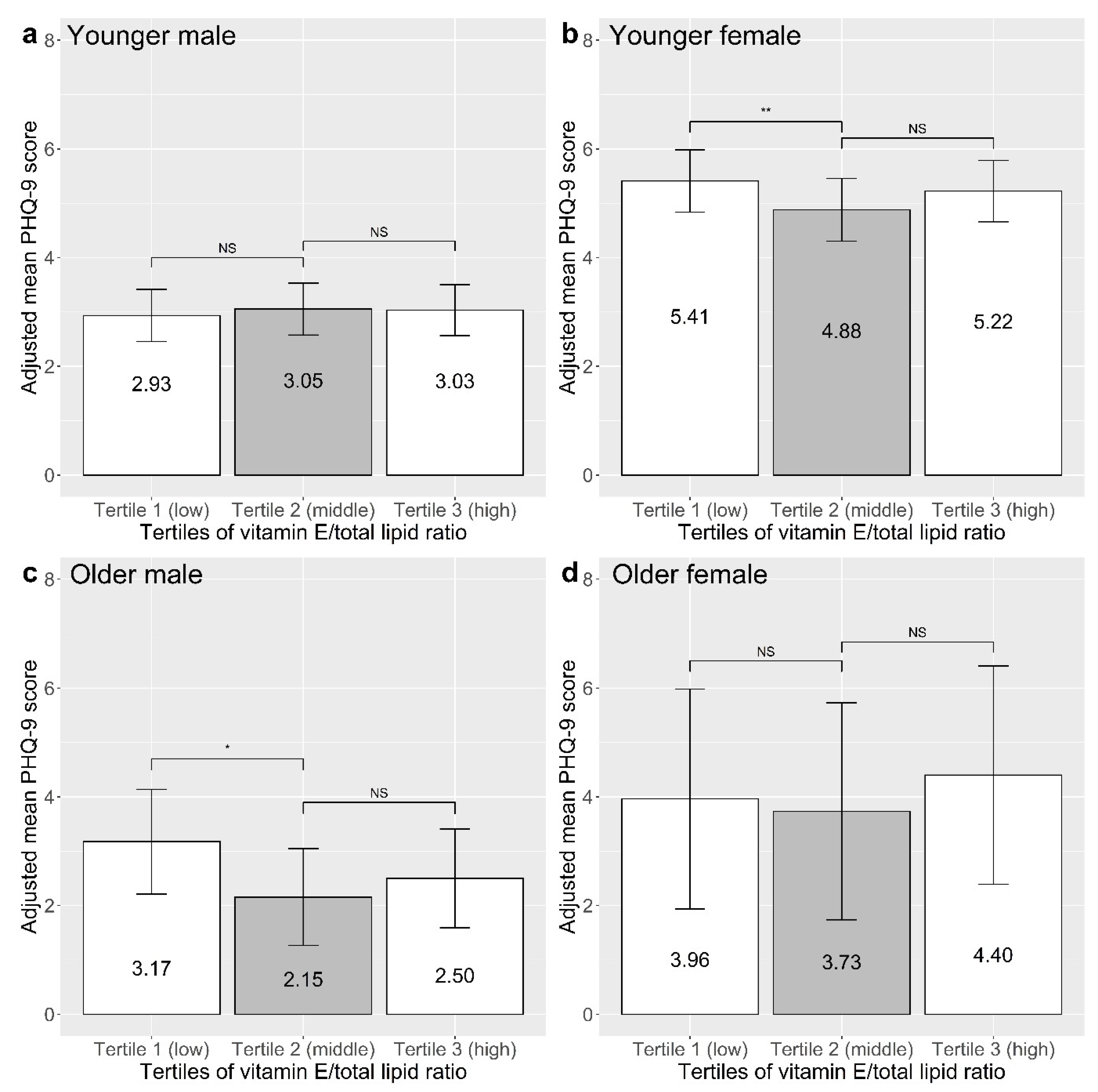
3.2. Association between Vitamin E/Total Lipid Ratio and Depressive Symptoms
3.3. Association between the Covariates and Depressive Symptoms
3.4. Association between Dietary Supplement Use and Vitamin E/Total Lipid Ratio
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Koo, S.K. Depression Status in Korea. Osong Public Health Res. Perspect. 2018, 9, 141–142. [Google Scholar] [CrossRef]
- Shin, C.; Kim, Y.; Park, S.; Yoon, S.; Ko, Y.H.; Kim, Y.K.; Kim, S.H.; Jeon, S.W.; Han, C. Prevalence and Associated Factors of Depression in General Population of Korea: Results from the Korea National Health and Nutrition Examination Survey, 2014. J. Korean Med. Sci. 2017, 32, 1861–1869. [Google Scholar] [CrossRef]
- Lépine, J.P.; Briley, M. The increasing burden of depression. Neuropsychiatr. Dis. Treat. 2011, 7, 3–7. [Google Scholar] [CrossRef] [Green Version]
- Na, Y.M.; Kim, K.S.; Lee, K.U.; Chae, J.H.; Kim, J.H.; Kim, D.J.; Bahk, W.M.; Jang, Y.S.; Lee, A.K.; Woo, Y.S.; et al. The relationship between depressive symptoms in outpatients with chronic illness and health care costs. Yonsei Med. J. 2007, 48, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Ayuso-Mateos, J.L.; Nuevo, R.; Verdes, E.; Naidoo, N.; Chatterji, S. From depressive symptoms to depressive disorders: The relevance of thresholds. Br. J. Psychiatry 2010, 196, 365–371. [Google Scholar] [CrossRef] [Green Version]
- Nagar, S. The Struggle of Mental Health Care Delivery in South Korea and Singapore. Harv. Int. Rev. 2022, 43, 39–43. [Google Scholar]
- Park, J.H.; Kim, K.W. A review of the epidemiology of depression in Korea. J. Korean Med. Assoc. 2011, 54, 362–369. [Google Scholar] [CrossRef] [Green Version]
- Ock, S.M.; Hwang, S.S.; Lee, J.S.; Song, C.H.; Ock, C.M. Dietary supplement use by South Korean adults: Data from the national complementary and alternative medicine use survey (NCAMUS) in 2006. Nutr. Res. Pract. 2010, 4, 69–74. [Google Scholar] [CrossRef] [Green Version]
- Park, H.A. Which types of dietary supplements are used in Korea? Data from the 2015 Korea National Health and Nutrition Examination Survey. Korean J. Health Promot. 2018, 18, 107–112. [Google Scholar] [CrossRef] [Green Version]
- Park, H.A. Top 10 dietary supplements of korean adults from the 4th Korea national health and nutrition examination survey. Korean J. Fam. Med. 2011, 32, 263–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.K.; Kim, S.Y.; Sok, S.R. Effects of Multivitamin Supplements on Cognitive Function, Serum Homocysteine Level, and Depression of Korean Older Adults With Mild Cognitive Impairment in Care Facilities. J. Nurs. Scholarsh. 2016, 48, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.; Kim, D.W.; Baek, Y.J.; Moon, S.H.; Jung, H.J.; Song, Y.J.; Paik, H.Y. Dietary supplement use and its effect on nutrient intake in Korean adult population in the Korea National Health and Nutrition Examination Survey IV (2007-2009) data. Eur. J. Clin. Nutr. 2014, 68, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Jun, S.; Chun, O.K.; Joung, H. Estimation of dietary total antioxidant capacity of Korean adults. Eur. J. Nutr. 2018, 57, 1615–1625. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Song, Y.; Lee, J.E.; Jun, S.; Shin, S.; Wie, G.A.; Cho, Y.H.; Joung, H. Total Antioxidant Capacity from Dietary Supplement Decreases the Likelihood of Having Metabolic Syndrome in Korean Adults. Nutrients 2017, 9, 1055. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.N.; Cho, Y.O. Vitamin E status of 20- to 59-year-old adults living in the Seoul metropolitan area of South Korea. Nutr. Res. Pract. 2015, 9, 192–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shim, J.S.; Kim, K.N.; Lee, J.S.; Yoon, M.O.; Lee, H.S. Dietary intake and major source foods of vitamin E among Koreans: Findings of the Korea National Health and Nutrition Examination Survey 2016–2019. Nutr. Res. Pract. 2022, 16, 616–627. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Park, Y.M.; Choi, B.Y.; Kim, M.K.; Roh, S.; Kim, K.; Yang, Y.J. Associations of serum levels of vitamins A, C, and E with the risk of cognitive impairment among elderly Koreans. Nutr. Res. Pract. 2018, 12, 160–165. [Google Scholar] [CrossRef] [Green Version]
- Saremi, A.; Arora, R. Vitamin E and cardiovascular disease. Am. J. Ther. 2010, 17, e56–e65. [Google Scholar] [CrossRef]
- Stolzenberg-Solomon, R.Z.; Sheffler-Collins, S.; Weinstein, S.; Garabrant, D.H.; Mannisto, S.; Taylor, P.; Virtamo, J.; Albanes, D. Vitamin E intake, alpha-tocopherol status, and pancreatic cancer in a cohort of male smokers. Am. J. Clin. Nutr. 2009, 89, 584–591. [Google Scholar] [CrossRef] [Green Version]
- Traber, M.G. Vitamin E inadequacy in humans: Causes and consequences. Adv. Nutr. 2014, 5, 503–514. [Google Scholar] [CrossRef] [Green Version]
- Manosso, L.M.; Camargo, A.; Dafre, A.L.; Rodrigues, A.L.S. Vitamin E for the management of major depressive disorder: Possible role of the anti-inflammatory and antioxidant systems. Nutr. Neurosci. 2022, 25, 1310–1324. [Google Scholar] [CrossRef] [PubMed]
- Yanik, M.; Erel, O.; Kati, M. The relationship between potency of oxidative stress and severity of depression. Acta Neuropsychiatr. 2004, 16, 200–203. [Google Scholar] [CrossRef] [PubMed]
- Tsuboi, H.; Shimoi, K.; Kinae, N.; Oguni, I.; Hori, R.; Kobayashi, F. Depressive symptoms are independently correlated with lipid peroxidation in a female population: Comparison with vitamins and carotenoids. J. Psychosom. Res. 2004, 56, 53–58. [Google Scholar] [CrossRef]
- Bajpai, A.; Verma, A.K.; Srivastava, M.; Srivastava, R. Oxidative stress and major depression. J. Clin. Diagn. Res. 2014, 8, CC04–CC07. [Google Scholar] [CrossRef] [PubMed]
- Dowlati, Y.; Herrmann, N.; Swardfager, W.; Liu, H.; Sham, L.; Reim, E.K.; Lanctôt, K.L. A meta-analysis of cytokines in major depression. Biol. Psychiatry 2010, 67, 446–457. [Google Scholar] [CrossRef]
- Haapakoski, R.; Mathieu, J.; Ebmeier, K.P.; Alenius, H.; Kivimäki, M. Cumulative meta-analysis of interleukins 6 and 1β, tumour necrosis factor α and C-reactive protein in patients with major depressive disorder. Brain Behav. Immun. 2015, 49, 206–215. [Google Scholar] [CrossRef] [Green Version]
- Tantavisut, S.; Tanavalee, A.; Honsawek, S.; Suantawee, T.; Ngarmukos, S.; Adisakwatana, S.; Callaghan, J.J. Effect of vitamin E on oxidative stress level in blood, synovial fluid, and synovial tissue in severe knee osteoarthritis: A randomized controlled study. BMC Musculoskelet. Disord. 2017, 18, 281. [Google Scholar] [CrossRef]
- Khatami, P.G.; Soleimani, A.; Sharifi, N.; Aghadavod, E.; Asemi, Z. The effects of high-dose vitamin E supplementation on biomarkers of kidney injury, inflammation, and oxidative stress in patients with diabetic nephropathy: A randomized, double-blind, placebo-controlled trial. J. Clin. Lipidol. 2016, 10, 922–929. [Google Scholar] [CrossRef]
- Seven, A.; Guzel, S.; Seymen, O.; Civelek, S.; Bolayirli, M.; Uncu, M.; Burcak, G. Effects of vitamin E supplementation on oxidative stress in streptozotocin induced diabetic rats: Investigation of liver and plasma. Yonsei Med. J. 2004, 45, 703–710. [Google Scholar] [CrossRef] [Green Version]
- Devaraj, S.; Tang, R.; Adams-Huet, B.; Harris, A.; Seenivasan, T.; de Lemos, J.A.; Jialal, I. Effect of high-dose alpha-tocopherol supplementation on biomarkers of oxidative stress and inflammation and carotid atherosclerosis in patients with coronary artery disease. Am. J. Clin. Nutr. 2007, 86, 1392–1398. [Google Scholar] [CrossRef] [Green Version]
- Devaraj, S.; Jialal, I. Alpha tocopherol supplementation decreases serum C-reactive protein and monocyte interleukin-6 levels in normal volunteers and type 2 diabetic patients. Free Radic. Biol. Med. 2000, 29, 790–792. [Google Scholar] [CrossRef] [PubMed]
- Pein, H.; Ville, A.; Pace, S.; Temml, V.; Garscha, U.; Raasch, M.; Alsabil, K.; Viault, G.; Dinh, C.P.; Guilet, D.; et al. Endogenous metabolites of vitamin E limit inflammation by targeting 5-lipoxygenase. Nat. Commun. 2018, 9, 3834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, J.; Zhang, Y. Associations of Dietary Vitamin C and E Intake With Depression. A Meta-Analysis of Observational Studies. Front. Nutr. 2022, 9, 857823. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Choi, J.Y.; Lee, H.H.; Park, Y. Associations between Dietary Pattern and Depression in Korean Adolescent Girls. J. Pediatr. Adolesc. Gynecol. 2015, 28, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.T.; Tsujiguchi, H.; Kambayashi, Y.; Hara, A.; Miyagi, S.; Yamada, Y.; Nakamura, H.; Shimizu, Y.; Hori, D.; Suzuki, F.; et al. Relationship between Vitamin Intake and Depressive Symptoms in Elderly Japanese Individuals: Differences with Gender and Body Mass Index. Nutrients 2017, 9, 1319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quo, Y.; Tseng, M.; Liu, C.; Huang, S. Dietary intake in patients with major depressive disorder-a pilot study. Nutr. Sci. J. 2010, 35, 34–45. [Google Scholar]
- Ravelli, M.N.; Schoeller, D.A. Traditional Self-Reported Dietary Instruments Are Prone to Inaccuracies and New Approaches Are Needed. Front. Nutr. 2020, 7, 90. [Google Scholar] [CrossRef]
- Banna, J.C.; Fialkowski, M.K.; Townsend, M.S. Misreporting of dietary intake affects estimated nutrient intakes in low-income Spanish-speaking women. J. Acad. Nutr. Diet. 2015, 115, 1124–1133. [Google Scholar] [CrossRef] [Green Version]
- Shibata, H.; Kumagai, S.; Watanabe, S.; Suzuki, T. Relationship of serum cholesterols and vitamin E to depressive status in the elderly. J. Epidemiol. 1999, 9, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Beydoun, M.A.; Beydoun, H.A.; Boueiz, A.; Shroff, M.R.; Zonderman, A.B. Antioxidant status and its association with elevated depressive symptoms among US adults: National Health and Nutrition Examination Surveys 2005–6. Br. J. Nutr. 2013, 109, 1714–1729. [Google Scholar] [CrossRef] [Green Version]
- Maes, M.; De Vos, N.; Pioli, R.; Demedts, P.; Wauters, A.; Neels, H.; Christophe, A. Lower serum vitamin E concentrations in major depression. Another marker of lowered antioxidant defenses in that illness. J. Affect. Disord. 2000, 58, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Owen, A.J.; Batterham, M.J.; Probst, Y.C.; Grenyer, B.F.; Tapsell, L.C. Low plasma vitamin E levels in major depression: Diet or disease? Eur. J. Clin. Nutr. 2005, 59, 304–306. [Google Scholar] [CrossRef] [Green Version]
- Al-Fartusie, F.S.; Al-Bairmani, H.K.; Al-Garawi, Z.S.; Yousif, A.H. Evaluation of Some Trace Elements and Vitamins in Major Depressive Disorder Patients: A Case-Control Study. Biol. Trace Elem. Res. 2019, 189, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Fiske, A.; Wetherell, J.L.; Gatz, M. Depression in older adults. Annu. Rev. Clin. Psychol. 2009, 5, 363–389. [Google Scholar] [CrossRef] [PubMed]
- Tsuboi, H.; Watanabe, M.; Kobayashi, F.; Kimura, K.; Kinae, N. Associations of depressive symptoms with serum proportions of palmitic and arachidonic acids, and α-tocopherol effects among male population—A preliminary study. Clin. Nutr. 2013, 32, 289–293. [Google Scholar] [CrossRef]
- Tiemeier, H.; Hofman, A.; Kiliaan, A.J.; Meijer, J.; Breteler, M.M. Vitamin E and depressive symptoms are not related. The Rotterdam Study. J. Affect. Disord. 2002, 72, 79–83. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994; p. xxvii, 886. [Google Scholar]
- Minović, I.; Sotomayor, C.; Eggersdorfer, M.; Riphagen, I.; Borst, M.H.; Dekker, L.; Navis, G.; Nolte, I.; Van Zon, S.; Reijneveld, S.A.; et al. Vitamin E Serum Levels and the Challenge to Correct for Lipids: Accounting for the Usual Double Correction for Variance Shared by Total Cholesterol and Fasting Triglycerides Reveals New Insights into the Association with the One-Carbon Pathway. In Vitamin E in Human Health; Humana Press: Cham, Switzerland, 2019; pp. 201–214. [Google Scholar] [CrossRef]
- Biesalski, H.K. Vitamin E requirements in parenteral nutrition. Gastroenterology 2009, 137, S92–S104. [Google Scholar] [CrossRef]
- Johnson, L.E. Vitamin E Deficiency. Available online: https://www.msdmanuals.com/professional/nutritional-disorders/vitamin-deficiency,-dependency,-and-toxicity/vitamin-e-deficiency (accessed on 25 January 2023).
- Phillips, D.L.; Pirkle, J.L.; Burse, V.W.; Bernert, J.T., Jr.; Henderson, L.O.; Needham, L.L. Chlorinated hydrocarbon levels in human serum: Effects of fasting and feeding. Arch. Environ. Contam. Toxicol. 1989, 18, 495–500. [Google Scholar] [CrossRef]
- Bernert, J.T.; Turner, W.E.; Patterson, D.G.; Needham, L.L. Calculation of serum “total lipid” concentrations for the adjustment of persistent organohalogen toxicant measurements in human samples. Chemosphere 2007, 68, 824–831. [Google Scholar] [CrossRef]
- Lorant, V.; Deliège, D.; Eaton, W.; Robert, A.; Philippot, P.; Ansseau, M. Socioeconomic inequalities in depression: A meta-analysis. Am. J. Epidemiol. 2003, 157, 98–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Probst, J.C.; Laditka, S.B.; Moore, C.G.; Harun, N.; Powell, M.P.; Baxley, E.G. Rural-urban differences in depression prevalence: Implications for family medicine. Fam. Med. 2006, 38, 653–660. [Google Scholar] [PubMed]
- Wu, D.; Liu, F.; Huang, S. Assessment of the relationship between living alone and the risk of depression based on longitudinal studies: A systematic review and meta-analysis. Front. Psychiatry 2022, 13, 954857. [Google Scholar] [CrossRef]
- Boden, J.M.; Fergusson, D.M. Alcohol and depression. Addiction 2011, 106, 906–914. [Google Scholar] [CrossRef] [PubMed]
- Fluharty, M.; Taylor, A.E.; Grabski, M.; Munafò, M.R. The Association of Cigarette Smoking With Depression and Anxiety: A Systematic Review. Nicotine Tob. Res. 2017, 19, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Katon, W.J. Epidemiology and treatment of depression in patients with chronic medical illness. Dialogues Clin. Neurosci. 2011, 13, 7–23. [Google Scholar] [CrossRef] [PubMed]
- Pearce, M.; Garcia, L.; Abbas, A.; Strain, T.; Schuch, F.B.; Golubic, R.; Kelly, P.; Khan, S.; Utukuri, M.; Laird, Y.; et al. Association Between Physical Activity and Risk of Depression: A Systematic Review and Meta-analysis. JAMA Psychiatry 2022, 79, 550–559. [Google Scholar] [CrossRef]
- Jantaratnotai, N.; Mosikanon, K.; Lee, Y.; McIntyre, R.S. The interface of depression and obesity. Obes. Res. Clin. Pract. 2017, 11, 1–10. [Google Scholar] [CrossRef]
- Armstrong, T.; Bull, F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J. Public. Health 2006, 14, 66–70. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sport. Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- World Health Organization. Global Physical Activity Questionnaire Analysis Guide; Prevention of Noncommunicable Diseases Department, Ed.; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Rodda, J.; Walker, Z.; Carter, J. Depression in older adults. Bmj 2011, 343, d5219. [Google Scholar] [CrossRef]
- Malik, A.; Eggersdorfer, M.; Trilok-Kumar, G. Vitamin E status in healthy population in Asia: A review of current literature. Int. J. Vitam. Nutr. Res. 2021, 91, 356–369. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Xu, W.; Wu, Q.; Zheng, H.; Li, Y. Ascorbic acid intake is inversely associated with prevalence of depressive symptoms in US midlife women: A cross-sectional study. J. Affect. Disord. 2022, 299, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Kong, Z.; Song, Y.; Liu, J.; Wang, X. The validity and reliability of the PHQ-9 on screening of depression in neurology: A cross sectional study. BMC Psychiatry 2022, 22, 98. [Google Scholar] [CrossRef] [PubMed]
- Sobotka, R.; Čapoun, O.; Kalousová, M.; Hanuš, T.; Zima, T.; Koštířová, M.; Soukup, V. Prognostic Importance of Vitamins A, E and Retinol-binding Protein 4 in Renal Cell Carcinoma Patients. Anticancer Res. 2017, 37, 3801–3806. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014. [Google Scholar]
- Bauer-Staeb, C.; Kounali, D.Z.; Welton, N.J.; Griffith, E.; Wiles, N.J.; Lewis, G.; Faraway, J.J.; Button, K.S. Effective dose 50 method as the minimal clinically important difference: Evidence from depression trials. J. Clin. Epidemiol. 2021, 137, 200–208. [Google Scholar] [CrossRef]
- Razmara, A.; Duckles, S.P.; Krause, D.N.; Procaccio, V. Estrogen suppresses brain mitochondrial oxidative stress in female and male rats. Brain Res. 2007, 1176, 71–81. [Google Scholar] [CrossRef] [Green Version]
- Son, S.W.; Lee, J.S.; Kim, H.G.; Kim, D.W.; Ahn, Y.C.; Son, C.G. Testosterone depletion increases the susceptibility of brain tissue to oxidative damage in a restraint stress mouse model. J. Neurochem. 2016, 136, 106–117. [Google Scholar] [CrossRef] [Green Version]
- Duong, P.; Tenkorang, M.A.A.; Trieu, J.; McCuiston, C.; Rybalchenko, N.; Cunningham, R.L. Neuroprotective and neurotoxic outcomes of androgens and estrogens in an oxidative stress environment. Biol. Sex. Differ. 2020, 11, 12. [Google Scholar] [CrossRef]
- Hartman, T.J.; Dorgan, J.F.; Virtamo, J.; Tangrea, J.A.; Taylor, P.R.; Albanes, D. Association between serum alpha-tocopherol and serum androgens and estrogens in older men. Nutr. Cancer 1999, 35, 10–15. [Google Scholar] [CrossRef]
- Mondul, A.M.; Rohrmann, S.; Menke, A.; Feinleib, M.; Nelson, W.G.; Platz, E.A.; Albanes, D. Association of serum α-tocopherol with sex steroid hormones and interactions with smoking: Implications for prostate cancer risk. Cancer Causes Control. 2011, 22, 827–836. [Google Scholar] [CrossRef] [Green Version]
- Mumford, S.L.; Browne, R.W.; Schliep, K.C.; Schmelzer, J.; Plowden, T.C.; Michels, K.A.; Sjaarda, L.A.; Zarek, S.M.; Perkins, N.J.; Messer, L.C.; et al. Serum Antioxidants Are Associated with Serum Reproductive Hormones and Ovulation among Healthy Women. J. Nutr. 2016, 146, 98–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, P.Y.; Beilin, J.; Meier, C.; Nguyen, T.V.; Center, J.R.; Leedman, P.J.; Seibel, M.J.; Eisman, J.A.; Handelsman, D.J. Age-related changes in serum testosterone and sex hormone binding globulin in Australian men: Longitudinal analyses of two geographically separate regional cohorts. J. Clin. Endocrinol. Metab. 2007, 92, 3599–3603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minkin, M.J. Menopause: Hormones, Lifestyle, and Optimizing Aging. Obstet. Gynecol. Clin. N. Am. 2019, 46, 501–514. [Google Scholar] [CrossRef]
- Pearson, P.; Lewis, S.A.; Britton, J.; Young, I.S.; Fogarty, A. The pro-oxidant activity of high-dose vitamin E supplements in vivo. BioDrugs 2006, 20, 271–273. [Google Scholar] [CrossRef] [PubMed]
- Winterbone, M.S.; Sampson, M.J.; Saha, S.; Hughes, J.C.; Hughes, D.A. Pro-oxidant effect of alpha-tocopherol in patients with type 2 diabetes after an oral glucose tolerance test—A randomised controlled trial. Cardiovasc. Diabetol. 2007, 6, 8. [Google Scholar] [CrossRef] [Green Version]
- Huang, A.A.; Huang, S.Y. Quantification of the Effect of Vitamin E Intake on Depressive Symptoms in United States Adults Using Restricted Cubic Splines. Curr. Dev. Nutr. 2023, 7, 100038. [Google Scholar] [CrossRef]
- Lee, A.; Tariq, A.; Lau, G.; Tok, N.W.K.; Tam, W.W.S.; Ho, C.S.H. Vitamin E, Alpha-Tocopherol, and Its Effects on Depression and Anxiety: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 656. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Younger Participants (Age < 65) | Older Participants (Age ≥ 65) | ||||
|---|---|---|---|---|---|
| Younger Males (n = 1551) | Younger Females (n = 1986) | Older Males (n = 432) | Older Females (n = 479) | p-Value | |
| Vitamin E, lipids, and PHQ-9 score | |||||
| Vitamin E (mg/L) | 13.16 a (4.71) | 13.21 a (4.25) | 13.10 a (4.98) | 15.04 b (6.94) | <0.001 |
| Total cholesterol (mg/dL) | 192.80 ac (36.28) | 194.61 a (36.36) | 178.95 b (38.61) | 189.35 c (39.31) | <0.001 |
| Triglyceride (mg/dL) | 169.94 a (157.67) | 108.87 b (74.42) | 139.25 c (80.32) | 139.34 c (83.84) | <0.001 |
| Total lipid (mg/dL) | 669.91 a (201.51) | 612.93 b (124.54) | 607.76 b (134.74) | 631.48 c (132.89) | <0.001 |
| Vitamin E/total lipid ratio (mg/g) | 1.99 a (0.54) | 2.16 b (0.56) | 2.16 b (0.66) | 2.38 c (0.85) | <0.001 |
| PHQ-9 score | 1.99 a (3.12) | 2.87 b (3.74) | 2.11 a (3.63) | 3.43 b (4.68) | <0.001 |
| Sociodemographic variables | |||||
| Educational attainment | <0.001 | ||||
| Elementary school or below | 86 (5.5) | 170 (8.6) | 175 (40.5) | 334 (69.7) | |
| Middle school | 106 (6.8) | 188 (9.5) | 72 (16.7) | 75 (15.7) | |
| High school | 580 (37.4) | 741 (37.3) | 125 (28.9) | 48 (10.0) | |
| University or above | 779 (50.2) | 887 (44.7) | 60 (13.9) | 22 (4.6) | |
| Equalized household income | <0.001 | ||||
| Quartile 1 (low) | 130 (8.4) | 183 (9.2) | 181 (41.9) | 244 (50.9) | |
| Quartile 2 | 368 (23.7) | 477 (24.0) | 119 (27.6) | 130 (27.1) | |
| Quartile 3 | 498 (32.1) | 647 (32.6) | 75 (17.4) | 67 (14.0) | |
| Quartile 4 (high) | 555 (35.8) | 679 (34.2) | 57 (13.2) | 38 (7.9) | |
| Residential area | <0.001 | ||||
| Urban | 1303 (84.0) | 1688 (85.0) | 326 (75.5) | 357 (74.5) | |
| Rural | 248 (16.0) | 298 (15.0) | 106 (24.5) | 122 (25.5) | |
| Living situation | <0.001 | ||||
| Lives alone | 150 (9.7) | 146 (7.4) | 63 (14.6) | 144 (30.1) | |
| Lives with other household member(s) | 1401 (90.3) | 1840 (92.7) | 369 (85.4) | 335 (69.9) | |
| Clinical variables | |||||
| Alcohol use status | <0.001 | ||||
| No | 392 (25.3) | 1013 (51.0) | 185 (42.8) | 399 (83.3) | |
| Yes | 1159 (74.7) | 973 (49.0) | 247 (57.2) | 80 (16.7) | |
| Smoking status | <0.001 | ||||
| Non-smoker | 982 (63.3) | 1886 (95.0) | 361 (83.6) | 470 (98.1) | |
| Smoker | 569 (36.7) | 100 (5.0) | 71 (16.4) | 9 (1.9) | |
| Chronic medical disease | <0.001 | ||||
| None | 1197 (77.2) | 1557 (78.4) | 134 (31.0) | 90 (18.8) | |
| One | 258 (16.6) | 326 (16.4) | 173 (40.1) | 171 (35.7) | |
| Two or more | 96 (6.2) | 103 (5.2) | 125 (28.9) | 218 (45.5) | |
| Physical activity | <0.001 | ||||
| Inadequate | 770 (49.7) | 1076 (54.2) | 248 (57.4) | 346 (72.2) | |
| Adequate | 781 (50.4) | 910 (45.8) | 184 (42.6) | 133 (27.8) | |
| BMI | <0.001 | ||||
| Underweight | 36 (2.3) | 109 (5.5) | 16 (3.7) | 7 (1.5) | |
| Normal weight | 466 (30.1) | 991 (49.9) | 154 (35.7) | 144 (30.1) | |
| Overweight | 393 (25.3) | 383 (19.3) | 112 (25.9) | 132 (27.6) | |
| Obesity | 656 (42.3) | 503 (25.3) | 150 (34.7) | 196 (40.9) | |
| PHQ-9 Score | ||||
|---|---|---|---|---|
| Vitamin E/Total Lipid Ratio | Model 1 | Model 2 | ||
| β | p-Value | β | p-Value | |
| Younger participants (Age < 65) | ||||
| Younger males | ||||
| Tertile 1 (low) | 0.01 | 0.834 | −0.02 | 0.522 |
| Tertile 2 (middle) | Ref | Ref | ||
| Tertile 3 (high) | −0.01 | 0.668 | 0.00 | 0.911 |
| Younger females | ||||
| Tertile 1 (low) | 0.08 | 0.004 | 0.07 | 0.008 |
| Tertile 2 (middle) | Ref | Ref | ||
| Tertile 3 (high) | 0.05 | 0.056 | 0.04 | 0.086 |
| Older participants (Age ≥ 65) | ||||
| Older males | ||||
| Tertile 1 (low) | 0.16 | 0.004 | 0.13 | 0.018 |
| Tertile 2 (middle) | Ref | Ref | ||
| Tertile 3 (high) | 0.06 | 0.281 | 0.04 | 0.416 |
| Older females | ||||
| Tertile 1 (low) | 0.05 | 0.349 | 0.02 | 0.667 |
| Tertile 2 (middle) | Ref | Ref | ||
| Tertile 3 (high) | 0.09 | 0.102 | 0.07 | 0.202 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, H.; Oh, J.W.; Son, N.-H.; Lee, S. Age and Sex Differences in the Association between Serum Vitamin E Levels and Depressive Symptoms: Korea National Health and Nutrition Examination Survey. Nutrients 2023, 15, 1915. https://doi.org/10.3390/nu15081915
Jeong H, Oh JW, Son N-H, Lee S. Age and Sex Differences in the Association between Serum Vitamin E Levels and Depressive Symptoms: Korea National Health and Nutrition Examination Survey. Nutrients. 2023; 15(8):1915. https://doi.org/10.3390/nu15081915
Chicago/Turabian StyleJeong, Hyunwoo, Jae Won Oh, Nak-Hoon Son, and San Lee. 2023. "Age and Sex Differences in the Association between Serum Vitamin E Levels and Depressive Symptoms: Korea National Health and Nutrition Examination Survey" Nutrients 15, no. 8: 1915. https://doi.org/10.3390/nu15081915