
Berry Dietary Interventions in Metabolic Syndrome: New Insights

 ,
,  , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction and Analysis
2.4. Risk of Bias
3. Results
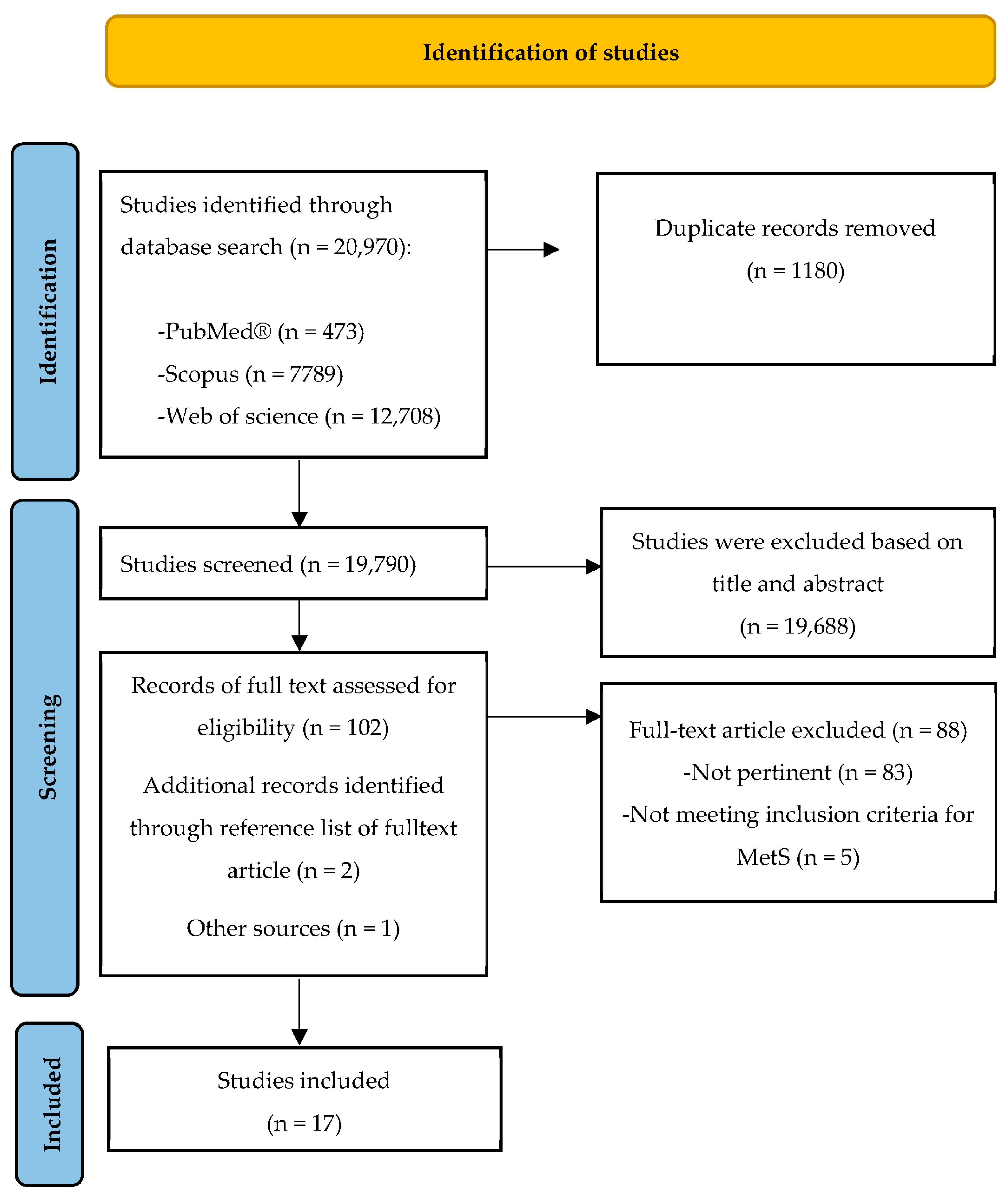
3.1. Study Selection
3.2. Study Characteristics and Main Findings
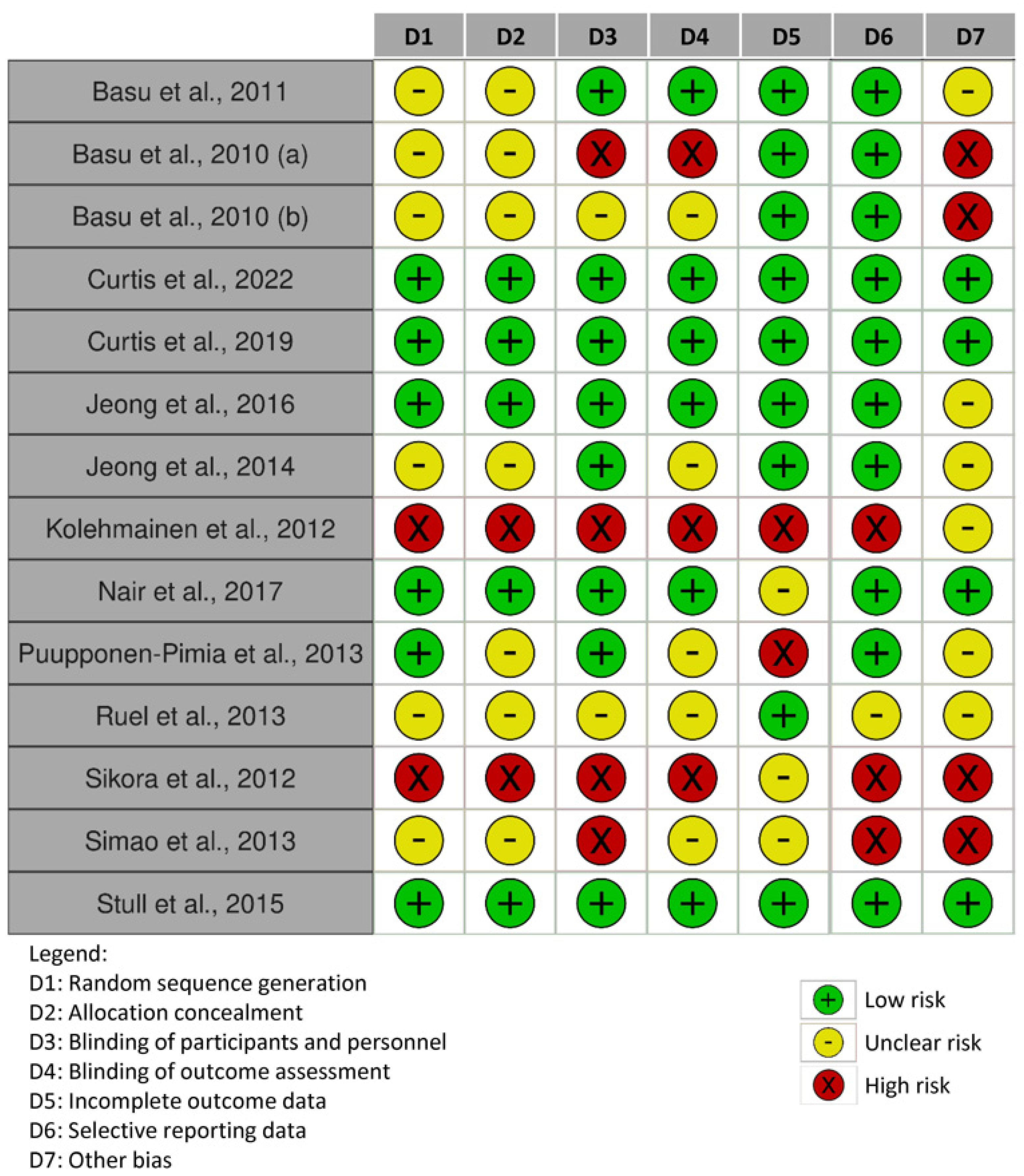
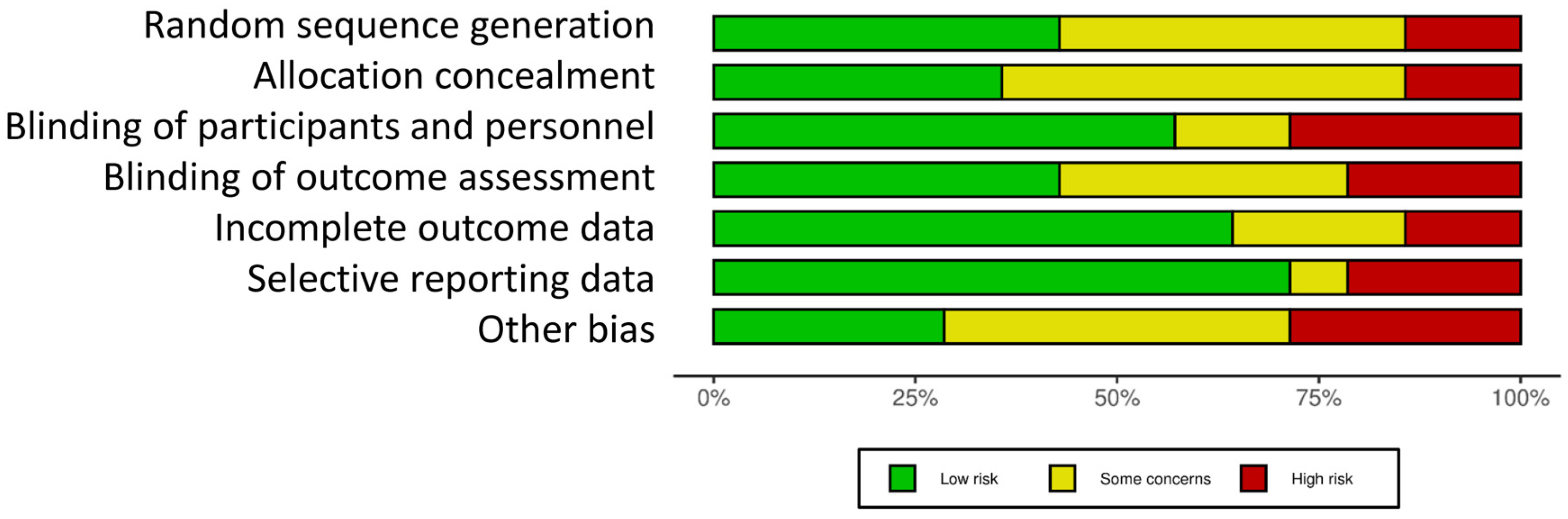
3.3. Risk of Bias
3.4. Main Findings
3.4.1. Effect of Blueberry (BB)
3.4.2. Effect of Bilberry (BiB)
3.4.3. Effect of Cranberry (CB)
3.4.4. Effect of Raspberry (RB)
3.4.5. Effect of Strawberry (StrB)
3.4.6. Effect of Chokeberry (ChB)
3.4.7. Effect of Berry Mix
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Scuteri, A.; Laurent, S.; Cucca, F.; Cockcroft, J.; Cunha, P.G.; Mañas, L.R.; Raso, F.U.M.; Muiesan, M.L.; Ryliškytė, L.; Rietzschel, E.; et al. Metabolic Syndrome across Europe: Different Clusters of Risk Factors. Eur. J. Prev. Cardiol. 2015, 22, 486–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsson, P.M.; Tuomilehto, J.; Rydén, L. The Metabolic Syndrome—What Is It and How Should It Be Managed? Eur. J. Prev. Cardiol. 2019, 26, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Vendrame, S.; Del Bo’, C.; Ciappellano, S.; Riso, P.; Klimis-Zacas, D. Berry Fruit Consumption and Metabolic Syndrome. Antioxidants 2016, 5, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the Metabolic Syndrome. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [Green Version]
- Nair, A.R.; Mariappan, N.; Stull, A.J.; Francis, J. Blueberry Supplementation Attenuates Oxidative Stress within Monocytes and Modulates Immune Cell Levels in Adults with Metabolic Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial. Food Funct. 2017, 8, 4118–4128. [Google Scholar] [CrossRef]
- Hirode, G.; Wong, R.J. Trends in the Prevalence of Metabolic Syndrome in the United States, 2011–2016. JAMA 2020, 323, 2526–2528. [Google Scholar] [CrossRef]
- Liang, X.P.; Or, C.Y.; Tsoi, M.F.; Cheung, C.L.; Cheung, B.M.Y. Prevalence of Metabolic Syndrome in the United States National Health and Nutrition Examination Survey (Nhanes) 2011–2018. Eur. Heart. J. 2021, 42, ehab724.2420. [Google Scholar] [CrossRef]
- Noubiap, J.J.; Nansseu, J.R.; Lontchi-Yimagou, E.; Nkeck, J.R.; Nyaga, U.F.; Ngouo, A.T.; Tounouga, D.N.; Tianyi, F.-L.; Foka, A.J.; Ndoadoumgue, A.L.; et al. Geographic Distribution of Metabolic Syndrome and Its Components in the General Adult Population: A Meta-Analysis of Global Data from 28 Million Individuals. Diabetes Res. Clin. Pract. 2022, 188, 109924. [Google Scholar] [CrossRef]
- Picasso, M.C.; Lo-Tayraco, J.A.; Ramos-Villanueva, J.M.; Pasupuleti, V.; Hernandez, A.V. Effect of Vegetarian Diets on the Presentation of Metabolic Syndrome or Its Components: A Systematic Review and Meta-Analysis. Clin. Nutr. 2019, 38, 1117–1132. [Google Scholar] [CrossRef] [Green Version]
- Dayi, T.; Ozgoren, M. Effects of the Mediterranean Diet on the Components of Metabolic Syndrome. J. Prev. Med. Hyg. 2022, 63, E56–E64. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Guasch-Ferré, M.; Lee, C.-H.; Estruch, R.; Clish, C.B.; Ros, E. Protective Effects of the Mediterranean Diet on Type 2 Diabetes and Metabolic Syndrome. J. Nutr. 2016, 146, S920–S927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Monforte, M.; Sánchez, E.; Barrio, F.; Costa, B.; Flores-Mateo, G. Metabolic Syndrome and Dietary Patterns: A Systematic Review and Meta-Analysis of Observational Studies. Eur. J. Nutr. 2017, 56, 925–947. [Google Scholar] [CrossRef] [PubMed]
- Basu, A. Role of Berry Bioactive Compounds on Lipids and Lipoproteins in Diabetes and Metabolic Syndrome. Nutrients 2019, 11, 1983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowalska, K.; Olejnik, A. Current Evidence on the Health-Beneficial Effects of Berry Fruits in the Prevention and Treatment of Metabolic Syndrome. Curr. Opin. Clin. Nutr. Metab. Care. 2016, 19, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Wilken, M.R.; Lambert, M.N.T.; Christensen, C.B.; Jeppesen, P.B. Effects of Anthocyanin-Rich Berries on the Risk of Metabolic Syndrome: A Systematic Review and Meta-Analysis. Rev. Diabet. Stud. 2022, 18, 42–57. [Google Scholar] [CrossRef]
- Cosme, F.; Pinto, T.; Aires, A.; Morais, M.C.; Bacelar, E.; Anjos, R.; Ferreira-Cardoso, J.; Oliveira, I.; Vilela, A.; Gonçalves, B. Red Fruits Composition and Their Health Benefits—A Review. Foods 2022, 11, 644. [Google Scholar] [CrossRef]
- Golovinskaia, O.; Wang, C.-K. Review of Functional and Pharmacological Activities of Berries. Molecules 2021, 26, 3904. [Google Scholar] [CrossRef]
- Jennings, A.; Welch, A.A.; Spector, T.; Macgregor, A.; Cassidy, A. Intakes of Anthocyanins and Flavones Are Associated with Biomarkers of Insulin Resistance and Inflammation in Women. J. Nutr. 2014, 144, 202–208. [Google Scholar] [CrossRef] [Green Version]
- Wedick, N.M.; Pan, A.; Cassidy, A.; Rimm, E.B.; Sampson, L.; Rosner, B.; Willett, W.; Hu, F.B.; Sun, Q.; van Dam, R.M. Dietary Flavonoid Intakes and Risk of Type 2 Diabetes in US Men and Women. Am. J. Clin. Nutr. 2012, 95, 925–933. [Google Scholar] [CrossRef] [Green Version]
- Cassidy, A.; Mukamal, K.J.; Liu, L.; Franz, M.; Eliassen, A.H.; Rimm, E.B. High Anthocyanin Intake Is Associated With a Reduced Risk of Myocardial Infarction in Young and Middle-Aged Women. Circulation 2013, 127, 188–196. [Google Scholar] [CrossRef] [Green Version]
- Kimble, R.; Keane, K.M.; Lodge, J.K.; Howatson, G. Dietary Intake of Anthocyanins and Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. Crit. Rev. Food Sci. Nutr. 2019, 59, 3032–3043. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Tian, Z.; Chen, H.; Zhao, Y.; Yang, Y. Anthocyanins, Anthocyanin-Rich Berries, and Cardiovascular Risks: Systematic Review and Meta-Analysis of 44 Randomized Controlled Trials and 15 Prospective Cohort Studies. Front. Nutr. 2021, 8, 2021. [Google Scholar] [CrossRef] [PubMed]
- Zurbau, A.; Au-Yeung, F.; Blanco Mejia, S.; Khan, T.A.; Vuksan, V.; Jovanovski, E.; Leiter, L.A.; Kendall, C.W.C.; Jenkins, D.J.A.; Sievenpiper, J.L. Relation of Different Fruit and Vegetable Sources With Incident Cardiovascular Outcomes: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. J. Am. Heart. Assoc. 2020, 9, e017728. [Google Scholar] [CrossRef] [PubMed]
- Marino, M.; Del Bo′, C.; Tucci, M.; Venturi, S.; Mantegazza, G.; Taverniti, V.; Møller, P.; Riso, P.; Porrini, M. A Mix of Chlorogenic and Caffeic Acid Reduces C/EBPß and PPAR-Γ1 Levels and Counteracts Lipid Accumulation in Macrophages. Eur. J. Nutr. 2022, 61, 1003–1014. [Google Scholar] [CrossRef] [PubMed]
- Najjar, R.S.; Mu, S.; Feresin, R.G. Blueberry Polyphenols Increase Nitric Oxide and Attenuate Angiotensin II-Induced Oxidative Stress and Inflammatory Signaling in Human Aortic Endothelial Cells. Antioxidants 2022, 11, 616. [Google Scholar] [CrossRef]
- Bouyahya, A.; EI Omari, N.; EL Hachlafi, N.; EI Jemly, M.; Hakkour, M.; Balahbib, A.; EI Menyiy, N.; Bakrim, S.; Naceiri Mrabti, H.; Khouchlaa, A.; et al. Chemical Compounds of Berry-Derived Polyphenols and Their Effects on Gut Microbiota, Inflammation, and Cancer. Molecules 2022, 27, 3286. [Google Scholar] [CrossRef]
- Xie, C.; Kang, J.; Ferguson, M.E.; Nagarajan, S.; Badger, T.M.; Wu, X. Blueberries Reduce Pro-Inflammatory Cytokine TNF-α and IL-6 Production in Mouse Macrophages by Inhibiting NF-ΚB Activation and the MAPK Pathway. Mol. Nutr. Food Res. 2011, 55, 1587–1591. [Google Scholar] [CrossRef]
- Mozos, I.; Flangea, C.; Vlad, D.C.; Gug, C.; Mozos, C.; Stoian, D.; Luca, C.T.; Horbańczuk, J.O.; Horbańczuk, O.K.; Atanasov, A.G. Effects of Anthocyanins on Vascular Health. Biomolecules 2021, 11, 811. [Google Scholar] [CrossRef]
- Rambaran, T.F.; Bergman, J.; Nordström, P.; Nordström, A. Effect of Berry Polyphenols on Glucose Metabolism: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Curr. Dev. Nutr. 2020, 4, 4007003. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curtis, P.J.; Berends, L.; van der Velpen, V.; Jennings, A.; Haag, L.; Chandra, P.; Kay, C.D.; Rimm, E.B.; Cassidy, A. Blueberry Anthocyanin Intake Attenuates the Postprandial Cardiometabolic Effect of an Energy-Dense Food Challenge: Results from a Double Blind, Randomized Controlled Trial in Metabolic Syndrome Participants. Clin. Nutr. 2022, 41, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Curtis, P.J.; van der Velpen, V.; Berends, L.; Jennings, A.; Feelisch, M.; Umpleby, A.M.; Evans, M.; Fernandez, B.O.; Meiss, M.S.; Minnion, M.; et al. Blueberries Improve Biomarkers of Cardiometabolic Function in Participants with Metabolic Syndrome—Results from a 6-Month, Double-Blind, Randomized Controlled Trial. Am. J. Clin. Nutr. 2019, 109, 1535–1545. [Google Scholar] [CrossRef] [Green Version]
- Sobolev, A.P.; Ciampa, A.; Ingallina, C.; Mannina, L.; Capitani, D.; Ernesti, I.; Maggi, E.; Businaro, R.; Ben, M.; Engel, P.; et al. Blueberry-Based Meals for Obese Patients with Metabolic Syndrome: A Multidisciplinary Metabolomic Pilot Study. Metabolites 2019, 9, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stull, A.; Cash, K.; Champagne, C.; Gupta, A.; Boston, R.; Beyl, R.; Johnson, W.; Cefalu, W. Blueberries Improve Endothelial Function, but Not Blood Pressure, in Adults with Metabolic Syndrome: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Nutrients 2015, 7, 4107–4123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basu, A.; Du, M.; Leyva, M.J.; Sanchez, K.; Betts, N.M.; Wu, M.; Aston, C.E.; Lyons, T.J. Blueberries Decrease Cardiovascular Risk Factors in Obese Men and Women with Metabolic Syndrome. J. Nutr. 2010, 140, 1582–1587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolehmainen, M.; Mykkänen, O.; Kirjavainen, P.V.; Leppänen, T.; Moilanen, E.; Adriaens, M.; Laaksonen, D.E.; Hallikainen, M.; Puupponen-Pimiä, R.; Pulkkinen, L.; et al. Bilberries Reduce Low-Grade Inflammation in Individuals with Features of Metabolic Syndrome. Mol. Nutr. Food. Res. 2012, 56, 1501–1510. [Google Scholar] [CrossRef]
- Simão, T.N.C.; Lozovoy, M.A.B.; Simão, A.N.C.; Oliveira, S.R.; Venturini, D.; Morimoto, H.K.; Miglioranza, L.H.S.; Dichi, I. Reduced-Energy Cranberry Juice Increases Folic Acid and Adiponectin and Reduces Homocysteine and Oxidative Stress in Patients with the Metabolic Syndrome. Br. J. Nutr. 2013, 110, 1885–1894. [Google Scholar] [CrossRef]
- Ruel, G.; Lapointe, A.; Pomerleau, S.; Couture, P.; Lemieux, S.; Lamarche, B.; Couillard, C. Evidence That Cranberry Juice May Improve Augmentation Index in Overweight Men. Nutr. Res. 2013, 33, 41–49. [Google Scholar] [CrossRef]
- Basu, A.; Betts, N.M.; Ortiz, J.; Simmons, B.; Wu, M.; Lyons, T.J. Low-Energy Cranberry Juice Decreases Lipid Oxidation and Increases Plasma Antioxidant Capacity in Women with Metabolic Syndrome. Nutr. Res. 2011, 31, 190–196. [Google Scholar] [CrossRef] [Green Version]
- Jeong, H.S.; Kim, S.; Hong, S.J.; Choi, S.C.; Choi, J.-H.; Kim, J.-H.; Park, C.-Y.; Cho, J.Y.; Lee, T.-B.; Kwon, J.-W.; et al. Black Raspberry Extract Increased Circulating Endothelial Progenitor Cells and Improved Arterial Stiffness in Patients with Metabolic Syndrome: A Randomized Controlled Trial. J. Med. Food 2016, 19, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Jeong, H.S.; Hong, S.J.; Lee, T.-B.; Kwon, J.-W.; Jeong, J.T.; Joo, H.J.; Park, J.H.; Ahn, C.-M.; Yu, C.W.; Lim, D.-S. Effects of Black Raspberry on Lipid Profiles and Vascular Endothelial Function in Patients with Metabolic Syndrome. Phytother. Res. 2014, 28, 1492–1498. [Google Scholar] [CrossRef] [PubMed]
- Tasic, N.; Jakovljevic, V.L.J.; Mitrovic, M.; Djindjic, B.; Tasic, D.; Dragisic, D.; Citakovic, Z.; Kovacevic, Z.; Radoman, K.; Zivkovic, V.; et al. Black Chokeberry Aronia Melanocarpa Extract Reduces Blood Pressure, Glycemia and Lipid Profile in Patients with Metabolic Syndrome: A Prospective Controlled Trial. Mol. Cell. Biochem. 2021, 476, 2663–2673. [Google Scholar] [CrossRef]
- Sikora, J.; Broncel, M.; Markowicz, M.; Chałubiński, M.; Wojdan, K.; Mikiciuk-Olasik, E. Short-Term Supplementation with Aronia Melanocarpa Extract Improves Platelet Aggregation, Clotting, and Fibrinolysis in Patients with Metabolic Syndrome. Eur. J. Nutr. 2012, 51, 549–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broncel, M.; Kozirog, M.; Duchnowicz, P.; Koter-Michalak, M.; Sikora, J.; Chojnowska-Jezierska, J. Aronia Melanocarpa Extract Reduces Blood Pressure, Serum Endothelin, Lipid, and Oxidative Stress Marker Levels in Patients with Metabolic Syndrome. Med. Sci. Monit. 2010, 16, CR28–CR34. [Google Scholar]
- Basu, A.; Fu, D.X.; Wilkinson, M.; Simmons, B.; Wu, M.; Betts, N.M.; Du, M.; Lyons, T.J. Strawberries Decrease Atherosclerotic Markers in Subjects with Metabolic Syndrome. Nutr. Res. 2010, 30, 462–469. [Google Scholar] [CrossRef] [Green Version]
- Puupponen-Pimiä, R.; Seppänen-Laakso, T.; Kankainen, M.; Maukonen, J.; Törrönen, R.; Kolehmainen, M.; Leppänen, T.; Moilanen, E.; Nohynek, L.; Aura, A.-M.; et al. Effects of Ellagitannin-Rich Berries on Blood Lipids, Gut Microbiota, and Urolithin Production in Human Subjects with Symptoms of Metabolic Syndrome. Mol. Nutr. Food Res. 2013, 57, 2258–2263. [Google Scholar] [CrossRef]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Final Report. Circulation 2002, 106, 3143. [Google Scholar] [CrossRef]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; World Health Organization: Geneva, Switzerland, 2000; ISBN 9241208945.
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C.; et al. Diagnosis and Management of the Metabolic Syndrome. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [Green Version]
- Basu, A.; Izuora, K.; Betts, N.M.; Kinney, J.W.; Salazar, A.M.; Ebersole, J.L.; Scofield, R.H. Dietary Strawberries Improve Cardiometabolic Risks in Adults with Obesity and Elevated Serum LDL Cholesterol in a Randomized Controlled Crossover Trial. Nutrients 2021, 13, 1421. [Google Scholar] [CrossRef]
- Martini, D.; Rossi, S.; Biasini, B.; Zavaroni, I.; Bedogni, G.; Musci, M.; Pruneti, C.; Passeri, G.; Ventura, M.; Di Nuzzo, S.; et al. Claimed Effects, Outcome Variables and Methods of Measurement for Health Claims Proposed under European Community Regulation 1924/2006 in the Framework of Protection against Oxidative Damage and Cardiovascular Health. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 473–503. [Google Scholar] [CrossRef]
- Huang, H.; Chen, G.; Liao, D.; Zhu, Y.; Xue, X. Effects of Berries Consumption on Cardiovascular Risk Factors: A Meta-Analysis with Trial Sequential Analysis of Randomized Controlled Trials. Sci. Rep. 2016, 6, 23625. [Google Scholar] [CrossRef] [PubMed]
- Luís, Â.; Domingues, F.; Pereira, L. Association between Berries Intake and Cardiovascular Diseases Risk Factors: A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Randomized Controlled Trials. Food Funct. 2018, 9, 740–757. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Gallegos, J.L.; Haskell-Ramsay, C.; Lodge, J.K. Effects of Chronic Consumption of Specific Fruit (Berries, Citrus and Cherries) on CVD Risk Factors: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Eur. J. Nutr. 2021, 60, 615–639. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases, 2013–2020; World Health Organization: Geneva, Switzerland, 2013; ISBN 9789241506236.
- Canoy, D.; Nazarzadeh, M.; Copland, E.; Bidel, Z.; Rao, S.; Li, Y.; Rahimi, K. How Much Lowering of Blood Pressure Is Required to Prevent Cardiovascular Disease in Patients With and Without Previous Cardiovascular Disease? Curr. Cardiol. Rep. 2022, 24, 851–860. [Google Scholar] [CrossRef] [PubMed]
- Vendrame, S.; Klimis-Zacas, D. Potential Factors Influencing the Effects of Anthocyanins on Blood Pressure Regulation in Humans: A Review. Nutrients 2019, 11, 1431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vendrame, S.; Adekeye, T.E.; Klimis-Zacas, D. The Role of Berry Consumption on Blood Pressure Regulation and Hypertension: An Overview of the Clinical Evidence. Nutrients 2022, 14, 2701. [Google Scholar] [CrossRef]
- Nikparast, A.; Sheikhhossein, F.; Amini, M.R.; Tavakoli, S.; Hekmatdoost, A. The Effects of Blackcurrant and Raspberry Consumption on Blood Pressure: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin. Nutr. Res. 2023, 12, 54. [Google Scholar] [CrossRef]
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; Peters, A.L.; Tsapas, A.; Wender, R.; Matthews, D.R. Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach: Update to a Position Statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2015, 38, 140–149. [Google Scholar] [CrossRef] [Green Version]
- Davies, M.J.; Aroda, V.R.; Collins, B.S.; Gabbay, R.A.; Green, J.; Maruthur, N.M.; Rosas, S.E.; Del Prato, S.; Mathieu, C.; Mingrone, G.; et al. Management of Hyperglycaemia in Type 2 Diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2022, 65, 1925–1966. [Google Scholar] [CrossRef]
- Tsuda, T. Recent Progress in Anti-Obesity and Anti-Diabetes Effect of Berries. Antioxidants 2016, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornell, S. A Review of GLP-1 Receptor Agonists in Type 2 Diabetes: A Focus on the Mechanism of Action of Once-weekly Agents. J. Clin. Pharm. 2020, 45, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Brunton, S.A.; Wysham, C.H. GLP-1 Receptor Agonists in the Treatment of Type 2 Diabetes: Role and Clinical Experience to Date. Postgrad. Med. 2020, 132, 3–14. [Google Scholar] [CrossRef]
- Daneshzad, E.; Shab-Bidar, S.; Mohammadpour, Z.; Djafarian, K. Effect of Anthocyanin Supplementation on Cardio-Metabolic Biomarkers: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin. Nutr. 2019, 38, 1153–1165. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Fang, J.; Gao, Z.; Zhang, C.; Xie, S. Higher Intake of Fruits, Vegetables or Their Fiber Reduces the Risk of Type 2 Diabetes: A Meta-analysis. J. Diabetes Investig. 2016, 7, 56–69. [Google Scholar] [CrossRef] [PubMed]
- Palma-Duran, S.A.; Vlassopoulos, A.; Lean, M.; Govan, L.; Combet, E. Nutritional Intervention and Impact of Polyphenol on Glycohemoglobin (HbA1c) in Non-Diabetic and Type 2 Diabetic Subjects: Systematic Review and Meta-Analysis. Crit. Rev. Food Sci. Nutr. 2017, 57, 975–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biondi, G.; Marrano, N.; Borrelli, A.; Rella, M.; Palma, G.; Calderoni, I.; Siciliano, E.; Lops, P.; Giorgino, F.; Natalicchio, A. Adipose Tissue Secretion Pattern Influences β-Cell Wellness in the Transition from Obesity to Type 2 Diabetes. Int. J. Mol. Sci. 2022, 23, 5522. [Google Scholar] [CrossRef] [PubMed]
- Dabke, K.; Hendrick, G.; Devkota, S. The Gut Microbiome and Metabolic Syndrome. J. Clin. Investig. 2019, 129, 4050–4057. [Google Scholar] [CrossRef]
- Cox, A.J.; West, N.P.; Cripps, A.W. Obesity, Inflammation, and the Gut Microbiota. Lancet. Diabetes Endocrinol. 2015, 3, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Sánchez, A.; Madrigal-Santillán, E.; Bautista, M.; Esquivel-Soto, J.; Morales-González, Á.; Esquivel-Chirino, C.; Durante-Montiel, I.; Sánchez-Rivera, G.; Valadez-Vega, C.; Morales-González, J.A. Inflammation, Oxidative Stress, and Obesity. Int. J. Mol. Sci. 2011, 12, 3117–3132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwingshackl, L.; Hoffmann, G.; Kalle-Uhlmann, T.; Arregui, M.; Buijsse, B.; Boeing, H. Fruit and Vegetable Consumption and Changes in Anthropometric Variables in Adult Populations: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. PLoS ONE 2015, 10, e0140846. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Pu, Y.; Xu, Y.; He, X.; Cao, J.; Ma, Y.; Jiang, W. Anti-Diabetic and Anti-Obesity: Efficacy Evaluation and Exploitation of Polyphenols in Fruits and Vegetables. Food Res. Int. 2022, 157, 111202. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Zhang, W.; Li, X.; Xu, Y.; Cao, J.; Jiang, W. The Anti-Obesogenic Effects of Dietary Berry Fruits: A Review. Food Res. Int. 2021, 147, 110539. [Google Scholar] [CrossRef]
- Riordan, J.; Solverson, P. Berry Anthocyanins in Rodent and Human Obesity and Diabetes: A Review of the Evidence. BioMed. 2022, 2, 210–237. [Google Scholar] [CrossRef]
- Land Lail, H.; Feresin, R.G.; Hicks, D.; Stone, B.; Price, E.; Wanders, D. Berries as a Treatment for Obesity-Induced Inflammation: Evidence from Preclinical Models. Nutrients 2021, 13, 334. [Google Scholar] [CrossRef] [PubMed]
- Del Bo’, C.; Martini, D.; Porrini, M.; Klimis-Zacas, D.; Riso, P. Berries and Oxidative Stress Markers: An Overview of Human Intervention Studies. Food Funct. 2015, 6, 2890–2917. [Google Scholar] [CrossRef]
- Joseph, S.V.; Edirisinghe, I.; Burton-Freeman, B.M. Berries: Anti-Inflammatory Effects in Humans. J. Agric. Food Chem. 2014, 62, 3886–3903. [Google Scholar] [CrossRef]
- Pap, N.; Fidelis, M.; Azevedo, L.; do Carmo, M.A.V.; Wang, D.; Mocan, A.; Pereira, E.P.R.; Xavier-Santos, D.; Sant’Ana, A.S.; Yang, B.; et al. Berry Polyphenols and Human Health: Evidence of Antioxidant, Anti-Inflammatory, Microbiota Modulation, and Cell-Protecting Effects. Curr. Opin. Food Sci. 2021, 42, 167–186. [Google Scholar] [CrossRef]
- Hosseini, B.; Berthon, B.S.; Saedisomeolia, A.; Starkey, M.R.; Collison, A.; Wark, P.A.B.; Wood, L.G. Effects of Fruit and Vegetable Consumption on Inflammatory Biomarkers and Immune Cell Populations: A Systematic Literature Review and Meta-Analysis. Am. J. Clin. Nutr. 2018, 108, 136–155. [Google Scholar] [CrossRef] [Green Version]
- Fallah, A.A.; Sarmast, E.; Jafari, T. Effect of Dietary Anthocyanins on Biomarkers of Oxidative Stress and Antioxidative Capacity: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Funct. Foods 2020, 68, 103912. [Google Scholar] [CrossRef]
- Martini, D.; Marino, M.; Angelino, D.; Del Bo’, C.; Del Rio, D.; Riso, P.; Porrini, M. Role of Berries in Vascular Function: A Systematic Review of Human Intervention Studies. Nutr. Rev. 2019, 78, 189–206. [Google Scholar] [CrossRef] [PubMed]
- Martini, D.; Marino, M.; Venturi, S.; Tucci, M.; Klimis-Zacas, D.; Riso, P.; Porrini, M.; Del Bo’, C. Blueberries and Their Bioactives in the Modulation of Oxidative Stress, Inflammation and Cardio/Vascular Function Markers: A Systematic Review of Human Intervention Studies. J. Nutr. Biochem. 2023, 111, 109154. [Google Scholar] [CrossRef] [PubMed]
- Ahles, S.; Joris, P.J.; Plat, J. Effects of Berry Anthocyanins on Cognitive Performance, Vascular Function and Cardiometabolic Risk Markers: A Systematic Review of Randomized Placebo-Controlled Intervention Studies in Humans. Int. J. Mol. Sci. 2021, 22, 6482. [Google Scholar] [CrossRef]
- Fairlie-Jones, L.; Davison, K.; Fromentin, E.; Hill, A. The Effect of Anthocyanin-Rich Foods or Extracts on Vascular Function in Adults: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients 2017, 9, 908. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| PICOS ITEMS | Inclusion Criteria |
|---|---|
| Population | Subjects that meet at least three out of five components of MetS |
| Intervention | Berries, berry extract alone or in combination. No medications |
| Comparison | No restriction |
| Outcome | MetS parameters and related markers |
| Study design | No restriction |
| Berry | Duration | Study Design | Participants/ MetS Classification | Drug Therapy | Intervention | MetS Findings and Related Parameters | Reference and Country |
|---|---|---|---|---|---|---|---|
| Blueberry | Single dose | Randomized, double-blind, controlled, cross-over | 45 subjects (age: 63 ± 7 y; BMI: 31.4 ± 3.1 kg/m2) MetS classification: Harmonized | Antihypertensive medication users (38%) or statin users (44%), or a combination | 26 g/day freeze-dried BB (equivalent to 1 cup fresh berries; 150 g) + energy-dense food (900 kcal) Highbush BB (scientific name not reported) Composition: 364 mg ACNs, 879 mg phenolics | ↓ GLC (at time 180 min) ↑↑ HDL-C =SBP, DBP Related parameters: ↓ insulin (at time 180 min), ↓ TC ↑↑ APO-A1, ↑↑ L-HDLP ↑ XL-HDLP | Curtis et al., 2022 (UK) [32] |
| 6 months | Randomized, double-blind, placebo-controlled, parallel arms | 115 subjects (age: 63 ± 7 y; BMI: 31.2 ± 3.0 kg/m2) MetS classification: Harmonized | Antihypertensive medication users (24%) or statin users (38%), or a combination | Group 1: 26 g/day freeze-dried BB (equivalent to 1 cup fresh berries; 150 g) Group 2: 13 g/day freeze-dried BB (equivalent to 1/2 cup fresh berries; 75 g) Highbush BB (scientific name not reported) Composition: Group 1: 879 mg phenolics, 364 mg ACNs Group 2: 439 mg phenolics, 182 mg ACNs | ↓ TG =GLC, HDL-C, SBP, DBP Related parameters: =insulin, HbA1c, TC, TC/HDL-C, LDL-C | Curtis et al., 2019 (UK) [33] | |
| Single dose | Controlled, crossover | 5 subjects (age: 26–61 y; BMI: 28–40 kg/m2) MetS classification: NCE-ATP III | No use of statins, anti-diabetics or chronic use of nonsteroidal anti-inflammatory drugs | High fat/high glycemic load meal + 150 g BB BB variety and scientific name not reported Composition: N.A. | N.A. (other markers are reported in Supplementary Table S1) | Sobolev et al., 2019 (Italy) [34] | |
| 6 weeks | Randomized, double-blind, placebo-controlled, parallel arms | 27 subjects (age: 56.5 ± 2.5 y; BMI: 34.7 ± 1.1 kg/m2) MetS classification: WHO | No use of non-prescription drugs | Twice daily, a 12-oz (∼356 mL) yogurt and a skim-milk-based smoothie with 45 g per day of freeze-dried BB powder (equivalent to approximately 2 cups of fresh berries) Highbush BB Tifblue (Vaccinium ashei) and Rubel (Vaccinium corymbosum) 50/50 Composition: 773.6 mg total phenolics, 290.3 mg ACNs | N.A. (other markers are reported in Supplementary Table S1) | Nair et al., 2017 (USA) [5] | |
| 6 weeks | Randomized, double-blinded, placebo-controlled, parallel arms | 23 subjects (age: 55 ± 2 y; BMI: 35.2 ± 0.8 kg/m2) MetS classification: WHO | Antihypertensive medication users (95%) | A skim-milk-based smoothie prepared with 45 g BB powder (equivalent to 2 cups of fresh berries) Highbush BB Tifblue (Vaccinium ashei) and Rubel (Vaccinium corymbosum) 50/50 Composition: 773.6 mg total phenolics, 290.3 mg ACNs | =GLC, TG, HDL-C, SBP, DBP Related parameters: =BW, BMI, % BF, % lean and fat mass, Insulin, TC, LDL-C | Stull et al., 2015 (USA) [35] | |
| 8 weeks | Randomized, single-blind, controlled, parallel arms | 48 subjects (age: 50.0 ± 3.0 y; BMI: 37.8 ± 2.3 kg/m2) MetS classification: NCE-ATP III | Antihypertensive medication users (20%) and multivitamin users | 480 mL/day BB drink (50 g freeze-dried BB corresponding to 350 g fresh berries) Highbush BB Tifblue (Vaccinium ashei) and Rubel (Vaccinium corymbosum) 50/50 Composition: 1624 mg phenolics, 742 mg ACNs | ↓ SBP, DBP =WC, GLC, TG, HDL-C; Related parameters: =BW, BMI, HbA1C, HOMA-IR, TC, LDL-C | Basu et al., 2010 (USA) [36] | |
| Bilberry | 8 weeks | Randomized, controlled, parallel arms | 27 subjects (age: 53 ± 6 y; BMI: 31.4 ± 4.7 kg/m2) MetS classification: NCE-ATP III | No information | 200 g of bilberry purée + 40 g dried bilberries (equivalent to 400 g fresh berries) Vaccinium myrtillus Composition: 1381 mg ACNs, 36.4 mg flavonol | =WC, TG, HDL-C, SBP, DBP Related parameters: =BW, %BF, TC, LDL-C, Apo-A1, Apo-B, markers of cholesterol synthesis | Kolehmainen et al., 2012 (Finland) [37] |
| Cranberry | 4 weeks | Controlled, parallel arms | 56 subjects (median age: 50 y; median BMI: 31 kg/m2) MetS classification: NCE-ATP III | Anti-hypertensive medication users | 700 mL/day reduced-energy cranberry juice Vaccinium macrocarpon Composition: N.A. | =WC Related parameters: =BMI | Simao et al., 2013 (Brazil) [38] |
| 4 weeks | Double-blind, placebo-controlled, crossover | 13 subjects § (age: 42 ± 11 y, BMI: 29.3 ± 2.8 kg/m2) MetS classification: NCE-ATP III | No medications known to affect lipid and insulin metabolism or blood pressure | 500 mL/day of low-calorie cranberry juice (27% juice) Vaccinium macrocarpon Composition: 400 mg total polyphenols, 20.8 mg ACNs | =SBP, DBP | Ruel et al., 2013 (Canada) [39] | |
| 8 weeks | Randomized, double-blind, placebo-controlled, parallel arms | 31 subjects (age: 52.0 ± 8.0 y; BMI: 40.0 ± 7.7 kg/m2) MetS classification: NCE-ATP III | Antihypertensive medication users (20%) and multivitamin users (25%) | 480 mL/day cranberry juice Vaccinium macrocarpon Composition: 229.0 mg total phenolics, 12.4 mg total ACNs, 119 mg proanthocyanidins | =GLC, TG, HDL-C, SBP, DBP Related parameters: =TC, LDL-C, VLDL-C | Basu et al., 2011 (USA) [40] | |
| Raspberry | 12 weeks | Randomized, double-blind, placebo-controlled, parallel arms | 51 subjects (age: 59 ± 10 y, BMI: 25 ± 4 kg/m2) MetS classification: Harmonized | Aspirin, beta blocker, ACE inhibitor, calcium blocker, diuretics, statin users | 750 mg/day dried unripe black raspberry powder Rubus occidentalis Composition: Reported for the fresh product but not for the powder | =SBP, DBP | Jeong et al., 2016 (Korea) [41] |
| 12 weeks | Controlled, parallel arms | 77 subjects (age: 60.0 ± 9.4 y; BMI: 25.7 ± 4.2 kg/m2) MetS classification: Harmonized | Aspirin, beta blocker, ACE inhibitor, statin, users | 750 mg/day of black raspberry powder in capsules Rubus occidentalis Composition: N.A. | N.A. Related parameters: ↓ TC, TC/HDL-C ratio =Apo-A1, Apo-B, Apo-B/Apo-A1 ratio | Jeong et al., 2014 (Korea) [42] | |
| Chokeberry | 4 weeks | Non-randomized, non-controlled | 143 subjects (age: 50–60 y; BMI: 29.7–34.4 kg/m2) MetS classification: AHA/NHLBI | Statin users | 30 mL/day Standardized chokeberry extract Aronia melanocarpa Composition: 431 mg polyphenols, 120 mg ACNs | ↓ WC, GLC, TG, SBP, DBP =HDL-C Related parameters: ↓ BW, TC, LDL-C =BMI | Tasic et al., 2021 (Poland) [43] |
| 8 weeks | Non-randomized, non-controlled | 38 subjects (age: 42–65 y; BMI: 31.1 ± 3.3 kg/m2) MetS classification: AHA/NHLBI | No hypolipemic, hypotensive, anticoagulant, antiplatelet, or profibrinolytic drugs | 300 mg/day chokeberry extract Aronia melanocarpa Composition: 60 mg total polyphenols, 20 mg ACNs | ↓ TG =WC, HDL-C Related parameters: ↓ TC, LDL-C =BMI | Sikora et al., 2012 (Poland) [44] | |
| 8 weeks | Non-randomized, non-controlled | 25 subjects (age: 42–65 y and BMI: 31.1 ± 3.2 kg/m2) MetS classification: AHA/NHLBI | No medication users | 300 mg/day chokeberry extract Aronia melanocarpa Composition: 3-O-cyanidin-galactoside (64.5%), 3-O-cyanidin-arabinoside (28.9%), 3-O-cyanidin-xyloside (4.2%), and 3-O-cyanidin- glucoside (2.4%) | ↓↓↓ TG, SBP ↓↓ DBP ↑↑↑ GLC, HDL-C =WC Related parameters ↓↓↓ TC, LDL-C =BMI | Broncel et al., 2010 (Poland) [45] | |
| Strawberry | 8 weeks | Randomized, controlled, parallel arms | 27 subjects (age: 47.0 ± 3.0 y; BMI: 37.5 ± 2.15 kg/m2) MetS classification: NCE-ATP III | Control group: (24%; antihypertensive medications users) Strawberry group: (0%) | Four cups daily strawberry drink with 25 g/cup of freeze-dried strawberry powder Strawberry: scientific name not reported Composition: 2 g total phenolics, 154 mg total ACNs | =WC, GLC, TG, SBP, DBP Related parameters: ↓ small LDL-C particles =BW, lipoprotein particle concentrations and size | Basu et al., 2010 (USA) [46] |
| Berry mix | 12 weeks | Randomized, controlled, parallel arms | 20 subjects (age: 53.0 ± 6.5 year; BMI: 31.8 ± 4.4 kg/m2) MetS classification: NCE-ATP III | No information | 300 g/day of fresh berries comprising 100 g of strawberry purée, 100 g of frozen raspberries, and 100 g of frozen cloudberries Berries’ scientific name not reported Composition: 789 mg ellagitannins, 70.7 mg ACNs, 4.1 mg flavonols | =WC, HDL-C, SBP, DBP Related parameters: =BMI, TC, LDL-C | Puupponen-Pimiä et al., 2013 (Finland) [47] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Venturi, S.; Marino, M.; Cioffi, I.; Martini, D.; Del Bo’, C.; Perna, S.; Riso, P.; Klimis-Zacas, D.; Porrini, M. Berry Dietary Interventions in Metabolic Syndrome: New Insights. Nutrients 2023, 15, 1906. https://doi.org/10.3390/nu15081906
Venturi S, Marino M, Cioffi I, Martini D, Del Bo’ C, Perna S, Riso P, Klimis-Zacas D, Porrini M. Berry Dietary Interventions in Metabolic Syndrome: New Insights. Nutrients. 2023; 15(8):1906. https://doi.org/10.3390/nu15081906
Chicago/Turabian StyleVenturi, Samuele, Mirko Marino, Iolanda Cioffi, Daniela Martini, Cristian Del Bo’, Simone Perna, Patrizia Riso, Dorothy Klimis-Zacas, and Marisa Porrini. 2023. "Berry Dietary Interventions in Metabolic Syndrome: New Insights" Nutrients 15, no. 8: 1906. https://doi.org/10.3390/nu15081906