
The Impact of Transjugular Intrahepatic Portosystemic Shunt on Nutrition in Liver Cirrhosis Patients: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
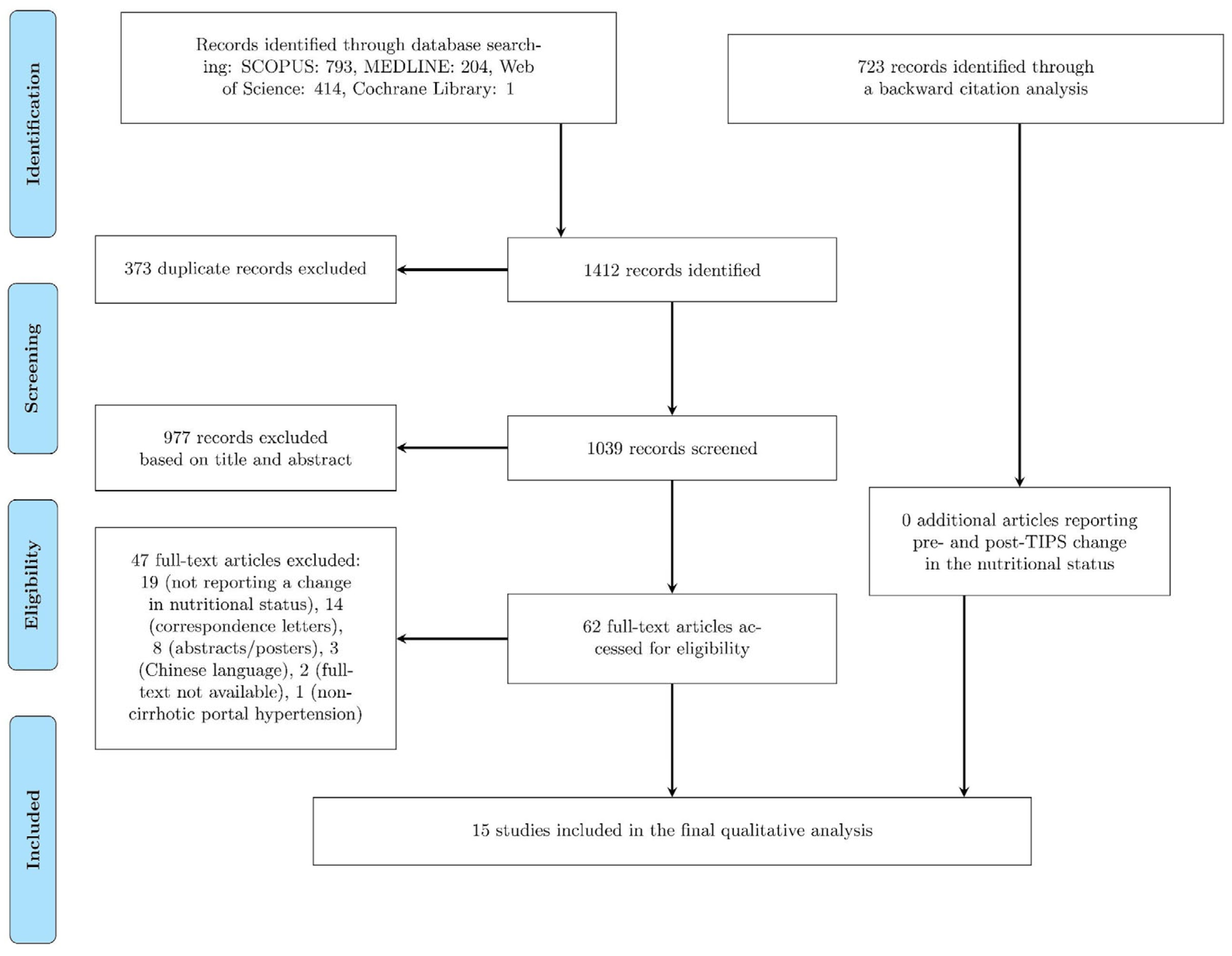
2.1. Literature Search
2.2. Criteria for the Selection of Studies
2.3. Study Selection, Data Extraction, and Data Calculation
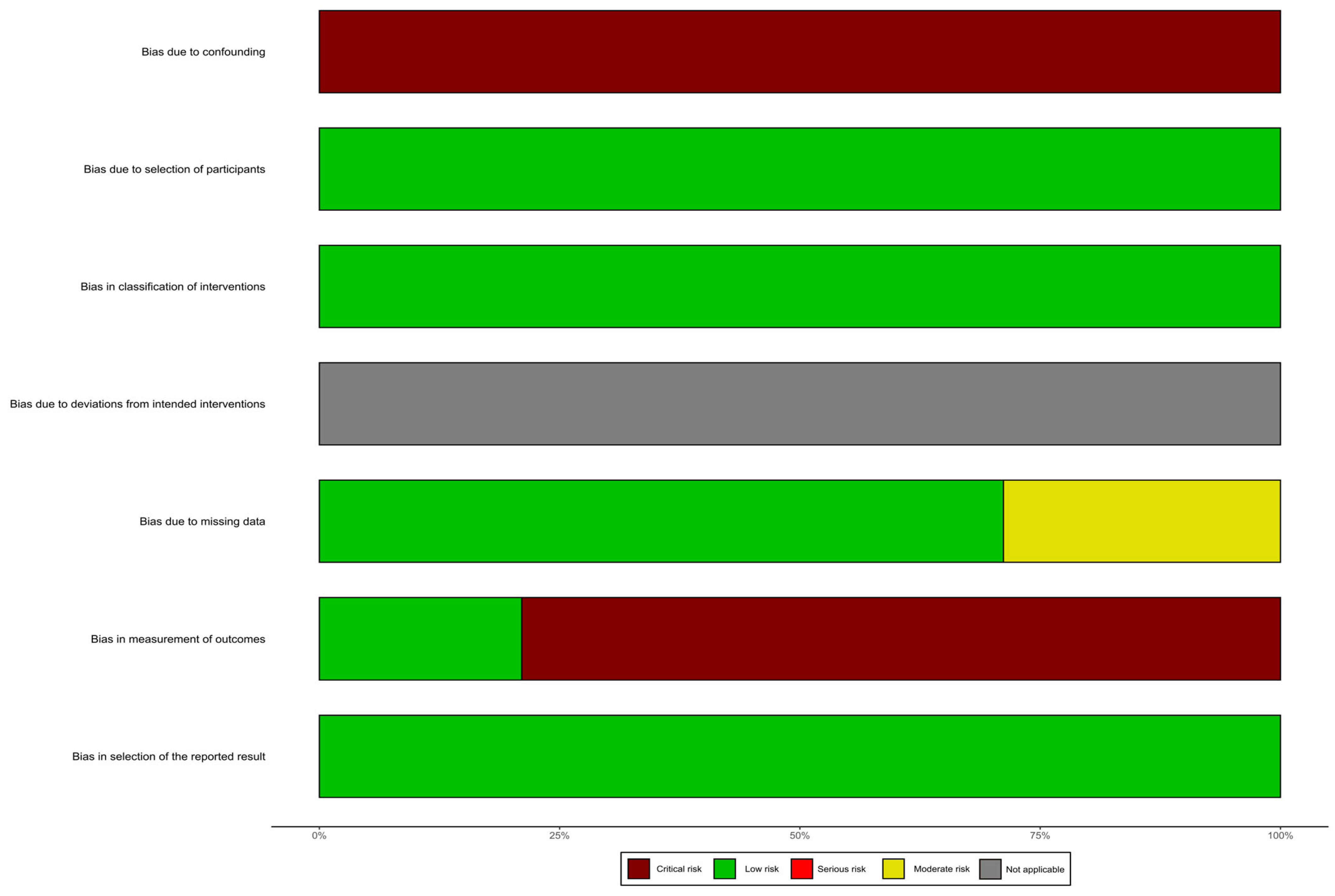
2.4. Risk of Bias Assessment
3. Results
3.1. Risk of Bias Assessment
3.2. Body Mass Index, Weight, and/or Body Cell Mass
3.3. Skeletal Muscle Volume, Skeletal Muscle Function
3.4. Adipose Tissue Volume

{kind=link}
{kind=link}
| Reference | Design | Sample Size | TIPS Indication | Follow-Up after | Measure | Change |
|---|---|---|---|---|---|---|
| Allard et al. (2001) [27] | - | 14 (71% ♂) | RA (100%) | 12 M | W, Dry W, FM, F10/F30, and MRR | Significant increase in Dry W and FM. |
| Artru et al. (2020) [19] | RS | 179 (72% ♂) | RA (47.5%), VB (52.5%) | 6 M | TPMT, TPMA, SFA, and VFA | Significant increase in TPMT, TPMA, and SFA and significant decrease in VFA. |
| Gioia et al. (2019) [13] | RS | 27 (85% ♂) | RA (56%), VB (44%) | 9.8 M | SMI | Significant increase in SMI. |
| Gioia et al. (2021) [14] | RS | 35 (80% ♂) | RA (54%), VB (46%) | 19 M | SMI, SATI, and VATI | Significant increase in SMI and SATI and significant decrease in VATI. |
| Holland-Fischer et al. (2010) [29] | - | 11 (73% ♂) | RA (64%), RA+VB (36%) | 6 M | W, BMI, BCM, LBM, and FM | Significant increase in all but FM. |
| Holland-Fischer et al. (2009) [28] | - | 17 | RA (59%), VB (29%), both (12%) | 13 M | W and BCM | Significant increase in BCM. |
| Jahangiri et al. (2019) [21] | RS | 76 (56.2% ♂) | RA/RH(52.6%), VB (47.4%) | 13.5 M | SMA | Significant increase in SMA. |
| Liu et al. (2022) [20] | RS | 224 (71% ♂) | RA (14%), VB (86%) | 12 M | SMA, SMI, SFA, SFT, AF W, and AF BMI | No significant change in SMA, SMI, SFA, and SFT in patients without sarcopenia. Significant increase in SMA, SMI, SFA, and SFT in patients with sarcopenia. No significant change in AF W and AF BMI in patients without ascites and sarcopenia. Significant increase in AF W and AF BMI in patients with sarcopenia but without ascites. |
| Montomoli et al. (2010) [26] | PS | 21 | RA (57%), VB (33%), both (10%) | 13 M | BMI, FM, and DLM | No significant change in overweight patients, significant increase in dry lean mass in under/normal weight patients. |
| Nolte et al. (2003) [25] | PS | 31 | RA, VB | 9 M | W, BMI, AF W, and AF BMI | Significant increase in W, BMI, AF W, and AF BMI in male patients, significant increase in AF W and AF BMI in female patients. |
| Pang et al. (2021) [22] | RS | 77 | RA, VB | 13 M | W, BMI | Significant increase in W and BMI. |
| Plauth et al. (2004) [24] | PS | 21 (62% ♂) | RA (33%), VB (43%), both (24%) | 12 M | W, BMI, MAFA, MAMA, and BCM | Significant increase in W, BMI, and MAMA. |
| Thomsen et al. (2012) [30] | - | 25 (60% ♂) | RA (68%), VB (20%), both (12%) | 6 M | W, BMI, FM*, and BCM | Significant increase in BCM. |
| Trotter et al. (1998) [23] | RS | 35 (69% ♂) | RA | 8.8 M | W | Significant increase in W. |
| Tsien et al. (2012) [15] | - | 57 (63% ♂) | RA (72%), VB (25%), both (3%) | 13.5 M | BMI, SMA, VAT, and SAT | Significant increase in SMA and significant decrease in SAT. |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Angeli, P.; Bernardi, M.; Villanueva, C.; Francoz, C.; Mookerjee, R.P.; Trebicka, J.; Krag, A.; Laleman, W.; Gines, P. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar]
- De Franchis, R.; Bosch, J.; Garcia-Tsao, G.; Reiberger, T.; Ripoll, C.; Abraldes, J.G.; Albillos, A.; Baiges, A.; Bajaj, J.; Bañares, R.; et al. Baveno VII—Renewing consensus in portal hypertension. J. Hepatol. 2022, 76, 959–974. [Google Scholar] [CrossRef] [PubMed]
- Merli, M.; Berzigotti, A.; Zelber-Sagi, S.; Dasarathy, S.; Montagnese, S.; Genton, L.; Plauth, M.; Parés, A. EASL Clinical Practice Guidelines on nutrition in chronic liver disease. J. Hepatol. 2019, 70, 172–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romiti, A.; Merli, M.; Martorano, M.; Parrilli, G.; Martino, F.; Riggio, O.; Truscelli, A.; Capocaccia, L.; Budillon, G. Malabsorption and nutritional abnormalities in patients with liver cirrhosis. Ital. J. Gastroenterol. 1990, 22, 118–123. [Google Scholar]
- Kim, G.; Kang, S.H.; Kim, M.Y.; Baik, S.K. Prognostic value of sarcopenia in patients with liver cirrhosis: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0186990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tantai, X.; Liu, Y.; Yeo, Y.H.; Praktiknjo, M.; Mauro, E.; Hamaguchi, Y.; Engelmann, C.; Zhang, P.; Jeong, J.Y.; van Vugt, J.L.A.; et al. Effect of sarcopenia on survival in patients with cirrhosis: A meta-analysis. J. Hepatol. 2022, 76, 588–599. [Google Scholar] [CrossRef] [PubMed]
- Montagnese, S.; Russo, F.P.; Amodio, P.; Burra, P.; Gasbarrini, A.; Loguercio, C.; Marchesini, G.; Merli, M.; Ponziani, F.R.; Riggio, O.; et al. Hepatic encephalopathy 2018: A clinical practice guideline by the Italian Association for the Study of the Liver (AISF). Dig. Liver Dis. 2019, 51, 190–205. [Google Scholar] [CrossRef]
- Lattanzi, B.; Gioia, S.; Di Cola, S.; D’Ambrosio, D.; Nardelli, S.; Tavano, D.; Farcomeni, A.; Merli, M.; Riggio, O. Prevalence and impact of sarcopenia in non-cirrhotic portal hypertension. Liver Int. 2019, 39, 1937–1942. [Google Scholar] [CrossRef]
- Nardelli, S.; Lattanzi, B.; Torrisi, S.; Greco, F.; Farcomeni, A.; Gioia, S.; Merli, M.; Riggio, O. Sarcopenia is risk factor for development of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt placement. Clin. Gastroenterol. Hepatol. 2017, 15, 934–936. [Google Scholar] [CrossRef]
- Praktiknjo, M.; Clees, C.; Pigliacelli, A.; Fischer, S.; Jansen, C.; Lehmann, J.; Pohlmann, A.; Lattanzi, B.; Krabbe, V.K.; Strassburg, C.P.; et al. Sarcopenia is associated with development of acute-on-chronic liver failure in decompensated liver cirrhosis receiving transjugular intrahepatic portosystemic shunt. Clin. Transl. Gastroenterol. 2019, 10, e00025. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Zhu, X.; Liu, J.; Shi, Q.; Du, H.; Chen, Y.; Huang, S.; Zhou, C.; Wang, Y.; Li, T.; et al. Development and Validation of Prognostic Models to Estimate the Risk of Overt Hepatic Encephalopathy after TIPS Creation: A Multicenter Study. Clin. Transl. Gastroenterol. 2022, 13, e00461. [Google Scholar] [CrossRef] [PubMed]
- Nardelli, S.; Lattanzi, B.; Merli, M.; Farcomeni, A.; Gioia, S.; Ridola, L.; Riggio, O. Muscle Alterations Are Associated with Minimal and Overt Hepatic Encephalopathy in Patients with Liver Cirrhosis. Hepatology 2019, 70, 1704–1713. [Google Scholar] [CrossRef] [PubMed]
- Gioia, S.; Merli, M.; Nardelli, S.; Lattanzi, B.; Pitocchi, F.; Ridola, L.; Riggio, O. The modification of quantity and quality of muscle mass improves the cognitive impairment after TIPS. Liver Int. 2019, 39, 871–877. [Google Scholar] [CrossRef]
- Gioia, S.; Ridola, L.; Cristofaro, L.; Merli, M.; Faccioli, J.; Riggio, O.; Nardelli, S. The improvement in body composition including subcutaneous and visceral fat reduces ammonia and hepatic encephalopathy after transjugular intrahepatic portosystemic shunt. Liver Int. 2021, 41, 2965–2973. [Google Scholar] [CrossRef]
- Tsien, C.; Shah, S.N.; Mccullough, A.J.; Dasarathy, S. Reversal of sarcopenia predicts survival after a transjugular intrahepatic portosystemic stent. Eur. J. Gastroenterol. Hepatol. 2013, 25, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Reprint—Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Phys. Ther. 2009, 89, 873–880. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Artru, F.; Miquet, X.; Azahaf, M.; Labreuche, J.; Ntandja Wandji, L.C.; Sergent, G.; Nobécourt, A.; Toumelin, P.; Lassailly, G.; Dharancy, S.; et al. Consequences of TIPSS placement on the body composition of patients with cirrhosis and severe portal hypertension: A large retrospective CT-based surveillance. Aliment. Pharmacol. Ther. 2020, 52, 1516–1526. [Google Scholar] [CrossRef]
- Liu, J.; Ma, J.; Yang, C.; Chen, M.; Shi, Q.; Zhou, C.; Huang, S.; Chen, Y.; Wang, Y.; Li, T.; et al. Sarcopenia in Patients with Cirrhosis after Transjugular Intrahepatic Portosystemic Shunt Placement. Radiology 2022, 303, 711–719. [Google Scholar] [CrossRef]
- Jahangiri, Y.; Pathak, P.; Tomozawa, Y.; Li, L.; Schlansky, B.L.; Farsad, K. Muscle Gain after Transjugular Intrahepatic Portosystemic Shunt Creation: Time Course and Prognostic Implications for Survival in Cirrhosis. J. Vasc. Interv. Radiol. 2019, 30, 866–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pang, N.; Zhao, C.; Li, J.; Li, L.; Yang, X.; Yang, M.; Wu, Z.; Feng, D. Body mass index changes after transjugular intrahepatic portosystemic shunt in individuals with cirrhosis. Nutrition 2021, 84, 111095. [Google Scholar] [CrossRef]
- Trotter, J.F.; Suhocki, P.V.; Rockey, D.C. Transjugular intrahepatic portosystemic shunt (TIPS) in patients with refractory ascites: Effect on body weight and child-pugh score. Am. J. Gastroenterol. 1998, 93, 1891–1894. [Google Scholar] [CrossRef] [PubMed]
- Plauth, M.; Schütz, T.; Buckendahl, D.P.; Kreymann, G.; Pirlich, M.; Grüngreiff, S.; Romaniuk, P.; Ertl, S.; Weiß, M.L.; Lochs, H. Weight gain after transjugular intrahepatic portosystemic shunt is associated with improvement in body composition in malnourished patients with cirrhosis and hypermetabolism. J. Hepatol. 2004, 40, 228–233. [Google Scholar] [CrossRef]
- Nolte, W.; Wirtz, M.; Rossbach, C.; Leonhardt, U.; Buchwald, A.B.; Scholz, K.H.; Ramadori, G. TIPS Implantation Raises Leptin Levels in Patients with Liver Cirrhosis. Exp. Clin. Endocrinol. Diabetes 2003, 111, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Montomoli, J.; Holland-Fischer, P.; Bianchi, G.; Grønbæk, H.; Vilstrup, H.; Marchesini, G.; Zoli, M. Body composition changes after transjugular intrahepatic portosystemic shunt in patients with cirrhosis. World J. Gastroenterol. 2010, 16, 348–353. [Google Scholar] [CrossRef]
- Allard, J.P.; Chau, J.; Sandokji, K.; Blendis, L.M.; Wong, F. Effects of ascites resolution after successful TIPS on nutrition in cirrhotic patients with refractory ascites. Am. J. Gastroenterol. 2001, 96, 2442–2447. [Google Scholar] [CrossRef]
- Holland-Fischer, P.; Vilstrup, H.; Frystyk, J.; Nielsen, D.T.; Flyvbjerg, A.; Grøonbæk, H. The IGF system after insertion of a transjugular in trahepatic porto-systemic shunt in patients with liver cirrhosis. Eur. J. Endocrinol. 2009, 160, 957–963. [Google Scholar] [CrossRef] [Green Version]
- Holland-Fischer, P.; Nielsen, M.F.; Vilstrup, H.; Tønner-Nielsen, D.; Mengel, A.; Schmitz, O.; Grønbæk, H. Insulin sensitivity and body composition in cirrhosis: Changes after TIPS. Am. J. Physiol. Gastrointest. Liver Physiol. 2010, 299, G486–G493. [Google Scholar] [CrossRef] [Green Version]
- Thomsen, K.L.; Sandahl, T.D.; Holland-Fischer, P.; Jessen, N.; Frystyk, J.; Flyvbjerg, A.; Grønbæk, H.; Vilstrup, H. Changes in adipokines after transjugular intrahepatic porto-systemic shunt indicate an anabolic shift in metabolism. Clin. Nutr. 2012, 31, 940–945. [Google Scholar] [CrossRef]
- Qi, X.; Jia, J.; Bai, M.; Guo, X.; Su, C.; Garcia-Pagan, J.C.; Han, G.; Fan, D. Transjugular intrahepatic portosystemic shunt for acute variceal bleeding. J. Clin. Gastroenterol. 2015, 49, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Salerno, F.; Cammà, C.; Enea, M.; Rössle, M.; Wong, F. Transjugular Intrahepatic Portosystemic Shunt for Refractory Ascites: A Meta-analysis of Individual Patient Data. Gastroenterology 2007, 133, 825–834. [Google Scholar] [CrossRef]
- Santolaria, F.; González-Reimers, E. Alcohol and nutrition: An overview. In Alcohol, Nutrition, and Health Consequences; Humana Press: Totowa, NJ, USA, 2013; pp. 3–14. [Google Scholar] [CrossRef]
- Lang, C.H.; Pruznak, A.M.; Nystrom, G.J.; Vary, T.C. Alcohol-induced decrease in muscle protein synthesis associated with increased binding of mTOR and raptor: Comparable effects in young and mature rats. Nutr. Metab. 2009, 6, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, G.; Wang, X.; Yang, T.; Yan, Y.; Xiang, T.; Yang, L.; Luo, X. High Interleukin-8 Levels Associated with Decreased Survival in Patients with Cirrhosis following Transjugular Intrahepatic Portosystemic Shunt. Front. Med. 2022, 9, 829245. [Google Scholar] [CrossRef] [PubMed]
- Wirtz, T.H.; Reuken, P.A.; Jansen, C.; Fischer, P.; Bergmann, I.; Backhaus, C.; Emontzpohl, C.; Reißing, J.; Brandt, E.F.; Koenen, M.T.; et al. Balance between macrophage migration inhibitory factor and sCD74 predicts outcome in patients with acute decompensation of cirrhosis. JHEP Rep. 2021, 3, 100221. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, J.M.; Claus, K.; Jansen, C.; Pohlmann, A.; Schierwagen, R.; Meyer, C.; Thomas, D.; Manekeller, S.; Claria, J.; Strassburg, C.P.; et al. Circulating CXCL10 in cirrhotic portal hypertension might reflect systemic inflammation and predict ACLF and mortality. Liver Int. 2018, 38, 875–884. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Hirose, H.; Senga, S.; Onitsuka, A.; Fuwa, S.; Mori, Y.; Yamada, T. Effect of portal hypertension caused by chronic high venous pressure on small-intestinal sugar absorption. Nutrition 2000, 16, 30–33. [Google Scholar] [CrossRef]
- Pinho, C.; Diniz, A.; Arruda, I.; Leão, A.; Albuquerque, E.; Rodrigues, G. Factors Associated with the Concentration of Visceral and Subcutaneous Fat. Health Care Curr. Rev. 2017, 5, 4. [Google Scholar] [CrossRef]
- Mittal, B. Subcutaneous adipose tissue & visceral adipose tissue. Indian J. Med. Res. 2019, 149, 571–573. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gazda, J.; Di Cola, S.; Lapenna, L.; Khan, S.; Merli, M. The Impact of Transjugular Intrahepatic Portosystemic Shunt on Nutrition in Liver Cirrhosis Patients: A Systematic Review. Nutrients 2023, 15, 1617. https://doi.org/10.3390/nu15071617
Gazda J, Di Cola S, Lapenna L, Khan S, Merli M. The Impact of Transjugular Intrahepatic Portosystemic Shunt on Nutrition in Liver Cirrhosis Patients: A Systematic Review. Nutrients. 2023; 15(7):1617. https://doi.org/10.3390/nu15071617
Chicago/Turabian StyleGazda, Jakub, Simone Di Cola, Lucia Lapenna, Saniya Khan, and Manuela Merli. 2023. "The Impact of Transjugular Intrahepatic Portosystemic Shunt on Nutrition in Liver Cirrhosis Patients: A Systematic Review" Nutrients 15, no. 7: 1617. https://doi.org/10.3390/nu15071617