
Nutrition Effects of a Family-Centered Health Promotion Program for Mexican-Heritage Children in the Lower Rio Grande Valley of Texas


 , and
, and
Abstract
:1. Introduction
2. Materials & Methods
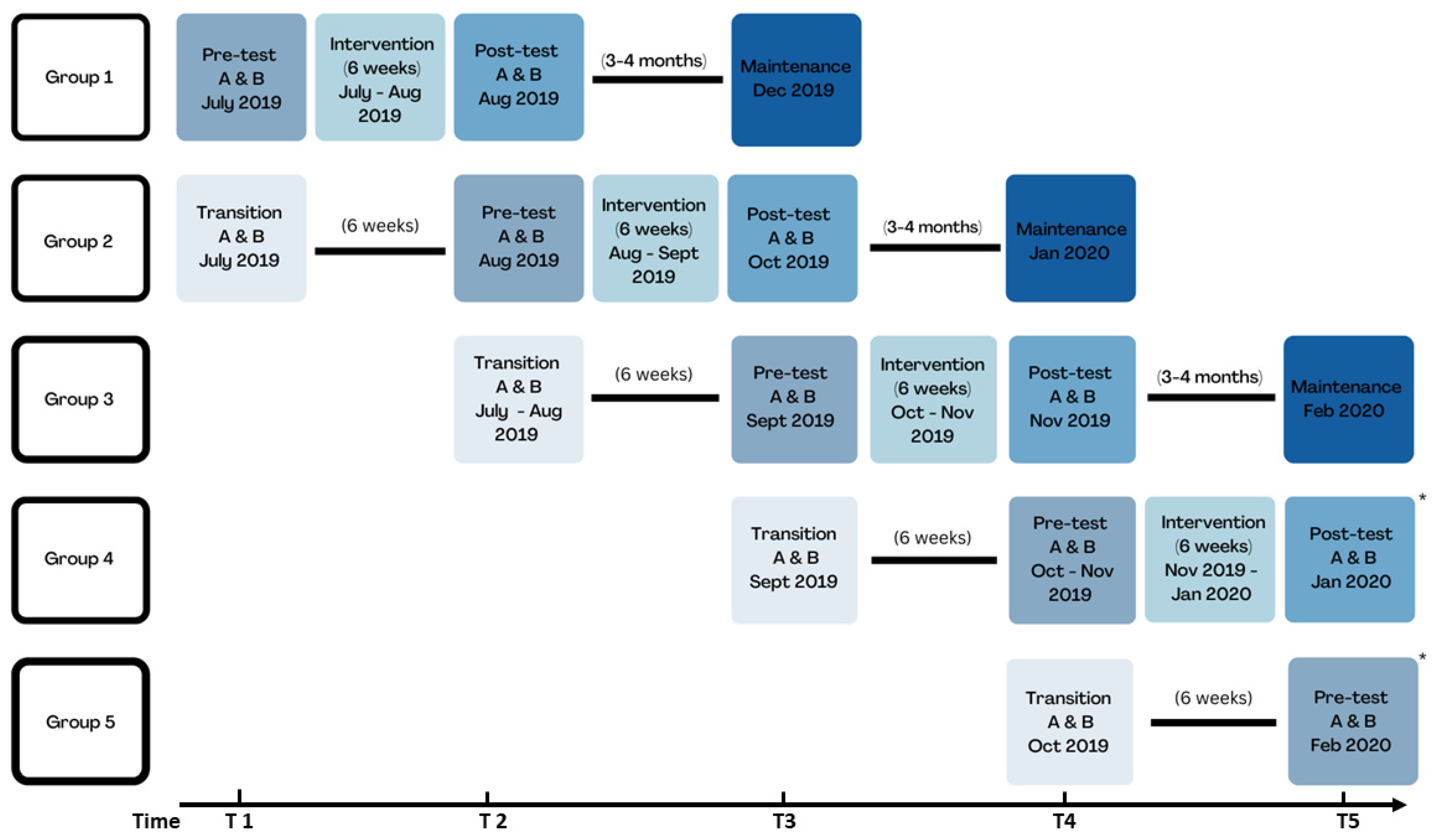
2.1. Overview, Study Design, and Context
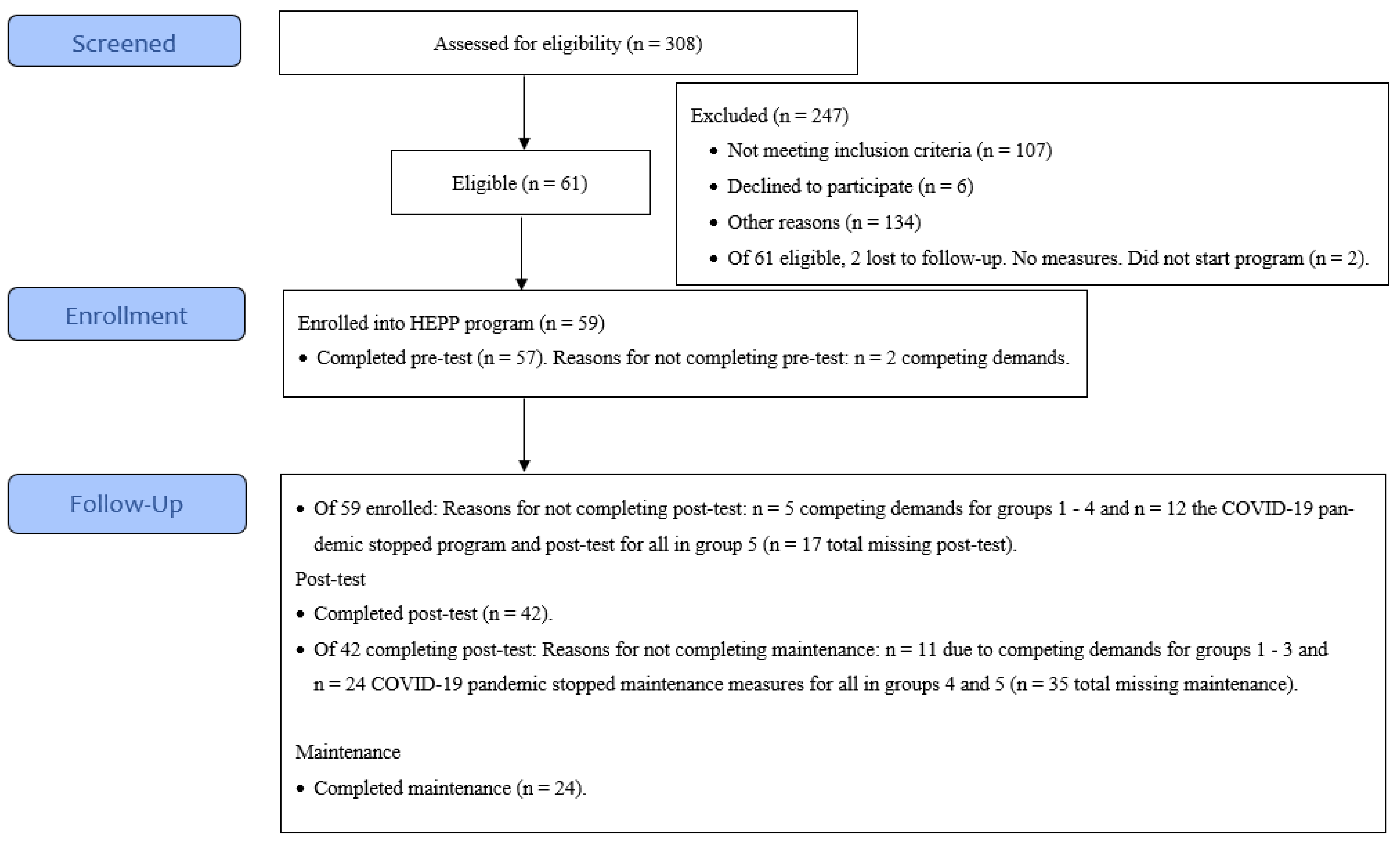
2.2. Participants
2.3. Program Design
Intervention Structure, Components, and Curriculum
2.4. Data Collection
2.5. Measures
2.5.1. Food Insecurity
2.5.2. Instant Skin Carotenoid Score
2.5.3. Children’s Body Mass Index (BMI)
2.5.4. Data Analysis and Interpretation
3. Results
3.1. Sample Characteristics
3.2. Within-Person Change for Instant Skin Carotenoid Scores and BMI for Children at Post-Test and Maintenance

{kind=link}
{kind=link}
| Outcomes | Total | Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | p-Value |
|---|---|---|---|---|---|---|---|
| Number of children, n | 55 | 9 | 10 | 13 | 12 | 11 | |
| Program period | |||||||
| Program dose, mean number of sessions (SD) | 4.72 (2.15) | 5.59 (0.94) | 4.69 (2.19) | 4.94 (2.12) | 5.42 (1.69) | 1.27 * (0.79) | <0.001 |
| Within-person change in instant skin carotenoid score | −15.3 (6.2) | 14.8 (23.8) | −18.2 (23.8) | −30.5 (21.6) | −21.7 (20.6) | - | |
| BMI | |||||||
| Within-person change in BMI percentile | −0.34 (0.4) | 1.79 (1.74) | 1.43 (1.74) | −3.27 (1.57) | −0.56 (1.51) | - | |
| Within-person change in BMI z-score | −0.03 (0.02) | 0.07 (0.07) | 0.04 (0.07) | −0.15 (0.06) | −0.03 (0.06) | - | |
| Control period | |||||||
| Within-person change in instant skin carotenoid score | −5.5 (4.2) | 4.9 (22.6) | −6 (20.6) | −13.4 (20.6) | −6 (21.6) | - | 0.695 |
| Within-person change in BMI percentile | 0.44 (0.41) | 0.66 (1.65) | 1.33 (1.51) | −0.58 (1.51) | 0.4 (1.57) | - | 0.787 |
| Within-person change in BMI z-score | 0.03 (0.02) | 0.02 (0.07) | 0.08 (0.06) | −0.01 (0.06) | 0.01 (0.06) | - | 0.561 |
| Outcomes | Total | Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | p-Value |
|---|---|---|---|---|---|---|---|
| Number of children, n | 24 | 8 | 7 | 9 | 0 | 0 | |
| Program dose, mean number of sessions (SD) | 4.72 (2.15) | 5.59 (0.94) | 4.69 (2.19) | 4.94 (2.12) | - | - | <0.001 |
| Within-person change in instant skin carotenoid score | −2.00 (7.3) | −3.38 (12.71) | −18.86 (13.59) | 12.22 (11.98) | - | - | 0.233 |
| Within-person change in BMI percentile | −1.6 (0.37) | −0.48 (0.64) | −2.45 (0.68) | −1.93 (0.6) | - | - | 0.0925 |
| Within-person change in BMI z-score | −0.05 (0.01) | −0.01 (0.03) | −0.07 (0.03) | −0.06 (0.02) | 0.2133 |
3.3. Program effects on Instant Skin Carotenoid Scores and BMI for Children at Post-Test
4. Discussion
4.1. Limitations and Strengths
4.2. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sharkey, J.R.; Nalty, C.; Johnson, C.M.; Dean, W.R. Children’s very low food security is associated with increased dietary intakes in energy, fat, and added sugar among Mexican-origin children (6–11 y) in Texas border colonias. BMC Pediatr. 2012, 12, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayala, G.X.; Baquero, B.; Arredondo, E.M.; Campbell, N.; Larios, S.; Elder, J.P. Association between family variables and Mexican American children’s dietary behaviors. J. Nutr. Educ. Behav. 2007, 39, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Horton, L.A.; Parada, H.; Slymen, D.J.; Arredondo, E.; Ibarra, L.; Ayala, G.X. Targeting children’s dietary behaviors in a family intervention: ‘Entre Familia: Reflejos de Salud’. Salud Publica Mex 2013, 55 (Suppl. S3), 397–405. [Google Scholar] [PubMed]
- Tucker, K.M.; Ingram, M.; Doubleday, K.; Piper, R.; Carvajal, S.C. La Vida Buena (The Good Life) evaluation: A quasi experimental intervention of a community health worker-led family-based childhood obesity program for Latino children 5-8 years of age on the US-Mexico border. BMC Public Health 2019, 19, 759. [Google Scholar] [CrossRef] [Green Version]
- Crespo, N.C.; Elder, J.P.; Ayala, G.X.; Slymen, D.J.; Campbell, N.R.; Sallis, J.F.; McKenzie, T.L.; Baquero, B.; Arredondo, E.M. Results of a multi-level intervention to prevent and control childhood obesity among Latino children: The Aventuras Para Niños Study. Ann. Behav. Med. 2012, 43, 84–100. [Google Scholar] [CrossRef] [Green Version]
- Davis, J.N.; Perez, A.; Asigbee, F.M.; Landry, M.J.; Vandyousefi, S.; Ghaddar, R.; Hoover, A.; Jeans, M.; Nikah, K.; Fischer, B.; et al. School-based gardening, cooking and nutrition intervention increased vegetable intake but did not reduce BMI: Texas sprouts—A cluster randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 18. [Google Scholar] [CrossRef] [PubMed]
- Barragan, M.; Luna, V.; Hammons, A.J.; Olvera, N.; Greder, K.; Drumond Andrade, F.C.; Fiese, B.; Wiley, A.; Teran-Garcia, M. The Abriendo Caminos Research Team, Reducing obesogenic eating behaviors in Hispanic children through a family-based, culturally-tailored RCT: Abriendo Caminos. Int. J. Environ. Res. Public Health 2022, 19, 1917. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S.; Taki, S.; Laird, Y.; Love, P.; Wen, L.M.; Rissel, C. Cultural adaptations of obesity-related behavioral prevention interventions in early childhood: A systematic review. Obes. Rev. 2022, 23, e13402. [Google Scholar] [CrossRef]
- Diaz, V.A.; Mainous, A.G., III; Pope, C. Cultural conflicts in the weight loss experience of overweight Latinos. Int. J. Obes. 2007, 31, 328–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lukas, C.V.; Cunningham-Sabo, L. Qualitative investigation of the Cooking with Kids program: Focus group interviews with fourth-grade students, teachers, and food educators. J. Nutr. Educ. Behav. 2011, 43, 517–524. [Google Scholar] [CrossRef]
- Davison, K.K.; Lawson, H.A.; Coatsworth, J.D. The Family-centered action model of intervention layout and implementation (FAMILI): The example of childhood obesity. Health Promot. Pract. 2012, 13, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.M.; Sharkey, J.R.; Umstattd Meyer, M.R.; Gómez, L.; Allicock, M.A.; Prochnow, T.; Beltrán, E.; Martinez, L. Designing for multilevel behavior change: A father-focused nutrition and physical activity program for Mexican-heritage families in south Texas border communities. Int. J. Environ. Res. Public Health 2021, 18, 10117. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.M.; Allicock, M.A.; Sharkey, J.R.; Umstattd Meyer, M.R.; Gomez, L.; Prochnow, T.; Laviolette, C.; Beltran, E.; Garza, L.M. Promotoras de salud in a father-focused nutrition and physical activity program for border communities: Approaches and lessons learned from collaboration. Int. J. Environ. Res. Public Health 2022, 19, 11660. [Google Scholar] [CrossRef]
- Prochnow, T.; Umstattd Meyer, M.R.; Johnson, C.; Delgado, H.; Gómez, L.; Sharkey, J. The development and pilot testing of the ¡Haz Espacio Para Papi! program physical activity curriculum for Mexican-heritage fathers and children. Am. J. Health Educ. 2021, 52, 145–153. [Google Scholar] [CrossRef]
- Balls-Berry, J.E.; Acosta-Pérez, E. The use of community engaged research principles to improve health: Community academic partnerships for research. P. R. Health Sci. J. 2017, 36, 84–85. [Google Scholar]
- Barkin, S.; Schlundt, D.; Smith, P. Community-engaged research perspectives: Then and now. Acad. Pediatr. 2013, 13, 93–97. [Google Scholar] [CrossRef]
- Panter-Brick, C.; Burgess, A.; Eggerman, M.; McAllister, F.; Pruett, K.; Leckman, J.F. Practitioner review: Engaging fathers—Recommendations for a game change in parenting interventions based on a systematic review of the global evidence. J. Child Psychol. Psychiatry 2014, 55, 1187–1212. [Google Scholar] [CrossRef] [PubMed]
- Davison, K.K.; Gicevic, S.; Aftosmes-Tobio, A.; Ganter, C.; Simon, C.L.; Newlan, S.; Manganello, J.A. Fathers’ representation in observational studies on parenting and childhood obesity: A systematic review and content analysis. Am. J. Public Health 2016, 106, e14–e21. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.J.; Young, M.D. The influence of fathers on children’s physical activity and dietary behaviors: Insights, recommendations and future directions. Curr. Obes. Rep. 2017, 6, 324–333. [Google Scholar] [CrossRef]
- Morgan, P.J.; Young, M.D.; Lloyd, A.B.; Wang, M.L.; Eather, N.; Miller, A.; Murtagh, E.M.; Barnes, A.T.; Pagoto, S.L. Involvement of fathers in pediatric obesity treatment and prevention trials: A systematic review. Pediatrics 2017, 139, e20162635. [Google Scholar] [CrossRef]
- Davison, K.K.; Kitos, N.; Aftosmes-Tobio, A.; Ash, T.; Agaronov, A.; Sepulveda, M.; Haines, J. The forgotten parent: Fathers’ representation in family interventions to prevent childhood obesity. Prev. Med. 2018, 111, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Duerksen, S.; Campbell, N.; Arredondo, E.; Ayala, G.; Baquero, B.; Elder, J. Aventuras para Niños: Obesity prevention in the homes, schools, and neighborhoods of Mexican American children. In Obesity in Europe: Young People’s Physical Activity and Sedentary Lifestyles; Peter Lang: Frankfurt, Germany, 2007; pp. 135–152. [Google Scholar]
- Vollmer, R.L.; Adamsons, K.; Mobley, A.R. Recruitment, engagement, and retention of fathers in nutrition education and obesity research. J. Nutr. Educ. Behav. 2019, 51, 1121–1125. [Google Scholar] [CrossRef]
- Miller, A.; Franzen-Castle, L.; Aguirre, T.; Krehbiel, M.; Colby, S.; Kattelmann, K.; Olfert, M.D.; Mathews, D.; White, A. Food-related behavior and intake of adult main meal preparers of 9-10 year-old children participating in iCook 4-H: A five-state childhood obesity prevention pilot study. Appetite 2016, 101, 163–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krahnstoever Davison, K.; Campbell, K. Opportunities to prevent obesity in children within families: An ecological approach. In Obesity Prevention and Public Health; Oxford Univeristy Press: Oxford, UK, 2005; pp. 208–230. [Google Scholar]
- Lehr, W.; Kantor, D. Inside the Family; Jossey-Bass: San Francisco, CA, USA, 1975. [Google Scholar]
- Glanz, K.; Rimer, B.K.; Viswanath, K. (Eds.) Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Jossey-Bass: San Francisco, CA, USA, 2008. [Google Scholar]
- Coleman-Jensen, A.; Rabbitt, M.P.; Gregory, C.A.; Singh, A. Household Food Security in the United States in 2021; U.S. Department of Agriculture (USDA), Economic Research Service: Washington, DC, USA, 2022.
- Hager, E.R.; Quigg, A.M.; Black, M.M.; Coleman, S.M.; Heeren, T.; Rose-Jacobs, R.; Cook, J.T.; Ettinger de Cuba, S.A.; Casey, P.H.; Chilton, M.; et al. Development and validity of a 2-item screen to identify families at risk for food insecurity. Pediatrics 2010, 126, e26–e32. [Google Scholar] [CrossRef] [Green Version]
- Longevity Link Corporation. The Veggie Meter® Non-Invasive Optical Biomarker for Personal Health. Available online: http://www.longevitylinkcorporation.com/home.html (accessed on 16 January 2023).
- Jahns, L.; Johnson, L.K.; Conrad, Z.; Bukowski, M.; Raatz, S.K.; Jilcott Pitts, S.; Wang, Y.; Ermakov, I.V.; Gellermann, W. Concurrent validity of skin carotenoid status as a concentration biomarker of vegetable and fruit intake compared to multiple 24-h recalls and plasma carotenoid concentrations across one year: A cohort study. Nutr. J. 2019, 18, 78. [Google Scholar] [CrossRef] [Green Version]
- Radtke, M.D.; Poe, M.; Stookey, J.; Jilcott Pitts, S.; Moran, N.E.; Landry, M.J.; Rubin, L.P.; Stage, V.C.; Scherr, R.E. Recommendations for the use of the Veggie Meter® for spectroscopy-based skin carotenoid measurements in the research setting. Curr. Dev. Nutr. 2021, 5, nzab104. [Google Scholar] [CrossRef] [PubMed]
- Jilcott Pitts, S.B.; Jahns, L.; Wu, Q.; Moran, N.E.; Bell, R.A.; Truesdale, K.P.; Laska, M.N. A non-invasive assessment of skin carotenoid status through reflection spectroscopy is a feasible, reliable and potentially valid measure of fruit and vegetable consumption in a diverse community sample. Public Health Nutr. 2018, 21, 1664–1670. [Google Scholar] [CrossRef] [Green Version]
- Ermakov, I.V.; Ermakova, M.; Sharifzadeh, M.; Gorusupudi, A.; Farnsworth, K.; Bernstein, P.S.; Stookey, J.; Evans, J.; Arana, T.; Tao-Lew, L.; et al. Optical assessment of skin carotenoid status as a biomarker of vegetable and fruit intake. Arch. Biochem. Biophys. 2018, 646, 46–54. [Google Scholar] [CrossRef]
- Jilcott Pitts, S.B.; Moran, N.E.; Wu, Q.; Harnack, L.; Craft, N.E.; Hanchard, N.; Bell, R.; Moe, S.G.; Johnson, N.; Obasohan, J.; et al. Pressure-mediated reflection spectroscopy criterion validity as a biomarker of fruit and vegetable intake: A 2-site cross-sectional study of 4 racial or ethnic groups. J. Nutr. 2022, 152, 107–116. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). A SAS Program for the 2000 CDC Growth Charts (ages 0 to <20 years). Available online: https://www.cdc.gov/nccdphp/dnpao/growthcharts/resources/sas.htm (accessed on 12 December 2022).
- Centers for Disease Control and Prevention (CDC). National Health and Nutrition Examination Survey. NHANES Procedure Manuals. Available online: https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/manuals.aspx?Cycle=2021-2022 (accessed on 17 March 2023).
- Cunningham-Sabo, L.; Lohse, B. Impact of a school-based cooking curriculum for fourth-grade students on attitudes and behaviors is influenced by gender and prior cooking experience. J. Nutr. Educ. Behav. 2014, 46, 110–120. [Google Scholar] [CrossRef]
- Hemming, K.; Haines, T.P.; Chilton, P.J.; Girling, A.J.; Lilford, R.J. The stepped wedge cluster randomised trial: Rationale, design, analysis, and reporting. BMJ 2015, 350, h391. [Google Scholar] [CrossRef] [Green Version]
- Hussey, M.A.; Hughes, J.P. Design and analysis of stepped wedge cluster randomized trials. Contemp. Clin. Trials 2007, 28, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Equator Network (Enhancing the QUAlity and Transparency of Health Research). The CONSORT Statement. Available online: https://www.equator-network.org/reporting-guidelines/consort/ (accessed on 1 March 2023).
- Pai, S.; Bahadur, K. The impact of food insecurity on child health. Pediatr. Clin. N. Am. 2020, 67, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Community Eligibility Provision. Available online: https://www.fns.usda.gov/cn/community-eligibility-provision (accessed on 3 March 2023).
- Cullen, K.W.; Dave, J.M. The new federal school nutrition standards and meal patterns: Early evidence examining the influence on student dietary behavior and the school food environment. J. Acad. Nutr. Diet 2017, 117, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.F.; Richardson, S.; Parker, E.; Catalano, P.J.; Rimm, E.B. Impact of the new U.S. Department of Agriculture school meal standards on food selection, consumption, and waste. Am. J. Prev. Med. 2014, 46, 388–394. [Google Scholar] [CrossRef] [Green Version]
- Robinson-O’Brien, R.; Burgess-Champoux, T.; Haines, J.; Hannan, P.J.; Neumark-Sztainer, D. Associations between school meals offered through the National School Lunch Program and the School Breakfast Program and fruit and vegetable intake among ethnically diverse, low-income children. J. Sch. Health 2010, 80, 487–492. [Google Scholar] [CrossRef] [Green Version]
- Di Noia, J.; Gellermann, W. Use of the spectroscopy-based Veggie Meter® to objectively assess fruit and vegetable intake in low-income adults. Nutrients 2021, 13, 2270. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, S.; Acciai, F.; Tasevska, N.; Ohri-Vachaspati, P. Using the Veggie Meter in elementary schools to objectively measure fruit and vegetable intake: A pilot study. Methods Protoc. 2021, 4, 33. [Google Scholar] [CrossRef]
- Scarmo, S.; Henebery, K.; Peracchio, H.; Cartmel, B.; Lin, H.; Ermakov, I.V.; Gellermann, W.; Bernstein, P.S.; Duffy, V.B.; Mayne, S.T. Skin carotenoid status measured by resonance Raman spectroscopy as a biomarker of fruit and vegetable intake in preschool children. Eur. J. Clin. Nutr. 2012, 66, 555–560. [Google Scholar] [CrossRef] [Green Version]
- Aguilera, A.L.; Stewart, C.P.; de la Torre, A.; Kaiser, L.L. Feasibility of skin carotenoids as a biomarker of vegetable intake among Mexican-origin children in a community setting: A cross-sectional pilot study. J. Epidemiol. Res. 2017, 4, 1–7. [Google Scholar] [CrossRef]
- Jones, A.M.; Keihner, A.; Mills, M.; MkNelly, B.; Khaira, K.K.; Pressman, J.; Scherr, R.E. Measuring skin carotenoids using reflection spectroscopy in a low-income school setting. Nutrients 2021, 13, 3796. [Google Scholar] [CrossRef]
- Gallo, S.; Jones, M.T.; Channell Doig, A.; Kogan, K.; Fields, J.; Wonderlich, J.A.; Hansen, A.; LaCharite, K.; Mehlenbeck, R. Feasibility of a multidisciplinary and culturally adapted pediatric weight management program for Latino families: Results from the Vidas Activas y Familias Saludables pilot study. J. Nutr. Educ. Behav. 2020, 52, 55–63. [Google Scholar] [CrossRef]
- Robinson, T.N.; Matheson, D.; Wilson, D.M.; Weintraub, D.L.; Banda, J.A.; McClain, A.; Sanders, L.M.; Haskell, W.L.; Haydel, K.F.; Kapphahn, K.I.; et al. A community-based, multi-level, multi-setting, multi-component intervention to reduce weight gain among low socioeconomic status Latinx children with overweight or obesity: The Stanford GOALS randomised controlled trial. Lancet Diabetes Endocrinol. 2021, 9, 336–349. [Google Scholar] [CrossRef]
- Kolotourou, M.; Radley, D.; Chadwick, P.; Smith, L.; Orfanos, S.; Kapetanakis, V.; Singhal, A.; Cole, T.J.; Sacher, P.M. Is BMI alone a sufficient outcome to evaluate interventions for child obesity? Child. Obes. 2013, 9, 350–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, A.L.; Hunt, L.P.; Cooper, A.; Shield, J.P. What reduction in BMI SDS is required in obese adolescents to improve body composition and cardiometabolic health? Arch. Dis. Child. 2010, 95, 256–261. [Google Scholar] [CrossRef]
- Aguilar, S.S.; Wengreen, H.J.; Dew, J. Skin carotenoid response to a high-carotenoid juice in children: A randomized clinical trial. J. Acad. Nutr. Diet 2015, 115, 1771–1778. [Google Scholar] [CrossRef] [PubMed]
- Shimokawa, M.A.L.; Siu, A.M.; Choi, S.Y.; Davis, J. The NEW Keiki program reduces BMI z-scores among overweight and obese children and BMI among their adult caregivers in Hawai’i. Hawaii J. Health Soc. Welf. 2020, 79 (Suppl. S1), 24–31. [Google Scholar]
- Overcash, F.; Ritter, A.; Mann, T.; Mykerezi, E.; Redden, J.; Rendahl, A.; Vickers, Z.; Reicks, M. Impacts of a vegetable cooking skills program among low-income parents and children. J. Nutr. Educ. Behav. 2018, 50, 795–802. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, T.M.; Perez, O.; Beltran, A.; Colón García, I.; Arredondo, E.; Parra Cardona, R.; Cabrera, N.; Thompson, D.; Baranowski, T.; Morgan, P.J. Cultural adaptation of ‘Healthy Dads, Healthy Kids’ for Hispanic families: Applying the ecological validity model. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 52. [Google Scholar] [CrossRef] [Green Version]
- Baltaci, A.; Hurtado Choque, G.A.; Davey, C.; Reyes Peralta, A.; Alvarez de Davila, S.; Zhang, Y.; Gold, A.; Larson, N.; Reicks, M. Padres Preparados, Jóvenes Saludables: Intervention impact of a randomized controlled trial on Latino father and adolescent energy balance-related behaviors. BMC Public Health 2022, 22, 1932. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.J.; Collins, C.E.; Plotnikoff, R.C.; Callister, R.; Burrows, T.; Fletcher, R.; Okely, A.D.; Young, M.D.; Miller, A.; Lloyd, A.B.; et al. The ‘Healthy Dads, Healthy Kids’ community randomized controlled trial: A community-based healthy lifestyle program for fathers and their children. Prev. Med. 2014, 61, 90–99. [Google Scholar] [CrossRef]
- Morgan, P.J.; Lubans, D.R.; Callister, R.; Okely, A.D.; Burrows, T.L.; Fletcher, R.; Collins, C.E. The ‘Healthy Dads, Healthy Kids’ randomized controlled trial: Efficacy of a healthy lifestyle program for overweight fathers and their children. Int. J. Obes. 2011, 35, 436–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, M.L.; Kenward, M.G.; Fairclough, D.L.; Horton, N.J. Differential dropout and bias in randomised controlled trials: When it matters and when it may not. BMJ 2013, 346, e8668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connell, N.S.; Dai, L.; Jiang, Y.; Speiser, J.L.; Ward, R.; Wei, W.; Carroll, R.; Gebregziabher, M. Methods for analysis of pre-post data in clinical research: A comparison of five common methods. J. Biom. Biostat. 2017, 8, 1–8. [Google Scholar]
- Natarajan, L.; Flatt, S.W.; Sun, X.; Gamst, A.C.; Major, J.M.; Rock, C.L.; Al-Delaimy, W.; Thomson, C.A.; Newman, V.A.; Pierce, J.P. Validity and systematic error in measuring carotenoid consumption with dietary self-report instruments. Am. J. Epidemiol. 2006, 163, 770–778. [Google Scholar] [CrossRef] [PubMed]
- Marshall, A.N.; Markham, C.; Ranjit, N.; Bounds, G.; Chow, J.; Sharma, S.V. Long-term impact of a school-based nutrition intervention on home nutrition environment and family fruit and vegetable intake: A two-year follow-up study. Prev. Med. Rep. 2020, 20, 101247. [Google Scholar] [CrossRef] [PubMed]
- Zarnowiecki, D.M.; Dollman, J.; Parletta, N. Associations between predictors of children’s dietary intake and socioeconomic position: A systematic review of the literature. Obes. Rev. 2014, 15, 375–391. [Google Scholar] [CrossRef] [PubMed]
- Appleton, K.M.; Hemingway, A.; Saulais, L.; Dinnella, C.; Monteleone, E.; Depezay, L.; Morizet, D.; Armando Perez-Cueto, F.J.; Bevan, A.; Hartwell, H. Increasing vegetable intakes: Rationale and systematic review of published interventions. Eur. J. Nutr. 2016, 55, 869–896. [Google Scholar] [CrossRef] [Green Version]
- Jones, R.A.; Sinn, N.; Campbell, K.J.; Hesketh, K.; Denney-Wilson, E.; Morgan, P.J.; Lubans, D.R.; Magarey, A. The importance of long-term follow-up in child and adolescent obesity prevention interventions. Int. J. Pediatr. Obes. 2011, 6, 178–181. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Agriculture (USDA). Food and Nutrition Security. Available online: https://www.usda.gov/nutrition-security (accessed on 3 March 2023).


| Characteristics | Total | Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | p-Value |
|---|---|---|---|---|---|---|---|
| Number of children, n | 57 | 12 | 10 | 12 | 12 | 11 | |
| Child | |||||||
| Mexican-heritage ethnicity | 57 (100%) | 9 (100%) | 10 (100%) | 12 (100%) | 12 (100%) | 11 (100%) | |
| Age | 10.21 ± 0.94 | 10.26 ± 0.27 | 10.36 ± 0.3 | 10.1 ± 0.27 | 10.52 ± 0.27 | 9.8 ± 0.28 | |
| Sex | 0.203 | ||||||
| Male | 27 (47.37%) | 5 (41.67%) | 3 (30%) | 9 (75%) | 4 (33.33%) | 6 (54.55%) | |
| Female | 30 (52.63%) | 7 (58.33%) | 7 (70%) | 3 (25%) | 8 (66.67%) | 5 (45.45%) | |
| Instant skin carotenoid score (biomarker for dietary intake of fruits and vegetables) | 213.54 ± 61.57 | 242.63 ± 17.77 | 208.7 ± 19.46 | 213.79 ± 17.77 | 194.46 ± 17.77 | 206.77 ± 18.56 | |
| BMI z-score | 1.14 ± 1.15 | 0.9 ± 0.34 | 1.05 ± 0.37 | 1.2 ± 0.34 | 1.35 ± 0.34 | 1.21 ± 0.36 | |
| BMI percentile | 77.57 ± 27.89 | 69.04 ± 8.21 | 74.26 ± 8.99 | 81.24 ± 8.21 | 82.84 ± 8.21 | 80.12 ± 8.57 | |
| BMI categories | 0.997 | ||||||
| <85th percentile | 22 (38.6%) | 6 (50%) | 4 (40%) | 4 (33.33%) | 4 (33.33%) | 4 (36.36%) | |
| 85th to <95th percentile | 11 (19.3%) | 2 (16.67%) | 2 (20%) | 2 (16.67%) | 3 (25%) | 2 (18.18%) | |
| ≥95th percentile | 24 (42.11%) | 4 (33.33%) | 4 (40%) | 6 (50%) | 5 (45.45%) | 5 (45.45%) | |
| Household food insecurity | 0.154 | ||||||
| Food Secure | 18 (31.58%) | 3 (25%) | 5 (50%) | 2 (16.67%) | 2 (16.67%) | 6 (54.55%) | |
| Food Insecure | 39 (68.42%) | 9 (75%) | 5 (50%) | 10 (83.33%) | 10 (83.33%) | 5 (45.45%) |
| Unadjusted Models | Adjusted Models | |||
|---|---|---|---|---|
| Outcome | Estimate | (95% CI) | Estimate | (95% CI) |
| Change in instant skin carotenoid score | −14.67 | (−30.9, 1.56) | −15.14 | (−24.95, −5.33) |
| Change in BMI percentile | −0.18 | (−2.16, 1.79) | −0.20 | (−0.89, 0.49) |
| Change in BMI z-score | −0.02 | (−0.1, 0.06) | −0.02 | (−0.05, 0.00) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laviolette, C.; Johnson, C.M.; Butler, J.L.; Biediger-Friedman, L.; Sharkey, J.R. Nutrition Effects of a Family-Centered Health Promotion Program for Mexican-Heritage Children in the Lower Rio Grande Valley of Texas. Nutrients 2023, 15, 1600. https://doi.org/10.3390/nu15071600
Laviolette C, Johnson CM, Butler JL, Biediger-Friedman L, Sharkey JR. Nutrition Effects of a Family-Centered Health Promotion Program for Mexican-Heritage Children in the Lower Rio Grande Valley of Texas. Nutrients. 2023; 15(7):1600. https://doi.org/10.3390/nu15071600
Chicago/Turabian StyleLaviolette, Chelsey, Cassandra M. Johnson, J. Lauren Butler, Lesli Biediger-Friedman, and Joseph R. Sharkey. 2023. "Nutrition Effects of a Family-Centered Health Promotion Program for Mexican-Heritage Children in the Lower Rio Grande Valley of Texas" Nutrients 15, no. 7: 1600. https://doi.org/10.3390/nu15071600