

Serum 25-Hydroxyvitamin D Is Differentially Associated with Early and Late Age-Related Macular Degeneration in the United States Population

Abstract
:1. Introduction
2. Materials and Methods
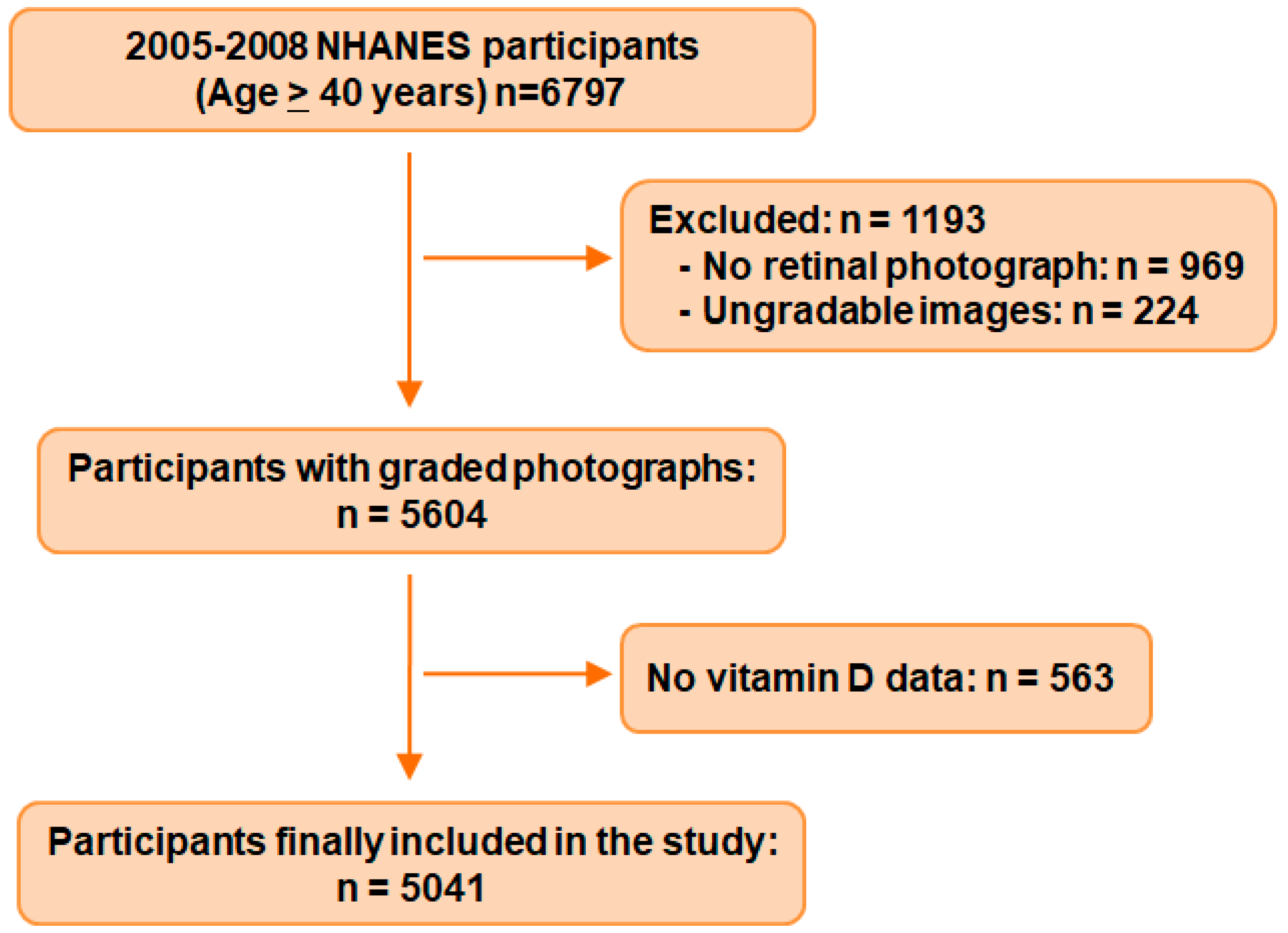
2.1. Sample and Population
2.2. Age-Related Macular Degeneration Grading
2.3. Measurement of Vitamin D
2.4. Covariates
2.5. Statistics Analysis
3. Results
3.1. General Characteristics of the Sample Population
3.2. Association of AMD and Serum 25(OH)D Level in the Whole Population
3.3. Association of AMD and Serum 25(OH)D Stratified by Age
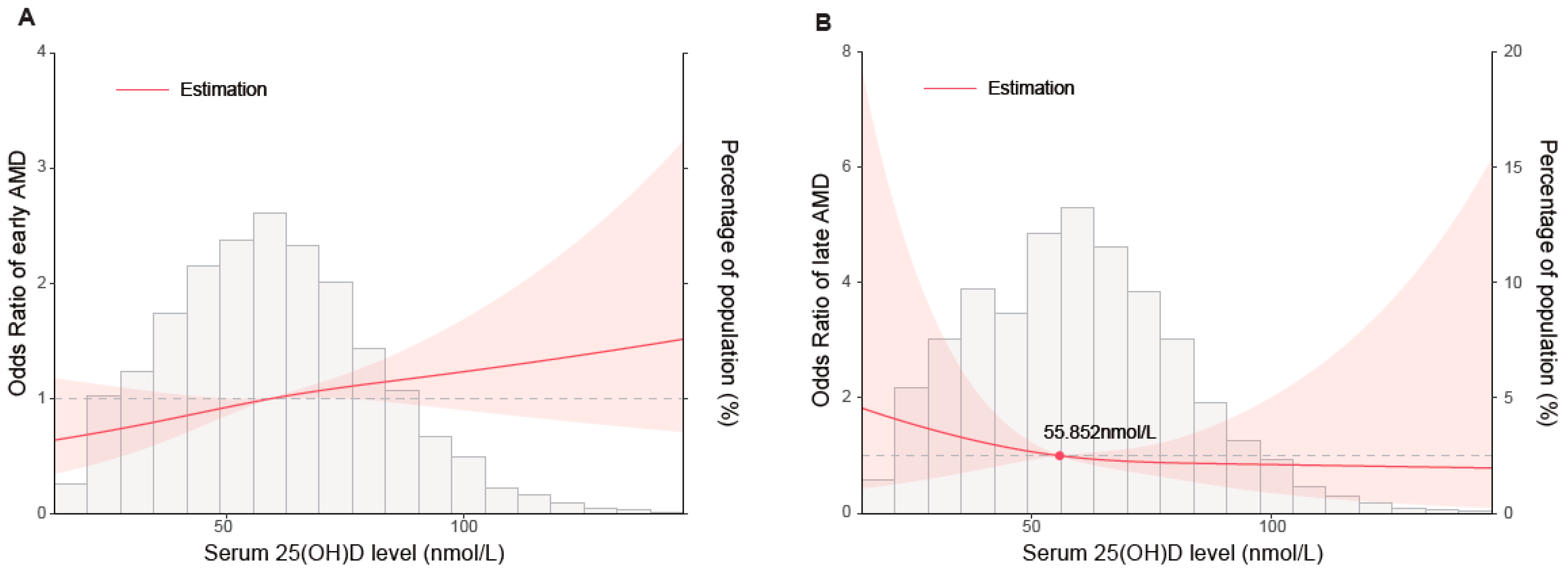
3.4. Restricted Cubic Spline Analysis
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jager, R.D.; Mieler, W.F.; Miller, J.W. Age-related macular degeneration. N. Engl. J. Med. 2008, 358, 2606–2617. [Google Scholar] [CrossRef] [Green Version]
- Fleckenstein, M.; Keenan, T.D.L.; Guymer, R.H.; Chakravarthy, U.; Schmitz-Valckenberg, S.; Klaver, C.C.; Wong, W.T.; Chew, E.Y. Age-related macular degeneration. Nat. Rev. Dis. Prim. 2021, 7, 31. [Google Scholar] [CrossRef]
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.; Klein, R.; Cheng, C.Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, P.; Liew, G.; Gopinath, B.; Wong, T.Y. Age-related macular degeneration. Lancet 2018, 392, 1147–1159. [Google Scholar] [CrossRef]
- Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E and beta carotene for age-related cataract and vision loss: AREDS report no. 9. Arch. Ophthalmol. 2001, 119, 1439–1452. [Google Scholar] [CrossRef]
- Arnold, C.; Winter, L.; Frohlich, K.; Jentsch, S.; Dawczynski, J.; Jahreis, G.; Bohm, V. Macular xanthophylls and omega-3 long-chain polyunsaturated fatty acids in age-related macular degeneration: A randomized trial. JAMA Ophthalmol. 2013, 131, 564–572. [Google Scholar] [CrossRef]
- Mares, J.A.; Voland, R.P.; Sondel, S.A.; Millen, A.E.; Larowe, T.; Moeller, S.M.; Klein, M.L.; Blodi, B.A.; Chappell, R.J.; Tinker, L.; et al. Healthy lifestyles related to subsequent prevalence of age-related macular degeneration. Arch. Ophthalmol. 2011, 129, 470–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Layana, A.G.; Minnella, A.M.; Garhofer, G.; Aslam, T.; Holz, F.G.; Leys, A.; Silva, R.; Delcourt, C.; Souied, E.; Seddon, J.M. Vitamin D and Age-Related Macular Degeneration. Nutrients 2017, 9, 1120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christakos, S.; Dhawan, P.; Verstuyf, A.; Verlinden, L.; Carmeliet, G. Vitamin D: Metabolism, Molecular Mechanism of Action, and Pleiotropic Effects. Physiol. Rev. 2016, 96, 365–408. [Google Scholar] [CrossRef] [Green Version]
- Zerwekh, J.E. Blood biomarkers of vitamin D status. Am. J. Clin. Nutr. 2008, 87, 1087S–1091S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, G.; Prosser, D.E.; Kaufmann, M. 25-Hydroxyvitamin D-24-hydroxylase (CYP24A1): Its important role in the degradation of vitamin D. Arch. Biochem. Biophys. 2012, 523, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Plum, L.A.; DeLuca, H.F. Vitamin D, disease and therapeutic opportunities. Nat. Rev. Drug Discov. 2010, 9, 941–955. [Google Scholar] [CrossRef] [PubMed]
- Zmijewski, M.A. Vitamin D and Human Health. Int. J. Mol. Sci. 2019, 20, 145. [Google Scholar] [CrossRef] [Green Version]
- Chan, H.N.; Zhang, X.J.; Ling, X.T.; Bui, C.H.; Wang, Y.M.; Ip, P.; Chu, W.K.; Chen, L.J.; Tham, C.C.; Yam, J.C.; et al. Vitamin D and Ocular Diseases: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 4226. [Google Scholar] [CrossRef] [PubMed]
- Tohari, A.M.; Alhasani, R.H.; Biswas, L.; Patnaik, S.R.; Reilly, J.; Zeng, Z.; Shu, X. Vitamin D Attenuates Oxidative Damage and Inflammation in Retinal Pigment Epithelial Cells. Antioxidants 2019, 8, 341. [Google Scholar] [CrossRef] [Green Version]
- Hewison, M. Vitamin D and the immune system: New perspectives on an old theme. Endocrinol. Metab. Clin. N. Am. 2010, 39, 365–379. [Google Scholar] [CrossRef] [Green Version]
- Albert, D.M.; Scheef, E.A.; Wang, S.; Mehraein, F.; Darjatmoko, S.R.; Sorenson, C.M.; Sheibani, N. Calcitriol is a potent inhibitor of retinal neovascularization. Investig. Ophthalmol. Vis. Sci. 2007, 48, 2327–2334. [Google Scholar] [CrossRef] [Green Version]
- Parekh, N.; Chappell, R.J.; Millen, A.E.; Albert, D.M.; Mares, J.A. Association between vitamin D and age-related macular degeneration in the Third National Health and Nutrition Examination Survey, 1988 through 1994. Arch. Ophthalmol. 2007, 125, 661–669. [Google Scholar] [CrossRef] [Green Version]
- Millen, A.E.; Nie, J.; Mares, J.A.; Lutsey, P.L.; LaMonte, M.J.; Meuer, S.M.; Sahli, M.W.; Andrews, C.A.; Klein, B.E.K.; Klein, R. Serum 25-Hydroxyvitamin D Concentrations and Incidence of Age-Related Macular Degeneration: The Atherosclerosis Risk in Communities Study. Investig. Ophthalmol. Vis. Sci. 2019, 60, 1362–1371. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.C.; Han, K.; Jee, D. Inverse relationship between high blood 25-hydroxyvitamin D and late stage of age-related macular degeneration in a representative Korean population. Investig. Ophthalmol. Vis. Sci. 2014, 55, 4823–4831. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.L.; Park, S.P. Association between serum vitamin D deficiency and age-related macular degeneration in Koreans: Clinical case-control pilot study. Medicine 2018, 97, e11908. [Google Scholar] [CrossRef]
- Ferreira, A.; Silva, N.; Furtado, M.J.; Carneiro, A.; Lume, M.; Andrade, J.P. Serum vitamin D and age-related macular degeneration: Systematic review and meta-analysis. Surv. Ophthalmol. 2021, 66, 183–197. [Google Scholar] [CrossRef]
- Wu, W.; Weng, Y.; Guo, X.; Feng, L.; Xia, H.; Jiang, Z.; Lou, J. The Association Between Serum Vitamin D Levels and Age-Related Macular Degeneration: A Systematic Meta-Analytic Review. Investig. Ophthalmol. Vis. Sci. 2016, 57, 2168–2177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, J.; Jaleel, T.; MacLeod, A.S.; Ji, J.S. Inverted U-shaped relationship between vitamin D and ever-reported eczema in US adults. Allergy 2019, 74, 964–975. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Q.; Cai, B.; Yin, A.; Huo, H.; Lan, K.; Zhou, G.; Shen, L.; He, B. L-shaped association of serum 25-hydroxyvitamin D concentrations with cardiovascular and all-cause mortality in individuals with osteoarthritis: Results from the NHANES database prospective cohort study. BMC Med. 2022, 20, 308. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, I.; Haynes, B. Reporting, updating, and correcting systematic reviews of the effects of health care. Br. Med. J. 1994, 309, 862–865. [Google Scholar] [CrossRef]
- Klein, R.; Klein, B.E.; Jensen, S.C.; Mares-Perlman, J.A.; Cruickshanks, K.J.; Palta, M. Age-related maculopathy in a multiracial United States population: The National Health and Nutrition Examination Survey III. Ophthalmology 1999, 106, 1056–1065. [Google Scholar] [CrossRef] [PubMed]
- Walpole, S.; Pritchard, A.L.; Cebulla, C.M.; Pilarski, R.; Stautberg, M.; Davidorf, F.H.; de la Fouchardiere, A.; Cabaret, O.; Golmard, L.; Stoppa-Lyonnet, D.; et al. Comprehensive Study of the Clinical Phenotype of Germline BAP1 Variant-Carrying Families Worldwide. J. Natl. Cancer Inst. 2018, 110, 1328–1341. [Google Scholar] [CrossRef]
- Cortes Alvarez, S.I.; Flores-Ruelas, Y.; Del Toro-Equihua, M.; Perez-Manzo, L.; Delgado-Enciso, I.; Sanchez-Ramirez, C.A. Serum 25-Hydroxyvitamin D correlates with systolic blood pressure in obese male schoolchildren. Nutr. Hosp 2022, 39, 562–568. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2018, 138, e426–e483. [Google Scholar] [CrossRef]
- rcssci: Visualization of Restricted Cubic Splines. Available online: https://cran.r-project.org/web/packages/rcssci/index.html (accessed on 23 February 2023).
- Millen, A.E.; Voland, R.; Sondel, S.A.; Parekh, N.; Horst, R.L.; Wallace, R.B.; Hageman, G.S.; Chappell, R.; Blodi, B.A.; Klein, M.L.; et al. Vitamin D status and early age-related macular degeneration in postmenopausal women. Arch. Ophthalmol. 2011, 129, 481–489. [Google Scholar] [CrossRef]
- Schick, T.; Ersoy, L.; Lechanteur, Y.T.; Saksens, N.T.; Hoyng, C.B.; den Hollander, A.I.; Kirchhof, B.; Fauser, S. History of Sunlight Exposure Is a Risk Factor for Age-Related Macular Degeneration. Retina 2016, 36, 787–790. [Google Scholar] [CrossRef] [PubMed]
- Sui, G.Y.; Liu, G.C.; Liu, G.Y.; Gao, Y.Y.; Deng, Y.; Wang, W.Y.; Tong, S.H.; Wang, L. Is sunlight exposure a risk factor for age-related macular degeneration? A systematic review and meta-analysis. Br. J. Ophthalmol. 2013, 97, 389–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annweiler, C.; Drouet, M.; Duval, G.T.; Pare, P.Y.; Leruez, S.; Dinomais, M.; Milea, D. Circulating vitamin D concentration and age-related macular degeneration: Systematic review and meta-analysis. Maturitas 2016, 88, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Seddon, J.M.; Reynolds, R.; Shah, H.R.; Rosner, B. Smoking, dietary betaine, methionine, and vitamin D in monozygotic twins with discordant macular degeneration: Epigenetic implications. Ophthalmology 2011, 118, 1386–1394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merle, B.M.J.; Silver, R.E.; Rosner, B.; Seddon, J.M. Associations Between Vitamin D Intake and Progression to Incident Advanced Age-Related Macular Degeneration. Investig. Opthalmol. Vis. Sci. 2017, 58, 4569–4578. [Google Scholar] [CrossRef] [Green Version]
- Chung, I.; Yu, W.D.; Karpf, A.R.; Flynn, G.; Bernardi, R.J.; Modzelewski, R.A.; Johnson, C.S.; Trump, D.L. Anti-proliferative effects of calcitriol on endothelial cells derived from two different microenvironments. J. Steroid Biochem. Mol. Biol. 2007, 103, 768–770. [Google Scholar] [CrossRef]
- Annweiler, C.; Schott, A.M.; Berrut, G.; Chauvire, V.; Le Gall, D.; Inzitari, M.; Beauchet, O. Vitamin D and ageing: Neurological issues. Neuropsychobiology 2010, 62, 139–150. [Google Scholar] [CrossRef]
- Singh, A.; Falk, M.K.; Subhi, Y.; Sorensen, T.L. The association between plasma 25-hydroxyvitamin D and subgroups in age-related macular degeneration: A cross-sectional study. PLoS ONE 2013, 8, e70948. [Google Scholar] [CrossRef] [PubMed]
- Seddon, J.M.; Gensler, G.; Milton, R.C.; Klein, M.L.; Rifai, N. Association between C-reactive protein and age-related macular degeneration. JAMA 2004, 291, 704–710. [Google Scholar] [CrossRef]
- Seddon, J.M.; Gensler, G.; Klein, M.L.; Milton, R.C. C-reactive protein and homocysteine are associated with dietary and behavioral risk factors for age-related macular degeneration. Nutrition 2006, 22, 441–443. [Google Scholar] [CrossRef]
- Kennel, K.A.; Drake, M.T.; Hurley, D.L. Vitamin D deficiency in adults: When to test and how to treat. Mayo Clin. Proc. 2010, 85, 752–757. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, J.; Cooper, S.C.; Ghosh, S.; Hewison, M. The Role of Vitamin D in Inflammatory Bowel Disease: Mechanism to Management. Nutrients 2019, 11, 1019. [Google Scholar] [CrossRef] [Green Version]
- Zinkernagel, M.S.; Zysset-Burri, D.C.; Keller, I.; Berger, L.E.; Leichtle, A.B.; Largiader, C.R.; Fiedler, G.M.; Wolf, S. Association of the Intestinal Microbiome with the Development of Neovascular Age-Related Macular Degeneration. Sci. Rep. 2017, 7, 40826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, P.; McClintic, S.M.; Nadeem, U.; Skondra, D. A Review of the Role of the Intestinal Microbiota in Age-Related Macular Degeneration. J. Clin. Med. 2021, 10, 2072. [Google Scholar] [CrossRef] [PubMed]
- Rinninella, E.; Mele, M.C.; Merendino, N.; Cintoni, M.; Anselmi, G.; Caporossi, A.; Gasbarrini, A.; Minnella, A.M. The Role of Diet, Micronutrients and the Gut Microbiota in Age-Related Macular Degeneration: New Perspectives from the Gut(-)Retina Axis. Nutrients 2018, 10, 1677. [Google Scholar] [CrossRef] [Green Version]
- Battistini, C.; Ballan, R.; Herkenhoff, M.E.; Saad, S.M.I.; Sun, J. Vitamin D Modulates Intestinal Microbiota in Inflammatory Bowel Diseases. Int. J. Mol. Sci. 2020, 22, 362. [Google Scholar] [CrossRef]
- Zuniga, S.; Firrincieli, D.; Housset, C.; Chignard, N. Vitamin D and the vitamin D receptor in liver pathophysiology. Clin. Res. Hepatol. Gastroenterol. 2011, 35, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.P.; Kong, M.; Zheng, S.; Ren, Y.; Zhu, L.; Shi, H.; Duan, Z. Vitamin D in liver diseases: From mechanisms to clinical trials. J. Gastroenterol. Hepatol. 2013, 28 (Suppl. 1), 49–55. [Google Scholar] [CrossRef]
- Roh, M.I.; Kim, J.H.; Byeon, S.H.; Koh, H.J.; Lee, S.C.; Kwon, O.W. Estimated prevalence and risk factor for age-related maculopathy. Yonsei Med. J. 2008, 49, 931–941. [Google Scholar] [CrossRef]
- Cho, B.J.; Heo, J.W.; Shin, J.P.; Ahn, J.; Kim, T.W.; Chung, H. Epidemiological association between systemic diseases and age-related macular degeneration: The Korea National Health and Nutrition Examination Survey 2008-2011. Investig. Opthalmology Vis. Sci. 2014, 55, 4430–4437. [Google Scholar] [CrossRef] [Green Version]
- Yates, J.R.; Sepp, T.; Matharu, B.K.; Khan, J.C.; Thurlby, D.A.; Shahid, H.; Clayton, D.G.; Hayward, C.; Morgan, J.; Wright, A.F.; et al. Complement C3 variant and the risk of age-related macular degeneration. N. Engl. J. Med. 2007, 357, 553–561. [Google Scholar] [CrossRef] [Green Version]
- Haroun, M.K.; Jaar, B.G.; Hoffman, S.C.; Comstock, G.W.; Klag, M.J.; Coresh, J. Risk factors for chronic kidney disease: A prospective study of 23,534 men and women in Washington County, Maryland. J. Am. Soc. Nephrol. 2003, 14, 2934–2941. [Google Scholar] [CrossRef] [Green Version]
- Xing, C.; Sivakumaran, T.A.; Wang, J.J.; Rochtchina, E.; Joshi, T.; Smith, W.; Mitchell, P.; Iyengar, S.K. Complement factor H polymorphisms, renal phenotypes and age-related macular degeneration: The Blue Mountains Eye Study. Genes Immun. 2008, 9, 231–239. [Google Scholar] [CrossRef] [Green Version]
- Dave, A.D.; Hess, K.; Chen, K.G.; Wiley, H.; Keenan, T.D.L.; Agron, E.; Chew, E.Y.; Cukras, C.A. Investigations of Renal Function and Age-Related Macular Degeneration Phenotypes. Transl. Vis. Sci. Technol. 2022, 11, 11. [Google Scholar] [CrossRef] [PubMed]
- Liew, G.; Mitchell, P.; Wong, T.Y.; Iyengar, S.K.; Wang, J.J. CKD increases the risk of age-related macular degeneration. J. Am. Soc. Nephrol. 2008, 19, 806–811. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.J.; Yeung, L.; Sun, C.C.; Huang, C.C.; Chen, K.S.; Lu, Y.H. Age-Related Macular Degeneration in Chronic Kidney Disease: A Meta-Analysis of Observational Studies. Am. J. Nephrol. 2018, 48, 278–291. [Google Scholar] [CrossRef] [PubMed]
- Weiner, D.E.; Tighiouart, H.; Reynolds, R.; Seddon, J.M. Kidney function, albuminuria and age-related macular degeneration in NHANES III. Nephrol. Dial. Transplant. 2011, 26, 3159–3165. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | Participants without AMD | Participants with Any AMD | All Participants | p-Value |
|---|---|---|---|---|
| Sample size, n (%) | 4636 (92.0) | 405 (8.0) | 5041 | N.A. |
| Study cycle, n (%) | 0.960 | |||
| 2005–2006 | 2158 (46.6) | 188 (46.4) | 2346 (46.5) | |
| 2007–2008 | 2478 (53.4) | 217 (53.6) | 2695 (53.5) | |
| Age, years, mean (SD) | 58.6 (12.1) | 70.4 (11.4) | 59.6 (12.5) | <0.001 |
| Sex (female), n (%) | 2310 (49.8) | 194 (47.9) | 2504 (49.7) | 0.457 |
| Race/ethnicity, n (%) | <0.001 | |||
| Mexican American | 738 (15.9) | 48 (11.9) | 784 (15.6) | |
| Other Hispanic | 324 (7.0) | 21 (5.2) | 345 (6.8) | |
| Non-Hispanic White | 2497 (53.9) | 294 (72.6) | 2791 (55.4) | |
| Non-Hispanic Black | 933 (20.1) | 33 (8.2) | 966 (19.2) | |
| Other | 144 (3.1) | 9 (2.2) | 153 (3.0) | |
| Serum 25(OH)D, nmol/L, mean (SD) | 59.8 (22.4) | 64.1 (22.3) | 60.1 (22.4) | <0.001 |
| 25(OH)D status, n (%) | 0.015 | |||
| <30 (deficiency) | 365 (7.9) | 22 (5.4) | 387 (7.6) | |
| 30–50 (insufficiency) | 1295 (27.9) | 95 (23.5) | 1390 (27.6) | |
| ≥50 (sufficiency) | 2976 (64.2) | 288 (71.1) | 3264 (64.8) | |
| Education, n (%) | 0.297 | |||
| Less than 9th grade | 657 (14.2) | 63 (15.6) | 720 (14.3) | |
| 9–11th grade | 689 (14.9) | 55 (13.6) | 744 (14.8) | |
| High school grad/GED or equivalent | 1134 (24.5) | 113 (27.9) | 1247 (24.7) | |
| Some college or AA degree | 1180 (25.5) | 106 (26.2) | 1286 (25.5) | |
| College graduate or above | 975 (21.0) | 68 (16.8) | 1043 (20.7) | |
| Unknown | 1 (0.02) | 0 | 1 (0.02) | |
| Poverty–income ratio, n (%) | <0.001 | |||
| <130% | 1073 (23.1) | 95 (23.5) | 1168 (23.2) | |
| 130–349% | 1625 (35.1) | 183 (45.2) | 1808 (35.9) | |
| ≥350% | 1655 (35.7) | 90 (22.2) | 1745 (34.6) | |
| Unknown | 283 (6.1) | 37 (9.1) | 320 (6.4) | |
| Obesity, n (%) | 0.059 | |||
| Underweight | 63 (1.4) | 4 (1.0) | 67 (1.3) | |
| Normal | 1102 (23.8) | 112 (27.7) | 1214 (24.1) | |
| Overweight | 1651 (35.6) | 159 (39.3) | 1810 (35.9) | |
| Obese | 1784 (38.5) | 127 (31.4) | 1911 (37.9) | |
| Unknown | 36 (0.8) | 3 (0.7) | 39 (0.8) | |
| Smoking status, n (%) | 0.002 | |||
| Non-smoker | 2211 (47.7) | 177 (43.7) | 2388 (47.4) | |
| Past smoker | 1480 (31.9) | 165 (40.7) | 1645 (32.6) | |
| Current smoker | 943 (20.3) | 63 (15.6) | 1006 (20.0) | |
| Unknown | 2 (0.04) | 0 | 2 (0.04) | |
| Alcohol consumption, n (%) | 0.027 | |||
| Never drinker | 612 (13.2) | 75 (18.5) | 687 (13.6) | |
| Former drinker | 498 (10.7) | 38 (9.4) | 536 (10.6) | |
| Current drinker | 3431 (74.0) | 284 (70.1) | 3715 (73.7) | |
| Unknown | 95 (2.1) | 8 (2.0) | 103 (2.0) | |
| General health condition, n (%) | 0.795 | |||
| Excellent, very good, or good | 3410 (73.6) | 292 (72.1) | 3702 (73.4) | |
| Fair, or poor | 1146 (24.7) | 105 (25.9) | 1251 (24.8) | |
| Unknown | 80 (1.7) | 8 (2.0) | 88 (1.8) | |
| History of systemic diseases, n (%) | ||||
| Cardiovascular disease | 649 (14.0) | 121 (29.9) | 770 (15.3) | <0.001 |
| Diabetes | 952 (20.5) | 81 (20.0) | 1033 (20.5) | 0.798 |
| Hypertension | 3055 (65.9) | 309 (76.3) | 3364 (66.7) | <0.001 |
| Hypercholesterolemia | 1910 (41.2) | 174 (43.0) | 2084 (41.3) | 0.725 |
| History of ocular condition, n (%) | ||||
| Cataract operation | 502 (10.8) | 131 (32.4) | 633 (12.6) | <0.001 |
| Glaucoma | 256 (5.5) | 42 (10.4) | 298 (5.9) | <0.001 |
| Serum 25(OH)D (nmol/L) | Any AMD | Early AMD | Late AMD | |||
|---|---|---|---|---|---|---|
| No. At-Risk | No. with Event (%) | No. At-Risk | No. with Event (%) | No. At-Risk | No. with Event (%) | |
| Overall | ||||||
| <30 (deficiency) | 387 | 22 (5.68) | 381 | 16 (4.20) | 371 | 6 (1.62) |
| 30–50 (insufficiency) | 1390 | 95 (6.83) | 1377 | 82 (5.95) | 1308 | 13 (0.99) |
| ≥50 (sufficiency) | 3264 | 288 (8.82) | 3232 | 256 (7.92) | 3008 | 32 (1.06) |
| <60 years | ||||||
| <30 (deficiency) | 217 | 3 (1.38) | 217 | 3 (1.38) | 214 | 0 (0) |
| 30–50 (insufficiency) | 753 | 23 (3.05) | 753 | 23 (3.05) | 730 | 0 (0) |
| ≥50 (sufficiency) | 1547 | 45 (2.91) | 1546 | 44 (2.85) | 1503 | 1 (0.07) |
| ≥60 years | ||||||
| <30 (deficiency) | 170 | 19 (11.2) | 164 | 13 (7.93) | 157 | 6 (3.82) |
| 30–50 (insufficiency) | 637 | 72 (11.3) | 624 | 59 (9.46) | 578 | 13 (2.25) |
| ≥50 (sufficiency) | 1717 | 243 (14.2) | 1686 | 212 (11.5) | 1505 | 31 (2.06) |
| Serum 25(OH)D Level (nmol/L) | Any AMD | Early AMD | Late AMD | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Crude | Model 1 | Model 2 | Crude | Model 1 | Model 2 | Crude | Model 1 | Model 2 | |
| <30 (deficiency) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) |
| 30–50 (insufficiency) | 1.22 (0.75–1.96) | 1.08 (0.64–1.85) | 1.07 (0.63–1.85) | 1.44 (0.83–2.50) | 1.34 (0.74–2.45) | 1.33 (0.73–2.43) | 0.61 (0.23–1.62) | 0.33 (0.10–1.09) | 0.27 (0.08–0.96) |
| ≥50 (sufficiency) | 1.61 (1.03–2.51) | 1.21 (0.73–2.02) | 1.17 (0.70–1.97) | 1.96 (1.17–3.29) | 1.54 (0.87–2.75) | 1.50 (0.84–2.68) | 0.65 (0.27–1.57) | 0.34 (0.12–1.01) | 0.28 (0.09–0.87) |
| Serum 25(OH)D (nmol/L) | Any AMD | Early AMD | Late AMD | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Crude | Model 1 | Model 2 | Crude | Model 1 | Model 2 | Crude | Model 1 | Model 2 | |
| <60 years | |||||||||
| <30 (deficiency) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) |
| 30–50 (insufficiency) | 2.25 (0.67–7.56) | 1.75 (0.50–6.07) | 1.86 (0.53–6.50) | 2.25 (0.67–7.56) | 1.71 (0.49–5.95) | 1.80 (0.51–6.32) | N.A. | N.A. | N.A. |
| ≥50 (sufficiency) | 2.14 (0.66–6.94) | 1.96 (0.57–6.67) | 1.82 (0.53–6.27) | 2.09 (0.64–6.79) | 1.82 (0.53–6.23) | 1.67 (0.49–5.76) | N.A. | N.A. | N.A. |
| ≥60 years | |||||||||
| <30 (deficiency) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) |
| 30–50 (insufficiency) | 1.01 (0.59–1.73) | 0.95 (0.52–1.74) | 0.93 (0.50–1.70) | 1.21 (0.65–2.27) | 1.23 (0.61–2.45) | 1.19 (0.60–2.39) | 0.58 (0.22–1.55) | 0.32 (0.09–1.08) | 0.26 (0.07–0.93) |
| ≥50 (sufficiency) | 1.31 (0.80–2.15) | 1.08 (0.61–1.91) | 1.04 (0.59–1.86) | 1.67 (0.93–3.00) | 1.46 (0.75–2.81) | 1.42 (0.73–2.77) | 0.53 (0.22–1.29) | 0.30 (0.10–0.91) | 0.24 (0.08–0.75) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, Y.; Chen, X.; Luo, S.; Jiang, S.; Mao, Y.; Xiao, W. Serum 25-Hydroxyvitamin D Is Differentially Associated with Early and Late Age-Related Macular Degeneration in the United States Population. Nutrients 2023, 15, 1216. https://doi.org/10.3390/nu15051216
Fu Y, Chen X, Luo S, Jiang S, Mao Y, Xiao W. Serum 25-Hydroxyvitamin D Is Differentially Associated with Early and Late Age-Related Macular Degeneration in the United States Population. Nutrients. 2023; 15(5):1216. https://doi.org/10.3390/nu15051216
Chicago/Turabian StyleFu, Yihang, Xiaoyun Chen, Sheng Luo, Shuangyan Jiang, Yuxiang Mao, and Wei Xiao. 2023. "Serum 25-Hydroxyvitamin D Is Differentially Associated with Early and Late Age-Related Macular Degeneration in the United States Population" Nutrients 15, no. 5: 1216. https://doi.org/10.3390/nu15051216