
Metabolic Profile of Patients with Long COVID: A Cross-Sectional Study
 ,
,  and
and 
Abstract
:1. Introduction
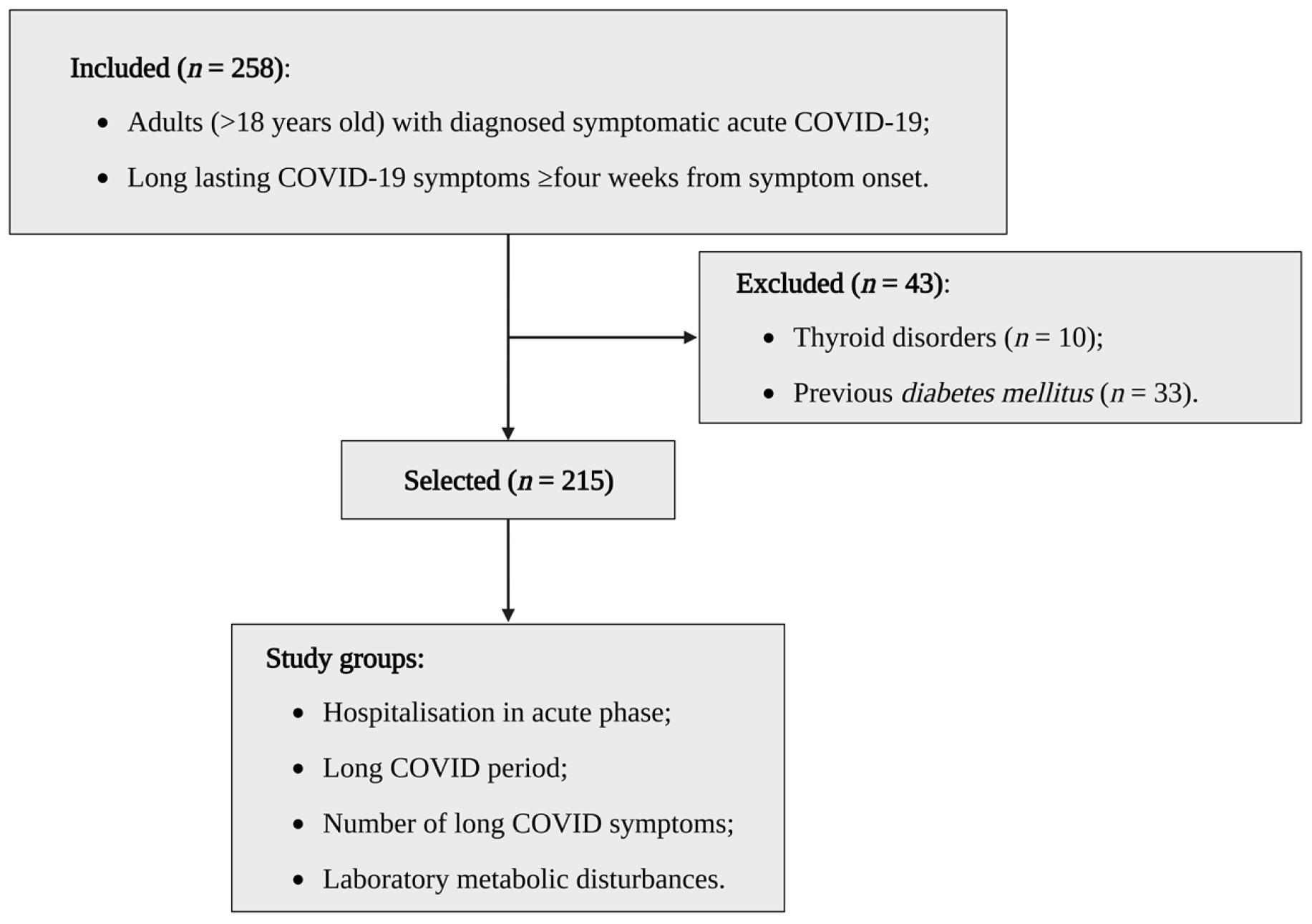
2. Materials and Methods
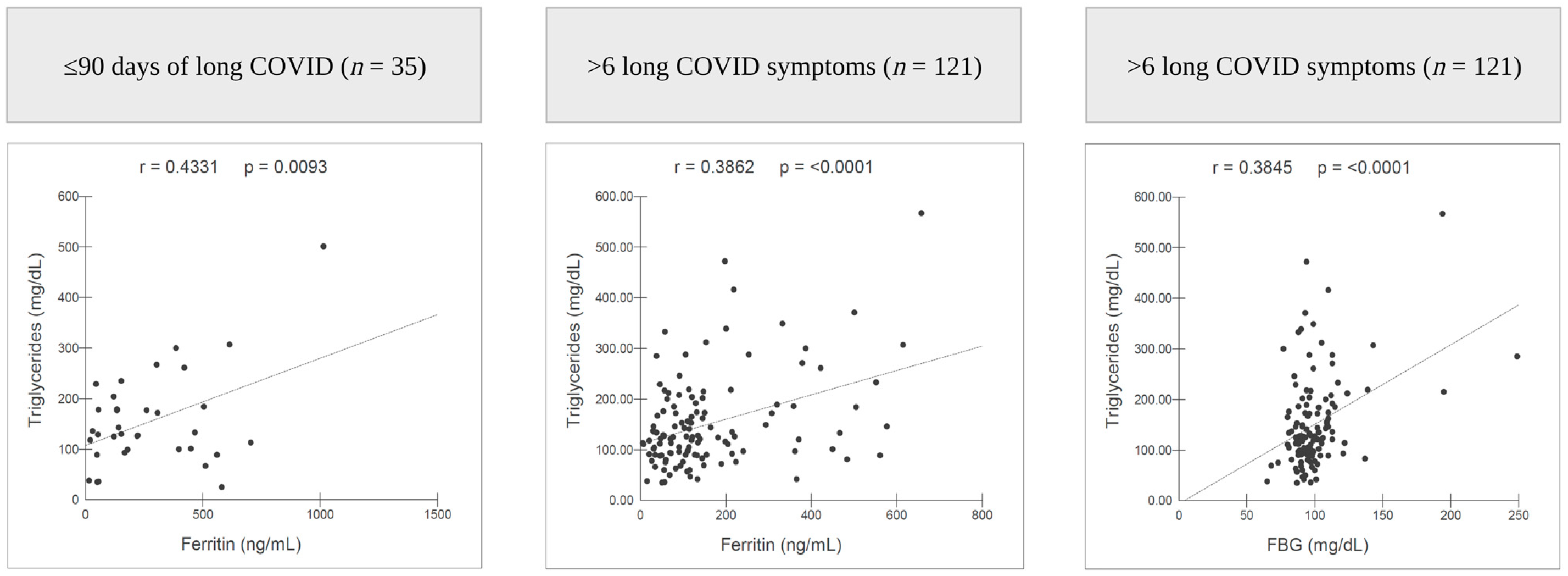
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Delli Muti, N.; Finocchi, F.; Tossetta, G.; Salvio, G.; Cutini, M.; Marzioni, D.; Balercia, G. Could SARS-CoV-2 infection affect male fertility and sexuality? APMIS 2022, 130, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Liptak, P.; Nosakova, L.; Rosolanka, R.; Skladany, L.; Banovcin, P. Acute-on-chronic liver failure in patients with severe acute respiratory syndrome coronavirus 2 infection. World J. Hepatol. 2023, 15, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Khreefa, Z.; Barbier, M.T.; Koksal, A.R.; Love, G.; Del Valle, L. Pathogenesis and Mechanisms of SARS-CoV-2 Infection in the Intestine, Liver, and Pancreas. Cells 2023, 12, 262. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Yaksi, N.; Teker, A.G.; Imre, A. Long COVID in Hospitalized COVID-19 Patients: A Retrospective Cohort Study. Iran. J. Public Health 2022, 51, 88–95. [Google Scholar] [CrossRef]
- Petersen, M.S.; Kristiansen, M.F.; Hanusson, K.D.; Danielsen, M.E.; Steig, B.; Gaini, S.; Strøm, M.; Weihe, P. Long COVID in the Faroe Islands: A Longitudinal Study Among Nonhospitalized Patients. Clin. Infect. Dis. 2021, 73, e4058–e4063. [Google Scholar] [CrossRef]
- Al-Aly, Z.; Xie, Y.; Bowe, B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature 2021, 594, 259–264. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute covid-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef]
- Raveendran, A.V. Long COVID-19: Challenges in the diagnosis and proposed diagnostic criteria. Diabetes Metab. Syndr. 2021, 15, 145–146. [Google Scholar] [CrossRef]
- Bai, F.; Tomasoni, D.; Falcinella, C.; Barbanotti, D.; Castoldi, R.; Mulè, G.; Augello, M.; Mondatore, D.; Allegrini, M.; Cona, A.; et al. Female gender is associated with long COVID syndrome: A prospective cohort study. Clin. Microbiol. Infect. 2022, 28, 611.e9–611.e16. [Google Scholar] [CrossRef]
- Michelen, M.; Manoharan, L.; Elkheir, N.; Cheng, V.; Dagens, A.; Hastie, C.; O’Hara, M.; Suett, J.; Dahmash, D.; Bugaeva, P.; et al. Characterising long COVID: A living systematic review. BMJ Glob. Health 2021, 6, e005427. [Google Scholar] [CrossRef] [PubMed]
- Frere, J.J.; tenOever, B.R. Cardiometabolic syndrome-an emergent feature of Long COVID? Nat. Rev. Immunol. 2022, 22, 399–400. [Google Scholar] [CrossRef] [PubMed]
- Pasini, E.; Corsetti, G.; Romano, C.; Scarabelli, T.M.; Chen-Scarabelli, C.; Saravolatz, L.; Dioguardi, F.S. Serum Metabolic Profile in Patients with Long-Covid (PASC) Syndrome: Clinical Implications. Front. Med. 2021, 8, 714426. [Google Scholar] [CrossRef] [PubMed]
- Stavem, K.; Ghanima, W.; Olsen, M.K.; Gilboe, H.M.; Einvik, G. Persistent symptoms 1.5–6 months after COVID-19 in non-hospitalised subjects: A population-based cohort study. Thorax 2021, 76, 405–407. [Google Scholar] [CrossRef]
- Einvik, G.; Dammen, T.; Ghanima, W.; Heir, T.; Stavem, K. Prevalence and Risk Factors for Post-Traumatic Stress in Hospitalized and Non-Hospitalized COVID-19 Patients. Int. J. Environ. Res. Public Health 2021, 18, 2079. [Google Scholar] [CrossRef]
- Logue, J.K.; Franko, N.M.; McCulloch, D.J.; McDonald, D.; Magedson, A.; Wolf, C.R.; Chu, H.Y. Sequelae in Adults at 6 Months After COVID-19 Infection. JAMA Netw. Open 2021, 4, e210830. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef]
- Carvalho-Schneider, C.; Laurent, E.; Lemaignen, A.; Beaufils, E.; Bourbao-Tournois, C.; Laribi, S.; Flament, T.; Ferreira-Maldent, N.; Bruyère, F.; Stefic, K.; et al. Follow-up of adults with noncritical COVID-19 two months after symptom onset. Clin. Microbiol. Infect. 2021, 27, 258–263. [Google Scholar] [CrossRef]
- Prieto, M.A.; Prieto, O.; Castro, H.M. Covid prolongado: Estudio de corte transversal [Long covid: Cross sectional study]. Rev. Fac. Cien. Med. Univ. Nac. Cordoba. 2021, 78, 33–36. [Google Scholar] [CrossRef]
- Zhao, Y.-M.; Shang, Y.-M.; Song, W.-B.; Li, Q.-Q.; Xie, H.; Xu, Q.-F.; Jia, J.-L.; Li, L.-M.; Mao, H.-L.; Zhou, X.-M.; et al. Follow-up study of the pulmonary function and related physiological characteristics of COVID-19 survivors three months after recovery. EClinicalMedicine 2020, 25, 100463. [Google Scholar] [CrossRef]
- Aung, N.; Khanji, M.Y.; Munroe, P.B.; Petersen, S.E. Causal Inference for Genetic Obesity, Cardiometabolic Profile and COVID-19 Susceptibility: A Mendelian Randomization Study. Front. Genet. 2020, 11, 586308. [Google Scholar] [CrossRef] [PubMed]
- Vimercati, L.; De Maria, L.; Quarato, M.; Caputi, A.; Gesualdo, L.; Migliore, G.; Cavone, D.; Sponselli, S.; Pipoli, A.; Inchingolo, F.; et al. Association between Long COVID and Overweight/Obesity. J. Clin. Med. 2021, 10, 4143. [Google Scholar] [CrossRef] [PubMed]
- Reiterer, M.; Rajan, M.; Gómez-Banoy, N.; Lau, J.D.; Gomez-Escobar, L.G.; Ma, L.; Gilani, A.; Alvarez-Mulett, S.; Sholle, E.T.; Chandar, V.; et al. Hyperglycemia in acute COVID-19 is characterized by insulin resistance and adipose tissue infectivity by SARS-CoV-2. Cell. Metab. 2021, 33, 2174–2188.e5. [Google Scholar] [CrossRef] [PubMed]
- Sonnweber, T.; Boehm, A.; Sahanic, S.; Pizzini, A.; Aichner, M.; Sonnweber, B.; Kurz, K.; Koppelstätter, S.; Haschka, D.; Petzer, V.; et al. Persisting alterations of iron homeostasis in COVID-19 are associated with non-resolving lung pathologies and poor patients’ performance: A prospective observational cohort study. Respir. Res. 2020, 21, 276. [Google Scholar] [CrossRef] [PubMed]
- Dahan, S.; Segal, G.; Katz, I.; Hellou, T.; Tietel, M.; Bryk, G.; Amital, H.; Shoenfeld, Y.; Dagan, A. Ferritin as a Marker of Severity in COVID-19 Patients: A Fatal Correlation. Isr. Med. Assoc. J. 2020, 22, 494–500. [Google Scholar]
- Para, O.; Caruso, L.; Pestelli, G.; Tangianu, F.; Carrara, D.; Maddaluni, L.; Tamburello, A.; Castelnovo, L.; Fedi, G.; Guidi, S.; et al. Ferritin as prognostic marker in COVID-19: The FerVid study. Postgrad. Med. 2022, 134, 58–63. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | n = 215 | Laboratory Metabolic Disturbances † | p * | |
|---|---|---|---|---|
| Yes | No | |||
| Female, n (%) | 138 (64.1) | 61 (59.8) | 77 (68.1) | 0.2581 |
| Age, mean ± SD, years | 49.6 ± 12.7 | 51.5 ± 11.6 | 47.9 ± 13.4 | 0.0351 |
| 18–59 years old, n (%) | 161 (74.8) | 72 (70.5) | 89 (78.7) | 0.2216 |
| ≥60 years old, n (%) | 54 (25.1) | 30 (29.4) | 24 (21.2) | |
| Weight, mean ± SD, kg | 77.7 ± 16.5 | 78.3 ± 16 | 77.1 ± 16.9 | 0.6089 |
| Height, mean ± SD, m | 1.61 ± 0.09 | 1.62 ± 0.10 | 1.6 ± 0.08 | 0.5450 |
| BMI, mean ± SD, kg/m2 | 29.7 ± 5.8 | 29.9 ± 5.7 | 29.6 ± 6 | 0.5952 |
| SBP, mean ± SD, mm/Hg | 125.3 ± 14.1 | 127.3 ± 14.2 | 123.6 ± 13.8 | 0.1480 |
| DBP, mean ± SD, mm/Hg | 83.9 ± 9.6 | 84.3 ± 9.8 | 83.6 ± 9.5 | 0.6107 |
| Current/Former smoker, n (%) | 63 (29.3) | 28 (27.4) | 35 (30.9) | 0.6770 |
| Reported comorbidities, n (%) | 77 (35.8) | 42 (41.1) | 35 (30.9) | 0.1569 |
| Hypertension, n (%) | 64 (29.7) | 36 (35.2) | 28 (24.7) | 0.1249 |
| Other (a), n (%) | 26 (12) | 14 (13.7) | 12 (10.6) | 0.6255 |
| Hospitalised in acute phase, n (%) | 78 (36.2) | 43 (42.1) | 35 (30.9) | 0.1185 |
| Hospitalisation period (b), mean ± SD, days | 19.6 ± 17.1 | 21.5 ± 19.8 | 17.4 ± 13.1 | 0.4101 |
| Hospitalised >7 days (b), n (%) | 64 (82) | 37 (86) | 27 (77.1) | 0.4700 |
| Fatigue (c), n (%) | 184 (85.5) | 85 (83.3) | 99 (87.6) | 0.4857 |
| Dyspnoea (c), n (%) | 178 (82.7) | 80 (78.4) | 98 (86.7) | 0.1533 |
| Muscle weakness (c), n (%) | 168 (78.1) | 88 (86.2) | 80 (70.7) | 0.0100 |
| Muscle pain (c), n (%) | 144 (66.9) | 62 (60.7) | 82 (72.5) | 0.0912 |
| Loss of balance (c), n (%) | 127 (59) | 67 (65.6) | 60 (53) | 0.0826 |
| Chest pain (c), n (%) | 116 (53.9) | 52 (50.9) | 64 (56.6) | 0.4877 |
| Headache (c), n (%) | 116 (53.9) | 51 (50) | 65 (57.5) | 0.3331 |
| Insomnia (c), n (%) | 111 (51.6) | 54 (52.9) | 57 (50.4) | 0.8185 |
| Visual disturbances (c), n (%) | 109 (50.6) | 53 (51.9) | 56 (49.5) | 0.8295 |
| Cough (c), n (%) | 97 (45.1) | 42 (41.1) | 55 (48.6) | 0.3342 |
| Tremor (c), n (%) | 85 (39.5) | 45 (44.1) | 40 (35.3) | 0.2436 |
| Lower limb oedema (c), n (%) | 78 (36.2) | 40 (39.2) | 38 (33.6) | 0.4784 |
| Number of long COVID symptoms, mean ± SD | 7 ± 2.7 | 6.9 ± 2.7 | 7 ± 2.6 | 0.9190 |
| ≤6 symptoms, n (%) | 94 (43.7) | 45 (44.1) | 49 (43.3) | 0.9791 |
| >6 symptoms, n (%) | 121 (56.2) | 57 (55.8) | 64 (56.6) | |
| Long COVID period, mean ± SD, days | 247.7 ± 151.2 | 241.9 ± 149.5 | 253 ± 153.2 | 0.6774 |
| ≤90 days, n (%) | 35 (16.2) | 19 (18.6) | 16 (14.1) | 0.4832 |
| ≤180 days, n (%) | 74 (34.4) | 38 (37.2) | 36 (31.8) | 0.4915 |
| >365 days, n (%) | 45 (20.9) | 21 (20.5) | 24 (21.2) | 0.9595 |
| LDL-C, mean ± SD, mg/dL | 128.7 ± 40 | - | - | - |
| HDL-C, mean ± SD, mg/dL | 45.7 ± 9.9 | 44.8 ± 10.4 | 46.4 ± 9.5 | 0.1633 |
| Total cholesterol, mean ± SD, mg/dL | 204.3 ± 44.6 | - | - | - |
| Triglycerides, mean ± SD, mg/dL | 154.1 ± 101.3 | - | - | - |
| FBG, mean ± SD, mg/dL | 99.5 ± 21.1 | - | - | - |
| HbA1c (d), mean ± SD, % | 5.9 ± 0.8 | - | - | - |
| Ferritin, mean ± SD, ng/mL | 176.5 ± 159 | 219.2 ± 189.2 | 138 ± 113.3 | 0.0005 |
| ESR, mean ± SD, mm | 39.5 ± 25.5 | 42.3 ± 26.2 | 36.9 ± 24.7 | 0.0987 |
| CRP positive, n (%) | 27 (12.5) | 16 (15.6) | 11 (9.7) | 0.2674 |
| Total, n (%) | 215 (100) | 102 (47.4) | 113 (52.5) | - |
| Variable | Hospitalised in Acute Phase | Long COVID Period | Number of Long COVID Symptoms | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes | No | p * | ≤90 Days | >90 Days | p * | ≤180 Days | >180 Days | p * | ≤365 Days | >365 Days | p * | ≤6 | >6 | p * | |
| BMI, mean ± SD, kg/m2 | 30.4 ± 5.3 | 29.3 ± 6.1 | 0.0586 | 28.7 ± 6 | 29.9 ± 5.8 | 0.2529 | 29.2 ± 5.8 | 30 ± 5.9 | 0.3977 | 29.3 ± 5.7 | 31.5 ± 6 | 0.0222 | 28.5 ± 5.8 | 30.7 ± 5.7 | 0.0019 |
| ≥30 kg/m2, n (%) | 39 (50) | 50 (36.4) | 0.0736 | 15 (42.8) | 74 (41.1) | 0.9965 | 32 (43.2) | 57 (40.4) | 0.8004 | 64 (37.6) | 25 (55.5) | 0.0456 | 24 (25.5) | 65 (53.7) | <0.0001 |
| SBP, mean ± SD, mmHg | 127.3 ± 16 | 124.3 ± 12.8 | 0.2322 | 127.1 ± 13.1 | 125 ± 14.3 | 0.3851 | 127.2 ± 13.8 | 124.3 ± 14.2 | 0.1322 | 124.9 ± 13.6 | 127.1 ± 15.9 | 0.6115 | 126.7 ± 14.6 | 124.3 ± 13.7 | 0.5017 |
| ≥130 mmHg, n (%) | 38 (48.7) | 64 (46.7) | 0.8881 | 17 (48.5) | 85 (47.2) | 0.9691 | 41 (55.4) | 61 (43.2) | 0.1211 | 79 (46.4) | 23 (51.1) | 0.6991 | 45 (47.8) | 57 (47.1) | 0.9791 |
| DBP, mean ± SD, mmHg | 83 ± 9.1 | 84.4 ± 9.9 | 0.3173 | 84.5 ± 7.8 | 83.8 ± 9.9 | 0.6832 | 84.5 ± 8.3 | 83.6 ± 10.3 | 0.3926 | 83.8 ± 9.4 | 84.2 ± 10.3 | 0.8287 | 83.7 ± 9.2 | 84.1 ± 9.9 | 0.7570 |
| ≥85 mmHg, n (%) | 28 (35.8) | 52 (37.9) | 0.8780 | 16 (45.7) | 64 (35.5) | 0.3439 | 29 (39.1) | 51 (36.1) | 0.7744 | 62 (36.4) | 18 (40) | 0.7932 | 35 (37.2) | 45 (37.1) | 0.8921 |
| LDL-C, mean ± SD, mg/dL | 126.1 ± 37.7 | 130.2 ± 41.3 | 0.8312 | 141 ± 45.6 | 126.3 ± 38.5 | 0.0834 | 133.6 ± 40.1 | 126.1 ± 39.8 | 0.2205 | 131.3 ± 39.5 | 118.7 ± 40.6 | 0.0481 | 129.6 ± 38.6 | 128 ± 41.1 | 0.5626 |
| ≥130 mg/dL, n (%) | 37 (47.4) | 64 (46.7) | 0.9678 | 21 (60) | 80 (44.4) | 0.1331 | 39 (52.7) | 62 (43.9) | 0.2824 | 65 (38.2) | 16 (35.5) | 0.8753 | 49 (52.1) | 52 (42.9) | 0.2317 |
| HDL-C, mean ± SD, mg/dL | 44.2 ± 10.9 | 46.5 ± 9.2 | 0.0969 | 45 ± 12.3 | 45.8 ± 9.4 | 0.5368 | 45.5 ± 11 | 45.7 ± 9.3 | 0.7898 | 46 ± 9.9 | 44.4 ± 9.9 | 0.2883 | 44.7 ± 9.2 | 46.4 ± 10.4 | 0.3985 |
| <40 mg/dL, n (%) | 28 (35.8) | 31 (22.6) | 0.0527 | 14 (40) | 45 (25) | 0.1068 | 24 (32.4) | 35 (24.8) | 0.3043 | 47 (27.6) | 12 (26.6) | 0.4572 | 27 (28.7) | 32 (26.4) | 0.8281 |
| Total cholesterol, mean ± SD, mg/dL | 207.7 ± 45.2 | 202.4 ± 44.3 | 0.3135 | 217.1 ± 49.8 | 201.9 ± 43.3 | 0.0619 | 210.3 ± 45.6 | 201.2 ± 44 | 0.1939 | 206.9 ± 44.9 | 194.7 ± 42.6 | 0.0964 | 203.9 ± 42.9 | 204.7 ± 46.1 | 0.9533 |
| ≥200 mg/dL, n (%) | 42 (53.8) | 62 (45.2) | 0.2846 | 20 (57.1) | 84 (46.6) | 0.3421 | 39 (52.7) | 65 (46) | 0.4372 | 86 (50.5) | 18 (40) | 0.2730 | 49 (52.1) | 55 (45.4) | 0.4045 |
| Triglycerides, mean ± SD, mg/dL | 197.7 ± 130.3 | 129.3 ± 69.5 | <0.0001 | 154.9 ± 94.1 | 153.9 ± 102.9 | 0.5899 | 166.9 ± 125 | 147.3 ± 86.1 | 0.3435 | 153.1 ± 105.4 | 157.8 ± 85 | 0.5230 | 158 ± 113.5 | 151 ± 91.1 | 0.9515 |
| ≥150 mg/dL, n (%) | 41 (52.5) | 42 (30.6) | 0.0025 | 14 (40) | 69 (38.3) | 0.9965 | 30 (40.5) | 53 (37.5) | 0.7833 | 63 (37) | 20 (44.4) | 0.4637 | 40 (42.5) | 43 (35.5) | 0.3644 |
| FGB, mean ± SD, mg/dL | 103.3 ± 27.5 | 97.3 ± 16.1 | 0.1502 | 96.2 ± 13.2 | 100.1 ± 22.3 | 0.7597 | 100 ± 20.8 | 99.2 ± 21.4 | 0.3669 | 99.2 ± 20 | 100.5 ± 25.2 | 0.6742 | 98.8 ± 19.7 | 100 ± 22.2 | 0.6705 |
| ≥100 mg/dL, n (%) | 29 (37.1) | 44 (32.1) | 0.5459 | 12 (34.2) | 61 (33.8) | 0.8810 | 28 (37.8) | 45 (31.9) | 0.4717 | 60 (35.2) | 13 (28.8) | 0.5288 | 31 (32.9) | 42 (34.7) | 0.9038 |
| HbA1c, mean ± SD, % (a) | 6 ± 0.7 | 5.8 ± 0.7 | 0.1528 | 6.3 ± 0.8 | 5.8 ± 0.7 | 0.0080 | 6 ± 0.9 | 5.9 ± 0.7 | 0.3892 | 6 ± 0.8 | 5.7 ± 0.7 | 0.0990 | 5.7 ± 0.6 | 6 ± 0.8 | 0.0421 |
| ≥6%, n (%) | 31 (49.2) | 32 (36.7) | 0.1757 | 19 (76) | 44 (35.2) | 0.0004 | 27 (54) | 36 (36) | 0.0536 | 52 (48.5) | 11 (25.5) | 0.0164 | 25 (38.4) | 38 (44.7) | 0.5479 |
| Ferritin, mean ± SD, ng/mL | 235.3 ± 195.3 | 143.1 ± 122.8 | 0.0002 | 275 ± 236.4 | 157.4 ± 131.7 | 0.0082 | 220.2 ± 205.3 | 153.6 ± 122.9 | 0.1145 | 179 ± 163 | 167.1 ± 142.7 | 0.9979 | 196 ± 172.7 | 161.4 ± 146.4 | 0.0370 |
| High ferritin (b) | 24 (30.7) | 19 (13.8) | 0.0051 | 14 (40) | 29 (16.1) | 0.0027 | 21 (28.3) | 22 (15.6) | 0.0408 | 36 (21.1) | 7 (15.5) | 0.5296 | 19 (20.2) | 24 (19.8) | 0.9179 |
| ESR, mean ± SD, mm | 36.9 ± 22.6 | 40.9 ± 26.9 | 0.4429 | 28.7 ± 6 | 38.6 ± 25.2 | 0.2699 | 42 ± 26.9 | 38.2 ± 24.7 | 0.3787 | 39.2 ± 24.7 | 40.5 ± 28.4 | 0.9688 | 39.8 ± 28.6 | 39.2 ± 22.9 | 0.5390 |
| High ESR (c) | 58 (74.3) | 95 (69.3) | 0.5326 | 27 (77.1) | 126 (70) | 0.5159 | 55 (74.3) | 98 (69.5) | 0.5600 | 119 (70) | 34 (75.5) | 0.5847 | 65 (69.1) | 88 (72.7) | 0.6725 |
| CRP, positive, n (%) | 11 (14.1) | 16 (11.6) | 0.7629 | 6 (17.1) | 21 (11.6) | 0.3710 | 11 (14.8) | 16 (11.3) | 0.6011 | 21 (12.3) | 6 (13.3) | 0.9390 | 10 (10.6) | 17 (14) | 0.5883 |
| Total, n (%) | 78 (36.2) | 137 (63.7) | - | 35 (16.2) | 180 (83.7) | - | 74 (34.4) | 141 (65.5) | - | 170 (79) | 45 (20.9) | - | 94 () | 121 () | - |
| Risk Variables (n = 150) | Long COVID Outcomes | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Long COVID Period >90 Days (n = 125) | Long COVID Period >365 Days (n = 43) | Number of Long COVID Symptoms >6 (n = 85) | Fatigue (n = 129) | |||||||||
| Coefficient | p-Value | Odds Ratio | Coefficient | p-Value | Odds Ratio | Coefficient | p-Value | Odds Ratio | Coefficient | p-Value | Odds Ratio | |
| Female gender | −0.4693 | 0.4882 | 0.6254 | −0.5481 | 0.2590 | 0.5781 | 1.0860 | 0.0178 | 2.9624 | 0.5822 | 0.3845 | 1.7900 |
| Age ≥ 60 years | −0.6034 | 0.3225 | 0.5469 | 0.2220 | 0.6323 | 1.2486 | −0.7495 | 0.0878 | 0.4726 | −0.9507 | 0.1056 | 0.3865 |
| Hospitalisation in acute phase | −1.7704 | 0.0051 | 0.1703 | −1.3458 | 0.0035 | 0.2603 | 1.2121 | 0.0082 | 3.3605 | 1.2778 | 0.0805 | 3.5886 |
| Long COVID period, ≤90 days | - | - | - | - | - | - | −0.9821 | 0.1029 | 0.3745 | −2.2518 | 0.0053 | 0.1052 |
| LDL-C ≥ 130 mg/dL | −0.9950 | 0.2245 | 0.3697 | −0.3672 | 0.5795 | 0.6927 | −0.2434 | 0.6839 | 0.7839 | 0.0877 | 0.9170 | 1.0916 |
| HDL-C < 40 mg/dL | −1.2671 | 0.0622 | 0.2816 | −0.2747 | 0.5727 | 0.7598 | −0.2601 | 0.5861 | 0.7709 | −1.0827 | 0.1018 | 0.3387 |
| Total cholesterol ≥ 200 mg/dL | −0.2851 | 0.7323 | 0.7520 | −0.3937 | 0.5515 | 0.6745 | −0.5681 | 0.3459 | 0.5666 | −0.7048 | 0.4166 | 0.4942 |
| Triglycerides ≥ 150 mg/dL | 1.2534 | 0.0833 | 3.5023 | 0.6445 | 0.1554 | 1.9051 | −0.4701 | 0.2797 | 0.6249 | −1.4015 | 0.0361 | 0.2462 |
| FBG ≥ 100 mg/dL | 0.3211 | 0.6416 | 1.3786 | −0.1047 | 0.8430 | 0.9006 | −0.0473 | 0.9226 | 0.9538 | 1.4034 | 0.0710 | 4.0690 |
| HbA1c ≥ 6% | −1.9821 | 0.0031 | 0.1378 | −1.2536 | 0.0136 | 0.2855 | 0.5892 | 0.2080 | 1.8026 | 0.1412 | 0.8434 | 1.1517 |
| High ferritin (a) | −1.6889 | 0.0134 | 0.1847 | −0.1393 | 0.8077 | 0.8699 | 0.4309 | 0.4334 | 1.5386 | 0.9373 | 0.2279 | 2.5531 |
| High ESR (b) | 0.2591 | 0.6855 | 1.2958 | 0.4676 | 0.3248 | 1.5962 | 0.3295 | 0.4478 | 1.3902 | 0.2968 | 0.6313 | 1.3455 |
| BMI ≥ 30 kg/m2 | 0.3330 | 0.5840 | 1.3952 | 1.0535 | 0.0169 | 2.8677 | 1.1749 | 0.0040 | 3.2379 | 1.1376 | 0.0865 | 3.1192 |
| SBP > 130 mmHg | 0.5560 | 0.4241 | 1.7436 | −0.0754 | 0.8794 | 0.9273 | 0.3615 | 0.4404 | 1.4354 | 0.2697 | 0.6757 | 1.3096 |
| DBP > 85 mmHg | −0.8934 | 0.1832 | 0.4093 | 0.0351 | 0.9455 | 1.0357 | −0.1534 | 0.7488 | 0.8578 | −0.0337 | 0.9605 | 0.9668 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menezes, D.C.d.; Lima, P.D.L.d.; Lima, I.C.d.; Uesugi, J.H.E.; Vasconcelos, P.F.d.C.; Quaresma, J.A.S.; Falcão, L.F.M. Metabolic Profile of Patients with Long COVID: A Cross-Sectional Study. Nutrients 2023, 15, 1197. https://doi.org/10.3390/nu15051197
Menezes DCd, Lima PDLd, Lima ICd, Uesugi JHE, Vasconcelos PFdC, Quaresma JAS, Falcão LFM. Metabolic Profile of Patients with Long COVID: A Cross-Sectional Study. Nutrients. 2023; 15(5):1197. https://doi.org/10.3390/nu15051197
Chicago/Turabian StyleMenezes, Daniel Carvalho de, Patrícia Danielle Lima de Lima, Igor Costa de Lima, Juliana Hiromi Emin Uesugi, Pedro Fernando da Costa Vasconcelos, Juarez Antônio Simões Quaresma, and Luiz Fábio Magno Falcão. 2023. "Metabolic Profile of Patients with Long COVID: A Cross-Sectional Study" Nutrients 15, no. 5: 1197. https://doi.org/10.3390/nu15051197