
Identifying Factors Which Influence Eating Disorder Risk during Behavioral Weight Management: A Consensus Study
 ,
,  , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Survey Development and Data Collection
- Individual characteristics—Participants were asked to rate the relevance of individual participant characteristics to the risk of developing an eating disorder in the context of weight management interventions. Items were rated on a five-point Likert scale from 1 = not relevant at all to 5 = very relevant. Participants were prompted to add individual characteristics not already included as free text.
- Intervention strategies—Participants were asked to rate various strategies used during weight management interventions as to whether they would likely increase, decrease or have no impact on eating disorder risk. Items were rated on a five-point Likert scale from 1 = very likely to reduce eating disorder risk to 5 = very likely to increase eating disorder risk. Participants were prompted to add intervention strategies not already included as free text.
- Delivery features—Participants were asked to rate the importance (important, not important, unsure) of key delivery features in relation to eating disorder risk during weight management interventions. Participants were prompted to add delivery features not already included as free text.
Content Validity and Pilot Testing
2.3. Analysis
3. Results
3.1. Participant Demographics
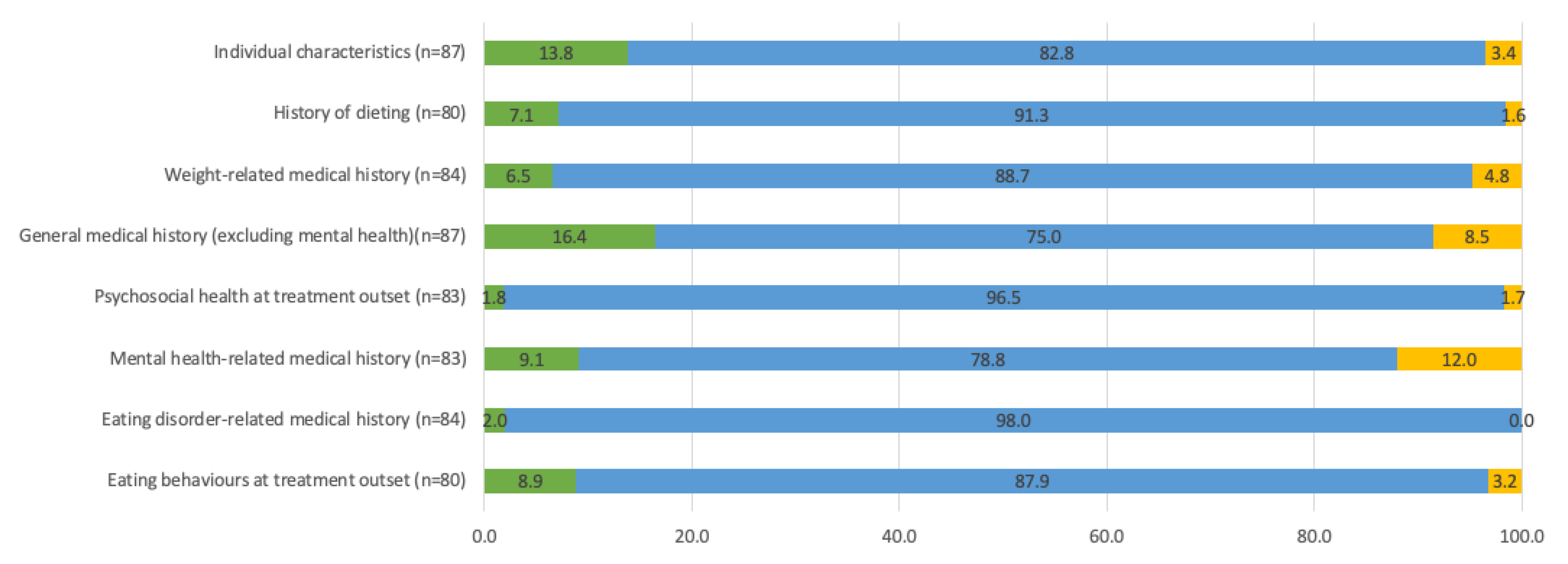
3.2. Individual Characteristics
3.3. Intervention Strategies Used during Weight Management Interventions
3.3.1. Intervention Framing and Outcomes
3.3.2. Dietary Strategies
3.3.3. Eating Behaviors and Disordered-Eating Related Strategies
3.3.4. Movement and Sleep Related Strategies
3.3.5. Psychosocial Health Related Strategies
3.4. Delivery Features
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jebeile, H.; Cardel, M.I.; Kyle, T.K.; Jastreboff, A.M. Addressing psychosocial health in the treatment and care of adolescents with obesity. Obesity 2021, 29, 1413–1422. [Google Scholar] [CrossRef] [PubMed]
- Jebeile, H.; Lister, N.B.; Baur, L.A.; Garnett, S.P.; Paxton, S.J. Eating disorder risk in adolescents with obesity. Obes. Rev. 2021, 22, e13173. [Google Scholar] [CrossRef] [PubMed]
- Lister, N.B.; Baur, L.A.; Paxton, S.J.; Jebeile, H. Contextualising Eating Disorder Concerns for Paediatric Obesity Treatment. Curr. Obes. Rep. 2021, 10, 322–331. [Google Scholar] [CrossRef] [PubMed]
- Da Luz, F.Q.; Hay, P.; Touyz, S.; Sainsbury, A. Obesity with Comorbid Eating Disorders: Associated Health Risks and Treatment Approaches. Nutrients 2018, 10, 829. [Google Scholar] [CrossRef] [Green Version]
- Stice, E.; Gau, J.M.; Rohde, P.; Shaw, H. Risk factors that predict future onset of each DSM–5 eating disorder: Predictive specificity in high-risk adolescent females. J. Abnorm. Psychol. 2017, 126, 38–51. [Google Scholar] [CrossRef]
- Cooper, Z.; Fairburn, C. Cognitive behavior therapy for bulimia nervosa. In The Treatment of Eating Disorders; Grilo, C., Mitchell, J., Eds.; Guilford Press: New York, NY, USA, 2010; pp. 243–270. [Google Scholar]
- Fairburn, C.G.; Cooper, Z.; Shafran, R. Cognitive behaviour therapy for eating disorders: A “transdiagnostic” theory and treatment. Behav. Res. Ther. 2003, 41, 509–528. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Shafran, R.; Cooper, Z. A cognitive behavioural theory of anorexia nervosa. Behav. Res. Ther. 1999, 37, 1–13. [Google Scholar] [CrossRef]
- Suarez-Albor, C.L.; Galletta, M.; Gómez-Bustamante, E. Factors associated with eating disorders in adolescents: A systematic review. Acta Bio Med. Atenei Parm. 2022, 93, e2022253. [Google Scholar] [CrossRef]
- Solmi, M.; Radua, J.; Stubbs, B.; Ricca, V.; Moretti, D.; Busatta, D.; Carvalho, A.F.; Dragioti, E.; Favaro, A.; Monteleone, A.M.; et al. Risk factors for eating disorders: An umbrella review of published meta-analyses. Rev. Bras. Psiquiatr. 2021, 43, 314–323. [Google Scholar] [CrossRef]
- Vartanian, L.R.; Porter, A.M. Weight stigma and eating behavior: A review of the literature. Appetite 2016, 102, 3–14. [Google Scholar] [CrossRef]
- Jebeile, H.; Kelly, A.S.; O’Malley, G.; Baur, L.A. Obesity in children and adolescents: Epidemiology, causes, assessment, and management. Lancet Diabetes Endocrinol. 2022, 10, 351–365. [Google Scholar] [CrossRef]
- Semlitsch, T.; Stigler, F.L.; Jeitler, K.; Horvath, K.; Siebenhofer-Kroitzsch, A. Management of overweight and obesity in primary care—A systematic overview of international evidence-based guidelines. Obes. Rev. 2019, 20, 1218–1230. [Google Scholar] [CrossRef]
- Hampl, S.E.; Hassink, S.G.; Skinner, A.C.; Armstrong, S.C.; Barlow, S.E.; Bolling, C.F.; Avila Edwards, K.C.; Eneli, I.; Hamre, R.; Joseph, M.M.; et al. Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents with Obesity. Pediatrics 2023, 151, e2022060640. [Google Scholar] [CrossRef]
- Wharton, S.; Lau, D.C.; Vallis, M.; Sharma, A.M.; Biertho, L.; Campbell-Scherer, D.; Adamo, K.; Alberga, A.; Bell, R.; Boulé, N.; et al. Obesity in adults: A clinical practice guideline. Can. Med. Assoc. J. 2020, 192, E875–E891. [Google Scholar] [CrossRef]
- Hartmann-Boyce, J.; Theodoulou, A.; Oke, J.L.; Butler, A.R.; Scarborough, P.; Bastounis, A.; Dunnigan, A.; Byadya, R.; Hobbs, F.D.R.; Sniehotta, F.F.; et al. Association between characteristics of behavioural weight loss programmes and weight change after programme end: Systematic review and meta-analysis. BMJ 2021, 374, n1840. [Google Scholar] [CrossRef]
- Al-Khudairy, L.; Loveman, E.; Colquitt, J.L.; Mead, E.; Johnson, R.E.; Fraser, H.; Olajide, J.; Murphy, M.; Velho, R.M.; O’Malley, C.; et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese adolescents aged 12 to 17 years. Cochrane Database Syst. Rev. 2017, 6, CD012651. [Google Scholar] [CrossRef] [Green Version]
- Alman, K.L.; Lister, N.B.; Garnett, S.P.; Gow, M.L.; Aldwell, K.; Jebeile, H. Dietetic management of obesity and severe obesity in children and adolescents: A scoping review of guidelines. Obes. Rev. 2020, 22, e13132. [Google Scholar] [CrossRef]
- Burke, L.E.; Wang, J.; Sevick, M.A. Self-Monitoring in Weight Loss: A Systematic Review of the Literature. J. Am. Diet. Assoc. 2011, 111, 92–102. [Google Scholar] [CrossRef] [Green Version]
- Pacanowski, C.R.; Linde, J.A.; Neumarksztainer, D. Self-Weighing: Helpful or Harmful for Psychological Well-Being? A Review of the Literature. Curr. Obes. Rep. 2015, 4, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Hayes, J.F.; Fitzsimmons-Craft, E.E.; Karam, A.M.; Jakubiak, J.; Brown, M.L.; Wilfley, D.E. Disordered Eating Attitudes and Behaviors in Youth with Overweight and Obesity: Implications for Treatment. Curr. Obes. Rep. 2018, 7, 235–246. [Google Scholar] [CrossRef]
- Lister, N.B.; Baur, L.A.; Paxton, S.J.; Garnett, S.P.; Ahern, A.L.; Wilfley, D.; Maguire, S.; Sainsbury, A.; Steinbeck, K.; Braet, C.; et al. Eating Disorders In weight-related Therapy (EDIT) Collaboration: Rationale and study design. Nutr. Res. Rev. 2023, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Johnson, B.J.; Hunter, K.E.; Golley, R.K.; Chadwick, P.; Barba, A.; Aberoumand, M.; Libesman, S.; Askie, L.; Taylor, R.W.; Robledo, K.P.; et al. Unpacking the behavioural components and delivery features of early childhood obesity prevention interventions in the TOPCHILD Collaboration: A systematic review and intervention coding protocol. BMJ Open 2022, 12, e048165. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- House, E.T.; Lister, N.B.; Seidler, A.L.; Li, H.; Ong, W.Y.; McMaster, C.M.; Paxton, S.J.; Jebeile, H. Identifying eating disorders in adolescents and adults with overweight or obesity: A systematic review of screening questionnaires. Int. J. Eat. Disord. 2022, 55, 1171–1193. [Google Scholar] [CrossRef]
- McMaster, C.M.; Paxton, S.J.; Maguire, S.; Hill, A.J.; Braet, C.; Seidler, A.L.; Nicholls, D.; Garnett, S.P.; Ahern, A.L.; Wilfley, D.E.; et al. The need for future research into the assessment and monitoring of eating disorder risk in the context of obesity treatment. Int. J. Eat. Disord. 2023, 1–11. [Google Scholar] [CrossRef]
- Jebeile, H.; Lister, N.B.; Libesman, S.; Hunter, K.E.; McMaster, C.M.; Johnson, B.J.; Baur, L.A.; Paxton, S.J.; Garnett, S.P.; Ahern, A.L.; et al. Eating Disorders In weight-related Therapy (EDIT): Protocol for a systematic review with individual par-ticipant data meta-analysis of eating disorder risk in behavioural weight management. medRxiv 2022. [Google Scholar] [CrossRef]
- Jebeile, H.; Gow, M.L.; Baur, L.A.; Garnett, S.P.; Paxton, S.J.; Lister, N.B. Treatment of obesity, with a dietary component, and eating disorder risk in children and adolescents: A systematic review with meta-analysis. Obes. Rev. 2019, 20, 1287–1298. [Google Scholar] [CrossRef] [Green Version]
- Pikoos, T.D.; Buzwell, S.; Sharp, G.; Rossell, S.L. The Zoom Effect: Exploring the Impact of Video Calling on Appearance Dissatisfaction and Interest in Aesthetic Treatment During the COVID-19 Pandemic. Aesthetic Surg. J. 2021, 41, NP2066–NP2075. [Google Scholar] [CrossRef]
- Puhl, R.; Suh, Y. Stigma and Eating and Weight Disorders. Curr. Psychiatry Rep. 2015, 17, 10. [Google Scholar] [CrossRef]


{kind=link}
| Age, n (%) | RESEARCHERS | ||
|---|---|---|---|
| 18–25 years | 7 (8) | Areas of research knowledge/experience/expertise,* n (%) | |
| 26–34 years | 19 (22) | Overweight/obesity | 25 (29) |
| 35–49 years | 35 (40) | Binge eating disorder | 20 (23) |
| 50–64 years | 18 (21) | Anorexia nervosa | 17 (20) |
| 60+ years | 8 (9) | Other eating disorders (e.g., ARFID, body image, EDNOS) | 17 (20) |
| Gender, n (%) | Bulimia nervosa | 14 (16) | |
| Female/Women | 81 (93) | Atypical anorexia nervosa | 13 (15) |
| Male/Men | 4 (5) | Years focused on research area, mean (SD) | |
| Nonbinary | 1 (1) | Overweight/obesity | 10.1 (9.1) |
| Prefer not to say | 1 (1) | Eating disorders | 8.6 (8.6) |
| Country of residence, n (%) | Co-occurring eating disorders and overweight/obesity | 6.4 (8.7) | |
| Australia | 37 (42) | Age group/s of research focus, n (%) | |
| USA | 33 (38) | Children (<10 years) | 9 (10) |
| UK | 10 (11) | Adolescents (10–17 years) | 18 (21) |
| Other ** | 7 (8) | Adults (>18 years) | 19 (22) |
| Cultural background/ethnicity, n (%) | LIVED EXPERIENCE | ||
| White | 57 (66) | Lived experience,* n (%) | |
| Mixed race | 4 (5) | High weight (BMI 25–39.9) | 46 (53) |
| Other (Asian n = 3, Black n = 1, Hispanic n = 1, New Zealand Māori, n = 1) | 6 (7) | High weight (BMI > 40) | 11 (13) |
| None | 19 (22) | Anorexia nervosa | 17 (20) |
| Prefer not to say | 2 (2) | Atypical anorexia nervosa | 11 (13) |
| Professional group * n (%) | Bulimia nervosa | 12 (14) | |
| Clinician | 60 (69) | Binge eating disorder | 16 (18) |
| Researcher | 32 (37) | Other Specified Feeding and Eating Disorders | 14 (16) |
| Neither | 16 (18) | Other eating disorder (e.g., ARFID, orthorexia) | 7 (8) |
| Other | 8 (9) | Carer/support for person with high weight | 12 (14) |
| CLINICIANS | Carer/support for person with an eating disorder | 14 (16) | |
| Discipline, n (%) | Other (Both anorexia nervosa and atypical anorexia nervosa based on BMI status; mental health conditions other than eating disorder) | 3 (3) | |
| Dietitian/nutritionist | 27 (31) | None of the above | 16 (18) |
| Psychologist/clinical psychologist | 13 (15) | Experience of weight management treatment, n (%) | |
| Pediatrician | 7 (8) | Previous weight management treatment | 18 (21) |
| Other ^ | 19 (22) | Currently receiving weight management treatment | 4 (5) |
| Area of clinical experience/expertise, * n (%) | Never received weight management treatment | 28 (32) | |
| Overweight/obesity | 49 (56) | Experience of eating disorder treatment, n (%) | |
| Binge eating disorder | 45 (52) | Previous eating disorder treatment | 16 (18) |
| Anorexia nervosa | 36 (41) | Currently receiving eating disorder treatment | 3 (3) |
| Bulimia nervosa | 36 (41) | Never received eating disorder treatment | 19 (22) |
| Atypical anorexia nervosa | 32 (37) | ||
| Other eating disorders ^^ | 32 (37) | ||
| Years involved in treatment, mean (SD) | |||
| Eating disorders | 11.7 (10.1) | ||
| Overweight/obesity | 10.9 (9.1) | ||
| Co-occurring eating disorders and overweight/obesity | 9.6 (8.9) | ||
| Hours per week involved in the treatment, mean (SD) | |||
| Eating disorders | 17.3 (15.0) | ||
| Overweight/obesity | 16.0 (15.7) | ||
| Co-occurring eating disorders and overweight/obesity | 10.2 (11.4) | ||
| Age group/s of patient seen, n (%) | |||
| Children (<10 years) | 20 (23) | ||
| Adolescents (10–17 years) | 36 (41) | ||
| Adults (>18 years) | 44 (51) | ||
| Category in Survey | Broad Theme | Specific Item |
|---|---|---|
| PART 1: INDIVIDUAL CHARACTERISTICS | ||
| Family and medical history | Genetic predisposition to obesity | Genetic risk factors for obesity Genetic influence on body shape/composition—what is normal body size for the individual |
| Weight status | History of weight fluctuation, including degree of weight change | |
| Medical history | History of bariatric surgery Investigate, diagnose and treat obstructive sleep apnea | |
| Experience of weight stigma from health professionals | Comments on weight status Withholding of medical care until weight loss occurs Trauma related to medical stigma Attitude of medical provider towards weight/BMI, especially for children/adolescents Stigmatizing micro-aggressions Previous attendance at support groups | |
| Psychosocial health and eating behaviors | Executive function | Difficulty with time management (especially parents of children) |
| Mental health (history or current) | Borderline personality disorder Addiction (including alcohol abuse) Self-harm, suicide attempts | |
| Disordered eating attitudes or behaviors | Purging Compulsive exercise Body checking Heavy use of apps/tracking food intake | |
| Emotional response to dieting/weight loss | Emotional response to unsuccessful weight loss Compliments for weight loss (negative, positive feedback), leading to further weight loss attempts Shame/guilt | |
| Other | Family context | Resilience of family Family history around negative attitudes to food/weight/body shape and food being used in families for emotional manipulation Exposure to self-disparaging comments about weight, especially from parents Patient/parent relationship Cultural factors |
| Minority groups (vulnerable/marginalized groups) | Power imbalance with health professionals Gender identity Athletes | |
| Social determinants of health (other than food insecurity) | ||
| Environmental context/social media use | Social media use Exposure to diet culture Body size in relation to those around them Experience of fatphobia Consider risk factors (e.g., body shape/weight disturbance) within the social context of the individual, e.g., body shape/weight disturbance is reasonable in the context of societies that deem larger bodies as less valuable | |
| PART 2: INTERVNETION STRATEGIES | ||
| Intervention framing | Communication approaches | Decrease emphasis on personal responsibility (decreases risk) Use encouragement (rather than measurements) Individualized framing Program language/images used, e.g., comparing to ‘success’ stories Emphasizes broader quality of life benefits rather than focusing on weight |
| Education approaches | Explaining the science of weight/appetite regulation and weight stigma (decrease risk) Using life expectancy to frame weight loss as a path to health and longevity Discussing weight in terms of healthy growth | |
| Dietary strategies | Role of family dynamics in food choice/selection | Consider food insecurity as part of intervention Food choices differ from rest of household Family education on eating disorder risk and flexible eating |
| Framing/labeling of foods | Framing/delivery/communication of all dietary strategies is important Consider how foods feel in the body, energy levels, satiation Use of good/bad language, e.g., dichotomizing food as “healthy” vs. “unhealthy” (increase risk) | |
| Dietary prescription | Rigid dietary prescriptions increase risk Weighing and measuring foods (increases risk) | |
| Eating behavior strategies | Role of culture | Consider cultural context of food and role of food in culture (decrease risk). |
| Address energy restriction | Energy restriction leading to hunger and binge eating (cycle) (increases risk). Education on a healthy menstrual cycle and link with under-eating and over-exercising. | |
| Context of eating behavior | Use of intuitive eating in the context of weight management increases eating disorder risk. Emotional eating is a normal part of intuitive and mindful eating and should not be demonized or categorized as disordered eating. | |
| Comments re eating behaviors | Examining disordered eating behaviors may not be appropriate in children (safety concern?) Screening for these eating behaviors may help to identify eating disorders and facilitate referral and support. Screening is unlikely to exacerbate disordered eating. | |
| Movement and sleep strategies | Sleep quality | Improve circadian alignment and total sleep time |
| Attitudes, beliefs and training/qualifications of trainers contributes to level of ED risk | Appearance- and weight-loss-focused personal trainer (increase risk) Focus on healthy habits, QOL, goals—unlikely to increase risk | |
| Motivations for activity | Mental and physical health motivations for exercise vs. shape/weight/appearance motivators Promoting PA/movement without a weight loss focus (decreases risk). Having exercise focused on weight loss rather than being fun. | |
| Psychosocial health | Education/approach to aspects of psychosocial health | Education on internalized and externally received weight biases. Health at Every Size principles Education that undereating is related to anxiety, depression and difficulty concentrating. Education on difficulty with maintaining long term weight loss—sense of failure can lead to shame. Strategies that utilize normalizing and addressing shame for carer and young person |
| PART 3: DELIVERY FEATURES | ||
| Duration of intervention | Need for long term support/continuity of care | Weight regain can lead to self-blame, feelings of failure Step up/step down pathways Multidisciplinary care |
| Mode of delivery | Mode of delivery | Telehealth/video conferencing associated with appearance concerns and body dissatisfaction |
| Setting | Environment | Environmental contributions, e.g., supportive chairs Safe space without intersectional biases. Understanding of group rules and behavior |
| Personnel | Training needs | Professionals (providing weight management) need to have a thorough understanding of ED and body image issues |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jebeile, H.; McMaster, C.M.; Johnson, B.J.; Garnett, S.P.; Paxton, S.J.; Seidler, A.L.; Jones, R.A.; Hill, A.J.; Maguire, S.; Braet, C.; et al. Identifying Factors Which Influence Eating Disorder Risk during Behavioral Weight Management: A Consensus Study. Nutrients 2023, 15, 1085. https://doi.org/10.3390/nu15051085
Jebeile H, McMaster CM, Johnson BJ, Garnett SP, Paxton SJ, Seidler AL, Jones RA, Hill AJ, Maguire S, Braet C, et al. Identifying Factors Which Influence Eating Disorder Risk during Behavioral Weight Management: A Consensus Study. Nutrients. 2023; 15(5):1085. https://doi.org/10.3390/nu15051085
Chicago/Turabian StyleJebeile, Hiba, Caitlin M. McMaster, Brittany J. Johnson, Sarah P. Garnett, Susan J. Paxton, Anna L. Seidler, Rebecca A. Jones, Andrew J. Hill, Sarah Maguire, Caroline Braet, and et al. 2023. "Identifying Factors Which Influence Eating Disorder Risk during Behavioral Weight Management: A Consensus Study" Nutrients 15, no. 5: 1085. https://doi.org/10.3390/nu15051085