
Demand for Water-Soluble Vitamins in a Group of Patients with CKD versus Interventions and Supplementation—A Systematic Review
 ,
, 
Abstract
:1. Introduction—CKD Causes and Metabolic Effects
1.1. Epidemiology and Classification
- Hyperglycemia;
- Hypertension;
- Hyperlipidemia;
- Hyperphosphatemia;
- Diets rich in animal protein.
- Inhibiting kidney damage;
- Preventing malnutrition;
- Reducing the severity of metabolic disorders.
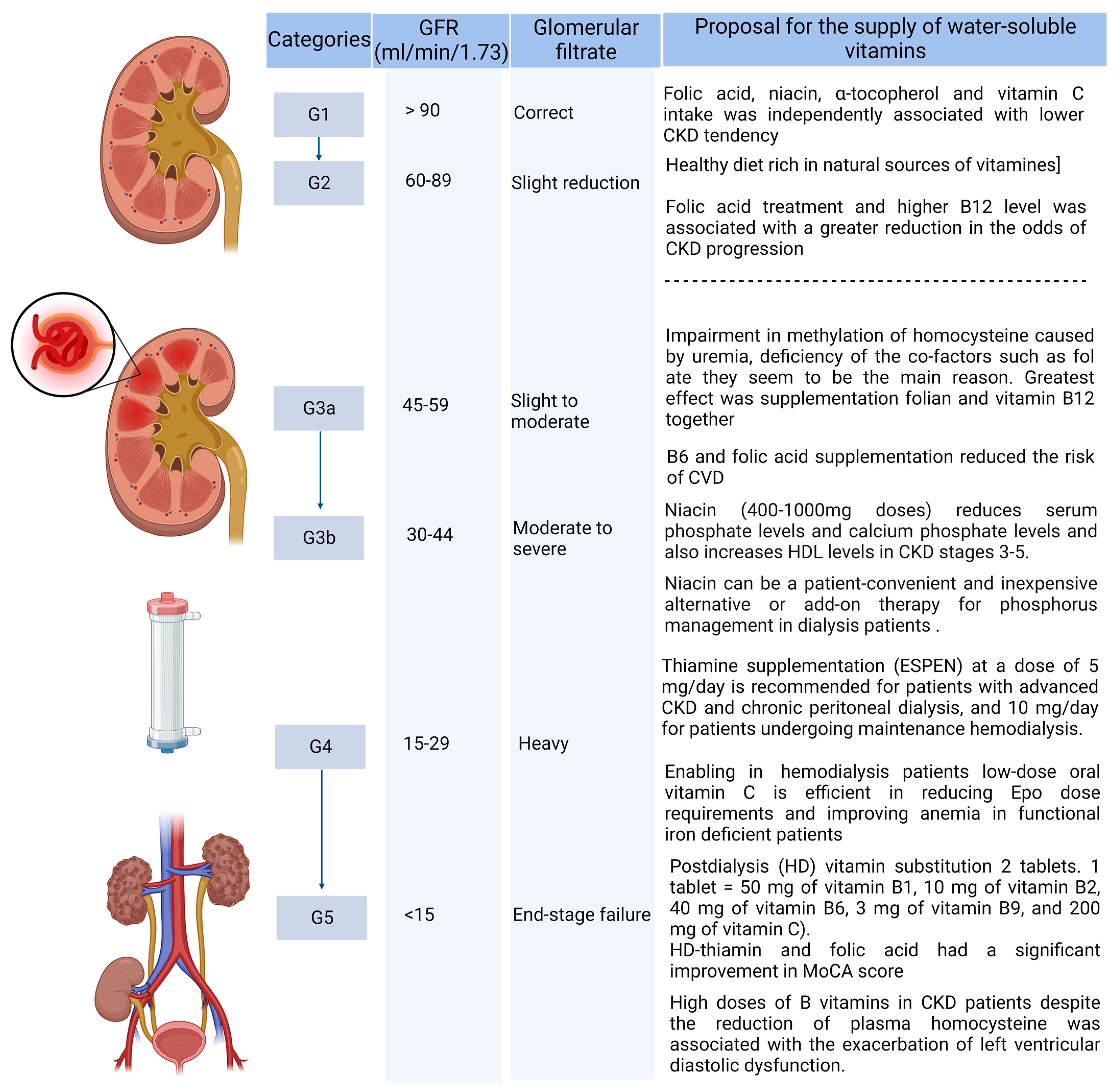
- Stage 1—Normal or high GFR (GFR > 90 mL/min/1.73 m2);
- Stage 2—Mild CKD (GFR = 60–89 mL/min/1.73 m2);
- Stage 3A—Moderate CKD (GFR = 45–59 mL/min/1.73 m2);
- Stage 3B—Moderate CKD (GFR = 30–44 mL/min/1.73 m2);
- Stage 4—Severe CKD (GFR = 15–29 mL/min/1.73 m2);
- Stage 5—End-stage CKD (GFR < 15 mL/min/1.73 m2).
1.2. Metabolic Effects in CKD
1.3. Nutritional Status in CKD
1.4. Peritoneal Dialysis and Hemodialysis vs. Macronutrients
1.5. Peritoneal Dialysis and Hemodialysis vs. Vitamins
1.6. Diet Rich in Vitamins and Antioxidants in CKD
1.7. Anitioxidant Therapy
1.8. Uremic Microbiota and Intestinal Inflammation and Its Impact on Vitamin Absorption
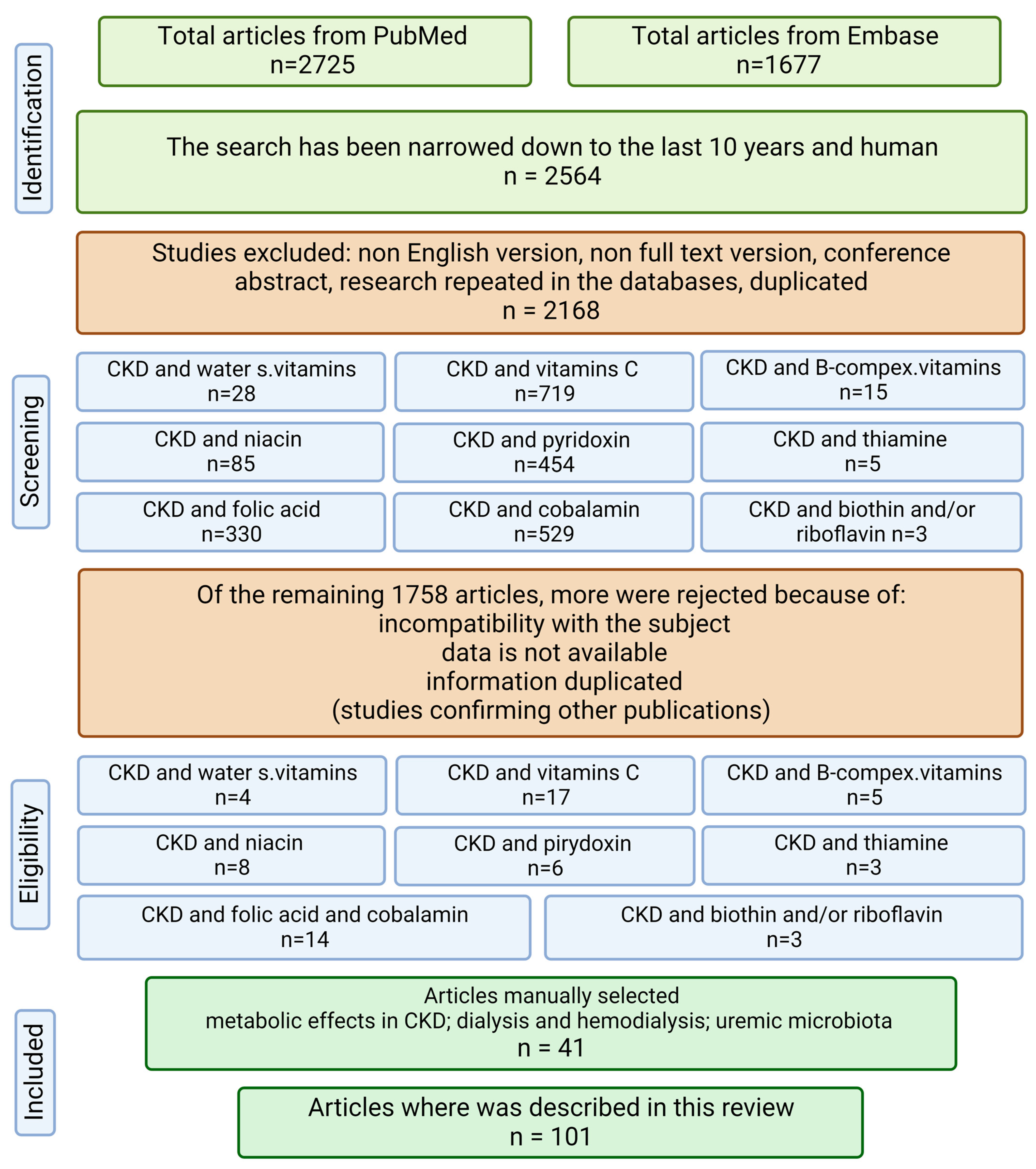
2. Material and Methods
3. Discussion—Supplementation with Water-Soluble Vitamins
3.1. Vitamin C Supplementation
3.2. Supplementation with Folate and Cobalamin
3.3. Pyridoxine Supplementation
3.4. Niacin Supplementation
3.5. Supplementation with Thiamine
3.6. Supplementation with Biotin
3.7. Supplementation with Riboflavin
4. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Capelli, I.; Cianciolo, G.; Gasperoni, L.; Zappulo, F.; Tondolo, F.; Cappuccilli, M.; La Manna, G. Folic Acid and Vitamin B12 Administration in CKD, Why Not? Nutrients 2019, 11, 383. [Google Scholar] [CrossRef]
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; De Francisco, A.L.; De Jong, P.E.; Griffith, K.E.; Hemmelgarn, B.R.; Iseki, K.; Lamb, E.J.; et al. Kidney Disease Improving Global Outcomes—KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. Suppl. 2013, 1, 1–150. [Google Scholar]
- Garneata, L.; Stancu, A.; Dragomir, D.; Stefan, G.; Mircescu, G. Ketoanalogue-Supplemented Vegetarian Very Low–Protein Diet and CKD Progression. J. Am. Soc. Nephrol. 2016, 27, 2164–2176. [Google Scholar] [CrossRef]
- Oliveira, E.A.; Zheng, R.; Carter, C.E.; Mak, R.H. Cachexia/Protein energy wasting syndrome in CKD: Causation and treatment. Semin. Dial. 2019, 32, 493–499. [Google Scholar] [CrossRef]
- Available online: https://www.who.int/ (accessed on 28 November 2022).
- Baker, R.J.; Syed, K.; Minteer, J.F. Cachexia. [Updated 2022 Aug 8]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470208/ (accessed on 20 September 2022).
- Ikizler, T.A.; Cano, N.J.; Franch, H.; Fouque, D.; Himmelfarb, J.; Kalantar-Zadeh, K.; Kuhlmann, M.K.; Stenvinkel, P.; TerWee, P.; Teta, D.; et al. Prevention and treatment of protein energy wasting in chronic kidney disease patients: A consensus statement by the International Society of Renal Nutrition and Metabolism. Kidney Int. 2013, 84, 1096–1107. [Google Scholar] [CrossRef]
- Carrero, J.J.; Stenvinkel, P.; Cuppari, L.; Ikizler, T.A.; Kalantar-Zadeh, K.; Kaysen, G.; Mitch, W.E.; Price, S.R.; Wanner, C.; Wang, A.Y.; et al. Etiology of the Protein-Energy Wasting Syndrome in Chronic Kidney Disease: A Consensus Statement From the International Society of Renal Nutrition and Metabolism (ISRNM). J. Ren. Nutr. 2013, 23, 77–90. [Google Scholar] [CrossRef]
- Fouque, D.; Kalantar-Zadeh, K.; Kopple, J.; Cano, N.; Chauveau, P.; Cuppari, L.; Franch, H.; Guarnieri, G.; Ikizler, T.A.; Kaysen, G.; et al. A proposed nomenclature and diagnostic criteria for protein–energy wasting in acute and chronic kidney disease. Kidney Int. 2008, 73, 391–398. [Google Scholar] [CrossRef]
- Hara, H.; Nakamura, Y.; Hatano, M.; Iwashita, T.; Shimizu, T.; Ogawa, T.; Kanozawa, K.; Hasegawa, H. Protein Energy Wasting and Sarcopenia in Dialysis Patients. Contrib. Nephrol. 2018, 196, 243–249. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Block, G.; Humphreys, M.H.; Kopple, J.D. Reverse epidemiology of cardiovascular risk factors in maintenance dialysis patients. Kidney Int. 2003, 63, 793–808. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.-J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76 (Suppl. 1), S1–S107. [Google Scholar] [CrossRef]
- Takashima, H.; Maruyama, T.; Abe, M. Significance of Levocarnitine Treatment in Dialysis Patients. Nutrients 2021, 13, 1219. [Google Scholar] [CrossRef]
- Schmidt, J.J.; Hafer, C.; Spielmann, J.; Hadem, J.; Schönenberger, E.; Schmidt, B.M.; Kielstein, J.T. Removal Characteristics and Total Dialysate Content of Glutamine and Other Amino Acids in Critically Ill Patients with Acute Kidney Injury Undergoing Extended Dialysis. Nephron Clin. Pract. 2014, 126, 62–66. [Google Scholar] [CrossRef]
- Murtas, S.; Aquilani, R.; Iadarola, P.; Deiana, M.L.; Secci, R.; Cadeddu, M.; Bolasco, P. Differences and Effects of Metabolic Fate of Individual Amino Acid Loss in High-Efficiency Hemodialysis and Hemodiafiltration. J. Ren. Nutr. 2020, 30, 440–451. [Google Scholar] [CrossRef]
- Bolasco, P. Hemodialysis—Nutritional Flaws in Diagnosis and Prescriptions. Could Amino Acid Losses Be the Sharpest “Sword of Damocles”? Nutrients 2020, 12, 1773. [Google Scholar] [CrossRef]
- Lim, V.S.; Bier, D.M.; Flanigan, M.J.; Sum-Ping, S.T. The effect of hemodialysis on protein metabolism. A leucine kinetic study. J. Clin. Investig. 1993, 91, 2429–2436. [Google Scholar] [CrossRef]
- Kirsch, A.H.; Lyko, R.; Nilsson, L.-G.; Beck, W.; Amdahl, M.; Lechner, P.; Schneider, A.; Wanner, C.; Rosenkranz, A.R.; Krieter, D.H. Performance of hemodialysis with novel medium cut-off dialyzers. Nephrol. Dial. Transplant. 2017, 32, 165–172. [Google Scholar] [CrossRef]
- Belmouaz, M.; Bauwens, M.; Lecron, J.-C.; Sibille, A.; Ecotiere, L.; Dufour, L.; Thierry, A.; Bridoux, F. Protein loss and medium cut-off haemodialysis. Clin. Kidney J. 2021, 14, 460–461. [Google Scholar] [CrossRef]
- Donadio, E.; Piccolomini, F.; Dimuccio, V.; Felicioli, A.; Balestreri, E.; Cianti, R.; Armini, A.; Bini, L.; Felicioli, R.; Donadio, C. Serum albumin fragmentation in end-stage renal disease patients—A pilot study. Clin. Chem. Lab. Med. 2009, 47, 1373–1379. [Google Scholar] [CrossRef]
- Panichi, V.; Maggiore, U.; Taccola, D.; Migliori, M.; Rizza, G.M.; Consani, C.; Bertini, A.; Sposini, S.; Perez-Garcia, R.; Rindi, P.; et al. Interleukin-6 is a stronger predictor of total and cardiovascular mortality than C-reactive protein in haemodialysis patients. Nephrol. Dial. Transplant. 2004, 19, 1154–1160. [Google Scholar] [CrossRef]
- Jerin, A.; Mosa, O.F.; Kališnik, J.M.; Žibert, J.; Skitek, M. Serum klotho as a marker for early diagnosis of acute kidney injury after cardiac surgery. J. Med. Biochem. 2019, 39, 133–139. [Google Scholar] [CrossRef]
- Guedes, A.M.; Marques, R.C.; Domingos, A.T.; Laranjo, C.; Silva, A.P.; Rodrigues, A. Protein Loss in Peritoneal Effluent: Different Meaning for 24-h versus PET Samples. Blood Purif. 2022, 1–8. [Google Scholar] [CrossRef]
- Maraj, M.; Kuśnierz-Cabala, B.; Dumnicka, P.; Gala-Błądzińska, A.; Gawlik, K.; Pawlica-Gosiewska, D.; Ząbek-Adamska, A.; Mazur-Laskowska, M.; Ceranowicz, P.; Kuźniewski, M. Malnutrition, Inflammation, Atherosclerosis Syndrome (MIA) and Diet Recommendations among End-Stage Renal Disease Patients Treated with Maintenance Hemodialysis. Nutrients 2018, 10, 69. [Google Scholar] [CrossRef] [PubMed]
- Szczuko, M.; Hawryłkowicz, W.; Kikut, J.; Drozd, A. The implications of vitamin content in the plasma in reference to the parameters of carbohydrate metabolism and hormone and lipid profiles in PCOS. J. Steroid Biochem. Mol. Biol. 2019, 198, 105570. [Google Scholar] [CrossRef]
- Suzuki, H.; Kunisawa, J. Vitamin-mediated immune regulation in the development of inflammatory diseases. Endocr. Metab. Immune Disord. Drug Targets 2015, 15, 212–215. [Google Scholar] [PubMed]
- Mandl, J.; Szarka, A.; Bánhegyi, G. Vitamin C: Update on physiology and pharmacology. Br. J. Pharmacol. 2009, 157, 1097–1110. [Google Scholar] [CrossRef]
- Tu, H.; Li, H.; Wang, Y.; Niyyati, M.; Wang, Y.; Leshin, J.; Levine, M. Low red blood cell vitamin C concentrations induce red blood cell fragility: A link to diabetes via glucose, glucose transporters, and dehydroascorbic acid. EBioMedicine 2015, 2, 1735–1750. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Alharbi, M.; Wani, K.; Abd-Alrahman, S.H.; Sheshah, E.; Alokail, M.S. Biochemical changes correlated with blood thiamine and its phosphate esters levels in patients with diabetes type 1 (DMT1). Int. J. Clin. Exp. Pathol. 2015, 8, 13483–13488. [Google Scholar] [PubMed]
- Jiao, X.; Chen, W.; Zhang, J.; Wang, W.; Song, J.; Chen, D.; Zhu, W.; Shi, Y.; Yu, X. Variant Alleles of the ESR1, PPARG, HMGA2, and MTHFR Genes Are Associated With Polycystic Ovary Syndrome Risk in a Chinese Population: A Case-Control Study. Front. Endocrinol. 2018, 9, 504. [Google Scholar] [CrossRef] [PubMed]
- Stein, G.; Sperschneider, H.; Koppe, S. Vitamin Levels in Chronic Renal Failure and Need for Supplementation. Blood Purif. 1985, 3, 52–62. [Google Scholar] [CrossRef]
- Bévier, A.; Novel-Catin, E.; Blond, E.; Pelletier, S.; Parant, F.; Koppe, L.; Fouque, D. Water-Soluble Vitamins and Trace Elements Losses during On-Line Hemodiafiltration. Nutrients 2022, 14, 3454. [Google Scholar] [CrossRef]
- Morena, M.; Cristol, J.-P.; Bosc, J.-Y.; Tetta, C.; Forret, G.; Leger, C.-L.; Delcourt, C.; Papoz, L.; Descomps, B.; Canaud, B. Convective and diffusive losses of vitamin C during haemodiafiltration session: A contributive factor to oxidative stress in haemodialysis patients. Nephrol. Dial. Transplant. 2002, 17, 422–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chazot, C.; Jean, G.; Kopple, J.D. Can Outcomes be Improved in Dialysis Patients by Optimizing Trace Mineral, Micronutrient, and Antioxidant Status? The Impact of Vitamins and their Supplementation. Semin. Dial. 2015, 29, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Schwotzer, N.; Kanemitsu, M.; Kissling, S.; Darioli, R.; Benghezal, M.; Rezzi, S.; Burnier, M.; Pruijm, M. Water-Soluble Vitamin Levels and Supplementation in Chronic Online Hemodiafiltration Patients. Kidney Int. Rep. 2020, 5, 2160–2167. [Google Scholar] [CrossRef]
- Sirover, W.D.; Liu, Y.; Logan, A.; Hunter, K.; Benz, R.L.; Prasad, D.; Avila, J.; Venkatchalam, T.; Weisberg, L.S.; Handelman, G.J. Plasma Ascorbic Acid Concentrations in Prevalent Patients With End-Stage Renal Disease on Hemodialysis. J. Ren. Nutr. 2015, 25, 292–300. [Google Scholar] [CrossRef]
- Nigwekar, S.U.; Kang, A.; Zoungas, S. Interventions for lowering plasma homocysteine levels in dialysis patients. Cochrane Database Syst Rev. 2016, 5, CD004683. [Google Scholar]
- Kowalska, K.; Brodowski, J.; Pokorska-Niewiada, K.; Szczuko, M. The Change in the Content of Nutrients in Diets Eliminating Products of Animal Origin in Comparison to a Regular Diet from the Area of Middle-Eastern Europe. Nutrients 2020, 12, 2986. [Google Scholar] [CrossRef]
- Traber, M.G.; Atkinson, J. Vitamin E, antioxidant and nothing more. Free Radic. Biol. Med. 2007, 43, 4–15. [Google Scholar] [CrossRef]
- Szczuko, M.; Kaczkan, M.; Drozd, A.; Maciejewska, D.; Palma, J.; Owczarzak, A.; Marczuk, N.; Rutkowski, P.; Małgorzewicz, S. Comparison of Fatty Acid Profiles in a Group of Female Patients with Chronic Kidney Diseases (CKD) and Metabolic Syndrome (MetS)–Similar Trends of Changes, Different Pathophysiology. Int. J. Mol. Sci. 2019, 20, 1719. [Google Scholar] [CrossRef]
- Sinopoli, A.; Caminada, S.; Isonne, C.; Santoro, M.M.; Baccolini, V. What Are the Effects of Vitamin A Oral Supplementation in the Prevention and Management of Viral Infections? A Systematic Review of Randomized Clinical Trials. Nutrients 2022, 14, 4081. [Google Scholar] [CrossRef]
- Sabatino, A.; Regolisti, G.; Gandolfini, I.; Delsante, M.; Fani, F.; Gregorini, M.C.; Fiaccadori, E. Diet and enteral nutrition in patients with chronic kidney disease not on dialysis: A review focusing on fat, fiber and protein intake. J. Nephrol. 2017, 30, 743–754. [Google Scholar] [CrossRef]
- Gluba-Brzózka, A.; Franczyk, B.; Rysz, J. Vegetarian Diet in Chronic Kidney Disease—A Friend or Foe. Nutrients 2017, 9, 374. [Google Scholar] [CrossRef] [PubMed]
- Garagarza, C.; Valente, A.; Caetano, C.; Ramos, I.; Sebastião, J.; Pinto, M.; Oliveira, T.; Ferreira, A.; Guerreiro, C.S. Do dietary patterns influence survival in hemodialysis patients? Clin. Nutr. ESPEN 2021, 46, S664. [Google Scholar] [CrossRef]
- Bolignano, D.; Cernaro, V.; Gembillo, G.; Baggetta, R.; Buemi, M.; D’Arrigo, G. Antioxidant agents for diabetic kidney disease: A systematic review and meta-analysis of randomized controlled trials. Nephrol. Dial. Transplant. 2017, 32, iii266–iii267. [Google Scholar] [CrossRef]
- Jun, M.; Venkataraman, V.; Razavian, M.; Cooper, B.; Zoungas, S.; Ninomiya, T.; Webster, A.C.; Perkovic, V. Antioxidants for chronic kidney disease. Cochrane Database Syst. Rev. 2012, 2014, CD008176. [Google Scholar] [CrossRef]
- Zahan, S.; Ahmed, K.A.; Moni, A.; Sinopoli, A.; Ha, H.; Uddin, J. Kidney protective potential of lactoferrin: Pharmacological insights and therapeutic advances. Korean J. Physiol. Pharmacol. 2022, 26, 1–13. [Google Scholar] [CrossRef]
- Khor, B.-H.; Narayanan, S.S.; Sahathevan, S.; Gafor, A.H.A.; Daud, Z.A.M.; Khosla, P.; Sabatino, A.; Fiaccadori, E.; Chinna, K.; Karupaiah, T. Efficacy of Nutritional Interventions on Inflammatory Markers in Haemodialysis Patients: A Systematic Review and Limited Meta-Analysis. Nutrients 2018, 10, 397. [Google Scholar] [CrossRef]
- Lin, P.-C.; Chou, C.-L.; Ou, S.-H.; Fang, T.-C.; Chen, J.-S. Systematic Review of Nutrition Supplements in Chronic Kidney Diseases: A GRADE Approach. Nutrients 2021, 13, 469. [Google Scholar] [CrossRef]
- Rysz, J.; Franczyk, B.; Ławiński, J.; Olszewski, R.; Ciałkowska-Rysz, A.; Gluba-Brzózka, A. The Impact of CKD on Uremic Toxins and Gut Microbiota. Toxins 2021, 13, 252. [Google Scholar] [CrossRef]
- Castillo-Rodriguez, E.; Fernandez-Prado, R.; Esteras, R.; Perez-Gomez, M.V.; Gracia-Iguacel, C.; Fernandez-Fernandez, B.; Kanbay, M.; Tejedor, A.; Lazaro, A.; Ruiz-Ortega, M.; et al. Impact of Altered Intestinal Microbiota on Chronic Kidney Disease Progression. Toxins 2018, 10, 300. [Google Scholar] [CrossRef]
- Cupisti, A.; D’Alessandro, C.; Gesualdo, L.; Cosola, C.; Gallieni, M.; Egidi, M.F.; Fusaro, M. Non-Traditional Aspects of Renal Diets: Focus on Fiber, Alkali and Vitamin K1 Intake. Nutrients 2017, 9, 444. [Google Scholar] [CrossRef]
- Pham, K.-O.; Hara, A.; Tsujiguchi, H.; Suzuki, K.; Suzuki, F.; Miyagi, S.; Kannon, T.; Sato, T.; Hosomichi, K.; Tsuboi, H.; et al. Association between Vitamin Intake and Chronic Kidney Disease According to a Variant Located Upstream of the PTGS1 Gene: A Cross-Sectional Analysis of Shika Study. Nutrients 2022, 14, 2082. [Google Scholar] [CrossRef] [PubMed]
- Rafeq, Z.; Roh, J.; Guarino, P.; Kaufman, J.; Joseph, J. Adverse myocardial effects of B-vitamin therapy in subjects with chronic kidney disease and hyperhomocysteinaemia. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 836–842. [Google Scholar] [CrossRef] [PubMed]
- Devi, S.; Kennedy, R.H.; Joseph, L.; Shekhawat, N.S.; Melchert, R.; Joseph, J. Effect of long-term hyperhomocysteinemia on myocardial structure and function in hypertensive rats. Cardiovasc. Pathol. 2006, 15, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Raimann, J.G.; Trial, T.F.; Abbas, S.R.; Liu, L.; Larive, B.; Beck, G.; Kotanko, P.; Levin, N.W.; Handelman, G. The effects of more frequent hemodialysis (HD) on plasma vitamin c concentration: An ancillary study of the frequent hemodialysis network (FHN) daily trial. J. Am. Soc. Nephrol. 2017, 28, 720. [Google Scholar] [CrossRef]
- Biniaz, V.; Sadeghi Shermeh, M.S.; Ebadi, A.; Tayebi, A.; Einollahi, B. The Effect of Vitamin C on Parathyroid Hormone in Patients on Hemodialysis With Secondary Hyperparathyroidism: A Double Blind, Placebo-Controlled Study. Nephro-Urol. Mon. 2013, 5, 962–966. [Google Scholar] [CrossRef]
- Ali, M.M.Z.; Behairy, M.A.E.; El Sharabasy, R.M.; Gharib, A.H.A. Effects of Oral Vitamin C on Hepcidin Levels and Erythropoietin Requirements in Functional Iron Deficiency Anemia among Hemodialysis Patients. QJM Int. J. Med. 2021, 114 (Suppl. 1), hcab100-015. [Google Scholar] [CrossRef]
- Conner, T.A.; McQuade, C.; Olp, J.; Pai, A.B. Effect of intravenous vitamin C on cytokine activation and oxidative stress in end-stage renal disease patients receiving intravenous iron sucrose. Biometals 2012, 25, 961–969. [Google Scholar] [CrossRef]
- Fontana, F.; Cazzato, S.; Giovanella, S.; Ballestri, M.; Leonelli, M.; Mori, G.; Alfano, G.; Ligabue, G.; Magistroni, R.; Cenacchi, G.; et al. Oxalate Nephropathy Caused by Excessive Vitamin C Administration in 2 Patients With COVID-19. Kidney Int. Rep. 2020, 5, 1815–1822. [Google Scholar] [CrossRef]
- Sedighi, O.; Makhlough, A.; Janbabai, G.; Neemi, M. Comparative Study of Intravenous Iron Versus Intravenous Ascorbic Acid for Treatment of Functional Iron Deficiency in Patients Under Hemodialysis. A Randomized Clinical Trial. Nephro-Urology Mon. 2013, 5, 913–917. [Google Scholar] [CrossRef]
- Generali, J.A.; Cada, D.J. Ascorbic Acid: Prevention of Contrast-Induced Nephropathy. Hosp. Pharm. 2012, 47, 842–844. [Google Scholar] [CrossRef]
- Dvoršak, B.; Kanič, V.; Ekart, R.; Bevc, S.; Hojs, R. Ascorbic Acid for the Prevention of Contrast-Induced Nephropathy After Coronary Angiography in Patients With Chronic Renal Impairment: A Randomized Controlled Trial. Ther. Apher. Dial. 2013, 17, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Hongsawong, N.; Chawprang, N.; Kittisakmontri, K.; Vittayananan, P.; Srisuwan, K.; Chartapisak, W. Vitamin C deficiency and impact of vitamin C administration among pediatric patients with advanced chronic kidney disease. Pediatr. Nephrol. 2021, 36, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Sultana, T.; DeVita, M.V.; Michelis, M.F. Oral vitamin C supplementation reduces erythropoietin requirement in hemodialysis patients with functional iron deficiency. Int. Urol. Nephrol. 2016, 48, 1519–1524. [Google Scholar] [CrossRef] [PubMed]
- Sultana, T.; DeVita, M.V.; Michelis, M.F. Oral Vitamin C supplemientation for functional iron deficiency in dialysis patients. Am. J. Kidney Dis. 2015, 65, A83. [Google Scholar]
- Jiang, K.; Tang, K.; Liu, H.; Xu, H.; Ye, Z.; Chen, Z. Ascorbic Acid Supplements and Kidney Stones Incidence Among Men and Women: A systematic review and meta-analysis. Urol J. 2019, 16, 115–120. [Google Scholar] [CrossRef]
- Rafie, S.; Jafari, M. A Comparative study on the effects of vitamin C and Pramipexole on restless legs syndrome treatment in hemodialysis patients: A randomized, doubleblind, placebo-controlled trial. Int. J. Pharm. Res. Allied Sci. 2016, 5, 128–134. [Google Scholar]
- Sagheb, M.M.; Dormanesh, B.; Fallahzadeh, M.K.; Akbari, H.; Nazari, S.S.; Heydari, S.T.; Behzadi, S. Efficacy of vitamins C, E, and their combination for treatment of restless legs syndrome in hemodialysis patients: A randomized, double-blind, placebo-controlled trial. Sleep Med. 2012, 13, 542–545. [Google Scholar] [CrossRef]
- Gungor, O.; Ulu, S.; Hasbal, N.B.; Onan, E.; Turgut, D.; Arici, M. Do Hemodialysis Patients Need Immune Boosting with Vitamin, Mineral, and Probiotic Supplementation during COVID-19 Pandemic? Turk. J. Nephrol. 2021, 30, 326–332. [Google Scholar] [CrossRef]
- Khokher, W.; Kesireddy, N.; Herath Mudiyanselage, P.; Iftikhar, S.; Beran, A.; Alom, M.; Rashid, R.; Ali, H.; Awad, M. The role of ascorbic acid in reducing the incidence of stage 3 acute kidney injury in patients wiyh septic shock: A systematic review and meta-analysis. Chest 2021, 160, A1057. [Google Scholar]
- Achour, O.; Elmtaoua, S.; Zellama, D.; Omezzine, A.; Moussa, A.; Rejeb, J.; Boumaiza, I.; Bouacida, L.; Ben Rejeb, N.; Achour, A.; et al. The C677T MTHFR genotypes influence the efficacy of B9 and B12 vitamins supplementation to lowering plasma total homocysteine in hemodialysis. J. Nephrol. 2016, 29, 691–698. [Google Scholar] [CrossRef]
- Righetti, M. Homocysteine-lowering vitamin B treatment decreases cardiovascular events in hemodialysis patients. Clin. Chem. Lab. Med. 2007, 45, 1586–1589. [Google Scholar] [CrossRef] [PubMed]
- Amini, M.; Khosravi, M.; Baradaran, H.R.; Atlasi, R. Vitamin B12 supplementation in end stage renal diseases: A systematic review. Med. J. Islam. Repub. Iran 2015, 29, 167. [Google Scholar]
- Bravo-Soto, G.A.; Madrid, T. Is folic acid supplementation useful for chronic kidney disease? Medwave 2016, 16, e6591. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Qin, X.; Luo, L.; Wang, B.; Huo, Y.; Hou, F.F.; Xu, X. Folic acid therapy reduces the risk of mortality associated with heavy proteinuria among hypertensive patients. J. Hypertens. 2017, 35, 1302–1309. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Ye, Z.; Wu, Q.; Yang, S.; Zhang, Y.; Zhou, C.; He, P.; Zhang, Y.; Nie, J.; Liang, M.; et al. Folate intake and incident chronic kidney disease: A 30-year follow-up study from young adulthood to midlife. Am. J. Clin. Nutr. 2022, 116, 599–607. [Google Scholar] [CrossRef]
- Yan, L.-J.; Zhang, F.-R.; Zeng, Y.-R.; Zheng, Y. Serum Folate and All-Cause Mortality is of Non-Linear Relationship Among Population with Chronic Kidney Disease: A Retrospective Cohort Study. Int. J. Gen. Med. 2021, 14, 2695–2702. [Google Scholar] [CrossRef]
- Qin, X.; Huo, Y.; Xie, D.; Hou, F.; Xu, X.; Wang, X. Homocysteine-lowering therapy with folic acid is effective in cardiovascular disease prevention in patients with kidney disease: A meta-analysis of randomized controlled trials. Clin. Nutr. 2013, 32, 722–727. [Google Scholar] [CrossRef]
- Li, Y.; Spence, J.D.; Wang, X.; Huo, Y.; Xu, X.; Qin, X. Effect of Vitamin B12 Levels on the Association Between Folic Acid Treatment and CKD Progression: A Post Hoc Analysis of a Folic Acid Interventional Trial. Am. J. Kidney Dis. 2020, 75, 325–332. [Google Scholar] [CrossRef]
- Lu, R.; Jin, H.; Xu, C.; Qian, C.; Wang, M.; Lin, Y.; Zhou, Y.; Gu, L.; Ni, Z. Effects of thiamine and folic acid on oxidative stress and cognitive function in maintenance hemodialysis patients: A pilot prospective randomized controlled study. Blood Purif. 2021, 50, 417. [Google Scholar] [CrossRef]
- Lydia, A.; Priantono, D.; Harimurti, K.; Alwi, I. The Relationship between Folic Acid and Vitamin B12 Serum Levels with High Sensitivity C-reactive Protein and Homocysteine in Chronic Hemodialysis Patients: A Cross-sectional Study. Acta Med. Indones. 2021, 53, 282–290. [Google Scholar]
- Xu, X.; Qin, X.; Li, Y.; Sun, D.; Wang, J.; Liang, M.; Wang, B.; Huo, Y.; Hou, F.F. Efficacy of folic acid therapy on the progression of chronic kidney disease: The renal substudy of the China stroke primary prevention trial. JAMA Intern. Med. 2016, 176, 1443–1450. [Google Scholar] [CrossRef]
- Nahas, A.R.M.F.; Al Zarzour, R.H.; Abu Laila, A.S.M.; Tabash, A.M.; Abu Mustafa, A.M.; Allyan, F.M.; Elregeb, A.M.; Teior, E.E.M.A.; Al-Shami, A.M.; Elnaem, M.H. Effect of B12 supplementation on renal anemia among hemodialysis patients at El-Najar hospital, Gaza strip. J. Ren. Inj. Prev. 2022, x, e32009. [Google Scholar] [CrossRef]
- Jankowska, M.; Rutkowski, B.; Dębska-Ślizień, A. Vitamins and Microelement Bioavailability in Different Stages of Chronic Kidney Disease. Nutrients 2017, 9, 282. [Google Scholar] [CrossRef] [PubMed]
- Obi, Y.; Mikami, S.; Hamano, T.; Obi, Y.; Tanaka, H.; Shimomura, A.; Rakugi, H.; Inoue, T.; Isaka, Y. Intravenous Vitamin B6 Increases Resistance to Erythropoiesis-Stimulating Agents in Hemodialysis Patients: A Randomized Controlled Trial. J. Ren. Nutr. Off. J. Counc. Ren. Nutr. Natl. Kidney Found. 2016, 26, 380–390. [Google Scholar] [CrossRef]
- Cappuccilli, M.; Bergamini, C.; Giacomelli, F.A.; Cianciolo, G.; Donati, G.; Conte, D.; Natali, T.; La Manna, G.; Capelli, I. Vitamin B Supplementation and Nutritional Intake of Methyl Donors in Patients with Chronic Kidney Disease: A Critical Review of the Impact on Epigenetic Machinery. Nutrients 2020, 12, 1234. [Google Scholar] [CrossRef] [PubMed]
- Nursalim, A.; Siregar, P.; Widyahening, I. Effect of folic acid, vitamin B6 and vitamin B12 supplementation on mortality and cardiovascular complication among patients with chronic kidney disease: An evidence-based case report. Acta Med. Indones. 2013, 45, 150–156. [Google Scholar]
- Takahashi, Y.; Tanaka, A.; Nakamura, T.; Fukuwatari, T.; Shibata, K.; Shimada, N.; Ebihara, I.; Koide, H. Nicotinamide suppresses hyperphosphatemia in hemodialysis patients. Kidney Int. 2004, 65, 1099–1104. [Google Scholar] [CrossRef]
- Edalat-Nejad, M.; Zameni, F.; Talaiei, A. The effect of niacin on serum phosphorus levels in dialysis patients. Indian J. Nephrol. 2012, 22, 174–178. [Google Scholar] [CrossRef]
- Selvam, M.; Sooraj, Y.S.; Gowthaman, S.; Ajeshkumar, R.N.P. Extended Release Nicotinic Acid—A Novel Oral Agent for Phosphate Control. Int. Urol. Nephrol. 2006, 38, 171–174. [Google Scholar] [CrossRef]
- Muller, D.; Mehling, H.; Otto, B.D.; Bergmann-Lips, R.; Luft, F.; Jordan, J.; Kettritz, R. Niacin Lowers Serum Phosphate and Increases HDL Cholesterol in Dialysis Patients. Clin. J. Am. Soc. Nephrol. 2007, 2, 1249–1254. [Google Scholar] [CrossRef]
- Restrepo Valencia, C.A.; Cruz, J. Safety and effectiveness of nicotinic acid in the management of patients with chronic renal disease and hyperlipidemia associated to hyperphosphatemia. Nefrologia 2008, 28, 61–66. [Google Scholar] [PubMed]
- Maccubbin, D.; Tipping, D.; Kuznetsova, O.; Hanlon, W.A.; Bostom, A.G. Hypophosphatemic Effect of Niacin in Patients without Renal Failure: A Randomized Trial. Clin. J. Am. Soc. Nephrol. 2010, 5, 582–589. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.; Lee, S. Niacin as a drug repositioning candidate for hyperphosphatemia management in dialysis patients. Ther. Clin. Risk Manag. 2014, 10, 875–883. [Google Scholar] [CrossRef] [PubMed]
- Edema, O.; Okoye, O.; Unuigbe, E.; Odonmeta, B.; Obodo, J. POS-255 niacin lowers serum phosphate levels in Nigerian chronic kidney disease patients. A randomized control trial. Kidney Int. Rep. 2021, 6, S107–S108. [Google Scholar] [CrossRef]
- Bukhari, F.J.; Moradi, H.; Gollapudi, P.; Ju Kim, H.; Vaziri, N.D.; Said, H.M. Effect of chronic kidney disease on the expression of thiamin and folic acid transporters. Nephrol. Dial. Transplant. 2011, 26, 2137–2144. [Google Scholar] [CrossRef]
- Frank, T.; Czeche, K.; Bitsch, R.; Stein, G. Assessment of thiamin status in chronic renal failure patients, transplant recipients and hemodialysis patients receiving a multivitamin supplementation. Int. J. Vitam. Nutr. Res. 2000, 70, 159–166. [Google Scholar] [CrossRef]
- Oguma, S.; Ando, I.; Hirose, T.; Totsune, K.; Sekino, H.; Sato, H.; Imai, Y.; Fujiwara, M. Biotin Ameliorates Muscle Cramps of Hemodialysis Patients: A Prospective Trial. Tohoku J. Exp. Med. 2012, 227, 217–223. [Google Scholar] [CrossRef]
- A Plasse, R.; Olson, S.W.; Yuan, C.M.; Nee, R. Biotin supplement interference with immunoassays for parathyroid hormone and 25-hydroxyvitamin D in a patient with metabolic bone disease on maintenance hemodialysis. Clin. Kidney J. 2020, 13, 710–712. [Google Scholar] [CrossRef]
- Szczuko, M.; Seidler, T.; Mierzwa, M.; Stachowska, E.; Chlubek, D. Effect of riboflavin supply on student body’s provision in north-western Poland with riboflavin measured by activity of glutathione reductase considering daily intake of other nutrients. Int. J. Food Sci. Nutr. 2011, 62, 431–438. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author, Year | Patient | Supplementation | Effect |
|---|---|---|---|
| Conner, 2012 [59] (prospective study) | N = 13 | Hemodialysis (HD) patients: 300 mg of vitamin C | Observed higher plasma concentrations of F2-isoprostanes, IL-1, IL-10, and TNF-α post-infusion |
| Sedighi, 2013 [61] (RCT study) | N = 40 | 300 mg of vitamin C post-dialysis, twice a week for 5 consecutive weeks, with a follow-up period of 12 weeks | Equal efficacy for intravenous iron and intravenous vitamin C for treatment of anemic HD patients with serum ferritin ≥500 mg/mL and TSAT ≤ 25% |
| Biniaz, 2014 [57] (retrospective studies) | N = 151 | Intervention: 250 mg of vitamin C after hemodialysis session 3 times a week for 8 weeks | After 2 months, median CRP reduced significantly in the vitamin C group to 10.7 (p = 0.04) vs. 22.6, and 30.6 mg/L in control groups |
| Garneata, 2015 [3] (RCT study) | N = 69 | Hemodialysis patients: ascorbic acid (300 mg 3 times/week) for 12 months intravenously | Ascorbic acid increased the amount of iron available for erythropoiesis and improved the correction of anemia |
| Rafie, 2016 [68] (RCT study) | N = 45 | HD patients: 250 mg of vitamin C daily for 8 weeks | Ascorbic acid was shown to be an effective and safe supplementation for the treatment of RLS in hemodialytic patients The treatment was not accompanied with serious adverse effects in short-term follow-up |
| Sultana, 2016 [65] (prospective study) | N = 15 | HD patients: 250 mg oral vitamin C daily for 3 months | Low-dose oral ascorbic acid was efficient in reducing erythropoietin dose requirements and improving anemia in functional iron deficient patients, without requiring additional iron administration |
| Ali, 2021 [58] (RCT study) | N = 31 | Treatment of erythropoietin-stimulating agents (ESAs), together with the oral supplementation of 500 mg of ascorbic acid every other day for 3 months in addition to iron therapy | Study group: reduction in both hepcidin and hs-CRP levels; reduction in serum iron and ferritin levels (p < 0.05); correlation between serum hepcidin and hs-CRP (R = 0.46, p <0.01) |
| Author, Year | Patient | Supplementation | Effect |
|---|---|---|---|
| Qin, 2013 [79] (meta-analysis, multicenter studies) | N = 8234 | Folic acid supplementation; B12 and folic acid supplementation; B6 and folic acid supplementation | Folic acid therapy reduced the risk of CVD in patients with kidney disease by 10%. Folic acid alone vs. folic acid with vitamin B6 and B12 did not significantly affect the effect of folic acid therapy. |
| Rafeq, 2013 [54] (RCT study) | N = 220 | Post hoc analysis HOST * | High-dose B vitamin therapy may be harmful in patients with CKD. |
| Xu, 2016 [83] (RCT, multicenter studies) | N = 7545 | 0.8 mg of folic acid; follow-up for an average of 4.5 years | Enalapril–folic acid therapy significantly slowed down the progression of CKD in patients with hypertension (compared to enalapril alone). |
| Achour, 2016 [72] (RCT study) | N = 132 | Cyanocobalamin (ampoule 1 mL/intramuscular injection of siphat) and folicum (folic acid, 5 mg/tablet) for 6 months | Supplementation with B vitamins (B9 and B12) correlated to the MTHFR genotypes was shown to significantly lower tHcy in HD patients regardless of MTHFR 677 genotype. Flushed out of the body after 2 months. |
| Li, 2017 [76] (RCT, multicenter Studies) | N = 20,702 | 10 mg enalapril or 10 mg enalapril and 8 mg folic acid (median treatment duration of 4.5 years) | Folic acid supplementation significantly reduced the risk of all-cause mortality in patients with heavy proteinuria, but not in those with absent or mild proteinuria. |
| Li, 2020 [80] (RCT, multicenter studies) | N = 1374 | 10 mg of enalapril or 10 mg of enalapril and 0.8 mg of cobalamin (median treatment duration of 4.4 years) | Folic acid treatment was associated with a greater reduction in the odds of CKD progression among patients with mild-to-moderate CKD and higher B12 levels. |
| Lu, 2021 [81] (RCT study) | N= 25 | Thiamin 90 mg/day combined with folic acid 30 mg/day for 96 weeks | Hemodialysis patients with cognitive impairment treated with thiamin and folic acid had a significant improvement on the MoCA score. |
| Lydia, 2021 [82] (cross-sectional study) | N = 80 | B12 and folic acid supplementation; no data (medical history) | There is a significant negative correlation between vitamin B12 and folic acid with homocysteine levels, especially in the high-risk cardiovascular group. |
| Yan, 2021 [78] (retrospective multicenter study) | N = 2142 | Levels of folic acid analyzed in the plasma | Reference range of folic acid in plasma was 14.7–19.1 ng/mL, with the best survival outcome in patients with CKD. |
| Nahas, 2022 [84] (prospective study) | N = 110 | B12 supplementation (1 mg once weekly for the next 4 weeks and 1 mg at the end of the second month) | Vitamin B12 deficiency should be addressed in ESRD patients receiving HD, while vitamin B12 supplementation may provide promising positive outcomes in the management of renal anemia among this population. |
| Author, Year | Patient | Supplementation | Effect |
|---|---|---|---|
| Takahashi, 2004 [89] (prospective study) | N = 65 | 500 mg of niacinamide for 12 weeks | Serum phosphorus decreased from 6.9 ± 1.5 to 5.4 ± 1.3 mg/dL. HDL increased from 47.4 +/− 14.9 to 67.2 +/− 22.3 mg/dL. LDL concentration decreased from 78.9 +/− 18.8 to 70.1 +/− 25.3 mg/dL. |
| Sampathkumar, 2006 [91] (prospective study) | N = 34 | 375 mg of nicotinic acid for 8 weeks | Serum phosphorus decreased from 7.7 ± 1.5 to 5.6 ±1.1 mg/dL. Calcium increased from 8.1 ± 1.0 to 8.5 ± 1.0 mg/dL. Serum alkaline phosphatase decreased from 107 ± 66 IU/L to 82 ± 46 IU/L. |
| Muller, 2007 [72] (prospective study) | N = 17 | 375 mg/dL to 2000 mg/dL of nicotinic acid (Niaspan), showing a systematic change every 2 weeks for 12 weeks | Serum phosphorus decreased from 7.2 +/− 0.5 to 5,9 +/− 0.6 mg/dl. HDL increased from 40 +/− 3.2 to 59 +/− 5.5 mg/dL. No effect on serum calcium levels. |
| Restrepo Valencia, 2008 [93] (observational study) | N = 9 | 500 mg of nicotinic acid for 3 months and 1000 mg for 5 months | Serum phosphorus decreased from 6.46 ± 0.53 to 3.94 ± 0.76 mg/dL. HDL increased, but there were no changes in LDL, PTH, hemoglobin, platelet count, AST, ALT and bilirubin, clotting tests (TTP and TP), uric acid, glycemia, albumin, creatinine, BUN, ferritin, folic acid, or vitamin B12. |
| Maccubbin, 2010 [94] (RCT study) | N = 1547 | 1 g/d of inhibitor laropiprant for 4 weeks and dose advanced to 2 g/d for 20 weeks combined with the selective prostaglandin D2 receptor subtype 1 | A sustained 0.13 mmol/L (0.4 mg/dL) reduction in serum phosphorus concentrations, approximately 10% from baseline, which was unaffected by estimated GFR levels ranging from 30 to > or =90 mL/min per 1.73 m(2). |
| Edalat-Nejad, 2012 [90] (RCT study) | N = 37 | 400 mg of niacin for 2 weeks, 600 mg for 2 weeks, 800 mg for 2 weeks, and 1000 mg for 2 weeks (8 weeks in total) | Serum phosphorus decreased from 6.66 ± 1.40 to 5.96 ± 0.87 mg/dL. HDL cholesterol increased from 35.3 ± 7.26 to 40.6 ± 10.1 mg/dL. |
| Edema, 2021 [96] (RCT study) | N = 89 | 500 mg of niacin for 4 weeks and 1000 mg for 4 weeks | Niacin reduced serum phosphate levels and calcium phosphate levels and also increased HDL levels in CKD stages 3–5 patients. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kędzierska-Kapuza, K.; Szczuko, U.; Stolińska, H.; Bakaloudi, D.R.; Wierzba, W.; Szczuko, M. Demand for Water-Soluble Vitamins in a Group of Patients with CKD versus Interventions and Supplementation—A Systematic Review. Nutrients 2023, 15, 860. https://doi.org/10.3390/nu15040860
Kędzierska-Kapuza K, Szczuko U, Stolińska H, Bakaloudi DR, Wierzba W, Szczuko M. Demand for Water-Soluble Vitamins in a Group of Patients with CKD versus Interventions and Supplementation—A Systematic Review. Nutrients. 2023; 15(4):860. https://doi.org/10.3390/nu15040860
Chicago/Turabian StyleKędzierska-Kapuza, Karolina, Urszula Szczuko, Hanna Stolińska, Dimitra Rafailia Bakaloudi, Waldemar Wierzba, and Małgorzata Szczuko. 2023. "Demand for Water-Soluble Vitamins in a Group of Patients with CKD versus Interventions and Supplementation—A Systematic Review" Nutrients 15, no. 4: 860. https://doi.org/10.3390/nu15040860