
A Systematic Review of Clinical Psychophysiology of Obsessive–Compulsive Disorders: Does the Obsession with Diet Also Alter the Autonomic Imbalance of Orthorexic Patients?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source/Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
3. Results
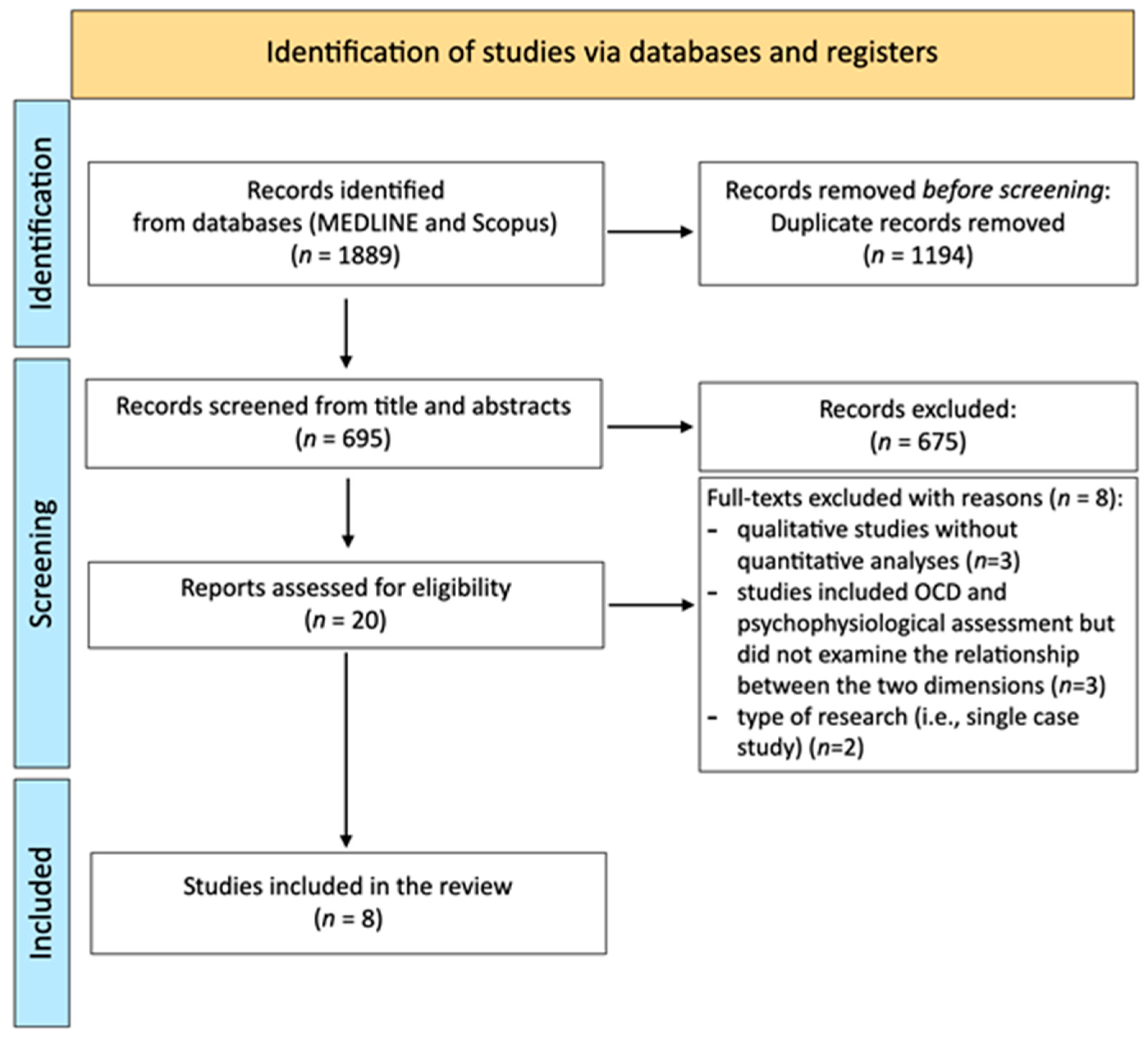
3.1. Search Results
3.2. Characteristics of Included Studies
3.3. Results for Obsessive–Compulsive Disorder
4. Discussion
4.1. Study Limitations
4.2. Directions for Future Research
4.3. Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Bratman, S. Health Food Junkie. Yoga (September/October). Available online: http://www.beyondveg.com/bratman-s/hfj/hf-junkie-1a.shtml (accessed on 18 November 2022).
- Niedzielski, A.; Kaźmierczak-Wojtaś, N. Prevalence of Orthorexia Nervosa and Its Diagnostic Tools-A Literature Review. Int. J. Environ. Res. Public Health 2021, 18, 5488. [Google Scholar] [CrossRef]
- Decyk, A.; Księżopolska, M. Orthorexia nervosa—The border between healthy eating and eating disorders. Rocz. Panstw. Zakl. Hig. 2022, 73, 381–385. [Google Scholar] [CrossRef]
- Barthels, F.; Barrada, J.R.; Roncero, M. Orthorexia nervosa and healthy orthorexia as new eating styles. PLoS ONE 2019, 14, e0219609. [Google Scholar] [CrossRef] [PubMed]
- Cena, H.; Barthels, F.; Cuzzolaro, M.; Bratman, S.; Brytek-Matera, A.; Dunn, T.; Varga, M.; Missbach, B.; Donini, L.M. Definition and diagnostic criteria for orthorexia nervosa: A narrative review of the literature. Eat Weight Disord. 2019, 24, 209–246. [Google Scholar] [CrossRef] [PubMed]
- Dunn, T.M.; Bratman, S. On orthorexia nervosa: A review of the literature and proposed diagnostic criteria. Eat Behav. 2016, 21, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Gortat, M.; Samardakiewicz, M.; Perzyński, A. Orthorexia nervosa—A distorted approach to healthy eating. Ortoreksja—Wypaczone podejście do zdrowego odżywiania się. Psychiatr. Pol. 2021, 55, 421–433. [Google Scholar] [CrossRef]
- Brytek-Matera, A. Orthorexia nervosa—An eating disorder, obsessive-compulsive disorder or disturbed eating habit? Arch. Psychiatry Psychother. 2012, 14, 55–60. [Google Scholar]
- Atchison, A.E.; Zickgraf, H.F. Orthorexia nervosa and eating disorder behaviors: A systematic review of the literature. Appetite 2022, 177, 106134. [Google Scholar] [CrossRef]
- Pontillo, M.; Zanna, V.; Demaria, F.; Averna, R.; Di Vincenzo, C.; De Biase, M.; Di Luzio, M.; Foti, B.; Tata, M.C.; Vicari, S. Orthorexia Nervosa, Eating Disorders, and Obsessive-Compulsive Disorder: A Selective Review of the Last Seven Years. J. Clin. Med. 2022, 11, 6134. [Google Scholar] [CrossRef]
- Barthels, F.; Horn, S.; Pietrowsky, R. Orthorexic eating behaviour, illness anxiety and dysfunctional cognitions characteristic of somatic symptom disorders in a non-clinical sample. Eat Weight Disord. 2021, 26, 2387–2391. [Google Scholar] [CrossRef]
- Anastasiades, E.; Argyrides, M. Healthy orthorexia vs orthorexia nervosa: Associations with body appreciation, functionality appreciation, intuitive eating and embodiment. Eat. Weight. Disord. EWD 2022, 27, 3197–3206. [Google Scholar] [CrossRef] [PubMed]
- Kalra, S.; Kapoor, N.; Jacob, J. Orthorexia nervosa. JPMA J. Pak. Med. Assoc. 2020, 70, 1282–1284. [Google Scholar] [PubMed]
- Bratman, S.; Knight, D. Health Food Junkies: Overcoming the Obsession with Healthful Eating; Broadway Books: New York, NY, USA, 2000. [Google Scholar]
- Barthels, F.; Müller, R.; Schüth, T.; Friederich, H.C.; Pietrowsky, R. Orthorexic eating behavior in patients with somatoform disorders. Eat Weight Disord. 2021, 26, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Roncero, M.; Barrada, J.R.; García-Soriano, G.; Guillén, V. Personality Profile in Orthorexia Nervosa and Healthy Orthorexia. Front. Psychol. 2021, 12, 710604. [Google Scholar] [CrossRef]
- McComb, S.E.; Mills, J.S. Orthorexia nervosa: A review of psychosocial risk factors. Appetite 2019, 140, 50–75. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Robbins, T.W.; Gillan, C.M.; Smith, D.G.; de Wit, S.; Ersche, K.D. Neurocognitive endophenotypes of impulsivity and compulsivity: Towards dimensional psychiatry. Trends Cogn. Sci. 2012, 16, 81–91. [Google Scholar] [CrossRef]
- Milad, M.R.; Rauch, S.L. Obsessive-compulsive disorder: Beyond segregated cortico-striatal pathways. Trends Cogn. Sci. 2012, 16, 43–51. [Google Scholar] [CrossRef]
- Thayer, J.F.; Hansen, A.L.; Saus-Rose, E.; Johnsen, B.H. Heart Rate Variability, Prefrontal Neural Function, and Cognitive Performance: The Neurovisceral Integration Perspective on Self-Regulation, Adaptation, and Health. Ann. Behav. Med. 2009, 37, 141–153. [Google Scholar] [CrossRef]
- Shaffer, F.; McCraty, R.; Zerr, C.L. A healthy heart is not a metronome: An integrative review of the heart’s anatomy and heart rate variability. Front. Psychol. 2014, 5, 1040. [Google Scholar] [CrossRef]
- Remijnse, P.L.; Nielen, M.M.; van Balkom, A.J.; Cath, D.C.; van Oppen, P.; Uylings, H.B.; Veltman, D.J. Reduced orbitofrontal-striatal activity on a reversal learning task in obsessive-compulsive disorder. Arch. Gen. Psychiatry 2006, 63, 1225–1236. [Google Scholar] [CrossRef]
- Chamberlain, S.R.; Fineberg, N.A.; Menzies, L.A.; Blackwell, A.D.; Bullmore, E.T.; Robbins, T.W.; Sahakian, B.J. Impaired cognitive flexibility and motor inhibition in unaffected first-degree relatives of patients with obsessive-compulsive disorder. Am. J. Psychiatry 2007, 164, 335–338. [Google Scholar] [CrossRef]
- Chamberlain, S.R.; Menzies, L.; Hampshire, A.; Suckling, J.; Fineberg, N.A.; del Campo, N.; Aitken, M.; Craig, K.; Owen, A.M.; Bullmore, E.T.; et al. Orbitofrontal dysfunction in patients with obsessive-compulsive disorder and their unaffected relatives. Science 2008, 321, 421–422. [Google Scholar] [CrossRef] [PubMed]
- Gu, B.M.; Park, J.Y.; Kang, D.H.; Lee, S.J.; Yoo, S.Y.; Jo, H.J.; Choi, C.H.; Lee, J.M.; Kwon, J.S. Neural correlates of cognitive inflexibility during task-switching in obsessive-compulsive disorder. Brain J. Neurol. 2008, 131, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Viswanath, B.; Janardhan Reddy, Y.C.; Kumar, K.J.; Kandavel, T.; Chandrashekar, C.R. Cognitive endophenotypes in OCD: A study of unaffected siblings of probands with familial OCD. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2009, 33, 610–615. [Google Scholar] [CrossRef] [PubMed]
- Remijnse, P.L.; van den Heuvel, O.A.; Nielen, M.M.; Vriend, C.; Hendriks, G.J.; Hoogendijk, W.J.; Uylings, H.B.; Veltman, D.J. Cognitive inflexibility in obsessive-compulsive disorder and major depression is associated with distinct neural correlates. PLoS ONE 2013, 8, e59600. [Google Scholar] [CrossRef]
- Gruner, P.; Pittenger, C. Cognitive inflexibility in Obsessive-Compulsive Disorder. Neuroscience 2017, 345, 243–255. [Google Scholar] [CrossRef]
- Graybiel, A.M. Habits, rituals, and the evaluative brain. Annu. Rev. Neurosci. 2008, 31, 359–387. [Google Scholar] [CrossRef]
- Simon, D.; Kaufmann, C.; Kniesche, R.; Kischkel, E.; Kathmann, N. Autonomic responses and neural-cardiac coupling during individually tailored symptom provocation in obsessive-compulsive disorder. J. Anxiety Disord. 2013, 27, 635–644. [Google Scholar] [CrossRef]
- Simon, D.; Kaufmann, C.; Musch, K.; Kischkel, E.; Kathmann, N. Fronto-striato-limbic hyperactivation in obsessive-compulsive disorder during individually tailored symptom provocation. Psychophysiology 2010, 47, 728–738. [Google Scholar] [CrossRef]
- Admon, R.; Bleich-Cohen, M.; Weizmant, R.; Poyurovsky, M.; Faragian, S.; Hendler, T. Functional and structural neural indices of risk aversion in obsessive-compulsive disorder (OCD). Psychiatry Res. 2012, 203, 207–213. [Google Scholar] [CrossRef]
- Stern, E.R.; Welsh, R.C.; Gonzalez, R.; Fitzgerald, K.D.; Abelson, J.L.; Taylor, S.F. Subjective uncertainty and limbic hyperactivation in obsessive-compulsive disorder. Hum. Brain Mapp. 2012, 34, 1956–1970. [Google Scholar] [CrossRef] [Green Version]
- Banca, P.; Voon, V.; Vestergaard, M.D.; Philipiak, G.; Almeida, I.; Pocinho, F.; Relvas, J.; Castelo-Branco, M. Imbalance in habitual versus goal directed neural systems during symptom provocation in obsessive-compulsive disorder. Brain 2015, 138 Pt 3, 798–811. [Google Scholar] [CrossRef]
- Thayer, J.F.; Lane, R.D. A model of neurovisceral integration in emotion regulation and dysregulation. J. Affect. Disord. 2000, 61, 201–216. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.L.; Johnsen, B.H.; Sollers, J.J., 3rd; Stenvik, K.; Thayer, J.F. Heart Rate Variability and its Relation to Prefrontal Cognitive Function: The Effects of Training and Detraining. Eur. J. Appl. Physiol. 2004, 93, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.N. Autonomic interactions in cardiac control. Ann. N. Y. Acad. Sci. 1990, 601, 209–221. [Google Scholar] [CrossRef] [PubMed]
- Uijtdehaage, S.H.J.; Thayer, J.F. Accentuated antagonism in the control of human heart rate. Clin. Auton. Res. 2000, 10, 107–110. [Google Scholar] [CrossRef]
- Ahern, G.L.; Sollers, J.J.; Lane, R.D.; Labiner, D.M.; Herring, A.M.; Weinand, M.E.; Hutzler, R.; Thayer, J.F. Heart rate and heart rate variability changes in the intracarotid sodium amobarbital test. Epilepsia 2001, 42, 912–921. [Google Scholar] [CrossRef]
- Ter Horst, G.J. Central autonomic control of the heart, angina, and pathogenic mechanisms of post-myocardial infarction depression. Eur. J. Morphol. 1999, 37, 257–266. [Google Scholar] [CrossRef]
- Thayer, J.F.; Lane, R.D. Claude Bernard and the heart-brain connection: Further elaboration of a model of neurovisceral integration. Neurosci. Biobehav. Rev. 2009, 33, 81–88. [Google Scholar] [CrossRef]
- Hansen, A.L.; Johnsen, B.H.; Thayer, J.F. Vagal influence on working memory and attention. Int. J. Psychophysiol. 2003, 48, 263–274. [Google Scholar] [CrossRef]
- Johnsen, B.H.; Thayer, J.F.; Laberg, J.C.; Wormnes, B.; Raadal, M.; Skaret, E.; Kvale, G.; Berg, E. Attentional and physiological characteristics of patients with dental anxiety. J. Anxiety Disord. 2003, 17, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Krypotos, A.-M.; Jahfari, S.; van Ast, V.A.; Kindt, M.; Forstmann, B.U. Individual differences in heart rate variability predict the degree of slowing during response inhibition and initiation in the presence of emotional stimuli. Front. Psychol. 2011, 2, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Brosschot, J.F. Psychosomatics and psychopathology: Looking up and down from the brain. Psychoneuroendocrinology 2005, 30, 1050–1058. [Google Scholar] [CrossRef]
- Appelhans, B.M.; Luecken, L.J. Heart rate variability as an index of regulated emotional responding. Rev. Gen. Psychol. 2006, 10, 229240. [Google Scholar] [CrossRef]
- Li, Z.; Snieder, H.; Su, S.; Ding, X.; Thayer, J.F.; Treiber, F.A.; Wang, X. A longitudinal study in youth of heart rate vari- ability at rest and in response to stress. Int. J. Psychophysiol. 2009, 73, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Ingjaldsson, J.T.; Laberg, J.C.; Thayer, J.F. Reduced heart rate variability in chronic alcohol abuse: Relationship with negative mood, chronic thought suppression, and compulsive drinking. Biol. Psychiatry 2003, 54, 1427–1436. [Google Scholar] [CrossRef]
- Aldao, A.; Nolen-Hoeksema, S.; Schweizer, S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clin. Psychol. Rev. 2010, 30, 217–237. [Google Scholar] [CrossRef]
- Gillie, B.L.; Vasey, M.W.; Thayer, J.F. Individual differences in resting heart rate variability moderate thought suppression success. Psychophysiology 2015, 52, 1149–1160. [Google Scholar] [CrossRef]
- Rachman, S.; Silva, P.D.E. Abnormal and normal obsessions. Behav. Res. Ther. 1977, 16, 233–248. [Google Scholar] [CrossRef]
- Wegner, D.M.; Schneider, D.J.; Carter, S.R.; White, T.L. Paradoxical effects of thought suppression. J. Personal. Soc. Psychol. 1987, 53, 5–13. [Google Scholar] [CrossRef]
- Wenzlaff, R.M.; Wegner, D.M. Thought suppression. Annu. Rev. Psychol. 2000, 51, 59–91. [Google Scholar] [CrossRef]
- Brewin, C.R.; Smart, L. Working memory capacity and suppression of intrusive thoughts. J. Behav. Ther. Exp. Psychiatry 2005, 36, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Ólafsson, R.P.; Emmelkamp, P.M.; Gunnarsdóttir, E.R.; Snæbjörnsson, T.; Ólason, D.T.; Kristjánsson, Á. Suppressing disgust related thoughts and performance on a subsequent behavioural avoidance task: Implications for OCD. Behav. Res. Ther. 2013, 51, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Wegner, D.M. Ironic processes of mental control. Psychol. Rev. 1994, 101, 34–52. [Google Scholar] [CrossRef] [PubMed]
- Hovland, A.; Pallesen, S.; Hammar, A.; Hansen, A.L.; Thayer, J.F.; Tarvainen, M.P.; Nordhus, I.H. The relationships among heart rate variability, executive functions, and clinical variables in patients with panic disorder. Int. J. Psychophysiol. 2012, 86, 269–275. [Google Scholar] [CrossRef]
- Thayer, J.F.; Sollers, J.J.; Ruiz-Padial, E.; Vila, J. Estimating respiratory frequency from autoregressive spectral analysis of heart period. IEEE Eng. Med. Biol. 2002, 21, 41–45. [Google Scholar] [CrossRef]
- Olbrich, S.; Olbrich, H.; Jahn, I.; Sander, C.; Adamaszek, M.; Hegerl, U.; Reque, F.; Stengler, K. EEG-vigilance regulation during the resting state in obsessive-compulsive disorder. Clin. Neurophysiol. 2013, 124, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Olbrich, H.; Jahn, I.; Stengler, K.; Seifritz, E.; Colla, M. Heart rate variability in obsessive compulsive disorder in comparison to healthy controls and as predictor of treatment response. Clin. Neurophysiol. 2022, 138, 123–131. [Google Scholar] [CrossRef]
- Beauchaine, T.P.; Thayer, J.F. Heart rate variability as a transdiagnostic biomarker of psychopathology. Int. J. Psychophysiol. 2015, 98, 338–350. [Google Scholar] [CrossRef]
- Slaap, B.R.; Nielen, M.M.; Boshuisen, M.L.; van Roon, A.M.; den Boer, J.A. Five-minute recordings of heart rate variability in obsessive-compulsive disorder, panic disorder and healthy volunteers. J. Affect. Disord. 2004, 78, 141–148. [Google Scholar] [CrossRef]
- Havnen, A.; Hovland, A.; Haug, E.T.; Hansen, B.; Kvale, G. Sleep and heart rate variability in patients with obsessive-compulsive disorder: Preliminary findings. Clin. Neuropsychiatry J. Treat. Eval. 2013, 10 (Suppl 1), 56–60. [Google Scholar]
- Milad, M.R.; Furtak, S.C.; Greenberg, J.L.; Keshaviah, A.; Im, J.J.; Falkenstein, M.J.; Jenike, M.; Rauch, S.L.; Wilhelm, S. Deficits in conditioned fear extinction in obsessive-compulsive disorder and neurobiological changes in the fear circuit. JAMA Psychiatry 2013, 70, 608–618, quiz 554. [Google Scholar] [CrossRef] [PubMed]
- Pruneti, C.; Saccò, M.; Cosentino, C.; Sgromo, D. Relevance of Autonomic Arousal in the Stress Response in Psychopathology”. J. Basic Appl. Sci. 2016, 12, 176–184. [Google Scholar] [CrossRef]
- Pruneti, C.; Cosentino, C.; Sgromo, D.; Innocenti, A. Skin Conductance Response as A Decisive Variable In Individuals With A DSM-IV TR Axis I Diagnosis. JMED Res. 2014, 2014, 565009. [Google Scholar] [CrossRef]
- Pittig, A.; Arch, J.J.; Lam, C.W.; Craske, M.G. Heart rate and heart rate variability in panic, social anxiety, obsessive-compulsive, and generalized anxiety disorders at baseline and in response to relaxation and hyperventilation. Int. J. Psychophysiol. 2013, 87, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Pöhlchen, D.; Priouret, M.; Kraft, M.S.; Binder, F.P.; Gürsel, D.A.; Berberich, G.; BeCOME Working Group; Koch, K.; Spoormaker, V.I. Examining Differences in Fear Learning in Patients With Obsessive-Compulsive Disorder With Pupillometry, Startle Electromyography and Skin Conductance Responses. Front. Psychiatry 2021, 12, 730742. [Google Scholar] [CrossRef]
- Whitton, A.E.; Henry, J.D.; Grisham, J.R. Cognitive and psychophysiological correlates of disgust in obsessive-compulsive disorder. Br. J. Clin. Psychol. 2015, 54, 16–33. [Google Scholar] [CrossRef]
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J.B.W. Structured Clinical Interview for DSM-IV Axis I Disorders-Patient Edition (SCID-I/P, Version 2.0); New York State Psychiatric Institute, Biometric Research Department: New York, NY, USA, 1995. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Zahn, T.P.; Leonard, H.L.; Swedo, S.E.; Rapaport, J.L. Autonomic activity in children and adolescents with obsessive- compulsive disorder. Psychiatry Res. 1996, 60, 67–76. [Google Scholar] [CrossRef]
- Lelliott, P.T.; Noshirvani, H.F.; Marks, I.M.; Monteiro, W.O.; Basoglu, M.; Cohen, S.D. Relationship of skin conductance activity to clinical features in obsessive-compulsive ritualizers. Psychol. Med. 1987, 17, 905–914. [Google Scholar] [CrossRef]
- Hoehn-Saric, R.; McLeod, D.R.; Hipsley, P. Is hyperarousal essential to obsessive- compulsive disorder?: Diminished physiologic flexibility, but not hyperarousal, characterizes patients with obsessive-compulsive disorder. Arch. Gen. Psychiatry 1995, 52, 688–693. [Google Scholar] [CrossRef]
- Pruneti, C.; Lento, R.M.; Fante, C.; Carrozzo, E.; Fontana, F. Autonomic Arousal and Differential Diagnosis in Clinical Psychology and Psychopathology. Ital. J. Psychopathol. 2010, 16, 43–52. [Google Scholar]
- Pruneti, C.; Guidotti, S.; Lento, R.M.; Renda, N. Dissociation between cognitive-behavioral and emotional-psycho- physiological aspects in Eating Disorders and its pre-post treatment stability. J. Psychopathol. 2022, 28, 30–38. [Google Scholar] [CrossRef]
- Sanislow, C.A.; Pine, D.S.; Quinn, K.J.; Kozak, M.J.; Garvey, M.A.; Heinssen, R.K.; Wang, P.S.; Cuthbert, B.N. Developing constructs for psychopathology research: Research domain criteria. J. Abnorm. Psychol. 2010, 119, 631–639. [Google Scholar] [CrossRef] [Green Version]
- Pribram, K.H.; McGuinness, D. Arousal, activation, and effort in the control of attention. Psychol. Rev. 1975, 82, 116–149. [Google Scholar] [CrossRef] [PubMed]
- Palomba, D.; Sarlo, M.; Angrilli, A.; Mini, A.; Stegagno, L. Cardiac responses associated with affective processing of unpleasant film stimuli. Int. J. Psychophysiol. Off. J. Int. Organ. Psychophysiol. 2000, 36, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Pruneti, C.; Vanello, N.; Paterni, M.; Landini, L.; Guidotti, S.; Ferdeghini, E.M. Combined functional magnetic resonance imaging and skin conductance to detect localized neural response to psychological stress: A pilot study. Arch. Ital. de Biol. 2021, 159, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Rozenman, M.; Piacentini, J.; O’Neill, J.; Bergman, R.L.; Chang, S.; Peris, T.S. Improvement in anxiety and depression symptoms following cognitive behavior therapy for pediatric obsessive compulsive disorder. Psychiatry Res. 2019, 276, 115–123. [Google Scholar] [CrossRef]
- Reid, J.E.; Laws, K.R.; Drummond, L.; Vismara, M.; Grancini, B.; Mpavaenda, D.; Fineberg, N.A. Cognitive behavioural therapy with exposure and response prevention in the treatment of obsessive-compulsive disorder: A systematic review and meta-analysis of randomised controlled trials. Compr. Psychiatry 2021, 106, 152223. [Google Scholar] [CrossRef] [PubMed]
- Pujol, J.; Soriano-Mas, C.; Alonso, P.; Cardoner, N.; Menchón, J.M.; Deus, J.; Vallejo, J. Mapping structural brain alterations in obsessive-compulsive disorder. Arch. Gen. Psychiatry 2004, 61, 720–730. [Google Scholar] [CrossRef]
- Stengler, K.; Olbrich, S.; Heider, D.; Dietrich, S.; Riedel-Heller, S.; Jahn, I. Mental health treatment seeking among patients with OCD: Impact of age of onset. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 813–819. [Google Scholar] [CrossRef]
- De Vincenzo, F.; Cosentino, C.; Quinto, R.M.; Di Leo, S.; Contardi, A.; Guidotti, S.; Iani, L.; Pruneti, C. Psychological adjustment and heart rate variability in ovarian cancer survivors. Mediterr. J. Clin. Psychol. 2022, 10. [Google Scholar] [CrossRef]
- Pruneti, C.; Guidotti, S. Cognition, Behavior, Sexuality, and Autonomic Responses of Women with Hypothalamic Amenorrhea. Brain Sci. 2022, 12, 1448. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Sample | Study Design | Measures | Main Results |
|---|---|---|---|---|
| Havnen et al. [64] | n = 31 OCD patients | Cross-sectional | Psychopathological Assessment: SCID-I; Y-BOCS Neuropsychological Assessment: Stroop Test Physiological Assessment: HR and HRV | HF-HRV negatively correlates with Y-BOCS and Stroop test. |
| Olbrich et al. [61] | n = 51 OCD patients n = 28 HC | Case-control and Quasi-experimental | Psychopathological Assessment: GCI; Y-BOCS Physiological Assessment: HR and HRV | Significantly higher HR in the unmedicated OCD-sample in comparison to the HC. Moreover, HF-HRV Power differentiates responders to non-responders. |
| Pittig et al. [68] | n = 82 patients with PD, SAD, GAD, or OCD n = 39 HC | Case-control | Psychopathological Assessment: ADIS-IV; ASI; PSWQ; Padua Inventory-Revised; FQ-S Physiological Assessment: HR and HRV | Significantly higher HF-HRV (baseline) in HC compared with all the patients’ categories. No significant differences in HR (relaxation) change between all anxiety disorders. Significantly lower HF-HRV (hyperventilation phase) in all anxiety disorders compared with HCs. |
| Pruneti et al. [66] | n = 89 patients with PD, GAD, MDE, AN, or OCD n = 34 HC | Cross-sectional and Case-control | Psychopathological Assessment: MMPI-2; SQ; PSQ Physiological Assessment: sEMG, SCL/SCR, PT, HR and HRV | Significantly lower levels of HR in OCD patients compared with HC and GAD in all of the three phases of the PSP. Lower levels of SCR in OCDs along with MDE, AN, and HCs, compared with PD and GAD. OCDs, along GAD, PD, MDE, and AN, report significantly higher levels of sEMG compared with HCs. |
| Pruneti et al. [67] | n = 104 patients with GAD, MDE, PD, or OCD | Cross-sectional | Psychopathological Assessment: MMPI-2; SQ; PSQ Physiological Assessment: sEMG, SCL/SCR, PT, HR and HRV | Significant differences between OCD and anxious patients (GAD and PD) with regards to the SCR values in the three phases of the PSP. In addition, SCR values in OCD patients fall within the typical range in all of the phases of the PSP. Only a slight reactivity to stress is present but characterized by the inability to relax. |
| Whitton et al. [70] | n = 25 patients with OCD n = 21 patients non-OCD anxiety disorders n = 25 HC | Observational and Longitudinal | Psychopathological Assessment: ADIS-IV; OCI-R; DASS-21; OBQ-44; DPSS-R; DS-R Physiological Assessment: facial EMG and EDA | Greater disgust propensity and self-reported disgust to images of body waste in OCDs compared to HC and anxious participants. No group differences in physiological responses. After controlling for trait disgust, obsessive beliefs positively correlates with increased self-reported disgust to neutral images and increased levator labii activity to negative non-disgusting images. |
| Pöhlchen et al. [69] | n = 37 patients with OCD n = 26 HC | Case-control | Psychopathological Assessment: Y- BOCS, OCI-R, HAM-A, HAM-D Physiological Assessment: SCR and EMG | No group differences in SCR, pupillometry, or subjective ratings in extinction learning and extinction recall. Only subtle differences in startle responses during extinction (higher amplitudes in OCD patients). |
| Milad et al. [65] | n = 21 patients with OCD n = 21 HC | Cross-sectional, Case-control, and fMRI study | Psychopathological Assessment: SCID-IV; Y-BOCS Physiological Assessment: SCR Neural Assessment: fMRI BOLD signals | Impaired extinction recall in OCD patients. Regarding the fMRI data, patients with OCD showed significantly reduced activation in the vmPFC across training phases as well as in the caudate and hippocampus during fear conditioning, and in the cerebellum, posterior cingulate cortex, and putamen during extinction recall. In addition, the OCD symptom severity positively correlated with the magnitude of extinction memory recall and the functional responses of the vmPFC while they negatively correlated with the functional responses of the dorsal anterior cingulate cortex. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pruneti, C.; Coscioni, G.; Guidotti, S. A Systematic Review of Clinical Psychophysiology of Obsessive–Compulsive Disorders: Does the Obsession with Diet Also Alter the Autonomic Imbalance of Orthorexic Patients? Nutrients 2023, 15, 755. https://doi.org/10.3390/nu15030755
Pruneti C, Coscioni G, Guidotti S. A Systematic Review of Clinical Psychophysiology of Obsessive–Compulsive Disorders: Does the Obsession with Diet Also Alter the Autonomic Imbalance of Orthorexic Patients? Nutrients. 2023; 15(3):755. https://doi.org/10.3390/nu15030755
Chicago/Turabian StylePruneti, Carlo, Gabriella Coscioni, and Sara Guidotti. 2023. "A Systematic Review of Clinical Psychophysiology of Obsessive–Compulsive Disorders: Does the Obsession with Diet Also Alter the Autonomic Imbalance of Orthorexic Patients?" Nutrients 15, no. 3: 755. https://doi.org/10.3390/nu15030755