
Gastrointestinal Manifestations and Low-FODMAP Protocol in a Cohort of Fabry Disease Adult Patients

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Subject Characteristics
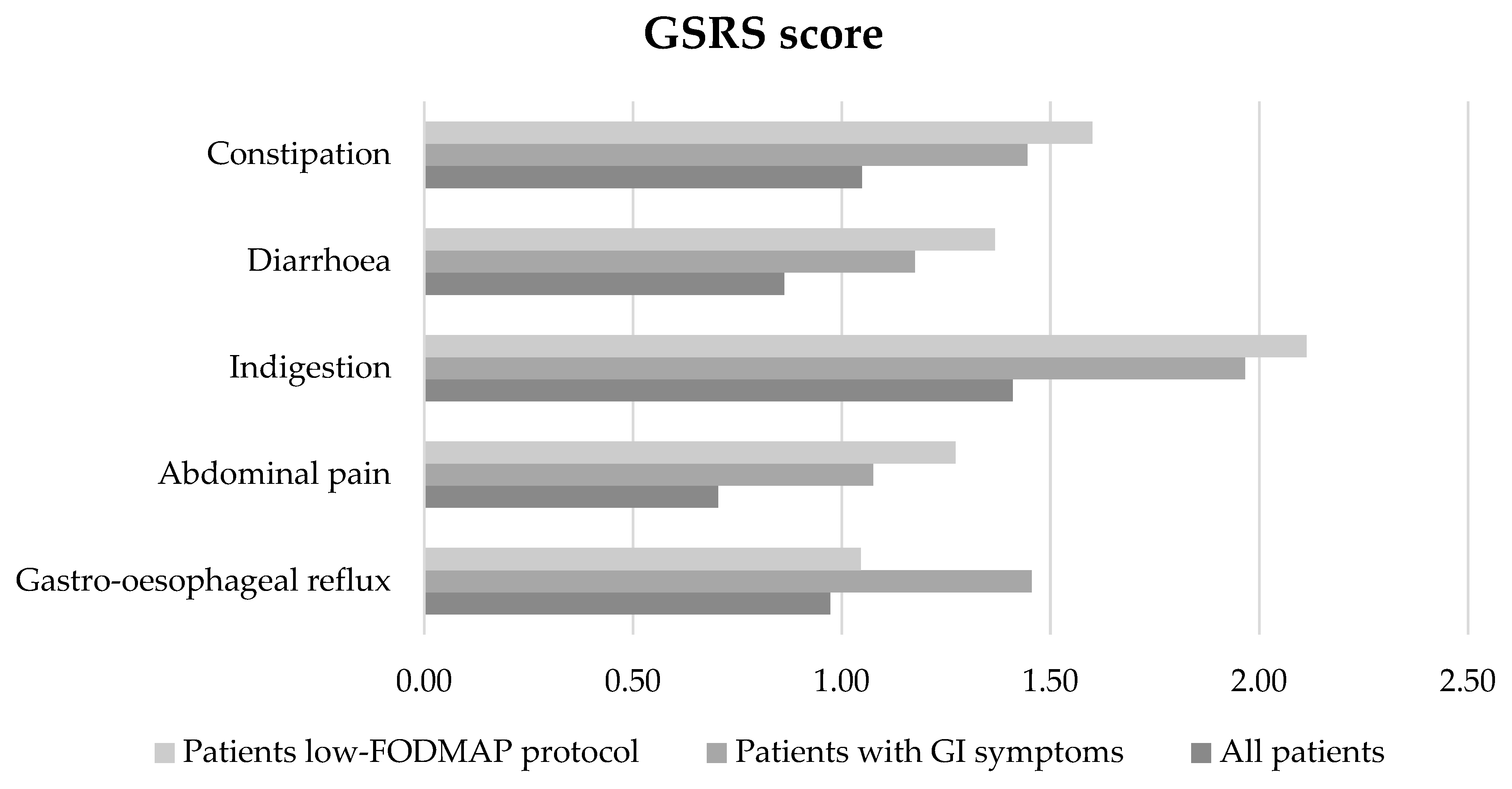
3.2. Gastrointestinal Manifestations
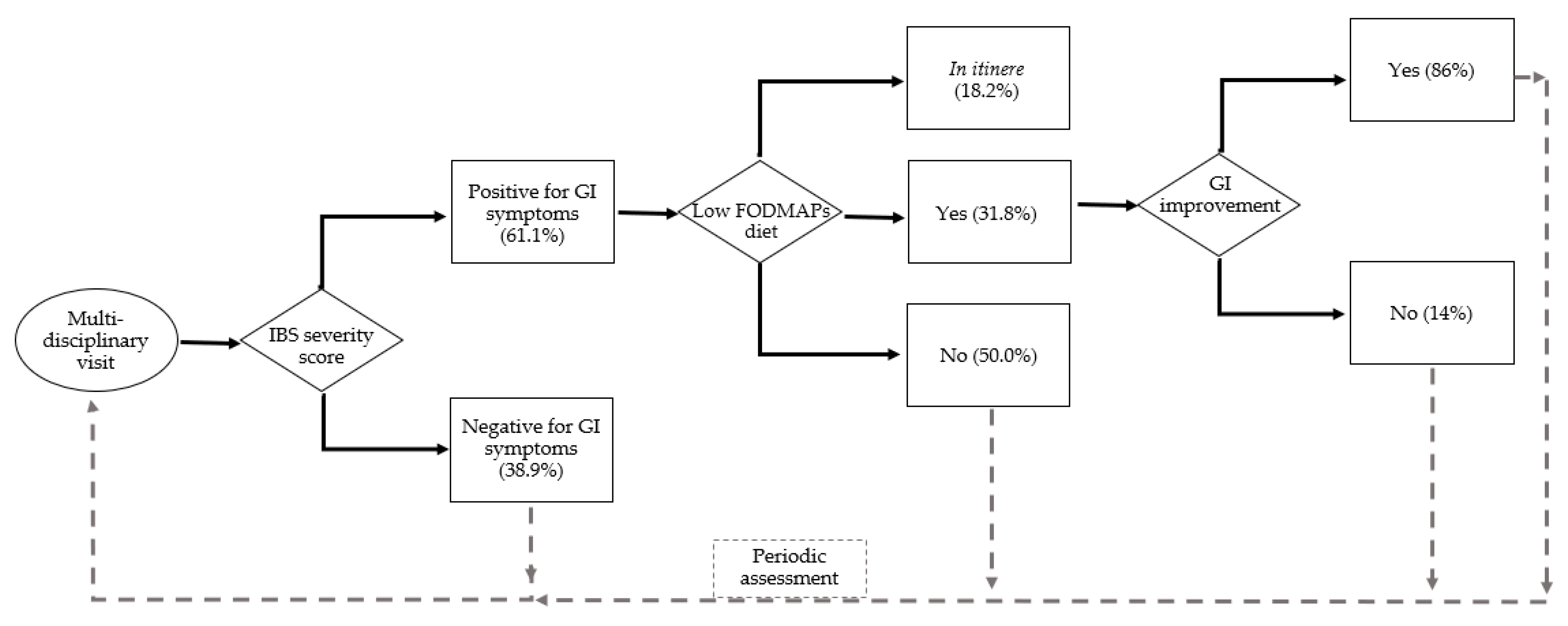
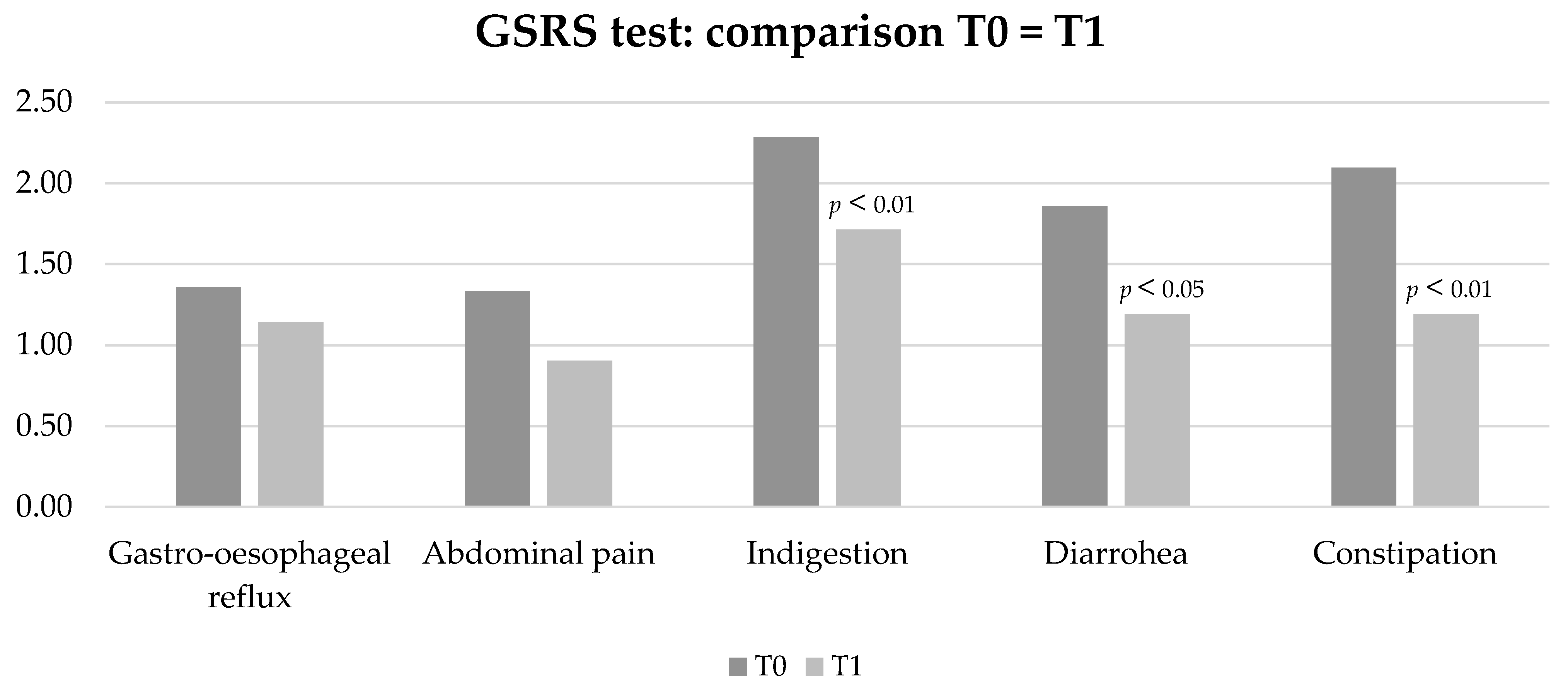
3.3. Low-FODMAP Diet
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Meikle, P.J.; Hopwood, J.J.; Clague, A.E.; Carey, W.F. Prevalence of lysosomal storage disorders. JAMA 1999, 281, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, P.V.; Klug, T.; Vermette, L.; Raburn-Miller, J.; Kiesling, J.; Rogers, S. Incidence of 4 Lysosomal Storage Disorders From 4 Years of Newborn Screening. JAMA Pediatr. 2018, 172, 696–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarate, Y.A.; Hopkin, R.J. Fabry’s disease. Lancet 2008, 372, 1427–1435. [Google Scholar] [CrossRef] [PubMed]
- El-Abassi, R.; Singhal, D.; England, J.D. Fabry’s disease. J. Neurol. Sci. 2014, 344, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Radulescu, D.; Crisan, D.; Militaru, V.; Buzdugan, E.; Stoicescu, L.; Grosu, A.; Vlad, C.; Grapa, C.; Radulescu, M.L. Gastrointestinal Manifestations and Treatment Options in Fabry Disease Patients. A Systematic Review. J. Gastrointestin. Liver Dis. 2022, 31, 98–106. [Google Scholar] [CrossRef]
- Mehta, A.; Clarke, J.T.R.; Giugliani, R.; Elliott, P.; Linhart, A.; Beck, M.; Sunder-Plassmann, G. Natural course of Fabry disease: Changing pattern of causes of death in FOS-Fabry Outcome Survey. J. Med. Genet. 2009, 46, 548–552. [Google Scholar] [CrossRef] [Green Version]
- Lenders, M.; Brand, E. Fabry disease–a multisystemic disease with gastrointestinal manifestations. Gut Microbes 2022, 14, 1–15. [Google Scholar] [CrossRef]
- Hoffmann, B.; Schwarz, M.; Mehta, A.; Keshav, S. Gastrointestinal symptoms in 342 patients with Fabry disease: Prevalence and response to enzyme replacement therapy. Clin. Gastroenterol. Hepatol. 2007, 5, 1447–1453. [Google Scholar] [CrossRef]
- Zar-Kessler, C.; Karaa, A.; Sims, K.B.; Clarke, V.; Kuo, B. Understanding the gastrointestinal manifestations of Fabry disease: Promoting prompt diagnosis. Therap. Adv. Gastroenterol. 2016, 9, 626–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spada, M.; Pagliardini, S.; Yasuda, M.; Tukel, T.; Thiagarajan, G.; Sakuraba, H.; Ponzone, A.; Desnick, R.J. High incidence of later-onset fabry disease revealed by newborn screening. Am. J. Hum. Genet. 2006, 79, 31–40. [Google Scholar] [CrossRef]
- Ortiz, A.; Germain, D.P.; Desnick, R.J.; Politei, J.; Mauer, M.; Burlina, A.; Eng, C.; Hopkin, R.J.; Laney, D.; Linhart, A.; et al. Fabry disease revisited: Management and treatment recommendations for adult patients. Mol. Genet. Metab. 2018, 123, 416–427. [Google Scholar] [CrossRef] [PubMed]
- Biegstraaten, M.; Arngrímsson, R.; Barbey, F.; Boks, L.; Cecchi, F.; Deegan, P.B.; Feldt-Rasmussen, U.; Geberhiwot, T.; Germain, D.P.; Hendriksz, C.; et al. Recommendations for initiation and cessation of enzyme replacement therapy in patients with Fabry disease: The European Fabry Working Group consensus document. Orphanet J. Rare Dis. 2015, 10, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friis, H.; Bodé, S.; Rumessen, J.J.; Gudmand-Høyer, E. Effect of simethicone on lactulose-induced H2 production and gastrointestinal symptoms. Digestion 1991, 49, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Argoff, C.E.; Barton, N.W.; Brady, R.O.; Ziessman, H.A. Gastrointestinal symptoms and delayed gastric emptying in Fabry’s disease: Response to metoclopramide. Nucl. Med. Commun. 1998, 19, 887–892. [Google Scholar] [CrossRef] [PubMed]
- Bassotti, G.; Usai-Satta, P.; Bellini, M. Linaclotide for the treatment of chronic constipation. Expert Opin. Pharmacother. 2018, 19, 1261–1266. [Google Scholar] [CrossRef]
- Page, J.G.; Dirnberger, G.M. Treatment of the irritable bowel syndrome with Bentyl (dicyclomine hydrochloride). J. Clin. Gastroenterol. 1981, 3, 153–156. [Google Scholar] [CrossRef]
- Francini-Pesenti, F.; Ravarotto, V.; Bertoldi, G.; Spinella, P.; Calò, L.A. Could nutritional therapy take us further in our approaches to Fabry disease? Nutrition 2020, 72, 110664. [Google Scholar] [CrossRef]
- Liu, J.; Chey, W.D.; Haller, E.; Eswaran, S. Low-FODMAP Diet for Irritable Bowel Syndrome: What We Know and What We Have Yet to Learn. Annu. Rev. Med. 2020, 71, 303–314. [Google Scholar] [CrossRef] [Green Version]
- Murray, K.; Wilkinson-Smith, V.; Hoad, C.; Costigan, C.; Cox, E.; Lam, C.; Marciani, L.; Gowland, P.; Spiller, R.C. Differential effects of FODMAPs (fermentable oligo-, di-, mono-saccharides and polyols) on small and large intestinal contents in healthy subjects shown by MRI. Am. J. Gastroenterol. 2014, 109, 110–119. [Google Scholar] [CrossRef] [Green Version]
- Chey, W.D.; Hashash, J.G.; Manning, L.; Chang, L. AGA Clinical Practice Update on the Role of Diet in Irritable Bowel Syndrome: Expert Review. Gastroenterology 2022, 162, 1737–1745.e5. [Google Scholar] [CrossRef]
- Carubbi, F.; Barbato, A.; Burlina, A.B.; Francini, F.; Mignani, R.; Pegoraro, E.; Landini, L.; De Danieli, G.; Bruni, S.; Strazzullo, P. Nutrition in adult patients with selected lysosomal storage diseases. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 733–744. [Google Scholar] [CrossRef]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. Expert consensus document. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [Green Version]
- Marco, M.L.; Sanders, M.E.; Gänzle, M.; Arrieta, M.C.; Cotter, P.D.; De Vuyst, L.; Hill, C.; Holzapfel, W.; Lebeer, S.; Merenstein, D.; et al. The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on fermented foods. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 196–208. [Google Scholar] [CrossRef]
- Hilz, M.J.; Arbustini, E.; Dagna, L.; Gasbarrini, A.; Goizet, C.; Lacombe, D.; Liguori, R.; Manna, R.; Politei, J.; Spada, M.; et al. Non-specific gastrointestinal features: Could it be Fabry disease? Dig. Liver Dis. 2018, 50, 429–437. [Google Scholar] [CrossRef] [Green Version]
- Cozma-Petrut, A.; Loghin, F.; Miere, D.; Dumitrascu, D.L. Diet in irritable bowel syndrome: What to recommend, not what to forbid to patients! World J. Gastroenterol. 2017, 23, 3771–3783. [Google Scholar] [CrossRef]
- Staudacher, H.M.; Whelan, K. The low FODMAP diet: Recent advances in understanding its mechanisms and efficacy in IBS. Gut 2017, 66, 1517–1527. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.E.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [Green Version]
- Wiklund, I.K.; Fullerton, S.; Hawkey, C.J.; Jones, R.H.; Longstreth, G.F.; Mayer, E.A.; Peacock, R.A.; Wilson, I.K.; Naesdal, J. An irritable bowel syndrome-specific symptom questionnaire: Development and validation. Scand. J. Gastroenterol. 2003, 38, 947–954. [Google Scholar] [CrossRef]
- Francis, C.Y.; Morris, J.; Whorwell, P.J. The irritable bowel severity scoring system: A simple method of monitoring irritable bowel syndrome and its progress. Aliment. Pharmacol. Ther. 1997, 11, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Battaglia, Y.; Fiorini, F.; Azzini, C.; Esposito, P.; De vito, A.; Granata, A.; Storari, A.; Mignani, R. Deficiency in the Screening Process of Fabry Disease: Analysis of Chronic Kidney Patients Not on Dialysis. Front. Med. 2021, 8, 640876. [Google Scholar] [CrossRef]
- Svarstad, E.; Marti, H.P. The Changing Landscape of Fabry Disease. Clin. J. Am. Soc. Nephrol. 2020, 15, 569. [Google Scholar] [CrossRef] [PubMed]
- Jahan, S.; Sarathchandran, S.; Akhter, S.; Goldblatt, J.; Stark, S.; Crawford, D.; Mallett, A.; Thomas, M. Prevalence of Fabry disease in dialysis patients: Western Australia Fabry disease screening study-the FoRWARD study. Orphanet J. Rare Dis. 2020, 15, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Politei, J.; Thurberg, B.L.; Wallace, E.; Warnock, D.; Serebrinsky, G.; Durand, C.; Schenone, A.B. Gastrointestinal involvement in Fabry disease. So important, yet often neglected. Clin. Genet. 2016, 89, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.I.A.; Morris, A.I.; Nasmyth, D.G.; Carroll, N. Colonic involvement in Fabry’s disease. Postgrad. Med. J. 1991, 67, 584–585. [Google Scholar] [CrossRef] [Green Version]
- MacDermot, K.D.; Holmes, A.; Miners, A.H. Anderson-Fabry disease: Clinical manifestations and impact of disease in a cohort of 98 hemizygous males. J. Med. Genet. 2001, 38, 750–760. [Google Scholar] [CrossRef] [Green Version]
- Bellini, M.; Tonarelli, S.; Nagy, A.G.; Pancetti, A.; Costa, F.; Ricchiuti, A.; de Bortoli, N.; Mosca, M.; Marchi, S.; Rossi, A. Low FODMAP Diet: Evidence, Doubts, and Hopes. Nutrients 2020, 12, 148. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Food Group | Foods to Be Restricted | Foods Allowed |
|---|---|---|
| Dairy products | Cow’s, sheep’s, buffalo’s, and goat’s milk, soft cheeses, cream (sour and whipped), yogurt, mozzarella with lactose, béchamel cottage cheese and cheese sauces, milk chocolate. | Lactose-free cow’s milk, butter, aged cheese (e.g., Parmesan), lactose-free yogurt, lactose-free cheese |
| Dairy alternatives | Coconut milk and cream, soy milk | Almond milk, kefir, rice milk |
| Cereals | Bread, pasta, breadsticks, pastry products, … if made with wheat (wheat), various flours (chickpea flour, lentil flour, pea flour, soy flour), spelt, rye, barley, kamut, cous-cous, semolina | Breadsticks, pasta and pastry products (products with wheat-free cereals and flours: quinoa, rice, oats, buckwheat, amaranth, millet, sorghum, tapioca, polenta, amaranth) |
| Fruit | Apricots, avocados, persimmons, cherries, figs, lychees, mangoes, apples, blackberries, pears, peaches, nectarines, plums, plums, canned fruit, fruit jams not allowed | Pineapple (1 slice), orange (<130 g), banana (½ banana), clementine (n° 2), strawberries (about n° 10), passion fruit (maracuja), kiwi (<60 g), raspberries (<120 g), mandarin (n° 2), melon (<150 g), blueberries (<70 g), papaya (<80 g), grapefruit (<160 g), grapes (<30 g), strawberry jams, blueberries, raspberries |
| Vegetables | Garlic, asparagus, beets, broccoli, artichokes, Brussels sprouts, cauliflower, cabbage, chicory, onion, mushrooms, okra, green peppers, leek, shallot, cabbage | Carrots, cucumbers, spring onion (green parts only), ribs, fennel, lettuce and leafy salad, eggplant (<180 g) potatoes, sweet potatoes (½ potato), red peppers (<120 g), tomatoes (less than 200 g), celery (less than 1 stalk), chopped spinach, pumpkin, courgettes (<300 g) |
| Legumes and nuts | All (chickpeas, beans, lentils, …), pistachios, cashews, soy | Green beans and peas |
| Desserts | Any prepared with foods to be limited | Any prepared with permitted foods. Dark chocolate |
| Beverages | Fruit/vegetable juices with a high FODMAP content, beer, barley coffee, spirits, sweet wines | Fruit/vegetable juices with low FODMAP content (coffee (in limited quantities), tea, red and white wine (in limited quantities), herbal teas from permitted foods |
| Sweeteners | Sorbitol, mannitol, isomalt, maltitol, xylitol, honey, molasses, saccharin, agave or agave syrup, fructose and the syrups that contain it | Small quantities of white or brown sugar, glucose, pure maple syrup, aspartame |
| Other | Whole or powdered garlic and onion and mix of powdered vegetables (may contain garlic or onion), pickles and spring onions, miso, nuts or vegetable extracts, nuts or meat extracts, ready-made seasonings containing substances to avoid | Vinegar, balsamic vinegar, homemade broth aromatic herbs (e.g., chives, basil, parsley, etc.), bamboo shoots, lemon, mayonnaise, mustard, butter, margarine, canola oil, extra virgin olive oil, spices (pepper, red chili, ginger, cinnamon, etc.), olives, salt, gomasio |
| Sex | Age | Disease Form | Therapy | Body Mass Index | Low-FODMAP Protocol | IBS Severity Score | PCS12 | MCS12 | |
|---|---|---|---|---|---|---|---|---|---|
| All patients (Mean values, n. 36) | 36.1% males, 36.9% females | 47.6 ± 16.2 | 63.9% Late, 25% Classical, 11.2% VUS | 44.5% ERT, 19.4% Oral, 36.1% none | 25.6 ± 6.0 | 30.5% yes (11,1% in itinere), 69.5% no | 116.2 ± 97.8 | 45.6 ± 7.2 | 51.5 ± 11.2 |
| All patients with GI manifestations (Mean values, n. 22) | 27.3% males 72.3% females | 47.1 ± 13.2 | 50% Late, 40.9% Classical, 9.1% VUS | 46.1% ERT, 22.7% Oral, 31.2% none | 24.6 ± 5.7 | 50% yes (18.2% in itinere), 50% no | 181.1 ± 66.8 | 45.5 ± 6.8 | 49.8 ± 12.6 |
| All patients adhering to low-FODMAP protocol (Mean values, n. 11) | 27.3% males 72.7% females | 42.3 ± 12.7 | 36.4% Late, 54.5% Classical, 9% VUS | 54.5% ERT, 18.2% Oral, 27.3% none | 23.1 ± 5.3 | 63.6% completed the protocol, 36.3% in itinere | 195.2 ± 63.5 | 46.3 ± 8.0 | 48.7 ± 11.7 |
| GI Manifestations | N. of Patients | Mean IBS Severity Scores ± SD |
|---|---|---|
| No | 14 (38.9%) | 13.4 ± 14.3 (0–45) |
| Moderate | 10 (27.7%) | 120.6 ± 31.8 (83–170) |
| Severe | 12 (33.3%) | 231.5 ± 40.1 (190–290) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gugelmo, G.; Vitturi, N.; Francini-Pesenti, F.; Fasan, I.; Lenzini, L.; Valentini, R.; Carraro, G.; Avogaro, A.; Spinella, P. Gastrointestinal Manifestations and Low-FODMAP Protocol in a Cohort of Fabry Disease Adult Patients. Nutrients 2023, 15, 658. https://doi.org/10.3390/nu15030658
Gugelmo G, Vitturi N, Francini-Pesenti F, Fasan I, Lenzini L, Valentini R, Carraro G, Avogaro A, Spinella P. Gastrointestinal Manifestations and Low-FODMAP Protocol in a Cohort of Fabry Disease Adult Patients. Nutrients. 2023; 15(3):658. https://doi.org/10.3390/nu15030658
Chicago/Turabian StyleGugelmo, Giorgia, Nicola Vitturi, Francesco Francini-Pesenti, Ilaria Fasan, Livia Lenzini, Romina Valentini, Gianni Carraro, Angelo Avogaro, and Paolo Spinella. 2023. "Gastrointestinal Manifestations and Low-FODMAP Protocol in a Cohort of Fabry Disease Adult Patients" Nutrients 15, no. 3: 658. https://doi.org/10.3390/nu15030658