

Supplementation of Mother’s Own Milk with Preterm Donor Human Milk: Impact on Protein Intake and Growth in Very Low Birth Weight Infants—A Randomized Controlled Study
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
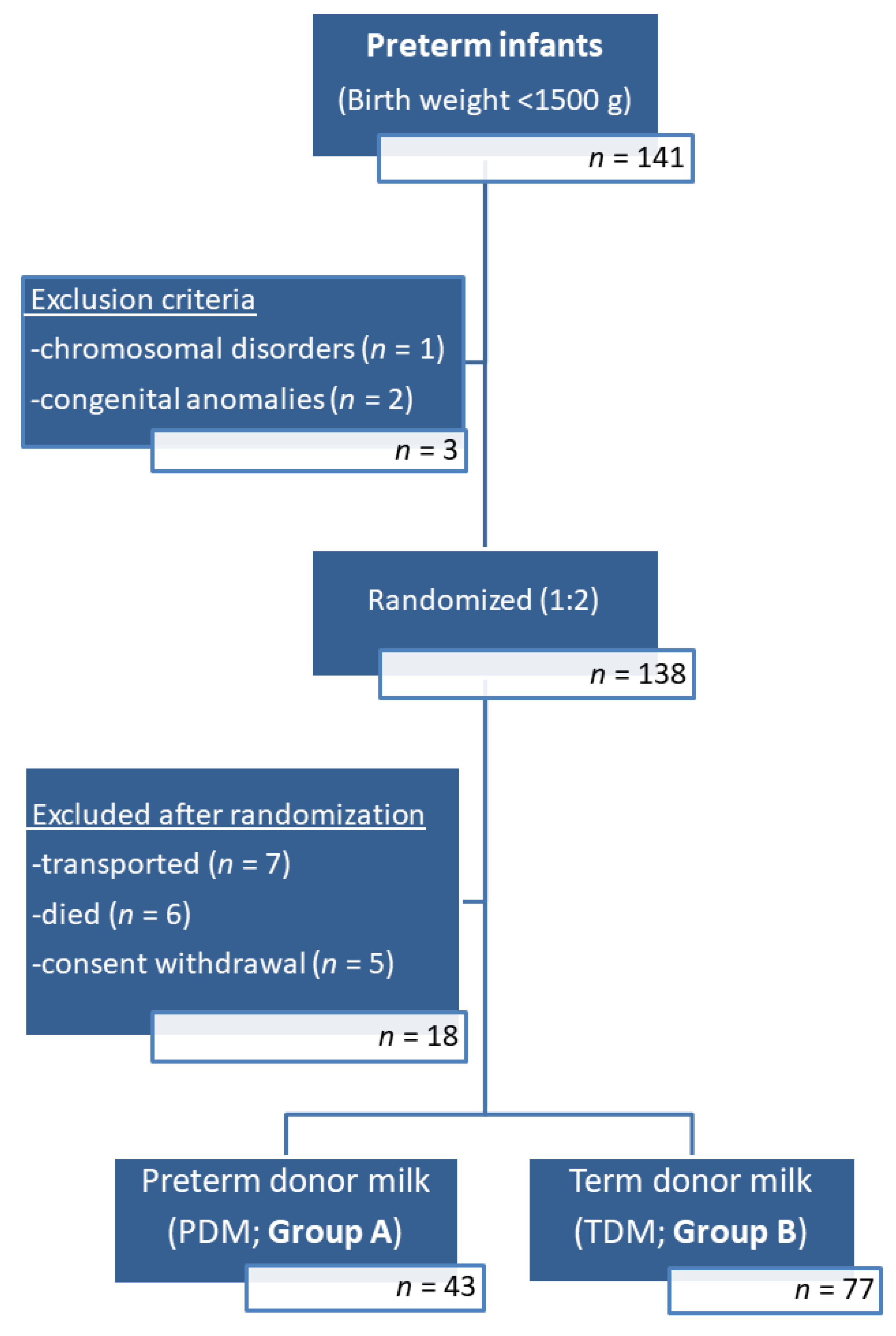
2.1. Study Design and Participants
2.2. Eligible Donor Mothers
2.3. Collection and Storage of Donor Human Milk
2.4. Feeding Protocol and Analysis of Human Milk
2.5. Data Collection
- CRIB II score (Clinical Risk Index for Babies), a validated measure of initial mortality risk and illness severity within the first hour of admission [28].
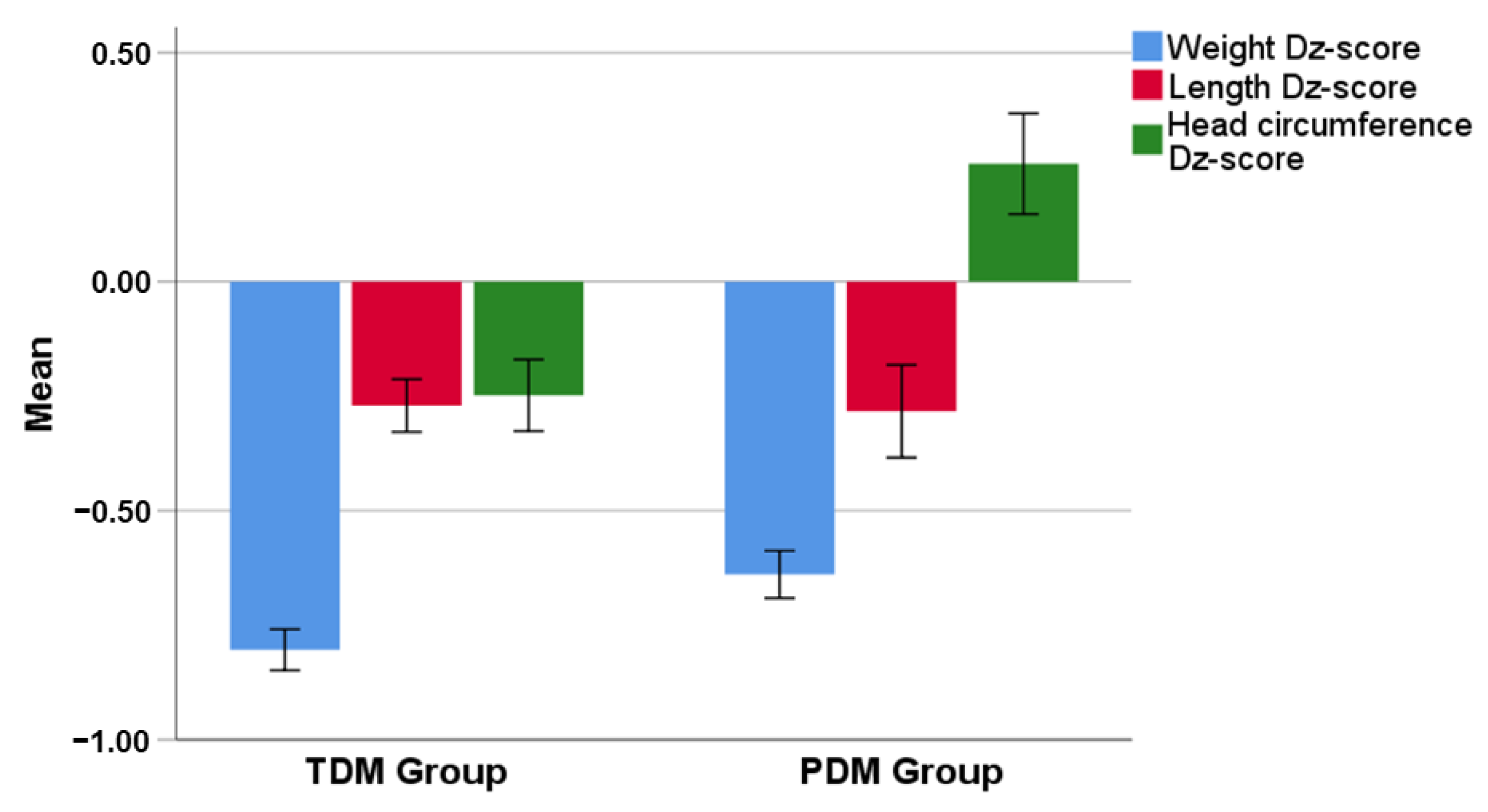
- Anthropometric characteristics (body weight and length, head circumference) at birth, at the end of donor milk period and at discharge. The anthropometric characteristics were recorded as both absolute values and z-scores; z-scores were documented according to the revised Fenton growth charts using the PediTools [29]. Small for gestational age (SGA) status was defined as birthweight z-score less than −2 SD from the mean. The difference (Δz-score) of z-score for body weight, body length and head circumference from birth to the end of donor milk period, as well as from birth to discharge, was calculated.
- Total protein and energy intake through parenteral nutrition, MOM, DM and fortification.
- Neonatal/Infant Morbidity. In particular:
- -
- Culture-positive sepsis (clinical signs of infection plus positive blood, urine or cerebrospinal fluid culture).
- -
- Necrotizing Enterocolitis (NEC) if fulfilling criteria compatible with Bell’s stage 2 or higher.
- -
- Bronchopulmonary dysplasia (BPD) defined as need for supplemental oxygen for more than 28 days.
- -
- Retinopathy of prematurity (ROP)—if fulfilling criteria compatible with Stage 3 according to international classification of retinopathy of prematurity (2005) [30].
- -
- Intraventricular hemorrhage (IVH)—any degree.
- -
- Patent ductus arteriosus (PDA) (presence of clinical signs plus ductal left to right shunt in echocardiography).
2.6. Statistical Analysis
3. Results
3.1. Protein and Calorie Intake
3.2. Growth
3.3. Clinical Characteristics and Morbidity during Hospitalization
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Morales, Y.; Schanler, R.J. Human milk and clinical outcomes in VLBW infants: How compelling is the evidence of benefit? Semin. Perinatol. 2007, 31, 83–88. [Google Scholar] [CrossRef]
- Schanler, R.J.; Shulman, R.J.; Lau, C. Feeding strategies for premature infants: Beneficial outcomes of feeding fortified human milk versus preterm formula. Pediatrics 1999, 103, 1150–1157. [Google Scholar] [CrossRef]
- Sen, S. Breast Milk and Breastfeeding: Benefits, Barriers, Maternal Predictors, and Opportunities for Innovation. Clin. Ther. 2022, 44, 170–171. [Google Scholar] [CrossRef] [PubMed]
- Lyons, K.E.; Ryan, C.A.; Dempsey, E.M.; Ross, R.P.; Stanton, C. Breast Milk, a Source of Beneficial Microbes and Associated Benefits for Infant Health. Nutrients 2020, 12, 1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, L.D.; Larson, E. Immunologic benefits of breast milk in relation to human milk banking. Am. J. Infect. Control 1993, 21, 235–242. [Google Scholar] [CrossRef]
- Magnus, P.D. Benefits of breast milk. Pediatrics 1980, 65, 192–193. [Google Scholar] [CrossRef] [PubMed]
- Eidelman, A.I. Breastfeeding and the use of human milk: An analysis of the American Academy of Pediatrics 2012 Breastfeeding Policy Statement. Breastfeed Med. 2012, 7, 323–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helenius, K.; Sjörs, G.; Shah, P.S.; Modi, N.; Reichman, B.; Morisaki, N.; Kusuda, S.; Lui, K.; Darlow, B.A.; Bassler, D.; et al. International Network for Evaluating Outcomes (iNeo) of Neonates. Survival in Very Preterm Infants: An International Comparison of 10 National Neonatal Networks. Pediatrics 2017, 140, e20171264. [Google Scholar] [CrossRef] [Green Version]
- Lincetto, O.; Banerjee, A. World Prematurity Day: Improving survival and quality of life for millions of babies born preterm around the world. Am. J. Physiol. Lung Cell Mol. Physiol. 2020, 319, 871–874. [Google Scholar] [CrossRef] [PubMed]
- McClure, E.M.; Goldenberg, R.L. Preterm neonatal survival: What is the role of prognostic models? BJOG 2022, 129, 539. [Google Scholar] [CrossRef]
- van Beek, P.E.; Groenendaal, F.; Broeders, L.; Dijk, P.H.; Dijkman, K.P.; van den Dungen, F.A.M.; van Heijst, A.F.J.; van Hillegersberg, J.L.; Kornelisse, R.F.; Onland, W.; et al. Survival and causes of death in extremely preterm infants in the Netherlands. Arch. Dis. Child Fetal Neonatal Ed. 2021, 106, 251–257. [Google Scholar] [CrossRef] [PubMed]
- ESPGHAN Committee on Nutrition; Arslanoglu, S.; Corpeleijn, W.; Moro, G.; Braegger, C.; Campoy, C.; Colomb, V.; Decsi, T.; Domellöf, M.; Fewtrell, M.; et al. Donor human milk for preterm infants: Current evidence and research directions. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Moro, G.E.; Arslanoglu, S.; Bertino, E.; Corvaglia, L.; Montirosso, R.; Picaud, J.C.; Polberger, S.; Schanler, R.J.; Steel, C.; van Goudoever, J.; et al. American Academy of Pediatrics; European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. XII. Human Milk in Feeding Premature Infants: Consensus Statement. J. Pediatr. Gastroenterol. Nutr 2015, 61, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Committee on Nutrition, Section on Breastfeeding, Committee on Fetus and Newborn. Donor Human Milk for the High-Risk Infant: Preparation, Safety, and Usage Options in the United States. Pediatrics 2017, 139, 20163440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dritsakou, K.; Liosis, G.; Valsami, G.; Polychronopoulos, E.; Skouroliakou, M. Improved outcomes of feeding low birth weight infants with predominantly raw human milk versus donor banked milk and formula. J. Matern. Fetal Neonatal Med. 2016, 29, 1131–1138. [Google Scholar] [CrossRef] [PubMed]
- Ballard, O.; Morrow, A.L. Human milk composition: Nutrients and bioactive factors. Pediatr. Clin. N. Am. 2013, 60, 49–74. [Google Scholar] [CrossRef] [Green Version]
- Bauer, J.; Gerss, J. Longitudinal analysis of macronutrients and minerals in human milk produced by mothers of preterm infants. Clin. Nutr. 2011, 30, 215–220. [Google Scholar] [CrossRef]
- Agostoni, C.; Buonocore, G.; Carnielli, V.P.; De Curtis, M.; Darmaun, D.; Decsi, T.; Domellöf, M.; Embleton, N.D.; Fusch, C.; Genzel-Boroviczeny, O.; et al. ESPGHAN Committee on Nutrition. Enteral nutrient supply for preterm infants: Commentary from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 85–91. [Google Scholar] [CrossRef]
- Stephens, B.E.; Walden, R.V.; Gargus, R.A.; Tucker, R.; McKinley, L.; Mance, M.; Nye, J.; Vohr, B.R. First-week protein and energy intakes are associated with 18-month developmental outcomes in extremely low birth weight infants. Pediatrics 2009, 123, 1337–1343. [Google Scholar] [CrossRef]
- Rigo, J.; Hascoët, J.M.; Billeaud, C.; Picaud, J.C.; Mosca, F.; Rubio, A.; Saliba, E.; Radkë, M.; Simeoni, U.; Guillois, B.; et al. Growth and Nutritional Biomarkers of Preterm Infants Fed a New Powdered Human Milk Fortifier: A Randomized Trial. J. Pediatr. Gastroenterol. Nutr. 2017, 65, e83–e93. [Google Scholar] [CrossRef]
- Atkinson, S.A. Special nutritional needs of infants for prevention of and recovery from bronchopulmonary dysplasia. J. Nutr. 2001, 131, 942–946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, D.M. Feeding the ill or preterm infant. Neonatal Netw. 2002, 21, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Huston, R.; Lee, M.; Rider, E.; Stawarz, M.; Hedstrom, D.; Pence, M.; Chan, V.; Chambers, J.; Rogers, S.; Sager, N.; et al. Early fortification of enteral feedings for infants <1250 grams birth weight receiving a human milk diet including human milk based fortifier. J. Neonatal Perinat. Med. 2020, 13, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Arslanoglu, S.; Boquien, C.Y.; King, C.; Lamireau, D.; Tonetto, P.; Barnett, D.; Bertino, E.; Gaya, A.; Gebauer, C.; Grovslien, A.; et al. Fortification of Human Milk for Preterm Infants: Update and Recommendations of the European Milk Bank Association (EMBA) Working Group on Human Milk Fortification. Front. Pediatr. 2019, 22, 7–76. [Google Scholar] [CrossRef] [PubMed]
- Khaira, S.; Pert, A.; Farrell, E.; Sibley, C.; Harvey-Wilkes, K.; Nielsen, H.C.; Volpe, M.V. Expressed Breast Milk Analysis: Role of Individualized Protein Fortification to Avoid Protein Deficit After Preterm Birth and Improve Infant Outcomes. Front. Pediatr. 2022, 9, 652038. [Google Scholar] [CrossRef]
- Italian Association of Human Milk Banks Associazione Italiana Banche del Latte Umano Donato. Guidelines for the establishment and operation of a donor human milk bank. J. Matern. Fetal Neonatal Med. 2010, 23, 1–20. [Google Scholar] [CrossRef]
- Leghi, G.E.; Middleton, P.F.; Netting, M.J.; Wlodek, M.E.; Geddes, D.T.; Muhlhausler, B.S. A Systematic Review of Collection and Analysis of Human Milk for Macronutrient Composition. J. Nutr. 2020, 1, 1652–1670. [Google Scholar] [CrossRef]
- Parry, G.; Tucker, J.; Tarnow-Mordi, W.; UK Neonatal Staffing Study Collaborative Group. CRIB II: An update of the clinical risk index for babies score. Lancet 2003, 361, 1789–1791. [Google Scholar] [CrossRef]
- Chou, J.H.; Roumiantsev, S.; Singh, R. PediTools Electronic Growth Chart Calculators: Applications in Clinical Care, Research, and Quality Improvement. J. Med. Internet Res. 2020, 22, 16204. [Google Scholar] [CrossRef]
- International Committee for the Classification of Retinopathy of Prematurity. The International Classification of Retinopathy of Prematurity revisited. Arch. Ophthalmol. 2005, 123, 991–999. [Google Scholar] [CrossRef]
- Hay, W.W.; Ziegler, E.E. Growth failure among preterm infants due to insufficient protein is not innocuous and must be prevented. J. Perinatol. 2016, 36, 500–502. [Google Scholar] [CrossRef] [PubMed]
- Horbar, J.D.; Ehrenkranz, R.A.; Badger, G.J.; Edwards, E.M.; Morrow, K.A.; Soll, R.F.; Buzas, J.S.; Bertino, E.; Gagliardi, L.; Bellù, R. Weight Growth Velocity and Postnatal Growth Failure in Infants 501 to 1500 Grams: 2000–2013. Pediatrics. 2015, 136, 84–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.M.; Kim, N.; Namgung, R.; Park, M.; Park, K.; Jeon, J. Prediction of Postnatal Growth Failure among Very Low Birth Weight Infants. Sci. Rep. 2018, 27, 3729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, L.D.; Hay, W.W., Jr. The nutritional dilemma for preterm infants: How to promote neurocognitive development and linear growth, but reduce the risk of obesity. J. Pediatr. 2013, 163, 1543–1545. [Google Scholar] [CrossRef]
- Hay, W.W., Jr.; Brown, L.D.; Denne, S.C. Energy requirements, protein-energy metabolism and balance, and carbohydrates in preterm infants. World Rev. Nutr. Diet. 2014, 110, 64–81. [Google Scholar] [CrossRef]
- Mills, L.; Coulter, L.; Savage, E.; Modi, N. Macronutrient content of donor milk from a regional human milk bank: Variation with donor mother-infant characteristics. Br. J. Nutr. 2019, 28, 1155–1167. [Google Scholar] [CrossRef] [Green Version]
- Lemons, J.A.; Moye, L.; Hall, D.; Simmons, M. Differences in the composition of preterm and term human milk during early lactation. Pediatr. Res. 1982, 16, 113–117. [Google Scholar] [CrossRef] [Green Version]
- Dritsakou, K.; Liosis, G.; Valsami, G.; Polychronopoulos, E.; Skouroliakou, M. The impact of maternal- and neonatal-associated factors on human milk’s macronutrients and energy. J. Matern. Fetal Neonatal Med. 2017, 30, 1302–1308. [Google Scholar] [CrossRef]
- Borràs-Novell, C.; Herranz Barbero, A.; Balcells Esponera, C.; López-Abad, M.; Aldecoa Bilbao, V.; Izquierdo Renau, M.; Iglesias Platas, I. Influence of maternal and perinatal factors on macronutrient content of very preterm human milk during the first weeks after birth. J. Perinatol. 2023, 43, 52–59. [Google Scholar] [CrossRef]
- Embleton, N.D.; Moltu, S.J.; Lapillonne, A.; van den Akker, C.H.P.; Carnielli, V.; Fusch, C.; Gerasimidis, K.; van Goudoever, J.B.; Haiden, N.; Iacobelli, S.; et al. Enteral Nutrition in Preterm Infants (2022): A Position Paper from the ESPGHAN Committee on Nutrition and invited experts. J. Pediatr. Gastroenterol. Nutr. 2022, 00005176-990000000-00204. [Google Scholar] [CrossRef]
- Alyahya, W.; Simpson, J.; Garcia, A.L.; Mactier, H.; Edwards, C.A. Early versus Delayed Fortification of Human Milk in Preterm Infants: A Systematic Review. Neonatology 2020, 117, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Castellano Yáñez, C.; Castillo Barrio, B.; Muñoz Labián, M.D.C.; Ortiz Movilla, R.; García Lara, N.R.; Royuela Vicente, A.; Marín Gabriel, M.A. Providing very preterm infants with donor human milk led to faster breastfeeding rates but worse biometric gains. Acta Paediatr. 2019, 108, 766–767. [Google Scholar] [CrossRef] [PubMed]
- Hoban, R.; Schoeny, M.E.; Esquerra-Zwiers, A.; Kaenkumchorn, T.K.; Casini, G.; Tobin, G.; Siegel, A.H.; Patra, K.; Hamilton, M.; Wicks, J.; et al. Impact of Donor Milk on Short- and Long-Term Growth of Very Low Birth Weight Infants. Nutrients 2019, 11, 241. [Google Scholar] [CrossRef] [Green Version]
- Ginovart, G.; Gich, I.; Gutiérrez, A.; Verd, S. A Fortified Donor Milk Policy is Associated with Improved In-Hospital Head Growth and Weight Gain in Very Low-Birth-Weight Infants. Adv. Neonatal Care 2017, 17, 250–257. [Google Scholar] [CrossRef]
- Madore, L.S.; Bora, S.; Erdei, C.; Jumani, T.; Dengos, A.R.; Sen, S. Effects of Donor Breastmilk Feeding on Growth and Early Neurodevelopmental Outcomes in Preterm Infants: An Observational Study. Clin. Ther. 2017, 39, 1210–1220. [Google Scholar] [CrossRef] [PubMed]
- Fang, L.; Zhang, M.; Wu, L.; Wang, R.; Lin, B.; Yao, J.; Chen, D. Is preterm donor milk better than preterm formula for very-low-birth-weight infants? Food Nutr. Res. 2021, 65. [Google Scholar] [CrossRef] [PubMed]
- Arslanoglu, S.; Moro, G.E.; Ziegler, E.E. Preterm infants fed fortified human milk receive less protein than they need. J. Perinatol. 2009, 29, 489–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landers, S.; Hartmann, B.T. Donor human milk banking and the emergence of milk sharing. Pediatr. Clin. N. Am. 2013, 60, 247–260. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total Population (N = 120) | Group A (N = 43) | Group B (N = 77) | p-Value | |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | ||
| Mother’s age (years) | 33.8 (5.1) | 32.7 (5.0) | 34.4 (5.0) | 0.233 + |
| Gestational age (weeks) | 29.7 (2.5) | 29.7 (2.4) | 29.7 (2.5) | 0.959 + |
| N (%) | N (%) | N (%) | ||
| Pregnancy | ||||
| Single | 88 (73.3) | 30 (69.8) | 52 (67.5) | 0.484 ‡ |
| Multiple | 32 (26.7) | 13 (30.2) | 25 (32.5) | |
| Gender | ||||
| Females | 47 (39.2) | 14 (32.6) | 33 (42.9) | 0.268 ‡ |
| Males | 73 (60.8) | 29 (67.4) | 44 (57.1) | |
| SGA | 10 (8.3) | 3 (7.0) | 7 (9.1) | 0.489 ‡ |
| Mean (SD) | Mean (SD) | Mean (SD) | ||
| Birth Weight (g) | 1169.8 (234.1) | 1182.9 (257.6) | 1162.5 (221.3) | 0.649 + |
| Birth Weight z-score | −0.48 (0.98) | −0.48 (0.93) | −0.48 (1.01) | 0.987 + |
| Body length at birth (cm) | 38.0 (3.3) | 38.2 (3.1) | 37.8 (3.3) | 0.562 + |
| Body length z-score | −0.20 (1.14) | −0.13 (1.21) | −0.24 (1.11) | 0.598 + |
| Head circumference at birth (cm) | 26.6 (2.0) | 26.5 (2.1) | 26.7 (1.9) | 0.720 + |
| Head circumference z-score at birth | −0.24 (1.26) | −0.38 (1.25) | −0.16 (1.26) | 0.362 + |
| CRIB II score | 6.9 (3.1) | 6.8 (3.1) | 6.9 (3.2) | 0.878 + |
| Median (IQR) | Median (IQR) | Median (IQR) | ||
| Length of hospitalization (days) | 56.5 (45.0–69.5) | 58.0 (47.0–68.0) | 55.0 (42.0–72.0) | 0.465 ++ |
| Total Population (N = 69) | PDM Mothers (N = 26) | TDM Mothers (N = 43) | p-Value | |
|---|---|---|---|---|
| Gestational age, weeks | 34.7 (4.6) | 29.8 (2.7) | 38.0 (2.0) | <0.001 + |
| Maternal age, years | 33.7 (3.7) | 32.9 (4.0) | 34.3 (3.4) | 0.130 + |
| Parity, N (%) | ||||
| 1st | 42 (60.9) | 20 (76.9) | 22 (51.2) | 0.138 ‡ |
| 2nd | 26 (37.7) | 6 (23.1) | 20 (46.5) | |
| 3rd | 1 (1.4) | 0 (0) | 1 (2.3) | |
| Multiple gestation, N (%) | 6 (8.7) | 4 (15.4) | 2 (4.6) | 0.138 ‡ |
| Total Population (N = 120) | Group A (N = 43) | Group B (N = 77) | p-Value | |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | ||
| During hospitalization | 3.03 (0.57) | 3.20 (0.60) | 2.93 (0.54) | 0.014 + |
| Donor milk period | ||||
| 1st week | 3.35 (1.05) | 3.53 (1.10) | 3.25 (1.01) | 0.023 ++ |
| 2nd week | 3.53 (1.13) | 3.67 (1.05) | 3.45 (1.17) | |
| 3rd week | 3.36 (0.99) | 3.67 (0.96) | 3.19 (0.97) | |
| At initiation of human milk fortification | 3.24 (0.84) | 3.57 (0.82) | 2.92 (0.85) | 0.006 + |
| Total Population (N = 120) | Group A (N = 43) | Group B (N = 77) | p-Value | |
|---|---|---|---|---|
| Ν (%) | Ν (%) | Ν (%) | ||
| Sepsis | ||||
| No | 91 (75.8) | 35 (81.4) | 56 (72.7) | 0.288 + |
| Yes | 29 (24.2) | 8 (18.6) | 21 (27.3) | |
| Necrotizing enterocolitis | ||||
| No | 118 (98.3) | 42 (97.7) | 76 (98.7) | 1.000 ++ |
| Yes | 2 (1.7) | 1 (2.3) | 1 (1.3) | |
| Retinopathy of prematurity | ||||
| No | 116 (96.7) | 41 (95.3) | 75 (97.4) | 0.617 ++ |
| Yes | 4 (3.3) | 2 (4.7) | 2 (2.6) | |
| Bronchopulmonary dysplasia | ||||
| No | 75 (62.5) | 24 (55.8) | 51 (66.2) | 0.258 + |
| Yes | 45 (37.5) | 19 (44.2) | 26 (33.8) | |
| Intraventricular hemorrhage | ||||
| No | 116 (96.7) | 42 (97.7) | 74 (96.1) | 1.000 ++ |
| Yes | 4 (3.3) | 1 (2.3) | 3 (3.9) | |
| Patent Ductus Arteriosus | ||||
| No | 73 (84.9) | 23 (85.2) | 50 (84.7) | 1.000 ++ |
| Yes | 13 (15.1) | 4 (14.8) | 9 (15.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gialeli, G.; Kapetanaki, A.; Panagopoulou, O.; Vourna, P.; Michos, A.; Kanaka-Gantenbein, C.; Liosis, G.; Siahanidou, T. Supplementation of Mother’s Own Milk with Preterm Donor Human Milk: Impact on Protein Intake and Growth in Very Low Birth Weight Infants—A Randomized Controlled Study. Nutrients 2023, 15, 566. https://doi.org/10.3390/nu15030566
Gialeli G, Kapetanaki A, Panagopoulou O, Vourna P, Michos A, Kanaka-Gantenbein C, Liosis G, Siahanidou T. Supplementation of Mother’s Own Milk with Preterm Donor Human Milk: Impact on Protein Intake and Growth in Very Low Birth Weight Infants—A Randomized Controlled Study. Nutrients. 2023; 15(3):566. https://doi.org/10.3390/nu15030566
Chicago/Turabian StyleGialeli, Giannoula, Anastasia Kapetanaki, Ourania Panagopoulou, Panagiota Vourna, Athanasios Michos, Christina Kanaka-Gantenbein, George Liosis, and Tania Siahanidou. 2023. "Supplementation of Mother’s Own Milk with Preterm Donor Human Milk: Impact on Protein Intake and Growth in Very Low Birth Weight Infants—A Randomized Controlled Study" Nutrients 15, no. 3: 566. https://doi.org/10.3390/nu15030566