
The Effects of a Multisector, Multilevel Intervention on Child Dietary Intake: California Childhood Obesity Research Demonstration Study
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
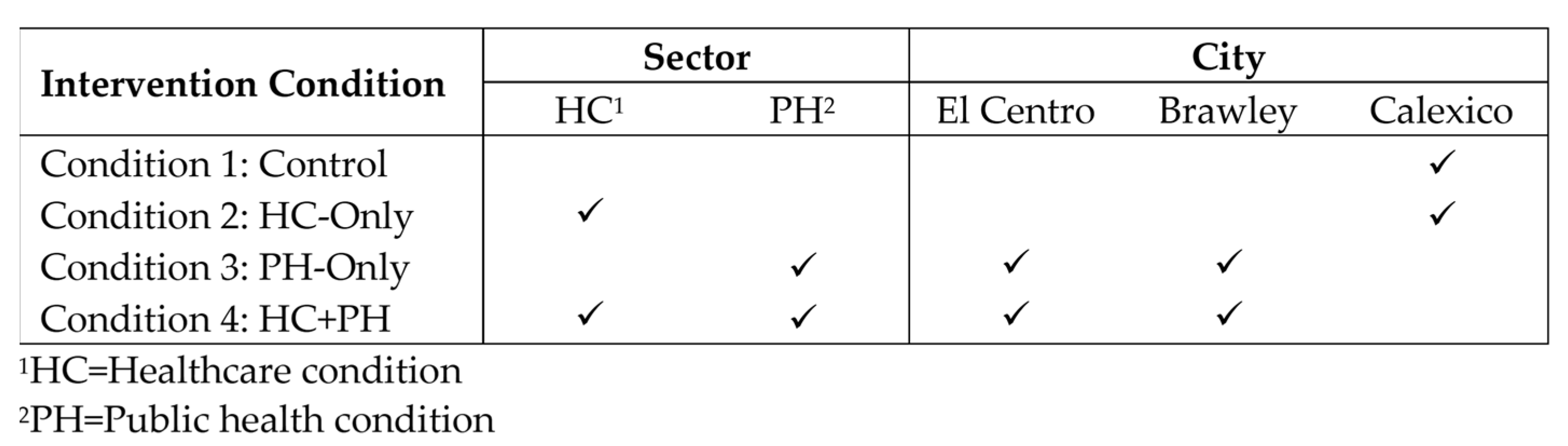
2.1. Study Design
2.2. Participant Recruitment
2.3. Baseline Assessment
2.4. Intervention Strategies
2.5. Measures
2.6. Data Analysis
3. Results
3.1. Non-Participants vs. Participants
3.2. Participants’ Baseline Characteristics
3.3. Intervention Effects on Child Dietary Outcomes and Potential Mediators
3.4. Mediating Role of Caregiver Dietary Intake, Parenting Strategies, and Family Meal Contexts
4. Discussion
Study Strengths and Limitations
5. Conclusions
Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- U.S. Department of Health and Human Services, U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans; Department of Agriculture: Washington, DC, USA, 2015.
- Wambogo, E.A.; Ansai, N.; Ahulwalia, N.; Ogden, C.L. Fruit and Vegetable Consumption among Children and Adolescents in the United States, 2015–2018. NCHS Data Brief. 2020. Available online: https://www.cdc.gov/nchs/data/databriefs/db391-H.pdf (accessed on 5 April 2021).
- The Agricultural Research Service, U.S. Department of Agriculture. Nutrient Intakes from Food and Beverages: Mean Amounts Consumed per Individual, by Gender and Age, What We Eat in America, NHANES 2017–2018. Available online: https://www.ars.usda.gov/ARSUserFiles/80400530/pdf/1718/Table_1_NIN_GEN_17.pdf (accessed on 5 June 2019).
- Evans, C.E.L.; Christian, M.S.; Cleghorn, C.L.; Greenwood, D.C.; Cade, J.E. Systematic review and meta-analysis of school-based interventions to improve daily fruit and vegetable intake in children aged 5 to 12 y. Am. J. Clin. Nutr. 2012, 96, 889–901. [Google Scholar] [CrossRef]
- Paineau, D.L.; Beaufils, F.; Boulier, A.; Cassuto, D.A.; Chwalow, J.; Combris, P.; Couet, C.; Jouret, B.; Lafay, L.; Laville, M.; et al. Family dietary coaching to improve nutritional intakes and body weight control: A randomized controlled trial. Arch. Pediatr. Adolesc. Med. 2008, 162, 34–43. [Google Scholar] [CrossRef]
- Stokols, D. Translating social ecological theory into guidelines for community health promotion. Am. J. Health Promot. 1996, 10, 282–298. [Google Scholar] [CrossRef]
- Ash, T.; Agaronov, A.; Young, T.; Aftosmes-Tobio, A.; Davison, K.K. Family-based childhood obesity prevention interventions: A systematic review and quantitative content analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 113. [Google Scholar] [CrossRef] [PubMed]
- Foltz, J.L.; Belay, B.; Dooyema, C.A.; Williams, N.; Blanck, H.M. Childhood Obesity Research Demonstration (CORD): The cross-site overview and opportunities for interventions addressing obesity community-wide. Child. Obes. 2015, 11, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Sen, M.; Uzuner, A.; Akman, M.; Bahadir, A.T.; Borekci, N.O.; Viggiano, E. Examination of a board game approach to children’s involvement in family-based weight management vs. traditional family-based behavioral counseling in primary care. Eur. J. Pediatr. 2018, 177, 1231–1238. [Google Scholar] [CrossRef]
- Sherwood, N.E.; Levy, R.L.; Seburg, E.M.; Crain, A.L.; Langer, S.L.; JaKa, M.M.; Kunin-Batson, A.; Jeffery, R.W. The Healthy Homes/Healthy Kids 5-10 Obesity Prevention Trial: 12 and 24-month outcomes. Pediatr. Obes. 2019, 14, e12523. [Google Scholar] [CrossRef] [PubMed]
- Adab, P.; Pallan, M.J.; Lancashire, E.R.; Hemming, K.; Frew, E.; Barrett, T.; Bhopal, R.; Cade, J.E.; Canaway, A.; Clarke, J.L.; et al. Effectiveness of a childhood obesity prevention programme delivered through schools, targeting 6 and 7 year olds: Cluster randomised controlled trial (WAVES study). BMJ 2018, 360, k211. [Google Scholar] [CrossRef]
- Williams, P.A.; Cates, S.C.; Blitstein, J.L.; Hersey, J.; Gabor, V.; Ball, M.; Kosa, K.; Wilson, H.; Olson, S.; Singh, A. Nutrition-education program improves preschoolers’ at-home diet: A group randomized trial. J. Acad. Nutr. Diet. 2014, 114, 1001–1008. [Google Scholar] [CrossRef]
- Robertson, W.; Fleming, J.; Kamal, A.; Hamborg, T.; Khan, K.A.; Griffiths, F.; Stewart-Brown, S.; Stallard, N.; Petrou, S.; Simkiss, D.; et al. Randomised controlled trial evaluating the effectiveness and cost-effectiveness of ‘Families for Health’, a family-based childhood obesity treatment intervention delivered in a community setting for ages 6 to 11 years. Health Technol. Assess. 2017, 21, 1–180. [Google Scholar] [CrossRef]
- Wang, Y.; Beydoun, M.A.; Li, J.; Liu, Y.; Moreno, L.A. Do children and their parents eat a similar diet? Resemblance in child and parental dietary intake: Systematic review and meta-analysis. J. Epidemiol. Community Health 2011, 65, 177–189. [Google Scholar] [CrossRef]
- Watts, A.W.; Masse, L.C.; Barr, S.I.; Lovato, C.Y.; Hanning, R.M. Parent-child associations in selected food group and nutrient intakes among overweight and obese adolescents. J. Acad. Nutr. Diet. 2014, 114, 1580–1586. [Google Scholar] [CrossRef] [PubMed]
- Haire-Joshu, D.; Elliott, M.B.; Caito, N.M.; Hessler, K.; Nanney, M.S.; Hale, N.; Boehmer, T.K.; Kreuter, M.; Brownson, R.C. High 5 for Kids: The impact of a home visiting program on fruit and vegetable intake of parents and their preschool children. Prev. Med. 2008, 47, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Jaakkola, J.M.; Pahkala, K.; Ronnemaa, T.; Viikari, J.; Niinikoski, H.; Jokinen, E.; Lagstrom, H.; Jula, A.; Raitakari, O. Longitudinal child-oriented dietary intervention: Association with parental diet and cardio-metabolic risk factors. The Special Turku Coronary Risk Factor Intervention Project. Eur. J. Prev. Cardiol. 2017, 24, 1779–1787. [Google Scholar] [CrossRef] [PubMed]
- Arredondo, E.M.; Elder, J.P.; Ayala, G.X.; Campbell, N.; Baquero, B.; Duerksen, S. Is parenting style related to children’s healthy eating and physical activity in Latino families? Health Educ. Res. 2006, 21, 862–871. [Google Scholar] [CrossRef]
- Crespo, N.C.; Elder, J.P.; Ayala, G.X.; Slymen, D.J.; Campbell, N.R.; Sallis, J.F.; McKenzie, T.L.; Baquero, B.; Arredondo, E.M. Results of a multi-level intervention to prevent and control childhood obesity among Latino children: The Aventuras Para Ninos Study. Ann. Behav. Med. 2012, 43, 84–100. [Google Scholar] [CrossRef]
- Saksena, M.J.; Okrent, A.M.; Anekwe, T.D.; Cho, C.; Dicken, C.; Effland, A.; Elitzak, H.; Guthrie, J.; Hamrick, K.S.; Hyman, J.; et al. America’s Eating Habits: Food Away From Home; Saksena, M., Okrent, A.M., Hamrick, K.S., Eds.; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2018. [Google Scholar]
- Mancino, L.; Todd, J.E.; Guthrie, J.; Lin, B.H. Food Away from Home and Childhood Obesity. Curr. Obes. Rep. 2014, 3, 459–469. [Google Scholar] [CrossRef]
- Dallacker, M.; Hertwig, R.; Mata, J. The frequency of family meals and nutritional health in children: A meta-analysis. Obes. Rev. 2018, 19, 638–653. [Google Scholar] [CrossRef]
- Ayala, G.X.; Ibarra, L.; Binggeli-Vallarta, A.; Moody, J.; McKenzie, T.L.; Angulo, J.; Hoyt, H.; Chuang, E.; Ganiats, T.G.; Gahagan, S.; et al. Our Choice/Nuestra Opcion: The Imperial County, California, Childhood Obesity Research Demonstration study (CA-CORD). Child. Obes. 2015, 11, 37–47. [Google Scholar] [CrossRef]
- U.S. Census Bureau. Selected Characteristics of the Native and Foreign-Born Populations: 2009–2013 American Community Survey 5-Year Estimates. Available online: https://factfinder.census.gov/faces/nav/jsf/pages/community_facts.xhtml (accessed on 12 July 2018).
- Babey, S.H.; Wolstein, J.; Diamant, A.L.; Bloom, A.; Golstein, H. A Patchwork of Progress: Changes in Overweight and Obesity among California 5th, 7th, and 9th Graders, 2005–2010. Available online: https://escholarship.org/uc/item/8wr3t0zc (accessed on 21 May 2018).
- Bandura, A. Social Foundations of Thought and Actions: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Broderick, C. Understanding Family Process: Basics of Family Systems Theory; Sage: Newbury Park, CA, USA, 1993. [Google Scholar]
- Jacobson, D.; Gance-Cleveland, B. A systematic review of primary healthcare provider education and training using the Chronic Care Model for Childhood Obesity. Obes. Rev. 2011, 12, e244–e256. [Google Scholar] [CrossRef]
- Skelton, J.A.; Buehler, C.; Irby, M.B.; Grzywacz, J.G. Where are family theories in family-based obesity treatment? Conceptualizing the study of families in pediatric weight management. Int. J. Obes. 2012, 36, 891–900. [Google Scholar] [CrossRef] [PubMed]
- Goldman, R.L.; Radnitz, C.L.; Mcgrath, R.E. The Role of Family Variables in Fruit and Vegetable Consumption in Pre-School Children. J. Public Health Res. 2012, 1, jphr.2012.e202. [Google Scholar] [CrossRef] [PubMed]
- Schmied, E.A.; Chuang, E.; Madanat, H.; Moody, J.; Ibarra, L.; Ortiz, K.; Macias, K.; Ayala, G.X. A Qualitative Examination of Parent Engagement in a Family-Based Childhood Obesity Program. Health Promot. Pract. 2018, 19, 905–914. [Google Scholar] [CrossRef] [PubMed]
- Chuang, E.; Ayala, G.X.; Schmied, E.; Ganter, C.; Gittelsohn, J.; Davison, K.K. Evaluation Protocol To Assess an Integrated Framework for the Implementation of the Childhood Obesity Research Demonstration Project at the California (CA-CORD) and Massachusetts (MA-CORD) Sites. Child. Obes. 2015, 11, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.-F.; Binggeli-Vallarta, A.; Cervantes, G.; Angulo, J.; Moody, J.S.; McKenzie, T.L.; Horton, L.A.; Ayala, G.X. Process evaluation of an early care and education intervention: The California childhood obesity research demonstration study (CA-CORD). Health Promot. Pract. 2020, 21, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Hunsberger, M.; O’Malley, J.; Block, T.; Norris, J.C. Relative validation of Block Kids Food Screener for dietary assessment in children and adolescents. Matern. Child Nutr. 2015, 11, 260–270. [Google Scholar] [CrossRef]
- National Cancer Institute. Percentage Energy from Fat Screener: Scoring Procedures. Available online: https://epi.grants.cancer.gov/diet/screeners/fat/scoring.html#scoring (accessed on 22 November 2019).
- Yaroch, A.L.; Tooze, J.; Thompson, F.E.; Blanck, H.M.; Thompson, O.M.; Colon-Ramos, U.; Shaikh, A.R.; McNutt, S.; Nebeling, L.C. Evaluation of three short dietary instruments to assess fruit and vegetable intake: The National Cancer Institute’s Food Attitudes and Behaviors (FAB) Survey. J. Acad. Nutr. Diet. 2012, 112, 1570–1577. [Google Scholar] [CrossRef]
- Larios, S.E.; Ayala, G.X.; Arredondo, E.M.; Baquero, B.; Elder, J.P. Development and validation of a scale to measure Latino parenting strategies related to children’s obesigenic behaviors. The parenting strategies for eating and activity scale (PEAS). Appetite 2009, 52, 166–172. [Google Scholar] [CrossRef]
- Ayala, G.X.; Elder, J.P.; Campbell, N.R.; Arredondo, E.; Baquero, B.; Crespo, N.C.; Slymen, D.J. Longitudinal intervention effects on parenting of the Aventuras para Ninos study. Am. J. Prev. Med. 2010, 38, 154–162. [Google Scholar] [CrossRef]
- Ayala, G.X.; Baquero, B.; Arredondo, E.M.; Campbell, N.; Larios, S.; Elder, J.P. Association between family variables and Mexican American children’s dietary behaviors. J. Nutr. Educ. Behav. 2007, 39, 62–69. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. Annual Update of the HHS Poverty Guidelines; Federal Register: Washington, DC, USA, 2011; Volume 76, pp. 3637–3638.
- Centers for Disease Control and Prevention (CDC). About Child & Teen BMI. Available online: https://www.cdc.gov/healthyweight/assessing/bmi/childrens_bmi/about_childrens_bmi.html#HowIsBMICalculated (accessed on 18 November 2020).
- Hochberg, Y.; Benjamini, Y. More powerful procedures for multiple significance testing. Stat. Med. 1990, 9, 811–818. [Google Scholar] [CrossRef] [PubMed]
- MacKinnon, D.P.; Fairchild, A.J.; Fritz, M.S. Mediation analysis. Annu. Rev. Psychol. 2007, 58, 593–614. [Google Scholar] [CrossRef] [PubMed]
- Batis, C.; Hernandez-Barrera, L.; Barquera, S.; Rivera, J.A.; Popkin, B.M. Food Acculturation Drives Dietary Differences among Mexicans, Mexican Americans, and Non-Hispanic Whites. J. Nutr. 2011, 141, 1898–1906. [Google Scholar] [CrossRef] [PubMed]
- Produce for Better Health Foundation. State of the Plate: 2015 Study on America’s Consumption of Fruit & Vegetables. Available online: http://www.PBHFoundation.org (accessed on 2 February 2021).
- Robson, S.M.; Stough, C.O.; Stark, L.J. The impact of a pilot cooking intervention for parent-child dyads on the consumption of foods prepared away from home. Appetite 2016, 99, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Horton, L.A.; Ayala, G.X.; Slymen, D.J.; Ibarra, L.; Hernandez, E.; Parada, H.; Rock, C.L.; Arredondo, E.M.; Elder, J.P. A Mediation Analysis of Mothers’ Dietary Intake: The Entre Familia: Reflejos de Salud Randomized Controlled Trial. Health Educ. Behav. 2018, 45, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Hingle, M.D.; O’Connor, T.M.; Dave, J.M.; Baranowski, T. Parental involvement in interventions to improve child dietary intake: A systematic review. Prev. Med. 2010, 51, 103–111. [Google Scholar] [CrossRef]
- Thompson, F.E.; Midthune, D.; Subar, A.F.; Kipnis, V.; Kahle, L.L.; Schatzkin, A. Development and evaluation of a short instrument to estimate usual dietary intake of percentage energy from fat. J. Am. Diet. Assoc. 2007, 107, 760–767. [Google Scholar] [CrossRef]


{kind=link}
| Targeted Sector | Intervention Activities Related to Dietary Intake | |||
|---|---|---|---|---|
| Capacity Building | Policy, System, and Environmental Changes | Media Campaign | ||
| Healthcare Condition | Federally Qualified Health Center (FQHC) (N = 1; 3 clinic sites) |
|
|
|
| Public Health Condition | ECE Centers (N = 23) |
|
|
|
| Elementary Schools (N = 13) |
|
|
| |
| Community Recreation Organizations (N = 3) |
|
|
| |
| Restaurants (N = 3) |
|
|
| |
| Overall (N = 1186) a | Control (N = 272) | HC-Only (N = 276) | PH-Only (N = 308) | HC + PH (N = 330) | p-Value | |
|---|---|---|---|---|---|---|
| Mean (SD) or % (n) | Mean (SD) or % (n) | Mean (SD) or % (n) | Mean (SD) or % (n) | Mean (SD) or % (n) | ||
| Child characteristics | ||||||
| Female | 50.5% (599) | 56.3% (153) | 52.2% (144) | 49.4% (152) | 45.5% (150) | 0.06 |
| Age | 6.4 (2.7) | 6.7 (2.7) | 6.5 (2.7) | 6.0 (2.6) | 6.5 (2.7) | <0.05 |
| Latino/Hispanic b | 98.5% (1165) | 99.3% (270) | 99.3% (274) | 97.7% (300) | 97.9% (321) | 0.23 |
| Foreign-born b | 8.3% (98) | 7.0% (19) | 13.8% (38) | 4.2% (13) | 8.5% (28) | <0.01 |
| Only spoke English b | 9.4% (111) | 3.3% (9) | 2.2% (6) | 19.5% (60) | 10.9% (36) | <0.01 |
| Daily cups fruit intake b | 1.4 (0.9) | 1.3 (0.8) | 1.4 (0.9) | 1.4 (0.9) | 1.4 (0.9) | 0.76 |
| Daily cups vegetable intake b | 0.6 (0.4) | 0.6 (0.4) | 0.6 (0.4) | 0.6 (0.4) | 0.6 (0.4) | 0.49 |
| Daily percentage energy from fat (%Efat) b | 35.0 (4.6) | 35.0 (4.2) | 35.0 (4.9) | 35.2 (4.6) | 34.7 (4.7) | 0.54 |
| BMI percentile | 76.3 (26.5) | 72.9 (27.9) | 78.4 (26.1) | 75.8 (26.4) | 77.9 (25.5) | 0.05 |
| Parenting strategies c | ||||||
| Monitoring | 4.1 (0.9) | 4.2 (0.8) | 4.0 (0.9) | 4.1 (0.9) | 4.1 (0.9) | 0.09 |
| Limit setting | 4.4 (1.0) | 4.4 (0.9) | 4.3 (1.0) | 4.4 (0.9) | 4.5 (1.0) | 0.23 |
| Discipline b | 2.7 (1.3) | 2.8 (1.4) | 2.6 (1.3) | 2.8 (1.4) | 2.7 (1.3) | 0.47 |
| Control | 3.1 (1.0) | 3.1 (1.0) | 3.1 (1.0) | 3.1 (1.0) | 3.1 (1.1) | 0.78 |
| Reinforcement b | 3.3 (1.5) | 3.4 (1.5) | 3.0 (1.5) | 3.5 (1.4) | 3.2 (1.5) | <0.01 |
| Permission seeking | 3.8 (1.2) | 3.8 (1.2) | 3.7 (1.2) | 4.0 (1.1) | 3.8 (1.4) | <0.01 |
| Overall (N = 848) a | Control (N = 195) | HC-only (N = 201) | PH-only (N = 223) | HC + PH (N = 229) | p-value | |
| Caregiver characteristics | ||||||
| Female | 98.4% (834) | 98.0% (191) | 98.5% (198) | 98.2% (219) | 98.7% (226) | 0.94 |
| Relationship to child | 0.47 | |||||
| Mother | 93.2% (790) | 92.8% (181) | 93.0% (187) | 91.5% (204) | 95.2% (218) | |
| Other relatives | 6.8% (58) | 7.2% (14) | 7.0% (14) | 8.5% (19) | 4.8% (11) | |
| Age d | 35.7 (8.5) | 37.0 (9.1) | 36.1 (8.8) | 34.8 (8.3) | 35.0 (7.6) | <0.05 |
| Latino/Hispanic d | 97.5% (824) | 98.0% (191) | 99.0% (198) | 95.5% (211) | 97.8% (224) | 0.12 |
| Foreign-born c | 67.1% (568) | 66.7% (130) | 75.1% (151) | 57.5% (127) | 69.9% (160) | <0.01 |
| Only spoke English d | 9.1% (77) | 5.1% (10) | 2.5% (5) | 19.4% (43) | 8.3% (19) | <0.01 |
| Married d | 72.7% (613) | 77.8% (151) | 69.2% (139) | 74.2% (164) | 70.0% (159) | 0.18 |
| Education d | <0.01 | |||||
| Less than high school | 31.7% (268) | 25.6% (50) | 35.8% (72) | 24.1% (53) | 40.6% (93) | |
| High school and above | 68.3% (577) | 74.4% (145) | 64.2% (129) | 75.9% (167) | 59.4% (136) | |
| Employed d | 39.5% (334) | 45.1% (88) | 39.8% (80) | 44.3% (98) | 29.7% (68) | <0.01 |
| Owns a home d | 21.9% (185) | 30.9% (60) | 16.4% (33) | 26.2% (58) | 14.9% (34) | <0.01 |
| Daily cups fruit intake d | 1.6 (1.3) | 1.7 (1.3) | 1.7 (1.3) | 1.6 (1.3) | 1.6 (1.4) | 0.59 |
| Daily cups vegetable intake d | 2.0 (1.3) | 2.0 (1.4) | 2.1 (1.3) | 2.0 (1.3) | 1.9 (1.3) | 0.69 |
| Daily percentage energy from fat (%Efat) d | 31.2 (4.2) | 31.2 (3.9) | 31.1 (4.5) | 31.1 (4.1) | 31.2 (4.4) | 0.99 |
| BMI (kg/m2) d | 31.8 (7.2) | 30.3 (6.2) | 31.4 (7.0) | 32.6 (7.5) | 32.6 (7.6) | <0.01 |
| Family characteristics | ||||||
| Household size e | 4.7 (1.5) | 4.7 (1.3) | 4.8 (1.5) | 4.7 (1.4) | 4.8 (1.6) | 0.37 |
| Ratio of family income to poverty (PIR) e,f | 0.9 (0.8) | 1.2 (1.0) | 0.7 (0.5) | 1.1 (0.9) | 0.8 (0.6) | <0.01 |
| Food assistance e,g | 70.6% (597) | 58.0% (113) | 74.1% (149) | 63.4% (140) | 85.2% (195) | <0.01 |
| Family diet-context | ||||||
| Days past week food from relatives’ or friends’ home | 1.0 (1.3) | 0.9 (1.2) | 1.1 (1.4) | 1.0 (1.3) | 0.9 (1.3) | 0.34 |
| Days past week food from restaurants | 1.3 (1.1) | 1.3 (1.0) | 1.3 (1.1) | 1.4 (1.1) | 1.2 (1.1) | 0.37 |
| Days past week family morning meal e | 3.7 (2.5) | 3.4 (2.4) | 3.9 (2.6) | 3.6 (2.5) | 3.7 (2.6) | 0.08 |
| Days past week family afternoon meal/snack e | 5.3 (2.2) | 5.0 (2.4) | 5.7 (1.8) | 5.1 (2.4) | 5.5 (2.2) | <0.01 |
| Days past week family evening meal e | 5.3 (2.3) | 4.9 (2.5) | 5.4 (2.2) | 5.5 (2.1) | 5.4 (2.2) | <0.01 |
| Full Sample (All Children) | Restricted Sample (Children with BMI Percentile ≥ 85%) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Adjusted Mean | β | SE | p-Value | Adjusted p-Value a | n | Adjusted Mean | β | SE | p-Value | Adjusted p-Value a | |
| CHILD DIET OUTCOMES | ||||||||||||
| Child daily cups fruit | 931 | 513 | ||||||||||
| Control | 227 | 1.16 | - | - | - | - | 108 | 1.09 | - | - | - | - |
| HC-only | 206 | 1.31 | 0.15 | 0.08 | 0.051 | 0.051 | 123 | 1.32 | 0.23 | 0.10 | 0.020 | 0.040 |
| PH-only | 241 | 1.17 | 0.01 | 0.07 | 0.918 | 0.918 | 130 | 1.06 | −0.02 | 0.10 | 0.809 | 0.918 |
| HC + PH | 257 | 1.15 | −0.01 | 0.07 | 0.891 | 0.891 | 152 | 1.15 | 0.06 | 0.10 | 0.507 | 0.891 |
| Child daily cups vegetables | 931 | 513 | ||||||||||
| Control | 227 | 0.57 | - | - | - | - | 108 | 0.55 | - | - | - | - |
| HC-only | 206 | 0.56 | −0.01 | 0.04 | 0.785 | 0.968 | 123 | 0.55 | 0.00 | 0.04 | 0.968 | 0.968 |
| PH-only | 241 | 0.57 | 0.00 | 0.03 | 0.993 | 0.993 | 130 | 0.53 | −0.03 | 0.04 | 0.503 | 0.993 |
| HC + PH | 257 | 0.56 | −0.01 | 0.04 | 0.737 | 0.854 | 152 | 0.56 | 0.01 | 0.04 | 0.854 | 0.854 |
| Child daily percentage energy from fat (%Efat) | 931 | 513 | ||||||||||
| Control | 227 | 34.94 | - | - | - | - | 108 | 35.51 | - | - | - | - |
| HC-only | 206 | 34.49 | −0.45 | 0.48 | 0.349 | 0.349 | 123 | 34.11 | −1.40 | 0.64 | 0.028 | 0.056 |
| PH-only | 241 | 36.01 | 1.07 | 0.46 | 0.020 | 0.040 | 130 | 36.20 | 0.69 | 0.63 | 0.274 | 0.274 |
| HC + PH | 257 | 35.40 | 0.45 | 0.46 | 0.329 | 0.658 | 152 | 35.62 | 0.11 | 0.62 | 0.861 | 0.861 |
| MEDIATORS: CAREGIVER DIETARY INTAKE | ||||||||||||
| Caregiver daily cups fruit | 669 | 380 | ||||||||||
| Control | 161 | 1.68 | - | - | - | - | 82 | 1.52 | - | - | - | - |
| HC-only | 152 | 1.83 | 0.16 | 0.15 | 0.289 | 0.289 | 96 | 1.90 | 0.38 | 0.19 | 0.043 | 0.086 |
| PH-only | 175 | 1.55 | −0.13 | 0.14 | 0.362 | 0.724 | 94 | 1.47 | −0.04 | 0.19 | 0.818 | 0.818 |
| HC + PH | 181 | 1.59 | −0.08 | 0.14 | 0.564 | 0.953 | 108 | 1.53 | 0.01 | 0.19 | 0.953 | 0.953 |
| Caregiver daily cups vegetable | 669 | 380 | ||||||||||
| Control | 161 | 1.97 | - | - | - | - | 82 | 1.75 | - | - | - | - |
| HC-only | 152 | 2.01 | 0.04 | 0.14 | 0.773 | 0.773 | 96 | 1.92 | 0.17 | 0.19 | 0.364 | 0.728 |
| PH-only | 175 | 1.80 | −0.17 | 0.14 | 0.221 | 0.442 | 94 | 1.68 | −0.07 | 0.19 | 0.721 | 0.721 |
| HC + PH | 181 | 1.93 | −0.04 | 0.14 | 0.785 | 0.785 | 108 | 1.97 | 0.22 | 0.19 | 0.236 | 0.472 |
| Caregiver daily percentage energy from fat (%Efat) | 655 | 373 | ||||||||||
| Control | 159 | 31.49 | - | - | - | - | 82 | 30.83 | - | - | - | - |
| HC-only | 148 | 30.13 | −1.36 | 0.50 | 0.006 | 0.012 | 92 | 30.46 | −0.37 | 0.66 | 0.576 | 0.576 |
| PH-only | 170 | 31.42 | −0.07 | 0.47 | 0.886 | 0.886 | 93 | 31.73 | 0.91 | 0.65 | 0.161 | 0.322 |
| HC + PH | 178 | 30.97 | −0.52 | 0.48 | 0.278 | 0.556 | 106 | 31.04 | 0.21 | 0.65 | 0.738 | 0.738 |
| MEDIATORS: PARENTING STRATEGIES b | ||||||||||||
| PEAS: Monitoring | 931 | 512 | ||||||||||
| Control | 227 | 4.07 | - | - | - | - | 108 | 4.14 | - | - | - | - |
| HC-only | 205 | 4.17 | 0.10 | 0.09 | 0.254 | 0.443 | 122 | 4.22 | 0.09 | 0.11 | 0.443 | 0.443 |
| PH-only | 241 | 4.10 | 0.03 | 0.09 | 0.759 | 0.813 | 130 | 4.11 | −0.03 | 0.11 | 0.813 | 0.813 |
| HC + PH | 258 | 4.21 | 0.14 | 0.09 | 0.107 | 0.214 | 152 | 4.23 | 0.09 | 0.11 | 0.400 | 0.400 |
| PEAS: Limit setting | 932 | 513 | ||||||||||
| Control | 227 | 4.44 | - | - | - | - | 108 | 4.44 | - | - | - | - |
| HC-only | 206 | 4.60 | 0.15 | 0.10 | 0.114 | 0.114 | 123 | 4.67 | 0.23 | 0.12 | 0.047 | 0.094 |
| PH-only | 241 | 4.44 | 0.00 | 0.09 | 0.997 | 0.997 | 130 | 4.55 | 0.12 | 0.11 | 0.317 | 0.634 |
| HC + PH | 258 | 4.49 | 0.05 | 0.09 | 0.572 | 0.572 | 152 | 4.55 | 0.11 | 0.11 | 0.331 | 0.572 |
| PEAS: Discipline | 923 | 508 | ||||||||||
| Control | 224 | 2.50 | - | - | - | - | 107 | 2.69 | - | - | - | - |
| HC-only | 205 | 2.43 | −0.07 | 0.14 | 0.612 | 0.612 | 122 | 2.54 | −0.14 | 0.18 | 0.419 | 0.612 |
| PH-only | 239 | 2.73 | 0.24 | 0.13 | 0.072 | 0.144 | 129 | 2.89 | 0.21 | 0.17 | 0.230 | 0.230 |
| HC + PH | 255 | 2.70 | 0.20 | 0.13 | 0.127 | 0.254 | 150 | 2.75 | 0.06 | 0.17 | 0.719 | 0.719 |
| PEAS: Control | 932 | 533 | ||||||||||
| Control | 227 | 2.92 | - | - | - | - | 108 | 2.72 | - | - | - | - |
| HC-only | 206 | 2.88 | −0.04 | 0.10 | 0.683 | 0.692 | 123 | 2.67 | −0.05 | 0.12 | 0.692 | 0.692 |
| PH-only | 241 | 2.82 | −0.10 | 0.09 | 0.289 | 0.289 | 130 | 2.54 | −0.18 | 0.12 | 0.128 | 0.256 |
| HC + PH | 258 | 2.81 | −0.11 | 0.09 | 0.249 | 0.283 | 152 | 2.60 | −0.12 | 0.12 | 0.283 | 0.283 |
| PEAS: Reinforcement | 927 | 510 | ||||||||||
| Control | 224 | 2.99 | - | - | - | - | 106 | 3.02 | - | - | - | - |
| HC-only | 205 | 3.30 | 0.32 | 0.15 | 0.041 | 0.063 | 122 | 3.38 | 0.37 | 0.20 | 0.063 | 0.063 |
| PH-only | 241 | 3.26 | 0.27 | 0.15 | 0.066 | 0.132 | 130 | 3.08 | 0.06 | 0.19 | 0.756 | 0.756 |
| HC + PH | 257 | 3.23 | 0.25 | 0.15 | 0.100 | 0.200 | 152 | 3.25 | 0.23 | 0.19 | 0.227 | 0.227 |
| PEAS: Permission seeking | 931 | 512 | ||||||||||
| Control | 227 | 3.61 | - | - | - | - | 108 | 3.62 | - | - | - | - |
| HC-only | 205 | 3.76 | 0.15 | 0.13 | 0.248 | 0.456 | 122 | 3.74 | 0.13 | 0.17 | 0.456 | 0.456 |
| PH-only | 241 | 3.68 | 0.07 | 0.13 | 0.557 | 0.557 | 130 | 3.73 | 0.12 | 0.17 | 0.484 | 0.557 |
| HC + PH | 258 | 3.78 | 0.17 | 0.13 | 0.192 | 0.384 | 152 | 3.76 | 0.14 | 0.16 | 0.388 | 0.388 |
| MEDIATORS: FAMILY MEAL CONTEXT | ||||||||||||
| Days past week food from relatives’ or friends’ home | 668 | 379 | ||||||||||
| Control | 160 | 1.21 | - | - | - | - | 81 | 1.18 | - | - | - | - |
| HC-only | 152 | 0.99 | −0.22 | 0.16 | 0.180 | 0.360 | 96 | 1.01 | −0.17 | 0.21 | 0.418 | 0.418 |
| PH-only | 175 | 1.27 | 0.06 | 0.15 | 0.699 | 0.717 | 94 | 1.25 | 0.08 | 0.21 | 0.717 | 0.717 |
| HC + PH | 181 | 1.05 | −0.16 | 0.16 | 0.296 | 0.592 | 108 | 1.17 | −0.01 | 0.21 | 0.950 | 0.950 |
| Days past week food from restaurants | 667 | 378 | ||||||||||
| Control | 159 | 1.46 | - | - | - | - | 80 | 1.50 | - | - | - | - |
| HC-only | 152 | 1.13 | −0.33 | 0.12 | 0.005 | 0.007 | 96 | 1.07 | −0.43 | 0.16 | 0.007 | 0.007 |
| PH-only | 175 | 1.34 | −0.12 | 0.11 | 0.276 | 0.276 | 94 | 1.23 | −0.28 | 0.16 | 0.081 | 0.162 |
| HC + PH | 181 | 1.36 | −0.10 | 0.11 | 0.372 | 0.407 | 108 | 1.37 | −0.13 | 0.16 | 0.407 | 0.407 |
| Days past week family morning meal | 668 | 379 | ||||||||||
| Control | 161 | 3.69 | - | - | - | - | 82 | 3.96 | - | - | - | - |
| HC-only | 152 | 3.14 | −0.55 | 0.27 | 0.039 | 0.039 | 96 | 3.11 | −0.85 | 0.35 | 0.017 | 0.034 |
| PH-only | 174 | 4.20 | 0.51 | 0.25 | 0.046 | 0.092 | 93 | 4.38 | 0.42 | 0.35 | 0.227 | 0.227 |
| HC + PH | 181 | 3.46 | −0.24 | 0.26 | 0.361 | 0.361 | 108 | 3.57 | −0.39 | 0.35 | 0.266 | 0.361 |
| Days past week family afternoon meal/snack | 667 | 379 | ||||||||||
| Control | 160 | 5.19 | - | - | - | - | 81 | 5.27 | - | - | - | - |
| HC-only | 152 | 4.92 | −0.27 | 0.25 | 0.272 | 0.544 | 96 | 5.08 | −0.19 | 0.34 | 0.583 | 0.583 |
| PH-only | 175 | 5.37 | 0.19 | 0.23 | 0.427 | 0.854 | 94 | 5.21 | −0.06 | 0.33 | 0.867 | 0.867 |
| HC + PH | 180 | 5.19 | 0.00 | 0.24 | 0.996 | 0.996 | 108 | 5.24 | −0.03 | 0.33 | 0.937 | 0.996 |
| Days past week family evening meal | 669 | 380 | ||||||||||
| Control | 161 | 5.42 | - | - | - | - | 82 | 5.17 | - | - | - | - |
| HC-only | 152 | 5.24 | −0.18 | 0.23 | 0.439 | 0.878 | 96 | 5.21 | 0.04 | 0.32 | 0.904 | 0.904 |
| PH-only | 175 | 5.28 | −0.14 | 0.22 | 0.517 | 0.920 | 94 | 5.14 | −0.03 | 0.32 | 0.920 | 0.920 |
| HC + PH | 181 | 5.25 | −0.17 | 0.23 | 0.444 | 0.888 | 108 | 5.18 | 0.01 | 0.31 | 0.966 | 0.966 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, S.-F.; Zive, M.M.; Schmied, E.; Helm, J.; Ayala, G.X. The Effects of a Multisector, Multilevel Intervention on Child Dietary Intake: California Childhood Obesity Research Demonstration Study. Nutrients 2023, 15, 4449. https://doi.org/10.3390/nu15204449
Lin S-F, Zive MM, Schmied E, Helm J, Ayala GX. The Effects of a Multisector, Multilevel Intervention on Child Dietary Intake: California Childhood Obesity Research Demonstration Study. Nutrients. 2023; 15(20):4449. https://doi.org/10.3390/nu15204449
Chicago/Turabian StyleLin, Shih-Fan, Michelle Murphy Zive, Emily Schmied, Jonathan Helm, and Guadalupe X. Ayala. 2023. "The Effects of a Multisector, Multilevel Intervention on Child Dietary Intake: California Childhood Obesity Research Demonstration Study" Nutrients 15, no. 20: 4449. https://doi.org/10.3390/nu15204449