The Effect of Nerolidol Renal Dysfunction following Ischemia–Reperfusion Injury in the Rat

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ischemia–Reperfusion Injury
2.2. Experimental Protocol and Administration of Nerolidol and Vehicle
2.3. Experimental Groups
2.4. Sample Collection and Analysis
2.5. Gene Expression Analysis
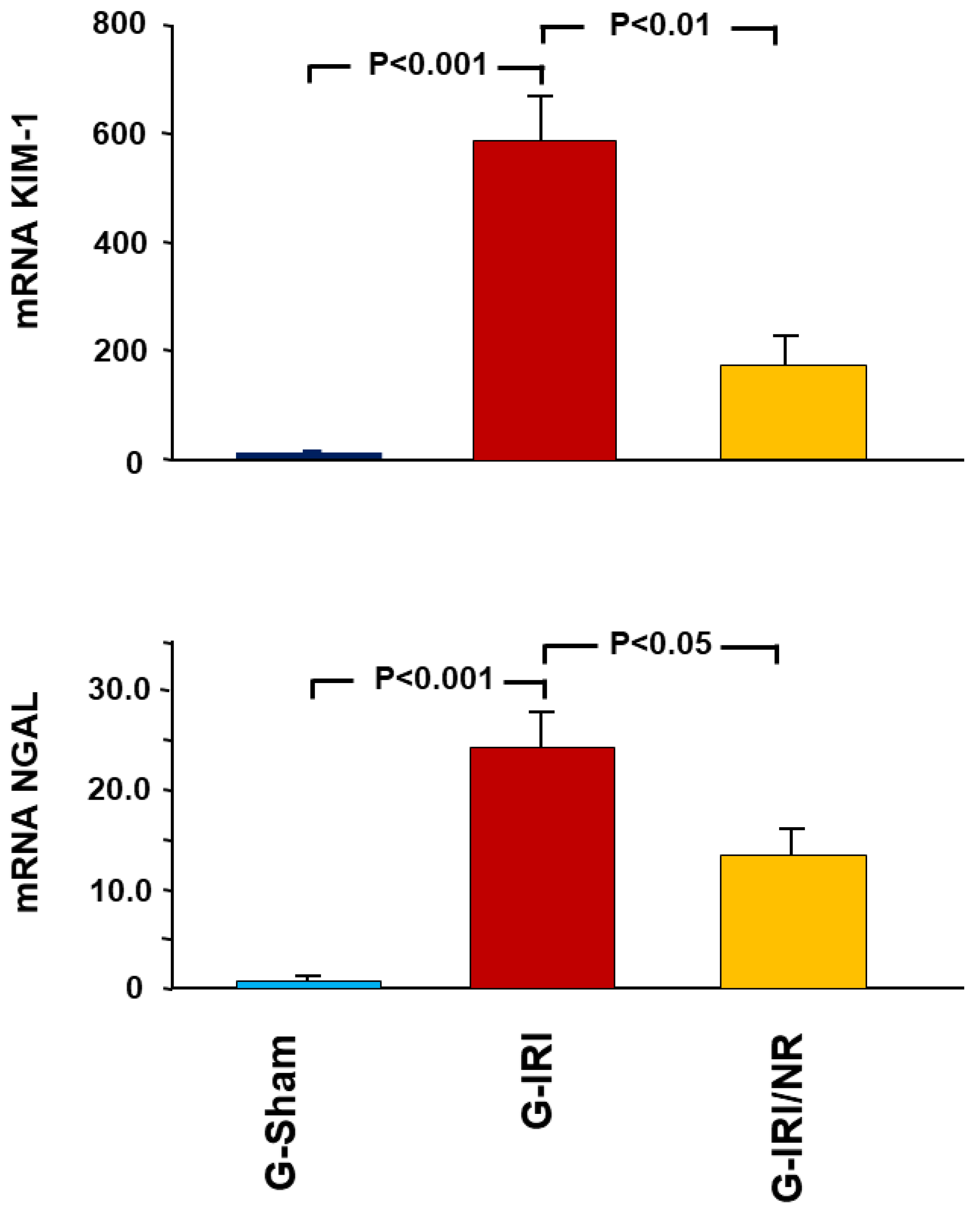
- Acute kidney injury markers, i.e., kidney injury molecule-1 (KIM1) and neutrophil gelatinase-associated lipocalin (NGAL);
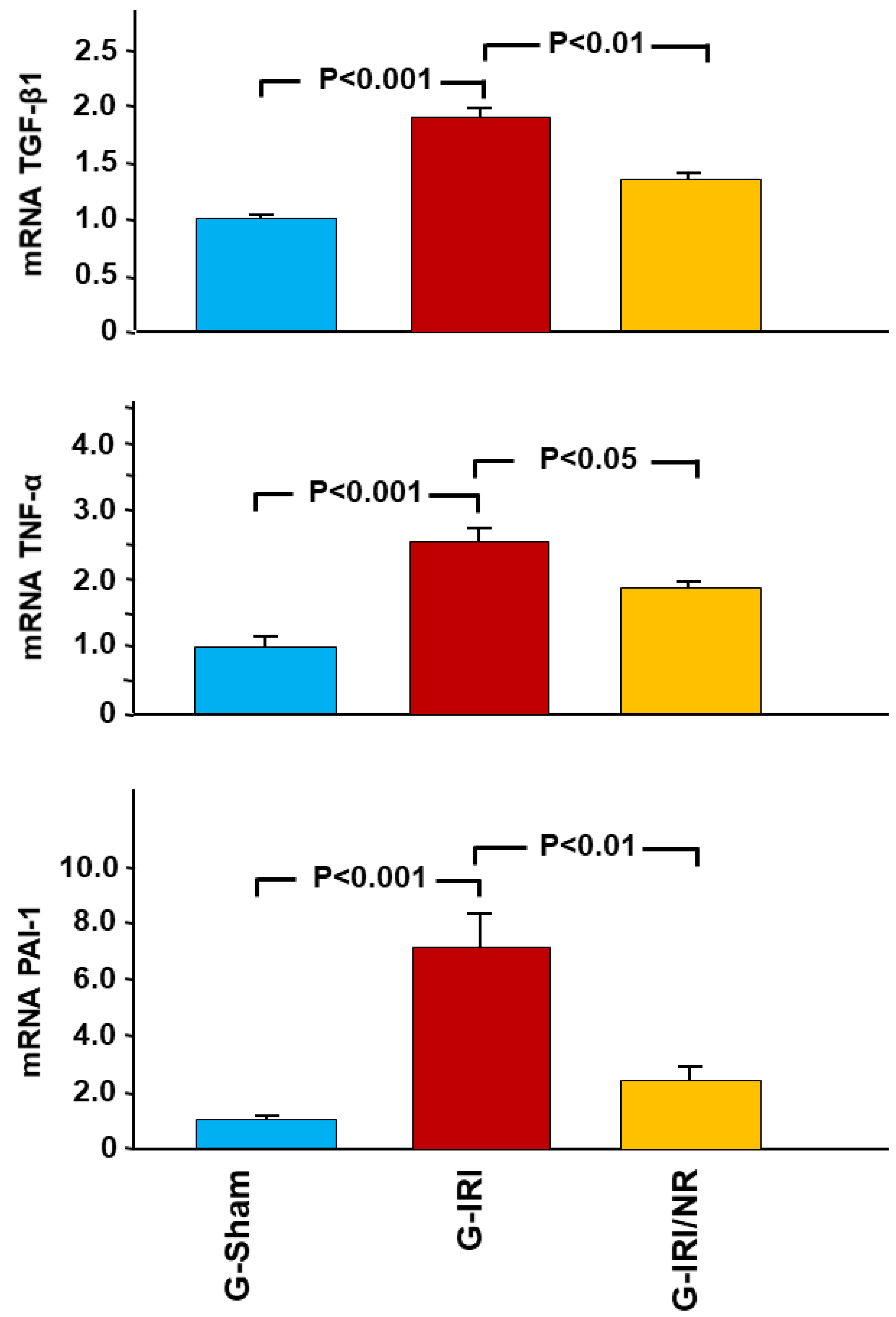
- Cytokines involved in the inflammation and fibrosis, i.e., tumor necrosis factor-α (TNFα), transforming growth factor-β (TGF-β1), interleukin-6 (IL-6), interleukin-1 beta (IL-1β) and plasminogen activator inhibitor-1 (PAI-1);
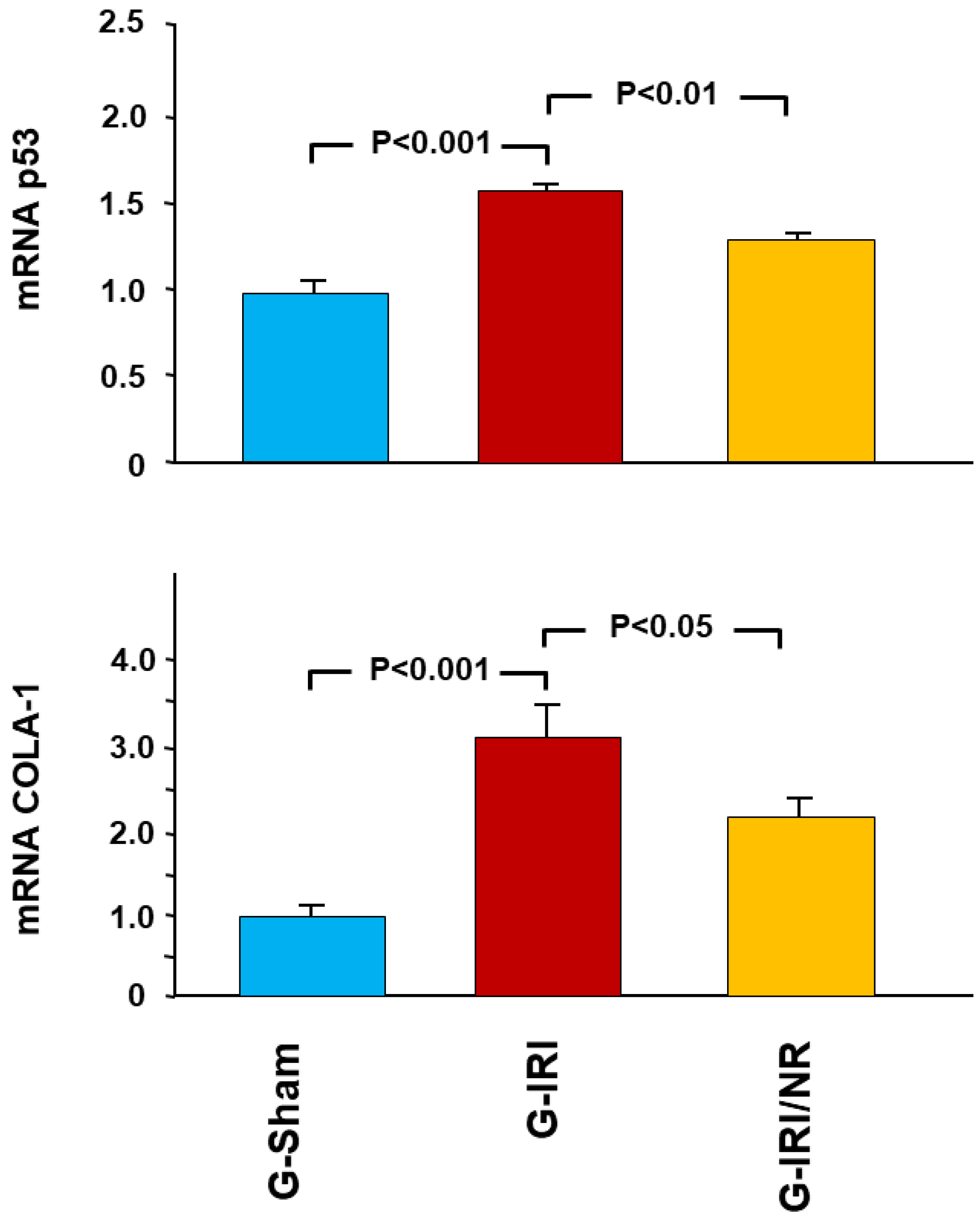
- The proapoptotic gene p53.
- Procollagen type-1 (COLA-1); and
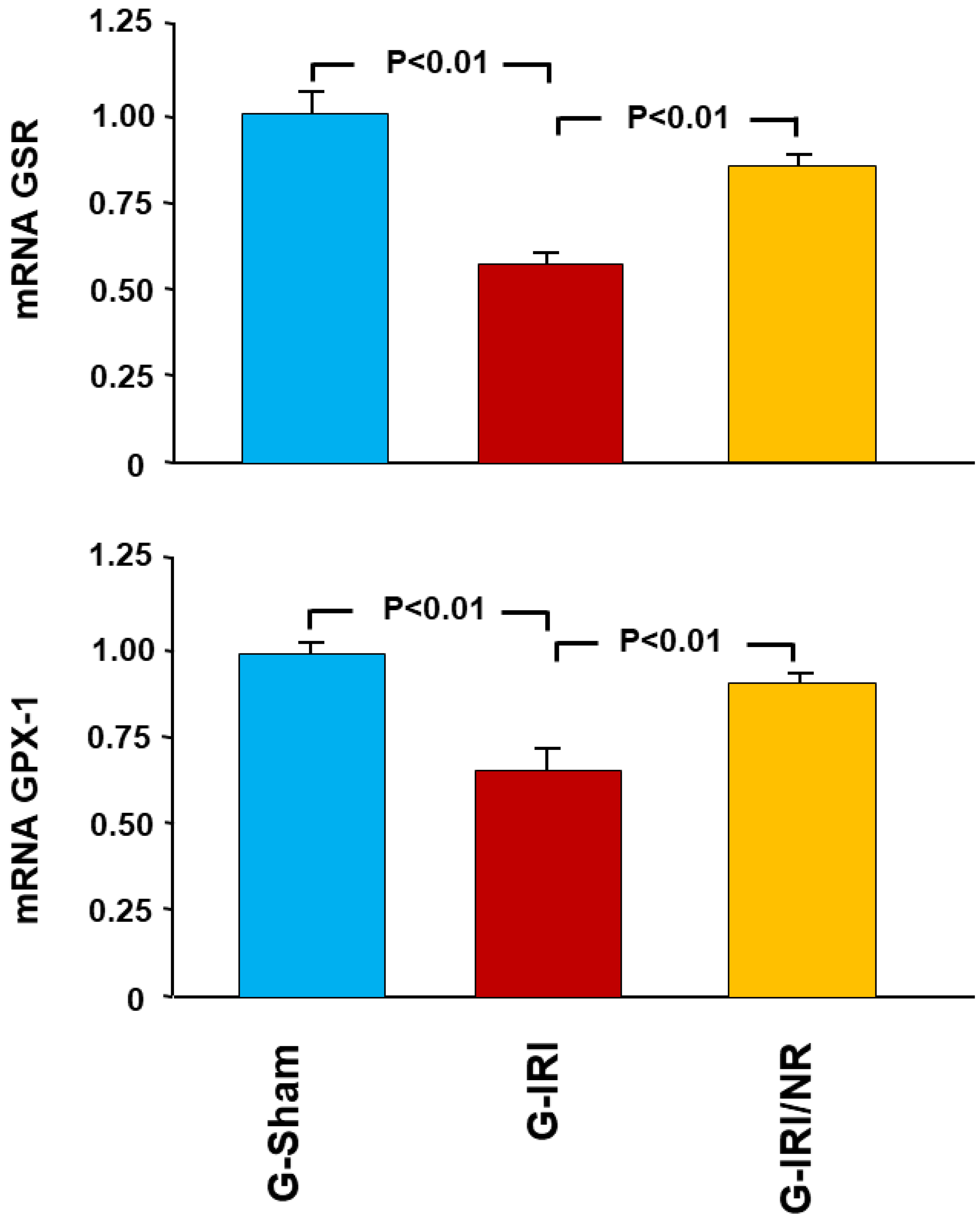
- The antioxidant enzymes glutathione peroxidase (GPX-1) and glutathione-disulfide reductase (GSR).
2.6. Enzyme-Linked Immunosorbent Assay (ELISA)
2.7. Histological Studies
3. Statistical Analysis
4. Results
4.1. Gene Expression Analysis Results
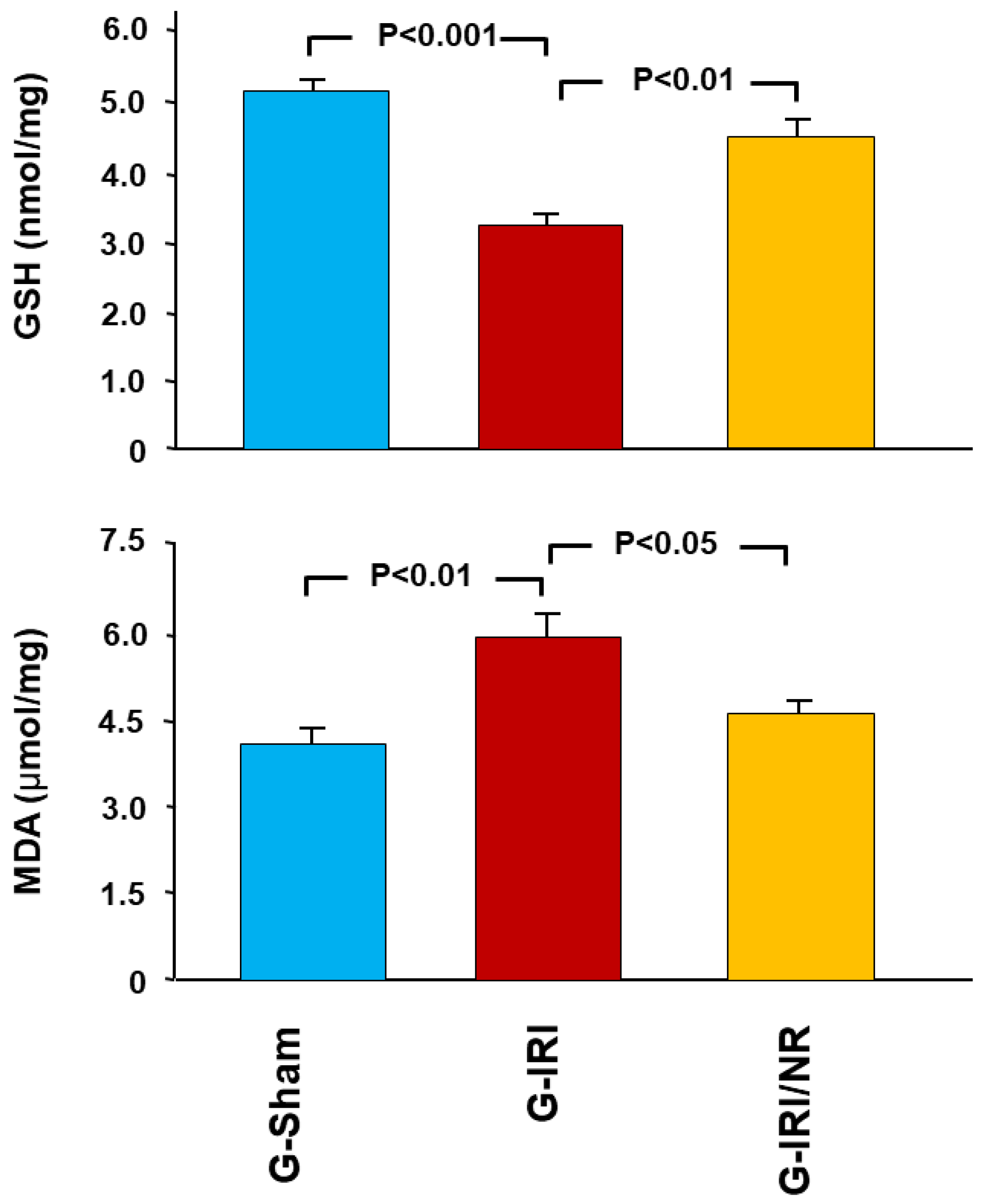
4.2. Enzyme-Linked Immunosorbent Assay (ELISA) Results
4.3. Histological Studies
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Weight, S.C.; Bell, P.R.; Nicholson, M.L. Renal ischaemia-reperfusion injury. Br. J. Surg. 1996, 83, 162–170. [Google Scholar] [PubMed]
- Myers, B.D.; Miller, D.C.; Mehigan, J.T.; Robertson, C.R.; Derby, G.; Spencer, R.; Friedman, S. Nature of the renal injury following total renal ischemia in man. J. Clin. Investig. 1984, 73, 329–341. [Google Scholar] [CrossRef] [Green Version]
- Hammad, F.T.; Davis, G.; Zhang, X.Y.; Wheatley, A.M. Endotelin ETA and ETB receptor antagonism during cold preservation in renal transplantation. Transplantation 2001, 71, 619–627. [Google Scholar] [CrossRef]
- Hammad, F.T.; Wheatley, A.M.; Davis, G. Role of endothelin ET(A) receptor antagonism in the post-transplant renal response to angiotensin II in the rat. Exp. Physiol. 2001, 86, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Goes, N.; Urmson, J.; Ramassar, V.; Halloran, P. Ischemic acute tubular necrosis induces an extensive local cytokine response. Evidence for induction of interferon-gamma, transforming growth factor-beta 1, granulocyte-macrophage colony-stimulating factor, interleukin-2, and interleukin-10. Transplantation 1995, 59, 565–572. [Google Scholar] [CrossRef]
- Petersen, N.S.; Mitchell, H.K. Recovery of protein synthesis after heat shock: Prior heat treatment affects the ability of cells to translate mRNA. Proc. Natl. Acad. Sci. USA 1981, 78, 1708–1711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troppmann, C.; Gillingham, K.J.; Benedetti, E.; Almond, P.S.; Gruessner, R.W.; Najarian, J.S.; Matas, A.J. Delayed graft function, acute rejection, and outcome after cadaver renal transplantation. Transplantation 1995, 59, 962–968. [Google Scholar] [CrossRef]
- Unal, S.; Ozmen, S.; DemIr, Y.; Yavuzer, R.; LatIfoğlu, O.; Atabay, K.; Oguz, M. The Effect of Gradually Increased Blood Flow on Ischemia-Reperfusion Injury. Ann. Plast. Surg. 2001, 47, 412–416. [Google Scholar] [CrossRef]
- Yang, C.W.; Kim, B.S.; Kim, J.; Ahn, H.J.; Park, J.H.; Jin, D.C.; Kim, Y.S.; Bang, B.K. Preconditioning with sodium arsenite inhibits apoptotic cell death in rat kidney with ischemia/reperfusion or cyclosporine-induced Injuries. The possible role of heat-shock protein 70 as a mediator of ischemic tolerance. Nephron Exp. Nephrol. 2001, 9, 284–294. [Google Scholar] [CrossRef]
- Ferreira, F.M.; Palmeira, C.M.; Oliveira, M.M.; Santos, D.; Simões, A.M.; Rocha, S.M.; Coimbra, M.A.; Peixoto, F. Nerolidol effects on mitochondrial and cellular energetics. Toxicol. Vitr. 2012, 26, 189–196. [Google Scholar] [CrossRef]
- Lapczynski, A.; Bhatia, S.; Letizia, C.; Api, A. Fragrance material review on nerolidol (isomer unspecified). Food Chem. Toxicol. 2008, 46, S247–S250. [Google Scholar] [CrossRef] [PubMed]
- Bakkali, F.; Averbck, S.; Averbck, D.; Ldaomar, M. Biological effects of essential oils—A review. Food Chem. Toxicol. 2008, 46, 446–475. [Google Scholar] [CrossRef] [PubMed]
- Asaikumar, L.; Vennila, L.; Akila, P.; Sivasangari, S.; Kanimozhi, K.; Premalatha, V.; Sindhu, G. Preventive effect of nerolidol on isoproterenol induced myocardial damage in Wistar rats: Evidences from biochemical and histopathological studies. Drug Dev. Res. 2019, 80, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Kaur, D.; Pahwa, P.; Goel, R.K. Protective Effect of Nerolidol Against Pentylenetetrazol-Induced Kindling, Oxidative Stress and Associated Behavioral Comorbidities in Mice. Neurochem. Res. 2016, 41, 2859–2867. [Google Scholar] [CrossRef] [PubMed]
- Neto, J.D.N.; De Almeida, A.A.C.; Oliveira, J.D.S.; Dos Santos, P.S.; De Sousa, D.P.; De Freitas, R.M. Antioxidant Effects of Nerolidol in Mice Hippocampus After Open Field Test. Neurochem. Res. 2013, 38, 1861–1870. [Google Scholar] [CrossRef]
- Krist, S.; Banovac, D.; Tabanca, N.; Wedge, D.E.; Gochev, V.K.; Wanner, J.; Schmidt, E.; Jirovetz, L. Antimicrobial Activity of Nerolidol and its Derivatives against Airborne Microbes and Further Biological Activities. Nat. Prod. Commun. 2015, 10, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Sun, D.; Bao, Y.; Shi, Y.; Cui, Y.; Guo, M. Nerolidol Protects Against LPS-induced Acute Kidney Injury via Inhibiting TLR4/NF-κB Signaling. Phytother. Res. 2017, 31, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Türkmen, N.B.; Yüce, H.; Taşlidere, A.; Şahin, Y.; Çiftçi, O. The Ameliorate Effects of Nerolidol on Thioasteamide-induced Oxidative Damage in Heart and Kidney Tissue. Turk. J. Pharm. Sci. 2022, 19, 1–8. [Google Scholar] [CrossRef]
- Hammad, F.T.; Al-Salam, S.; AlZaabi, S.S.; Alfalasi, M.M.; Hammad, A.F.; Yasin, J.; Lubbad, L. The effect of neprilysin and renin inhibition on the renal dysfunction following ischemia-reperfusion injury in the rat. Physiol. Rep. 2021, 9, e14723. [Google Scholar] [CrossRef]
- Klopell, F.C.; Lemos, M.; Sousa, J.P.B.; Comunello, E.; Maistro, E.L.; Bastos, J.K.; de Andrade, S.F. Nerolidol, an Antiulcer Constituent from the Essential Oil of Baccharis dracunculifolia DC (Asteraceae). Z. Nat. C J. Biosci. 2007, 62, 537–542. [Google Scholar] [CrossRef]
- Chatauret, N.; Badet, L.; Barrou, B.; Hauet, T. Ischemia-reperfusion: From cell biology to acute kidney injury. Front. Biosci. 2014, 24, S4–S12. [Google Scholar] [CrossRef] [PubMed]
- Furuichi, K.; Wada, T.; Kaneko, S.; Murphy, P.M. Roles of chemokines in renal ischemia/reperfusion injury. Front. Biosci. 2008, 13, 4021–4028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammad, F.T.; Al-Salam, S.; Lubbad, L. Curcumin Provides Incomplete Protection of the Kidney in Ischemia Reperfusion Injury. Physiol. Res. 2012, 61, 503–511. [Google Scholar] [CrossRef]
- Hammad, F.T.; Al-Salam, S.; Lubbad, L. Does aliskiren protect the kidney following ischemia reperfusion injury? Physiol. Res 2013, 62, 681–690. [Google Scholar] [CrossRef]
- Lerman, L.; Textor, S.C. Pathophysiology of ischemic nephropathy. Urol. Clin. N. Am. 2001, 28, 793–803. [Google Scholar] [CrossRef]
- Spurgeon, K.R.; Donohoe, D.L.; Basile, D.P. Transforming growth factor-beta in acute renal failure: Receptor expression, effects on proliferation, cellularity, and vascularization after recovery from injury. Am. J. Physiol. Ren. Physiol. 2005, 288, F568–F577. [Google Scholar] [CrossRef]
- Baldissera, M.D.; Souza, C.F.; Grando, T.H.; Moreira, K.L.; Schafer, A.S.; Cossetin, L.F.; Da, S.A.; Da Veiga, M.L.; Da Rocha, M.I.U.; Stefani, L.M.; et al. Nerolidol-loaded nanospheres prevent behavioral impairment via ameliorating Na(+), K(+)-ATPase and AChE activities as well as reducing oxidative stress in the brain of Trypanosoma evansi-infected mice. Naunyn Schmiedebergs. Arch. Pharm. 2017, 390, 139–148. [Google Scholar] [CrossRef]
- Dobashi, K.; Ghosh, B.; Orak, J.; Singh, I.; Singh, A. Kidney ischemia-reperfusion: Modulation of antioxidant defenses. Mol. Cell. Biochem. 2000, 205, 1–11. [Google Scholar] [CrossRef]
- Jiang, G.P.; Liao, Y.J.; Huang, L.L.; Zeng, X.J.; Liao, X.H. Effects and molecular mechanism of pachymic acid on ferroptosis in renal ischemia reperfusion injury. Mol. Med. Rep. 2020, 23, 63. [Google Scholar] [CrossRef] [PubMed]
- AlAsmari, A.F.; Ali, N.; Alharbi, M.; Alqahtani, F.; Alasmari, F.; Almoqbel, D.; AlSwayyed, M.; Alshammari, A.; Alanazi, M.M.; Alhoshani, A.; et al. Geraniol Ameliorates Doxorubicin-Mediated Kidney Injury through Alteration of Antioxidant Status, Inflammation, and Apoptosis: Potential Roles of NF-κB and Nrf2/Ho-1. Nutrients 2022, 14, 1620. [Google Scholar] [CrossRef]
- Hammad, F.T.; Al Salam, S.; Nemmar, A.; Ali, M.; Lubbad, L. The Effect of Arabic Gum on Renal Function in Reversible Unilateral Ureteric Obstruction. Biomolecules 2019, 9, 25. [Google Scholar] [CrossRef] [Green Version]
- Speeckaert, M.M.; Speeckaert, R.; Laute, M.; Vanholder, R.; Delanghe, J.R. Tumor Necrosis Factor Receptors: Biology and Therapeutic Potential in Kidney Diseases. Am. J. Nephrol. 2012, 36, 261–270. [Google Scholar] [CrossRef]
- Ding, Y.; Choi, M.E. Regulation of autophagy by TGF-beta: Emerging role in kidney fibrosis. Semin. Nephrol 2014, 34, 62–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chorostowska-Wynimko, J.; Swiercz, R.; Skrzypczak-Jankun, E.; Wojtowicz, A.; Selman, S.H.; Jankun, J. A novel form of the plasminogen activator inhibitor created by cysteine mutations extends its half-life: Relevance to cancer and angiogenesis. Mol. Cancer Ther. 2003, 2, 19–28. [Google Scholar]
- Ghosh, A.K.; Vaughan, D.E. PAI-1 in tissue fibrosis. J. Cell. Physiol. 2012, 227, 493–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, A.I.; Tang, S.C.; Lai, K.N.; Leung, J.C. Kidney injury molecule-1: More than just an injury marker of tubular epithelial cells? J. Cell. Physiol. 2013, 228, 228–917. [Google Scholar] [CrossRef]
- Mishra, J.; Ma, Q.; Prada, A.; Mitsnefes, M.; Zahedi, K.; Yang, J.; Barasch, J.; Devarajan, P. Identification of Neutrophil Gelatinase-Associated Lipocalin as a Novel Early Urinary Biomarker for Ischemic Renal Injury. J. Am. Soc. Nephrol. 2003, 14, 2534–2543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comper, W.D.; Hilliard, L.M.; Nikolic-Paterson, D.J.; Russo, L.M. Disease-dependent mechanisms of albuminuria. Am. J. Physiol. Physiol. 2008, 295, F1589–F1600. [Google Scholar] [CrossRef] [Green Version]
- Eppel, G.A.; Osicka, T.M.; Pratt, L.M.; Jablonski, P.; Howden, B.O.; Glasgow, E.F.; Comper, W.D. The return of glomerular-filtered albumin to the rat renal vein. Kidney Int. 1999, 55, 1861–1870. [Google Scholar] [CrossRef] [Green Version]
- Osicka, T.M.; Strong, K.J.; Nikolic-Paterson, D.; Atkins, R.C.; Jerums, G.; Comper, W.D. Renal processing of serum proteins in an albumin-deficient environment: An in vivo study of glomerulonephritis in the Nagase analbuminaemic rat. Nephrol. Dial. Transplant. 2004, 19, 320–328. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| KIM-1 (NM_173149.2) | Forward | GCCTGGAATAATCACACTGTAAG |
| Reverse | GCAACGGACATGCCAACATAG | |
| Probe | d FAM-TCCCTTTGAGGAAGCCGCAGA-BHQ-1 | |
| Lipocalin 2 (LCN2) (NM_130741.1) | Forward | CTGTTCCCACCGACCAATGC |
| Reverse | CCACTGCACATCCCAGTCA | |
| Probe | FAM-TGACAACTGAACAGACGGTGAGCG-BHQ-1 | |
| TNF-α (NM_012675.3) | Forward | CTCACACTCAGATCATCTTCTC |
| Reverse | CCGCTTGGTGGTTTGCTAC | |
| Probe | FAM-CTCGAGTGACAAGCCCGTAGCC-BHQ-1 | |
| TGF-β1 NM_012620.1 | Forward | GTGGCTGAACCAAGGAGACG |
| Reverse | CGTGGAGTACATTATCTTTGCTGTC | |
| Probe | FAM-ACAGGGCTTTCGCTTCAGTGCTC-BHQ-1 | |
| PAI-1 (NM_012620.1) | Forward | GGCACAATCCAACAGAGACAA |
| Reverse | GGCTTCTCATCCCACTCTCAAG | |
| Probe | FAM-CCTCTTCATGGGCCAGCTGATGG-BHQ-1 | |
| IL-6 (NM_012589.2) | Forward | TCACAGAGGATACCACCCACAACA |
| Reverse | CACAAGTCCGGAGAGGAGAC | |
| Probe | FAM-TCAGAATTGCCATTGCACAACTCT-BHQ-1 | |
| IL-1β (NM_031512.2) | Forward | ATGCCTCGTGCTGTCTGACC |
| Reverse | GCTCATGGAGAATACCACTTGTTGG | |
| Probe | FAM-AGCTGAAAGCTCTCCACCTCAATGGA-BHQ-1 | |
| p53 (NM_030989.3) | Forward | CGAGATGTTCCGAGAGCTGAATG |
| Reverse | GTCTTCGGGTAGCTGGAGTG | |
| Probe | FAM-CCTTGGAATTAAAGGATGCCCGTGC-BHQ-1 | |
| COL1A (NM_053304.1) | Forward | CTGACTGGAAGAGCGGAGAGT |
| Reverse | CCTGTCTCCATGTTGCAGTAGAC | |
| Probe | FAM-ACTGGATCGACCCTAACCAAGGC-BHQ-1 | |
| GSR NM_053906.2 | Forward | CATCCCTACCGTGGTCTTCAG |
| Reverse | ATGGACGGCTTCATCTTCAGT | |
| Probe | FAM-CCACCCGCCTATCGGGACAGT-BHQ-1 | |
| GPx-1 NM_030826.4 | Forward | GTGCTGCTCATTGAGAATGTCG |
| Reverse | TCATTCTTGCCATTCTCCTGATG | |
| Probe | FAM-TCCCTCTGAGGCACCACGAC-BHQ-1 | |
| PPIA (NM_017101.1) | Forward | GCGTCTGCTTCGAGCTGT |
| Reverse | CACCCTGGCACATGAATCC | |
| Probe | Quasar 670-TGCAGACAAAGTTCCAAAGACAGCA-BHQ-2 |
| Group | ||||
|---|---|---|---|---|
| G-Sham | G-IRI | G-IRI/NR | ||
| S. Creatinine (mg/dL) | Basal | 0.31 ± 0.02 | 0.30 ± 0.02 | 0.32 ± 0.02 |
| Pre-IRI | 0.29 ± 0.01 | 0.32 ± 0.05 | 0.33 ± 0.02 | |
| Post-IRI | 0.29 ± 0.02 | 1.51 ± 0.48 * | 0.37 ± 0.02 *,$ | |
| S. Urea (mg/dL) | Basal | 28.9 ± 1.4 | 29.0 ± 1.4 | 31.1 ± 2.8 |
| Pre-IRI | 26.6 ± 0.8 | 30.7 ± 2.8 | 28.8 ± 2.3 | |
| Post-IRI | 25.4 ± 0.6 | 82.2 ± 19.8 * | 31.7 ± 2.1 $ | |
| Creatinine Clearance (mL/min) | Basal | 62.3 ± 4.3 | 64.7 ± 9.1 | 63.5 ± 5.7 |
| Pre-IRI | 72.7 ± 3.4 | 69.9 ± 6.6 | 67.0 ± 5.1 | |
| Post-IRI | 76.4 ± 3.0 | 33.5 ± 7.8 * | 74.1 ± 2.8 $ | |
| (1) | ||||
| $ | Group | |||
|---|---|---|---|---|
| * | G-Sham | G-IRI | G-IRI/NR | |
| 24-h Urinary Albumin (µg) | Basal | 0.073 ± 0.005 | 0.078 ± 0.013 | 0.073 ± 0.009 |
| Pre-IRI | 0.077 ± 0.006 | 0.079 ± 0.009 | 0.079 ± 0.006 | |
| Post-IRI | 0.069 ± 0.005 | 0.783 ± 0.111 * | 0.570 ± 0.078 *,$ | |
| Albumin/Creatinine Ratio | Basal | 13.9 ± 1.1 | 13.1 ± 2.1 | 13.6 ± 1.7 |
| Pre-IRI | 13.9 ± 0.9 | 13.7 ± 2.2 | 13.8 ± 0.8 | |
| Post-IRI | 12.4 ± 0.9 | 166.1 ± 27.0 * | 88.8 ± 11.0 *,$ | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hammad, F.T.; Al-Salam, S.; Ahmad, R.; Yasin, J.; Hammad, A.F.; Rasheed, J.A.; Lubbad, L. The Effect of Nerolidol Renal Dysfunction following Ischemia–Reperfusion Injury in the Rat. Nutrients 2023, 15, 455. https://doi.org/10.3390/nu15020455
Hammad FT, Al-Salam S, Ahmad R, Yasin J, Hammad AF, Rasheed JA, Lubbad L. The Effect of Nerolidol Renal Dysfunction following Ischemia–Reperfusion Injury in the Rat. Nutrients. 2023; 15(2):455. https://doi.org/10.3390/nu15020455
Chicago/Turabian StyleHammad, Fayez T., Suhail Al-Salam, Rahaf Ahmad, Javed Yasin, Awwab F. Hammad, Jasmine Abdul Rasheed, and Loay Lubbad. 2023. "The Effect of Nerolidol Renal Dysfunction following Ischemia–Reperfusion Injury in the Rat" Nutrients 15, no. 2: 455. https://doi.org/10.3390/nu15020455