
Teaching Kitchens and Culinary Gardens as Integral Components of Healthcare Facilities Providing Whole Person Care: A Commentary
Abstract
:1. Introduction
2. Development of the Pediatric Weight and Wellness Program
- Medical supervision and ongoing assessment of associated weight-related comorbidities with a pediatric obesity medicine specialist.
- Psychological evaluations and support provided by a child health clinical psychologist addressing issues such as body dysmorphia, motivation, individual and family behavioral changes, and screenings for depression and anxiety.
- Individualized nutrition plans by a dietitian with certification in pediatric weight management.
- Exercise education and assessments along with personal and group fitness sessions provided by an exercise physiologist with certification in personal training by the American College of Sports Medicine, in addition to partnership with local fitness facilities within and outside of the hospital system.
- Parent and child/teen health coaching provided by health and wellness educators.
- Experiential cooking and garden education classes consisting of age-appropriate health education sessions with an emphasis on treatment or prevention of weight-related comorbidities.
- Teen and parent support groups
- Hospital-affiliated resources for at-risk families experiencing food insecurity which became more pronounced during the COVID-19 pandemic (2020–2022).
2.1. PWW Program Culinary Medicine Workshops
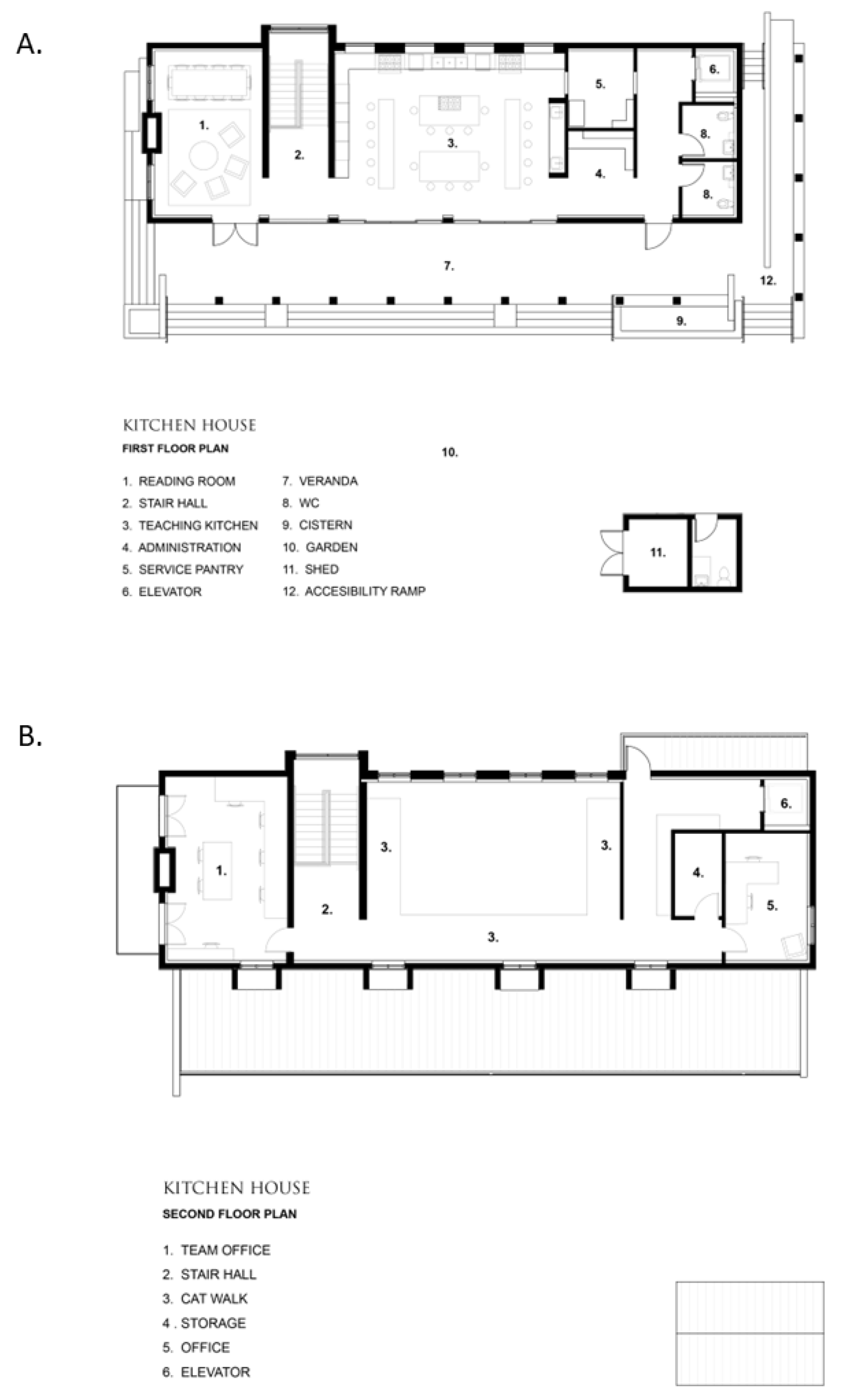
2.2. Partnership with Edible Education Experience at the Emeril Lagasse Foundation Kitchen House and Culinary Garden
2.3. Preliminary Outcomes of PWW Culinary Medicine Workshops
3. Organizational Efforts to Extend the Influence of Teaching Kitchens and Culinary Gardens within the Context of Culinary Medicine
3.1. Development of Advisory and Governance Boards
3.2. Culinary Medicine Curriculum Guide
3.3. Books, Film, and Resource Development
3.4. Employee Wellness
Employee Health and Wellbeing Program Preliminary Outcomes
4. Lessons Learned and Opportunities
- Providing access to experts in various health-related fields, including medicine (primary and specialty care physicians and providers), psychologists, dietitians, and educators. Experiential seed-to-table experiences in combination with a didactical component in culinary medicine are effective in actively engaging participants [5].
- Providing expertise in data acquisition, outcome development, and research methods for demonstrating the efficacy and effectiveness of their program to the scientific community.
- Providing teaching models for healthy lifestyles.
- Providing medical leadership for the collaborative development of an evidence-based culinary medicine curriculum.
- Providing financial resources, such as working with hospital foundations or assisting with obtaining community grants.
- Providing support through the organization’s governance or advisory boards.
- Providing research and learning “laboratories” as locations for the early determination of effective interventions in culinary medicine [5].
- Providing access to culinary experts including garden and culinary educators, chefs, gardeners, and farmers.
- Providing effective seed-to-table teaching models for culinary and garden education while empowering the community to make healthy food choices.
- Providing culinary and garden leadership and expertise in the collaborative development of an evidence-based culinary medicine curriculum.
- Providing a platform for increased community engagement.
- Providing program flexibility, including a safe outdoor meeting space, well-ventilated indoor kitchen, and virtual programming in times of public health crises such as the recent COVID-19 pandemic.
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stierman, B.; Afful, J.; Carroll, M.D.; Chen, T.-C.; Davy, O.; Fink, S.; Fryar, C.D.; Gu, Q.; Hales, C.M.; Hughes, J.P. National Health and Nutrition Examination Survey 2017–March 2020 Prepandemic Data Files—Development of Files and Prevalence Estimates for Selected Health Outcomes. Natl. Health Stat. Rep. 2021, 158, 1–21. [Google Scholar] [CrossRef]
- Fryar, C.D.; Carroll, M.D.; Afful, J. Prevalence of Overweight, Obesity, and Severe Obesity among Adults Aged 20 and Over: United States, 1960–1962 through 2017–2018. Natl. Health Stat. Health E-Stats. 2020; pp. 1–7. Available online: https://stacks.cdc.gov/view/cdc/58669 (accessed on 5 September 2023).
- Ricanati, E.H.; Golubić, M.; Yang, D.; Saager, L.; Mascha, E.J.; Roizen, M.F. Mitigating preventable chronic disease: Progress report of the Cleveland Clinic’s Lifestyle 180 program. Nutr. Metab. 2011, 8, 83. [Google Scholar] [CrossRef] [PubMed]
- La Puma, J. What is culinary medicine and what does it do? Popul. Health Manag. 2016, 19, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, D.M.; Pacheco, L.S.; McClure, A.C.; McWhorter, J.W.; Janisch, K.; Massa, J. Perspective: Teaching Kitchens: Conceptual Origins, Applications and Potential for Impact within Food Is Medicine Research. Nutrients 2023, 15, 2859. [Google Scholar] [CrossRef] [PubMed]
- Stauber, Z.; Razavi, A.C.; Sarris, L.; Harlan, T.S.; Monlezun, D.J. Multisite medical student–led community culinary medicine classes improve patients’ diets: Machine learning–augmented propensity score–adjusted fixed effects cohort analysis of 1381 subjects. Am. J. Lifestyle Med. 2022, 16, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Chu, Y.L.; Storey, K.E.; Veugelers, P.J. Involvement in meal preparation at home is associated with better diet quality among Canadian children. J. Nutr. Educ. Behav. 2014, 46, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Razavi, A.C.; Sapin, A.; Monlezun, D.J.; McCormack, I.G.; Latoff, A.; Pedroza, K.; McCullough, C.; Sarris, L.; Schlag, E.; Dyer, A. Effect of culinary education curriculum on Mediterranean diet adherence and food cost savings in families: A randomised controlled trial. Public Health Nutr. 2021, 24, 2297–2303. [Google Scholar] [CrossRef] [PubMed]
- Razavi, A.C.; Dyer, A.; Jones, M.; Sapin, A.; Caraballo, G.; Nace, H.; Dotson, K.; Razavi, M.A.; Harlan, T.S. Achieving dietary sodium recommendations and atherosclerotic cardiovascular disease prevention through culinary medicine education. Nutrients 2020, 12, 3632. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.A.; Cousineau, B.A.; Rastorguieva, K.; Bonnet, J.P.; Bergquist, S.H. A Teaching Kitchen Program Improves Employee Micronutrient and Healthy Dietary Consumption. Nutr. Metab. Insights 2023, 16, 117863882311591. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, D.M.; Anthony, I.B. Teaching kitchens in the learning and work environments: The future is now. Glob. Adv. Health Med. 2020, 9, 2164956120962442. [Google Scholar] [CrossRef] [PubMed]
- Edible Education Experience. Available online: https://www.edibleed.org/company (accessed on 31 May 2023).
- The Food Is Medicine Map. Available online: https://teachingkitchens.org/map-fim/ (accessed on 31 May 2023).
- Guthrie, G.E.; Flynt, S.; Fals, A. Plant-Powered Recipes to Help You Feel Whole; AdventHealth Press: Altamonte Springs, FL, USA, 2020. [Google Scholar]
- Guthrie, G.E. Eat Plants, Feel Whole; AdventHealth Press: Altamonte Springs, FL, USA, 2020. [Google Scholar]
- Cabrera, E.; Flynt, S.; Hechler, E. Simply Healthy: The Art of Eating Well, Diabetes Edition; AdventHealth Press: Altamonte Springs, FL, USA, 2019. [Google Scholar]
- Hauser, M.E.; Nordgren, J.R.; Adam, M.; Gardner, C.D.; Rydel, T.; Bever, A.M.; Steinberg, E. The first, comprehensive, open-source culinary medicine curriculum for health professional training programs: A global reach. Am. J. Lifestyle Med. 2020, 14, 369–373. [Google Scholar] [CrossRef] [PubMed]
- EXECUTIVE SUMMARY: Biden-Harris Administration National Strategy on Hunger, Nutrition, and Health|The White House. Available online: https://www.whitehouse.gov/briefing-room/statements-releases/2022/09/27/executive-summary-biden-harris-administration-national-strategy-on-hunger-nutrition-and-health/ (accessed on 25 September 2023).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Workshop | Education Topics Covered | Hands-On Experiences | Disease-Specific Topics |
|---|---|---|---|
| Culinary Garden |
|
|
|
| Garden to Table |
|
|
|
| Kitchen Creations |
|
|
|
| Culinary Medicine Prediabetes/Type 2 Diabetes |
|
|
|
| Grocery Store Tour and Scavenger Hunt |
|
|
|
| Know Your Body |
|
|
|
| Targeted Metrics | n | Improved and/or Maintained (n, %) | Worsened and/or Declined (n, %) |
|---|---|---|---|
| Anthropometrics | |||
| % Body Fat | 100 | 65 (65.0%) | 35 (35.0%) |
| Waist * | 143 | 59 (55.1%) | 48 (44.9%) |
| Hip * | 143 | 68 (63.6%) | 39 (36.5%) |
| Cardiometabolic Risk Factors | |||
| Total Cardiometabolic Risk (Improved ≥2 risk factors) | 25 | 19 (76.0%) | 6 (24.0%) |
| High Blood Pressure (Systolic ≥ 95%) | 9 | 9 (100.0%) | 0 (0%) |
| High Blood Pressure (Diastolic ≥ 95%) | 9 | 7 (77.8%) | 2 (22.2%) |
| High Insulin (≥20 mIU/L) | 78 | 58 (74.4%) | 20 (25.6%) |
| High Blood Glucose (≥100 mg/dL) | 23 | 18 (78.3%) | 5 (21.7%) |
| High HbA1c (≥5.7%) | 31 | 24 (77.4%) | 7 (22.6%) |
| High LDL Cholesterol (≥110 mg/dL) | 45 | 33 (73.3%) | 12 (26.7%) |
| High Total Cholesterol (≥170 mg/dL) | 48 | 34 (70.8%) | 14 (29.2%) |
| High Triglyceride (≥100 mg/dL 10 years and under/≥130 mg/dL 11 years and over) | 62 | 48 (77.4%) | 14 (22.6%) |
| Low HDL Cholesterol (≤40 mg/dL) | 32 | 21 (65.6%) | 11 (34.4%) |
| Quality of Life | |||
| Elevated PSC (≥28) ** | 16 | 12 (75.0%) | 4 (25.0%) |
| Sleep and Activity | |||
| Screen Time | 101 | 83 (82.2%) | 18 (17.8%) |
| Sleep | 232 | 152 (65.5%) | 80 (34.5%) |
| Family Activity | 198 | 140 (70.7%) | 58 (29.3%) |
| Individual Activity | 198 | 117 (59.1%) | 81 (40.9%) |
| Nutritional Intake | |||
| Sugar Sweetened Beverage Intake | 205 | 173 (84.4%) | 32 (15.6%) |
| Vegetable Intake | 204 | 168 (82.4%) | 36 (17.7%) |
| Fruit Intake | 205 | 169 (82.4%) | 36 (17.6%) |
| Family Meals | 204 | 168 (82.4%) | 36 (17.7%) |
| Fast Food Intake | 205 | 166 (81.0%) | 39 (19.0%) |
| Breakfast | 58 | 43 (74.1%) | 15 (25.9%) |
| Dairy Intake | 199 | 142 (71.4%) | 57 (28.6%) |
| Survey Question | Percentage of Participants | ||
|---|---|---|---|
| How confident are you in your ability to: | Somewhat/Very Confident Pre (%) | Somewhat/Very Confident Post (%) | Change (%) |
| Incorporate seasonal foods into meals? | 51.9 | 90.4 | +38.5 |
| Design and prepare a balanced plant-based meal? | 50.0 | 88.5 | +38.5 |
| Identify foods growing in the seasonal garden? | 48.8 | 84.6 | +35.8 |
| Identify a whole grain vs. a refined grain? | 51.3 | 84.6 | +33.3 |
| Choose foods that are nutritious? | 82.1 | 98.1 | +16.0 |
| Identify the difference between processed and unprocessed foods? | 78.4 | 94.2 | +15.8 |
| Utilizing kitchen tools while preparing a meal? | 84.0 | 96.2 | +12.2 |
| Use a kitchen knife while preparing a meal? | 84.6 | 94.2 | +9.6 |
| How likely are you to: | Often/Always Pre (%) | Often/Always Post (%) | Change (%) |
| Eat plant-based meals cooked at home? | 30.1 | 50.0 | +19.9 |
| Share your skills and/or knowledge about cooking? | 40.4 | 57.1 | +16.7 |
| Prepare a new recipe? | 57.8 | 68.9 | +11.1 |
| Engage in conversations about your food choices? | 58.0 | 67.9 | +9.9 |
| How do the following values influence your food choices? | Somewhat/Very Important Pre (%) | Somewhat/Very Important Post (%) | Change (%) |
| Seasonal | 50.6 | 80.8 | +30.2 |
| Social impact | 34.8 | 63.5 | +28.7 |
| Environmental impact | 51.3 | 76.9 | +25.6 |
| Grown locally | 56.0 | 80.8 | +24.8 |
| Calorie density | 70.4 | 86.3 | +15.9 |
| Cost | 87.4 | 94.2 | +6.8 |
| Nutritional value | 91.4 | 94.2 | +2.8 |
| Taste | 97.5 | 100.0 | +2.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fals, A.M.; Brennan, A.M. Teaching Kitchens and Culinary Gardens as Integral Components of Healthcare Facilities Providing Whole Person Care: A Commentary. Nutrients 2023, 15, 4162. https://doi.org/10.3390/nu15194162
Fals AM, Brennan AM. Teaching Kitchens and Culinary Gardens as Integral Components of Healthcare Facilities Providing Whole Person Care: A Commentary. Nutrients. 2023; 15(19):4162. https://doi.org/10.3390/nu15194162
Chicago/Turabian StyleFals, Angela M., and Andrea M. Brennan. 2023. "Teaching Kitchens and Culinary Gardens as Integral Components of Healthcare Facilities Providing Whole Person Care: A Commentary" Nutrients 15, no. 19: 4162. https://doi.org/10.3390/nu15194162